
Abstract
Objective
Healthcare assistants (HCAs) are frontline caregivers for older adults. This study evaluated the effectiveness of combining augmented reality (AR) and virtual reality (VR) to implement oral healthcare simulation training for HCAs.
Methods
An experimental design was adopted. HCAs were recruited and randomly assigned to an AR/VR group (n = 40) or a control group (n = 40). The AR/VR group received 2.5 h of AR/VR training. Participants were trained on the Bass brushing technique through AR and on scenario-based oral care procedures for various physical and oral health conditions in older adults through VR. A self-administered questionnaire was employed to collect data before and after the training. Generalized estimating equations were used to analyze the differences between pretest and posttest results.
Results
After the training, the HCAs in the AR/VR group achieved a significantly greater increase in their level of oral care-related knowledge (β = 2.55, effect size [ES] = 1.62), self-efficacy (β = 4.23, ES = 0.75), and behavioral intention (β = 2.10, ES = 0.55) relative to the control group.
Conclusion
This study revealed that the application of an AR/VR simulation system can effectively improve the geriatric oral care performance of HCAs.
Introduction
As populations worldwide continue to age, the demand for long-term care has consistently increased. In 2018, Taiwan became an aged society in which the proportion of people aged 65 years or older was 14%. Taiwan is expected to become a super-aged society by 2025, at which point the proportion of older adults in its population is expected to exceed 20%. 1 For older adults, oral health considerably affects general health and quality of life. 2 Moreover, poor oral health is associated with aspiration pneumonia. 3 Deteriorating oral function can also affect the oral health-related quality of life of older adults. 4 A study indicated that the chewing ability of older adults influences the types of foods and beverages that they want to consume. 5 Oral frailty in older people is associated with an increased risk of depression, physical frailty, sarcopenia, disability, and mortality.6,7 Professional oral care interventions can reduce the amount of oral bacteria and the incidence of pneumonia among older adults.8,9 Long-term care facilities that provide excellent oral care are linked to a lower incidence of pneumonia, 10 a lower risk of hospitalization, 8 and lower medical expenses. 11
Virtual reality (VR) can be used to create an immersive learning environment through visualization, 12 which enables learners to absorb more from course content than they can through a traditional learning environment. A state-of-the-art system can be used to create an immersive environment that enables users to experience a virtual world. Augmented reality (AR) integrates visual and sensory cues to enhance feedback and immersion. That is, AR combines virtual elements with the real-world environment. Through AR, virtual scenarios can be superimposed onto the real world to increase user interactivity. The major difference between AR and VR is that AR users are not fully immersed in a virtual environment; they are placed in a virtual world with real-life elements. 13 VR has been widely applied in medical education and surgical training as well as in clinical practice.14–16 In recent studies, VR has also been used in healthcare, including in the care of patients with stroke, Parkinson's disease, cerebral palsy, and autism spectrum disorder.17–20 AR has more frequently been applied in medical education in various fields, such as emergency medicine, remote medicine, prehospital care, and other forms of relevant training. 21 For oral health-related applications, AR has been implemented in training for surgery and dental implants or to improve education and specialty training in prosthodontics, especially for training clinical and operational skills.22,23
Healthcare assistants (HCAs) are frontline workers who provide assistance in nursing homes and other long-term care settings for older adults. These assistants, who can serve as home health aides, personal or home care aides, companions, nursing assistants, or home health nurses, often work in a patient's home. One of their responsibilities is to assist an older adult in properly practicing and fully implementing oral care after accounting for their physical problems and oral health conditions. In Taiwan, HCAs provide household assistance and daily care services to older adults. 24 A certified HCA must undergo continuing education to maintain their skills and capabilities. Among HCAs who have undergone oral health professional education, the oral care knowledge and skills of HCAs who received multimedia instruction have been reported to improve more than those of HCAs who received traditional instruction.25,26 However, instruction-based education does not provide an environment that places learners in realistic situations. Although learners can learn toothbrushing skills through the demonstrations, they cannot practice toothbrushing. AR/VR technology may provide a solution to this problem. VR simulations can increase the realism and comprehensiveness of learning, and AR can increase the thoroughness of skills training.
The coronavirus disease 2019 (COVID-19) pandemic has created considerable challenges for healthcare professionals worldwide. HCAs are members of a vulnerable population within the healthcare delivery system, and they have been severely affected by the COVID-19 pandemic.27,28 During the pandemic, learning through the traditional classroom teaching method increased the risk of exposure such that HCAs found it difficult to continue receiving high-quality education. AR/VR training enables learners to experience realistic scenarios in a risk-free environment. Studies have mostly explored VR technology29–31 and AR technology21–23 separately in their experiments; learners could not develop operational skills through VR-based experiments. To address this problem, the present study combined an AR toothbrush training system with an individualized VR scenario-based training system to improve the learning outcomes related to the geriatric oral care performance of HCAs. In another study, a VR training system implemented for dental hygiene students had positive effects on the knowledge, attitudes, self-efficacy, and behavioral intention of students with respect to providing oral healthcare for older adults with disabilities. 29 The present study is the first to evaluate the combined use of AR and VR for oral healthcare simulation training with the aim of improving the geriatric oral care performance of HCAs.
Materials and methods
Research design and participants
The present study used a randomized control trial design that was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (KMUHIRB-F(I)-20200098). An informed consent form was signed by all the participants of the present study. The study period was from October 2021 to January 2022.
Individuals aged 65 years or older were excluded from the present study. G*Power (version 3.1.9.4) was used to determine the expected effect size (ES), which was calculated to be 0.3 on the basis of a pilot study in which an alpha level of 0.05, a power of 80%, and a dropout rate of 20% were applied. The total expected sample size was 35 for each group. Overall, 80 certified HCAs working at long-term care institutions were recruited for our study and were randomly assigned to an AR/VR group (n = 40) or a control group (n = 40).
Instruments
A structured questionnaire was developed to collect data pertaining to demographic information, oral care-related knowledge, attitudes toward oral care, self-efficacy of oral care, and behavioral intention to perform oral care. The questionnaire was reviewed by a panel of experts to assess its face and content validity. The content validity index of the questionnaire was between 0.98 and 1.00. The questionnaire was pilot-tested with a convenience sample of 10 HCAs to ensure that respondents (i.e. participants) could understand its content. On the basis of the pilot test results, the items of the questionnaire were revised to enhance their clarity and appropriateness.
Outcome measures
All items related to the outcome measures were modified from an established and validated questionnaire used in another study. 29 Table 1 presents the statements on oral care-related knowledge, attitudes, self-efficacy, and behavioral intention. Each measure was checked for reliability and internal consistency.
Statements of oral care-related knowledge, attitude, self-efficacy, and behavioral intention to oral care.
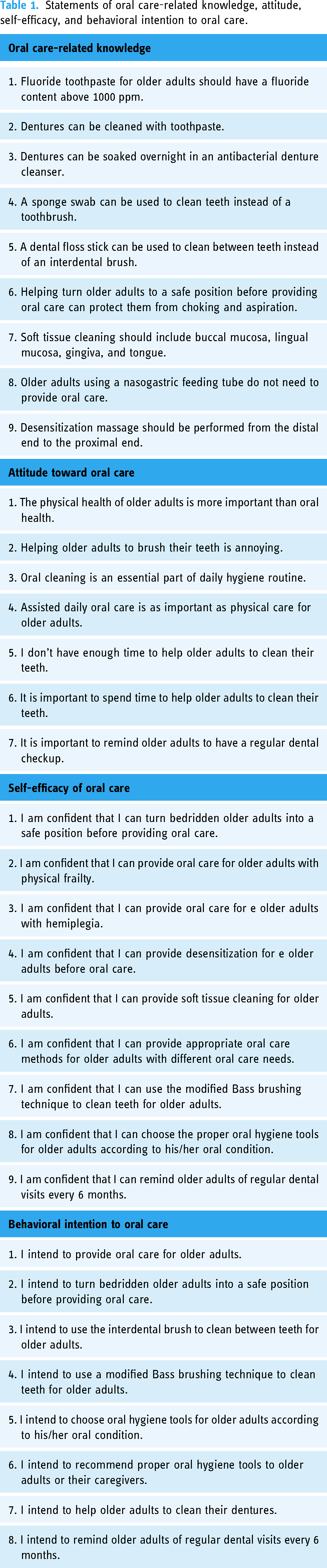
Oral care-related knowledge
Nine statements were used to measure oral care-related knowledge, including “Helping turn elderly people to a safe position before providing oral care can protect them from choking and aspiration.” For such items, the possible responses included True (1), False (0), and I do not know (0), with total scores ranging from 0 to 9 and a higher score indicating a higher level of oral care-related knowledge. The Kuder–Richardson-20 reliability coefficient for oral care-related knowledge was 0.56.
Attitudes toward oral care
Seven statements were used to assess attitudes toward oral care, including “Oral cleaning is an essential part of daily hygiene routine.” Each item was scored on a 5-point Likert scale, with endpoints ranging from 1 (strongly disagree) to 5 (strongly agree) and total possible scores ranging from 7 to 35. The Cronbach's α for the scale was 0.84.
Self-efficacy of oral care
Nine statements were used to measure the self-efficacy of oral care, including “I am confident that I can turn bedridden elderly people into a safe position before providing oral care.” Each item was scored on a 5-point scale, with endpoints ranging from 1 (strongly disagree) to 5 (strongly agree) and total possible scores ranging from 9 to 45. The Cronbach's α for the scale was 0.94.
Behavioral intention to oral care
The behavioral intention measures assessed how likely the participants were to regularly engage in oral care behavior; they were scored using a 5-point scale, with endpoints ranging from 1 (strongly disagree) to 5 (strongly agree) and total possible scores ranging from 8 to 40. Eight statements were used to evaluate behavioral intention to perform oral care, including “I intend to provide oral care for older adults.” The Cronbach's α for the scale was 0.94.
Intervention
The participants in the AR/VR group received VR-based training for 1.5 h and AR-based training for 1 h, whereas those in the control group did not undergo any intervention. The AR-based training system (PVIX Oral, EPED) digitized the steps of the Bass toothbrushing technique and used optical tracking technology to enable the participants to conduct self-assessments and obtain feedback scores in real-time. The AR system was equipped with an optical tracking unit, a three-dimensional (3D) training head model, and a wireless toothbrush (Figure 1). The training system started with an introduction to the steps of the Bass toothbrushing technique. A learner was required to brush away colored patches (simulated dental plaque) on the surface of a set of teeth in a practice window by using the Bass technique. The training system provides immediate scoring for the learners’ performance of the four steps after the completion of the AR practice as a form of evaluation of the learners’ brushing skills. These four parts are (a) placing the toothbrush at a 45° angle to the gum line, (b) brushing teeth gently, (c) performing straight brushing for the inner side of the six front teeth, and (d) removing simulated dental plaque. Each part was scored between 0 and 100, and the minimum passing grade for each step was 80. Each participant in the AR/VR group was allowed a maximum of twice practice for the AR training.

(a) AR-based training system. (b) An optical tracking unit. (c) A 3D training head model. (d) A wireless toothbrush. (e) Software of Bass toothbrushing technique step. (f) An example score.
The VR-based training system (PVIX VR, EPED) was analyzed in another study. 29 The VR training module of the system comprised three sessions pertaining to the individualized standard procedures of oral care, which were classified on the basis of three types of physical conditions (i.e. physical frailty, hemiplegia, and paralysis) and oral conditions (i.e., denture wearing and missing teeth) of older adults. In the present study, the participants in the AR/VR group were required to wear 3D glasses and use a controller (Figure 2). Each session began with an introduction to the physical and oral health of older adults. Subsequently, the participants learned correct oral care steps and skills by watching an animated video that indicated the oral health status of a virtual object. The geriatric oral care components comprised oral desensitization, denture cleaning, teeth cleaning (i.e. modified Bass brushing technique and interdental brush using), soft tissue cleaning, the use of a moisturizing mouth rinse, and the issuing of dental visit reminders. Each session was followed by a quiz, which was implemented as an automatic assessment process to ensure the quality of the intervention's learning outcomes. Each participant in the AR/VR group was allowed a maximum of twice to practice for the VR training module.

VR-based training system: (a) four-sided projection screen, (b) a 3D glass, (c) controller, (d) physical and oral condition of a virtual object, (e) choice of oral care tools, (f) animated videos of tooth cleaning skills, and (g) a quiz.
Each participant made an appointment to receive one-on-one assistance from a researcher in their free time; the intervention of the present study was conducted in the AR/VR oral care training classroom at Kaohsiung Medical University. Each AR/VR training session involved three steps and required 2.5 h to complete for each participant. First, each participant read a short introduction on the use of the AR and VR systems on an iPad (15 min). Second, they performed the oral care steps on a virtual older adult client through the VR-based system (90 min). Third, they performed the Bass brushing technique on a training head model through the AR-based system (60 min; Figure 3).

Procedure of the VR- and AR-based training (a), A short introduction on an iPad (b), using the VR-based curriculum (c), using the AR-based curriculum.
Data collection
Information was collected at pretest and posttest. All participants completed the self-administered questionnaires within 10–15 min of completing the training at baseline and posttest. All data were collected at the AR/VR oral care training center.
Statistical analysis
Stata version 13.1 (Stata Corp LP, College Station, TX, USA) was used for statistical analysis. A chi-square test and two sample t-tests were performed to compare the demographic variables of the AR/VR and control groups. The pretest and posttest mean differences in oral care-related knowledge, attitude, self-efficacy, and behavioral intention in both groups were tested by paired t-tests. The correlations between the outcome variables of the AR/VR group at posttest were analyzed by analyzing their Pearson correlation coefficients. Linear regression with generalized estimating equations adjusted for age and gender and confounding factors was performed to obtain the regression coefficients for conducting between-group comparisons of the outcome variables. The ES (Cohen's d) of continuous variables was calculated by dividing the mean difference between the two groups with respect to the changes that occurred from pretest to posttest by the standard deviation of the sample. ES values of 0.20, 0.50, and 0.80 were regarded as small, moderate, and large values, respectively. 32 A 95% confidence interval (CI) and a p-value of <0.05 were used to determine significance. All statistical analyses involved a two-tailed test.
Results
Recruitment
Figure 4 presents the Consolidated Standards of Reporting Trials (CONSORT) 33 ; a flowchart of the process for recruiting participants. All participants completed the pretest and posttest procedures.
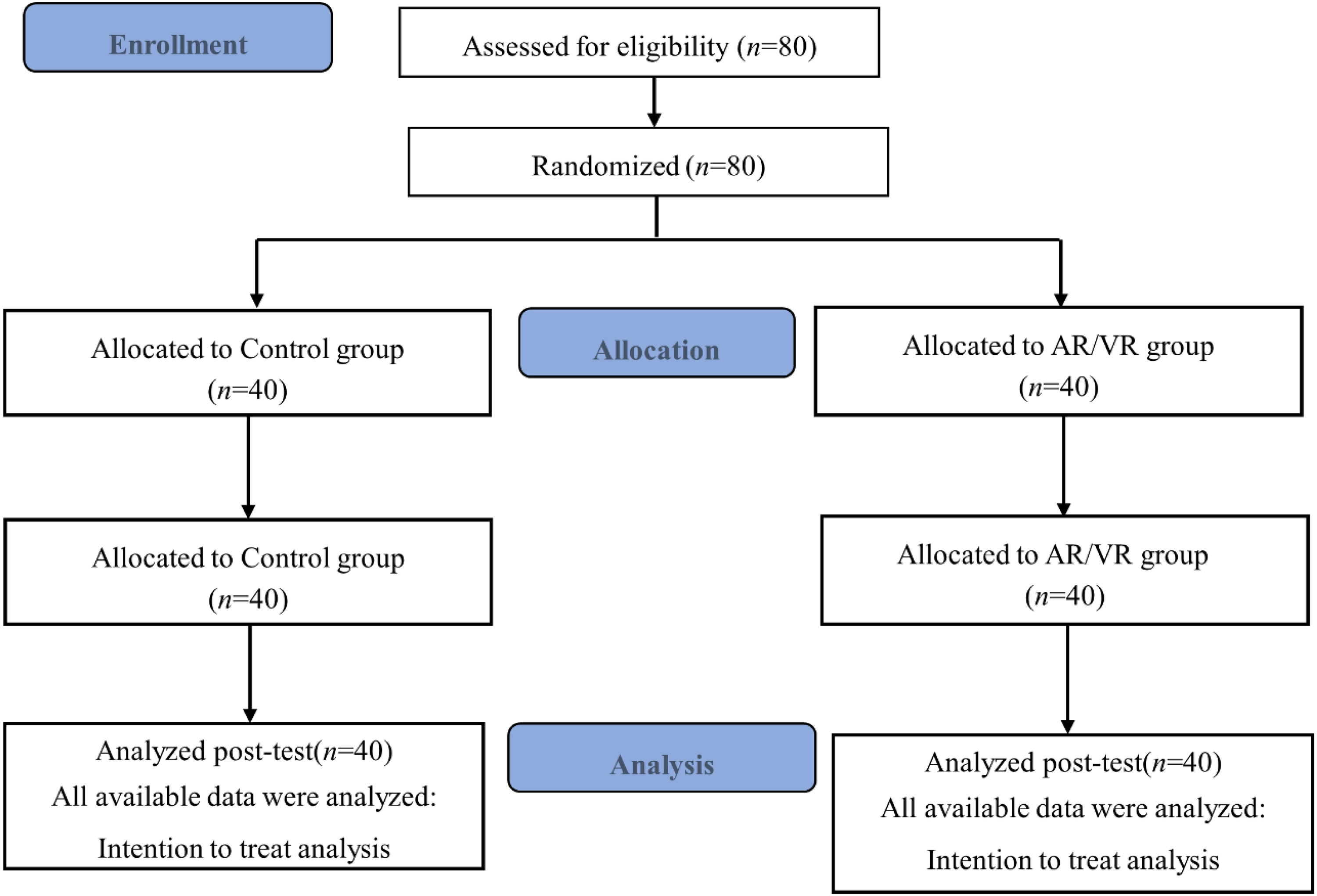
CONSORT flowchart of participant recruitment.
Baseline information
The distribution of baseline information among the participants is presented in Table 2. No differences in the variables were observed between the two groups (all p > 0.05). In both groups, most of the participants had served as HCAs for 1–5 years (AR/VR group, 67.5%; control group, 62.6%). Furthermore, 62.5% of the participants reported that they had never undergone oral health educational training. Only 12.5% and 20.0% of the participants in the AR/VR and control groups, respectively, reported that they always provided dental care for the older adults whom they served. The association between oral care-related knowledge and attitude toward oral care (r = 0.278, p < 0.05), attitude toward oral care and self-efficacy of oral care (r = 0.277, p < 0.05), self-efficacy of oral care, and behavioral intention (r = 0.642, p < 0.001) at baseline was found in the present study.
Demographic information among the AR/VR group and control group.

AR: augmented reality; VR: virtual reality.
P was the difference between groups by chi-square test and two sample t-test.
Effects of intervention on oral care-related knowledge, attitudes, self-efficacy, and behavioral intention
Figure 5 presents a comparison of the pretest and posttest results of the AR/VR and control groups with respect to their oral care-related knowledge, attitudes toward oral care, self-efficacy of oral care, and behavioral intention to perform oral care. HCAs in the AR/VR group had a higher level of oral care-related knowledge (mean difference = 2.6 ± 0.3, p < 0.001), attitudes (mean difference = 1.9 ± 0.8, p = 0.022), self-efficacy of oral care (mean difference = 4.5 ± 1.1, p < 0.001), and behavioral intention to perform oral care (mean difference = 1.9 ± 0.7, p = 0.009) at posttest.
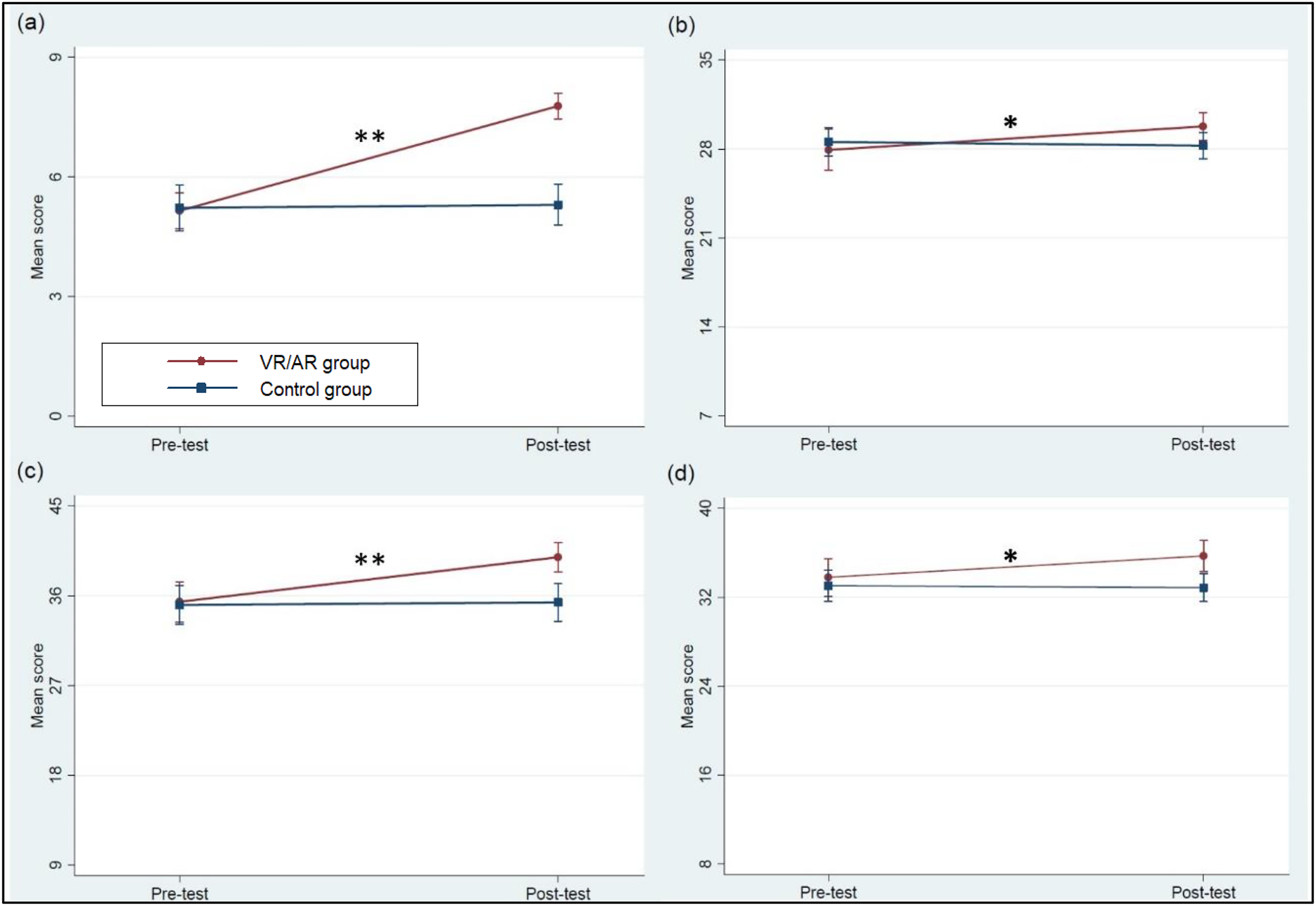
Pretest and posttest mean scores of oral care-related knowledge, attitude, self-efficacy, and behavioral intention to oral care at AR/VR and control groups (a), oral care-related knowledge (b), attitude toward oral care (c), self-efficacy of oral care (d), behavioral intention to oral care.
Table 3 presents the correlations between oral care-related knowledge, attitudes toward oral care, self-efficacy of oral care, and behavioral intention to perform oral care in the AR/VR group at posttest. Attitudes toward oral care (r = 0.727, p < 0.001) and self-efficacy of oral care (r = 0.880, p < 0.001) were positively correlated with behavioral intention. Similarly, self-efficacy of oral care was positively associated with attitudes toward oral care (r = 0.609, p < 0.001). However, oral care-related knowledge was negatively associated with attitudes toward oral care (r = −0.343, p < 0.05).
Correlation between oral care-related knowledge, attitude, self-efficacy, and behavioral intention among healthcare assistants in the AR/VR group at posttest.

AR: augmented reality; VR: virtual reality.
*p < 0.05; **p < 0.001.
Table 4 presents the regression-estimated differences in oral care-related knowledge, attitudes, self-efficacy of oral care, and behavioral intention between the AR/VR and control groups. The AR/VR group exhibited greater improvements in their oral care-related knowledge (β = 2.55, 95% CI = 1.87, 3.23; ES = 1.62), self-efficacy of oral care (β = 4.23, 95% CI = 1.78, 6.67; ES = 0.75), and behavioral intention (β = 2.10, 95% CI = 0.44, 3.75; ES = 0.55) at posttest than did the control group.
Main and interaction effects of change oral care-related knowledge, attitude toward oral care, self-efficacy of oral care, behavioral intention between AR/VR and control groups.

AR: augmented reality; CI: confidence interval; ES: effect size; VR: virtual reality.
aReference group, control group.
bReference group, pretest.
cReference group, control group × pretest.
dGEE regression coefficients (β) adjusted for age, gender, and confounding factors.
ES was calculated as the mean difference of change between pretest and posttest measurements between the two groups.
Discussion
We discovered that compared with the participants in the control group, those in the AR/VR group exhibited a significant improvement in terms of their level of knowledge, self-efficacy, and behavioral intention. The greatest ES was observed for the level of knowledge and self-efficacy, and a median ES was observed for attitudes and behavioral intention. Furthermore, in the AR/VR group, attitudes toward oral care and self-efficacy were positively associated with behavioral intention. The implementation of AR/VR simulation for oral care training produced favorable results. VR-based training was implemented in a simulated environment where the participants were trained to properly perform oral care procedures and steps with consideration of the physical and oral health conditions of an older adult. Through the AR-based learning approach, the participants were taught proper brushing techniques by enabling them to practice on real objects in a virtual environment.
The present study revealed that AR/VR training significantly increased the participants’ behavioral intention to perform oral care. According to the theory of reasoned action, which was proposed by Fishbein in 1967, 34 an individual's intention to engage in a behavior determines whether they exhibit that behavior. That is, an individual's intention to engage in healthy behaviors can predict changes in their health-related behaviors. Studies have reported that VR-based interventions effectively increase a person's intention to receive a COVID-19 vaccine35,36 and increase men's intention to perform testicular self-examinations when taking a shower or to seek help for testicular swelling. 37 The application of AR technology has also been reported to improve the walking behavior of AR technology users 38 and enhance the intentions of students to avoid drug use. 39
In the present study, significant improvements were observed in the level of knowledge, and self-efficacy of oral care among the participants who underwent AR/VR intervention. VR is a viable teaching strategy for improving knowledge acquisition and the care self-efficacy of trainees in medical education and patient care.31,40,41 A study demonstrated that AR was effective in improving the injection-related knowledge and skills of nursing students. 42 Another study reported that skills training can improve a learner's self-efficacy.43,44 Our study used an AR training system that enables learners to practice their toothbrushing skills, which improved their self-efficacy in oral care. Scholars also indicated that the application of AR in training increases the self-efficacy of learners. 45 Furthermore, a study that explored the application of VR-based interventions for dementia caregivers demonstrated that virtual learning increased their knowledge of dementia. 46 Through the integration of a VR environment and AR-based equipment, researchers can create simulated scenarios that combine virtual and real worlds to enable learners to learn through simulated practice.
Our findings also indicated that in the AR/VR group, attitudes and self-efficacy of oral care were positively associated with behavioral intention. Similar to a previous study on health-related intention that reported a change in the attitude and self-efficacy of a participant could lead to a change in their behavioral intention. 47 A study on the physical activities of university students revealed that physical activity self-efficacy and the behavioral intention to join a physical activity were correlated. 48 According to the theory of planned behavior, 49 the attitudes and self-efficacy of an individual are factors that influence their behavioral intention. In the present study, a stronger attitude toward oral care was positively associated with a higher level of self-efficacy in oral care after the completion of AR/VR training. Studies that have included nursing students have reported a link between self-efficacy and attitudes related to clinical care50,51 and a link between attitudes and self-efficacy related to sexual healthcare. 52
This study is subject to a number of limitations. First, the diverse backgrounds of the HCAs could have influenced the research outcomes. Nevertheless, we adopted a randomized controlled design and did not detect any significant differences between the two groups for any variable at baseline. Second, the time difference between the pretest and the pretest is only 1 week, and learners may still remember the questions of the pretest, which poses a threat to the posttest. It is recommended that future studies should track longitudinal effects. Third, data were collected through a self-reported questionnaire, which could have led to social desirability bias. Fourth, this is the first study to evaluate a hybrid AR/VR simulation training on the knowledge, attitude, self-efficacy, and behavioral intention of HCAs; future studies should also investigate the follow-up effects on their behavior change. Finally, the participants in the present study were recruited from multiple centers in southern Taiwan, which is representative; however, the generalization of findings to other geographical areas should be done carefully.
Conclusion
The present study is the first to apply an AR/VR simulated system for oral care training for HCAs. Our study revealed that combining a hybrid AR/VR training system was effective in improving the oral care-related knowledge, self-efficacy, and behavioral intention of HCAs. During the COVID-19 pandemic, implementing the traditional classroom teaching method increased the risk of exposure such that HCAs found it difficult to receive high-quality on-the-job education and training. The AR/VR training can be accessed every day and enables self-learning during an infectious disease outbreak. AR and VR immersive learning technologies can be transformative tools for conducting risk-free oral care training for HCAs. Furthermore, a hybrid AR/VR system can be incorporated into training programs and continuing medical education for healthcare professionals to improve their geriatric oral care performance.
Footnotes
Acknowledgements
The authors thank the Southern Taiwan Science Park Bureau of the Ministry of Science and Technology and the Ministry of Science and Technology, Taiwan for their assistance.
Contributorship
HLH was responsible for the project. YLC and HLH drafted the manuscript. YLC, PCL, and PCL assisted with recruitment, collected, conducted data analysis, and interpretation of results. CYL, YK, and YKC provided advice throughout the project, commented, and assisted in editing the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (KMUHIRB-F(I)-20200098).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Southern Taiwan Science Park Bureau of the Ministry of Science and Technology (grant number: CY-05-07-39-110) and the National Science and Technology Council, Taiwan (grant number: NSTC112-2314-B-037-082-MY3).
Guarantor
HLH.