
Abstract
Background
In emergency departments, suturing is a typical procedure for closing lacerated wounds but is invasive and often causes anxiety and pain. Virtual reality (VR) intervention has been reported as a relaxing measure.
Objective
The study aims to examine the effects of VR intervention on anxiety, pain, physiological parameters, local anesthesia requirements and satisfaction in Chinese adult patients undergoing wound closure in emergency departments in Hong Kong.
Methods
Adult patients who had lacerated wounds and were undergoing wound closure by suturing can communicate in Chinese and were hemodynamically stable were invited for this trial. Eighty patients were randomly assigned to the VR group, which received VR intervention and standard care, or to the control group, which received standard care only. The primary outcome was anxiety, and the secondary outcomes included pain, blood pressure, pulse rate, satisfactory with pain management, service satisfactory, and extra local analgesia requirement. Outcomes were conducted at baseline, during the procedure and 5 min after the procedure.
Results
The VR group had a significantly greater reduction in anxiety (p < 0.001), pain (p < 0.001), systolic blood pressure (p < 0.001), diastolic blood pressure (p < 0.001), pulse rate (p = 0.003) and requested less amount of additional local anesthesia (p = 0.025). The satisfactory level with pain management (p = 0.019) and service (p = 0.002) were significantly higher in participants who received VR intervention. In addition, most participants preferred to have VR in the future, and no major adverse events associated with the use of VR were reported.
Conclusion
This pilot study provides insight into the use of VR and the direction of future studies. It may effectively improve psychological and physiological outcomes in adult patients during wound-closure procedures in emergency departments.
Introduction
Wound closure by suturing is one of the most common treatments for patients with lacerated wounds in emergency departments (EDs). In Hong Kong, simple lacerated wound closure is usually performed by trained nurses. The wound closure rate is approximately 2.6% per year in a regional public ED that provides services for a population of 501,491. 1 The clients are usually anxious because of unexpected injury and invasive wound-closure procedures. Numerous studies have shown that 75% of ED patients experience anxiety during a painful procedure2–4 and approximately 50% of them report that pain is caused by minor diagnostic or therapeutic medical procedures, such as laceration wound repair.5,6 Anxiety is associated with increased self-reported pain intensity, decreased pain tolerance, and reduced satisfaction with pain management and pain-related complications.2,7 Failure to manage anxiety and pain effectively during wound closure may delay procedures and causes complications.8 Experience of anxiety and pain may increase the need for local anesthesia, reduce patient's satisfaction rate, and cause negative physiological parameters, such as increased blood pressure and pulse rate.9,10
Traditionally, pharmacological intervention is broadly applied to ensure smooth procedure and reduce patients’ anxiety and pain. However, side effects and contraindications should be considered, such as vomiting, nausea, and respiratory depression, in addition to increased risk of local anesthetic systematic toxicity.11,12
Thus, nonpharmacological interventions, such as distraction techniques by chatting and deep breathing exercises, are commonly used by nurses but are oftentimes underused in the busy acute care environment of an ED because they are labor intensive. These interventions fail to provide distraction because patients would inevitably see the needle and equipment, which cause considerable distress in patients during wound-closure procedures. Therefore, strategies that alleviate anxiety and pain through distraction is warranted.
Virtual reality
Virtual reality (VR) causes distraction through a three-dimensional computer-generated environment, where a user can become an active participant through a head-mounted device. 13 Virtual reality users can effectively divert their attention from the real world to the virtual world when they are immersed in a virtual environment.13,14 Besides, VR is safe, noninvasive, inexpensive, and convenient; does not require additional labor to operate; and allows repeatable distraction intervention.15,16 Therefore, it can easily provide intervention for patients in health care settings. The use of VR as a distraction strategy in clinical settings is attracting considerable interest.15–17 Virtual reality decreases anxiety and pain in various surgical procedures, including cesarean section,17 hand surgery15 and lipoma resection. 16 However, inconsistent results were found in plastic surgery,18 maxillofacial, dental and ear–nose–throat surgery19 and most studies have been conducted on children.18,19
To the best of our knowledge, no study has specifically focused on the effects of VR on anxiety and pain in Chinese adult patients undergoing laceration wound repair in an ED. Therefore, an empirical trial is needed. The Medical Research Council (MRC) framework suggests conducting a pilot and feasibility study to test the acceptability, feasibility, and potential effectiveness before conducting a full scale of randomized controlled trial (RCT) to prove its effectiveness. 20 The MRC framework was adopted in this study to guide the development and evaluation of VR use in the wound closure procedure in the ED. Based on the pilot RCT results, necessary changes can be made in future RCTs to better adapt to the clinical setting. The purpose of this study aimed to examine the preliminary effects of VR intervention on anxiety, pain, and physiological parameters in terms of blood pressure and pulse rate, satisfaction, and local anesthesia requirements in Chinese adult patients who undergoing suturing in Hong Kong EDs.
Theoretical framework of VR intervention
Despite using the MRC framework, this study was also guided by stress and coping theory, which has been extensively used in numerous studies.21,22 According to the theory, the wound-closure procedure acts as a stressor for the patients in this study because patients often experience anxiety and pain due to unexpected injury, unfamiliar environment, suturing equipment, and wound closure experience.23 Needle-related procedures, such as suturing, are the common causes of distress and pain. 24 When confronted with this stressor, patients prefer available measures, such as viewing videos via VR and receiving medication, to decrease their physiological discomfort and psychological distress. People confronted with a situation in which a stressor is unavoidable, they may distract themselves from the stressful situation to decrease their stress levels by using watching television, engaging in other pleasurable activities, exercising, or reading. 25 Given that VR acts as a distractor; it engages users in an immersive environment and interacts with a computer-generated environment that may divert their attention from the real world. 26 When patients are distracted by VR, they become less aware of their anxiety and pain. As a result, physiological parameters, such as blood pressure and pulse rate, decreases, medication is reduced and satisfaction increases.
Aim
In this study, we aimed to examine the preliminary effects of VR intervention on anxiety, pain, blood pressure, pulse rate, satisfaction, and local anesthesia requirements in Chinese adult patients undergoing wound-closure procedures in EDs in Hong Kong.
Hypotheses for testing
We evaluated three hypotheses: VR can alleviate anxiety and pain experienced by Chinese adult patients undergoing wound-closure procedures, the intervention can decrease extra local anesthesia requirements and physiological parameters during the procedures, and the intervention can significantly increase satisfaction during wound-closure procedures.
Methods
Design
This is a prospective parallel, RCT comprising an intervention group and a control group. The intervention group received standard care and VR intervention during the procedures, whereas the control group received only standard care. This design was guided by the CONSORT checklist. 27 The study was conducted from January 2023 to August 2023.
Setting
The study was conducted in a minor operation room of the ED of a regional public hospital in Hong Kong, China. This operation room is responsible for performing wide-awake local anesthesia surgery, particularly wound closure by suturing, incision and drainage, nail trephination, foreign body removal, and wound exploration.
Subjects and sample size
Since it is a pilot study, there are no fixed rules for sample size calculation. Hertzog recommended that at least thirty participants per intervention or control group is needed to obtain a direct estimate of a between-group effect size for subsequent power analysis. And considering a conservative estimated dropout rate of 20%, a sample size of 38 per group is required. 28 Therefore, the sample size for this pilot study was set at 80.
A convenience sample of Chinese adult patients with wound-closure procedure was recruited. Patients who (1) are conscious and oriented, (2) are Chinese adults (age over 18) with simple lacerated wounds, (3) can read and write Chinese, and (4) are hemodynamically stable, as evidenced by blood pressure of 90–140 mmHg systolic and 60–90 mmHg diastolic blood pressure, were considered qualified to participate in this study. Meanwhile, patients who (1) had visual, hearing, or cognitive impairment, (2) had a history of senile dementia, seizure disorder, motion sickness, and psychiatric disorders, (3) had infection or injury above the neck, and (4) were known to be on contact precaution were excluded.
Randomization and blinding
Eligible participants were randomly assigned to the intervention group (I) or the control group (C). Blocked randomization with a block size of eight was used in maintaining a good balance in sample size between the two groups throughout the subject recruitment period. Computer-generated random codes were prepared in advance, and serially numbered opaque sealed envelopes were used and kept by a person not involved in the study. The envelope was opened sequentially for each consented participant who had completed the baseline data collection. A research assistant (RA) and eligible patients were blinded to group allocation until baseline data collection was completed. Given the nature of the intervention, neither the patients nor RA was blinded to the intervention.
Control: Standard care
In standard care, emergency nurse performed wound-closure procedure after local anesthesia and wound exploration in a minor operator room. Patients had the opportunity to request additional local anesthesia during the procedure. All simple lacerated wounds were performed by emergency nurses who completed the suturing courses. A simple lacerated wound refers to a break in the skin that does not involve the nerves, tendons, arteries, veins, and bones. 29
Intervention: VR
In addition to standard care, VR intervention was offered to patients before local anesthesia and during wound closure. During the intervention, patients experienced a sense of immersion through the device delivering the VR sounds and images. VIVA Focus goggles were used, which are commercially available. The volume of the video was controlled by patients. After the procedure, the VR goggles were removed immediately by the RA, and a dressing was applied and fixated on sutured wounds. To minimize the risk of contact infection, the patients wore disposable surgical caps and eye masks.
Given that no previous works related to VR has been conducted on Chinese adult patients during wound-closure procedures in the EDs of Hong Kong, we selected VR videos according to the preferences of a panel (three adult patients with wound closure by suturing and suggestions from three professional of health care providers in the ED). The selected five VR videos included landscape, ocean, travel, sport, and animal videos with background music and English subtitle. These three adult patients were not included in the final sample. Given that not all patients in Hong Kong understood English well, videos with English subtitles would not be selected, such as travel and sport videos.
These videos were chosen due to distraction and relaxation purposes, and their common use in previous studies, and suitability for the duration of the wound-closure procedure.15,17
Measures
Data were collected at baseline (T0), 10 min after starting the suturing (T1) and 5 min after the completion of wound closure (T2) for all participants. Any adverse side effects of VR such as headache, nausea, and dizziness were also recorded throughout the procedure. The primary and secondary outcomes are listed below.
Primary outcome
Anxiety: This outcome was measured using the Chinese version of the State Trait Anxiety Inventory-Form Y1 for adults (CSTAI-Form Y1), which includes 20 items; each item was rated on a four-point Likert scale, and total scores ranged from 20 to 80. High scores indicated high level of anxiety. The CSTAI-Form Y1 was used in this study because it evaluates the current feeling of anxiety that measures subjective feelings of tension, nervousness, apprehension, and worry.30,31 The Chinese version of STAI was validated in Hong Kong and was found to have a high degree of internal consistency (alpha = 0.9).32,33
Secondary outcomes
Pain Intensity, satisfaction with pain management and procedure: Visual analog scales (VAS) were used to measure patients’ pain intensity and satisfaction with pain management and service. Visual analog scale is a 10 cm-long horizontal line with verbal descriptors (word anchors) at each end and the respondent marks on the line that represents individual perception of the current state. The score was obtained by measuring the distance (centimeter) from point zero to the marked point. 34 The VAS is a valid tool for measuring psychological and health variables, such as pain and satisfaction, which are widely used in clinical studies.35,36
Additional local anesthesia use: Additional local anesthesia requirements during the procedure were retrieved from the procedure nurse and medical records.
Physiological parameters: Physiological parameters (pulse rate and systolic and diastolic blood pressures) were measured at all the three time points T0, T1 and T2 by a standard multiple functions monitor. This monitor was available at the study institution. Blood pressure and pulse rate are considered as an objective measurement that can be used as proxy measures of physiological response to anxiety. 37
Two further questions were used to ascertain participants’ video preference and opinions of the VR intervention.
Demographic and clinical data
Demographic and clinical characteristics of the patients included age, gender and education level, previous local anesthesia experience, regular follow-up, and medication taking and previous VR experience.
Procedure and data collection
The RA screened all the patients for eligibility. Patient who met the inclusion criteria were invited to participate in the study. The RA had emergency care experience and received training to conduct the study. Patients who were deemed eligible were asked to sign consent forms. Before randomization, the RA collected the baseline data (demographic data, anxiety, blood pressure, pulse rate, and pain score) of the participants. Randomization was based on the prior prepared random group allocation sequence. Patients in the intervention group were required to select a VR video. The RA then provided them with VR goggles to view the selected video before local anesthesia. The blood pressure and pulse rate were recorded at 10 min after starting the suturing. Any adverse side effects of VR such as headache, nausea, and dizziness were also recorded throughout the procedure. The VR equipment was removed by RA when the dressing was applied and fixated on the sutured wound. Five minutes after wound closure, the pain and anxiety levels, blood pressure, pulse rate, and satisfaction with pain management and procedure were recorded by participants through self-reports.
Ethical considerations
Ethics approval was obtained from the clinical research ethical committee of New Territories West Cluster, Hospital Authority, Hong Kong. The trial was registered in Clinical Trials.Gov with registration number NCT05796076 on March 21, 2023. All participants had been well informed about the purposes and procedures of the study before signing written informed consent forms. Participant were informed of their freedom to withdraw at any time without suffering negative consequences. Confidentiality and anonymity were assured during the study.
Statistical analysis
Data were analyzed using SPSS version 26 (IBM Corp, Armonk, New York), and the intention-to-treat principle was applied. The baseline characteristics of the groups was compared using a chi-square for categorical variables and independent t-test for continuous variables, and the comparability of the groups was investigated by randomization. Confounding variables were considered in subsequent analyses. To examine the effectiveness of the VR intervention, we compared its outcomes with the outcomes of the control group by using Generalized Estimation Equation (GEE) models, which were selected because they can accommodate missing data caused by dropouts; they can also accommodate data missing at random without needing to impute missing data and are thus particularly suitable for an ITT analysis. 38 Given the potential confounders may be identified in between group difference at baseline, we conducted the GEE analysis while controlling for these confounders if any.
The between-group Cohen's d was calculated for the estimation of the effect sizes of the VR group as compared with the control group on each outcome measure. Two-tail tests were used with a significance level of .05.
Result
A total of 107 patients were assessed for eligibility, and 27 were excluded: 12 patients did not meet the eligibility criteria and 15 patients declined to participate in the study after the purpose of study was explained. A total of 80 patients underwent randomization: 40 patients in the VR group and 40 in the control group (Figure 1). The participants’ mean age was 41.13 (SD, 11.69) years for the intervention group and 47.08 (SD, 14.15) years for the control group. Males comprised 57.5% (n = 23) of the VR group and 67.5% (n = 27) of the control group. The attrition rates at T1 and T2 for the VR group and control group, respectively, were 5% (n = 2). The total attrition rate for all participants was 5% at T2 because patients with tendon cuts did not complete the wound-closure procedures. Most participants had received secondary education or above (82.5%) and had no personal history of local anesthesia surgery (52.5%) and had no previous used VR technology (88.8%), and over three quarters of the patients had no regular follow-up (78.8%) and medication taking (81.3%). No statistically significant difference in sociodemographic characteristics between the two groups at baseline (Table 1).
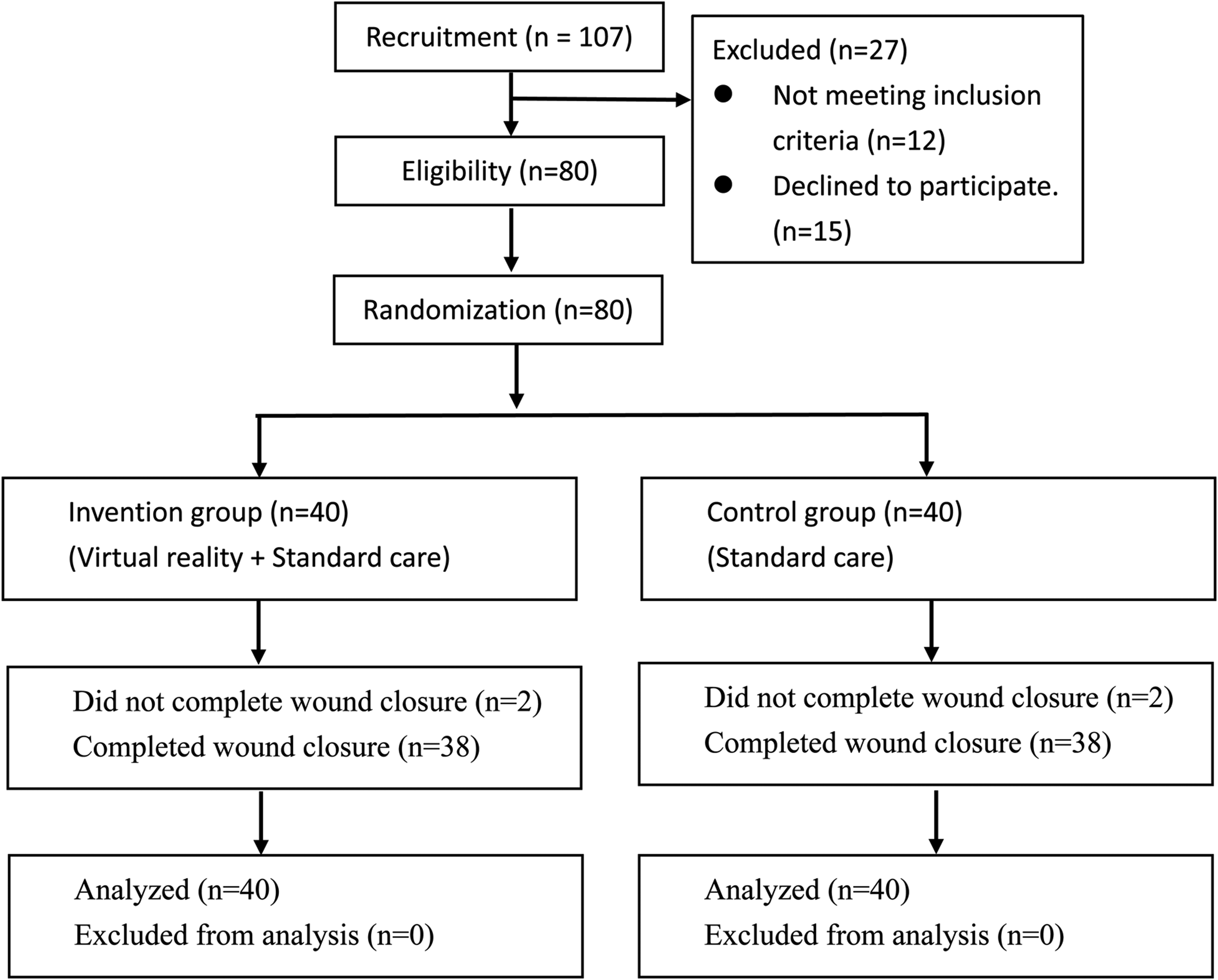
Study flowchart.
Characteristics of the participants.

Notes: Categorical variables were compared between the two groups using Chi-square test.
Their CSTAI-Form Y1 scores were 49.68 (SD 12.22). The patients in the VR group reported moderate pain (5.37; SD 2.01), compared with the control group (3.61; SD 2.43; p < 0.01). Their pulse rates were 72.06 (SD 10.73) beat per minute, and their mean systolic blood pressure and diastolic blood pressure were 130.46 mmHg (SD 8.42) and 78.41 mmHg (SD 8.40), respectively. No statistically significant differences in baseline physical and psychological characteristics were observed between the groups, in contrast to the pain scores (Table 2).
Baseline physiological and psychological characteristics of the participants.
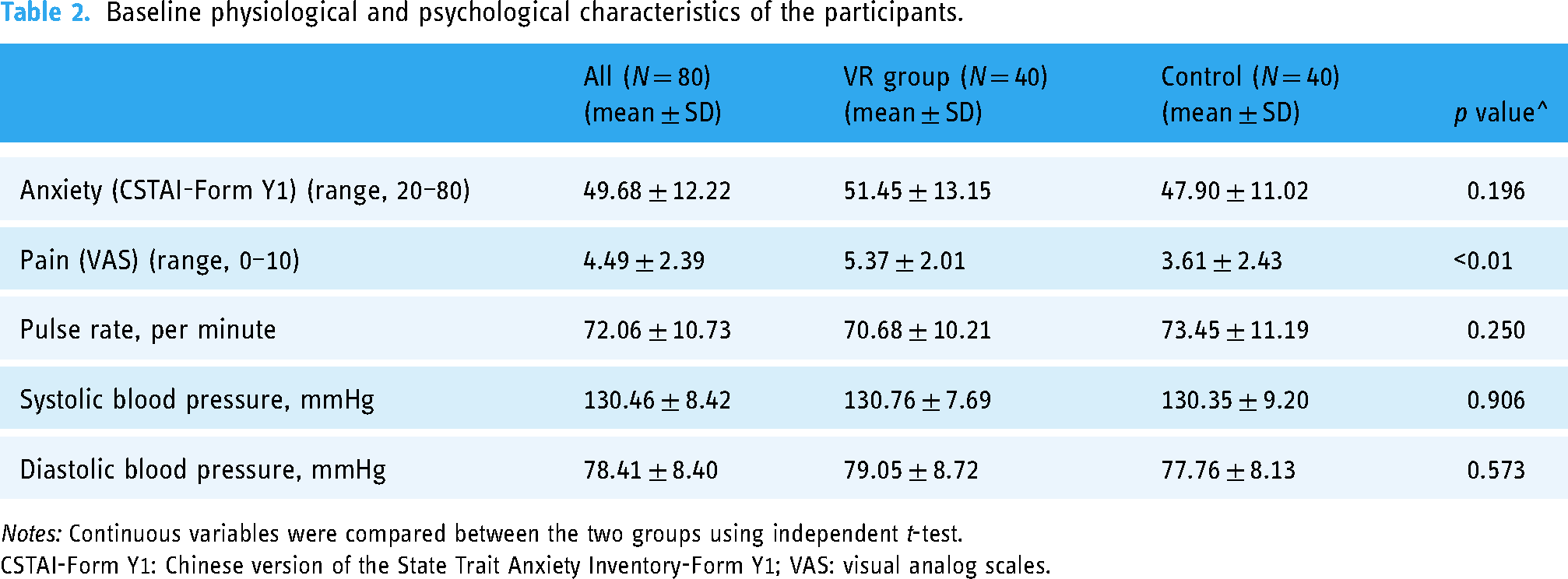
Notes: Continuous variables were compared between the two groups using independent t-test.
CSTAI-Form Y1: Chinese version of the State Trait Anxiety Inventory-Form Y1; VAS: visual analog scales.
Table 3 summarizes the mean, the SD of the outcomes and the effect size of the GEE results of the outcomes (anxiety levels, pain level, systolic blood pressure, diastolic blood pressure, and pulse rate) between the groups. The VR group showed better performance and had a large effect size, which was indicated by greater decreases in anxiety level (Cohen's d, −1.76; p < 0.001), pain level (Cohen's d, −3.32; p < 0.001), systolic blood pressure (Cohen's d, −0.91; p < 0.001), diastolic blood pressure (Cohen's d −1.14; p < 0.001), although there was a medium effect size on the reduction in pulse rate (Cohen's d, −0.66; p < 0.003). After the procedures, the VR group showed greater decrease in systolic blood pressure, with a Cohen's d of −1.06 (p < 0.001). The VR group showed significant decrease in diastolic blood pressure (Cohen's d, −0.58; p < 0.008) and pulse rate (Cohen's d, −0.54; p < 0.013).
Results of generalized estimated equation (GEE) models for the comparison of the repeated measures outcome variables between the two groups.

Notes: T0 = Before the suturing procedure; T1 = 10 min after starting the suturing; T2 = 5 min after the completion of the procedure.
GEE: generalized estimating equations; CI: confidence interval.
* p < 0.05; ** p < 0.01.
Control confounders: age, baseline pain level.
The VR intervention significantly increased the level of satisfaction with pain management (p = 0.019) and service (p = 0.002). Most participants (86.8%, n = 33) in the VR group and 89.5% (n = 34) in the control group indicated that they would prefer using VR in reducing anxiety in future surgical procedures. The reduction in local anesthesia was significantly greater for the VR group during wound closure (0% vs. 15.8%; Table 4).
Outcome measures between the virtual reality and control groups.

Notes: Continuous and categorical variables were compared between the two groups using independent t-test and chi-square test, respectively.
VR: virtual reality; LA: local anesthesia.
Each participant in this study had a simple laceration wound, the wound length was approximately 1–3 cm, and most of them found in the lower limb. The duration of the wound-closure procedure was approximately 30 min. Only one patient reported mild dizziness after using VR, but the patient was able to complete the suturing procedure.
Discussion
To the best of our knowledge, this study was the first to use a RCT to examine the effects of VR on anxiety, pain, physiological parameters, local anesthesia requirements, satisfaction with pain management, and service satisfaction in Chinese adult patients undergoing wound-closure procedures in the ED.
The results showed that the patients experienced moderate anxiety before the procedure. This result is congruent with the results of a previous study. 17 Negative feelings not only cause negative physiological manifestations but can also increase the complications of medication administration. 39 Thus, psychological assessment and VR before suturing should be considered.
The patients in the VR group demonstrated a significantly greater reduction in anxiety level. The results were consistent with previous studies suggesting that VR is an effective intervention for reducing anxiety in adult patients during surgery.15–17 A possible explanation for this finding is that VR is a form of distraction that shifts patients’ attention from the real world to the virtual world. It alters their perception of reality and tasks their brain to focus more on their virtual world rather than wound-closure procedures.13,14,16 And VR headsets block a patient's external view of the procedure, particularly the medical equipment, health care personnel, and their sounds, thereby increasing the level of immersion and diverting the attention of the patient from stress stimuli.
Moreover, the results showed that VR significantly reduced pain in patients in the VR group, consistent with those of previous study demonstrating that VR is effective in reducing pain. 16 A possible explanation for these results is that VR changes the way a patient interprets incoming pain signals and thereby reducing the amount of pain-related brain activity. 40
Significant differences between the two groups were found in terms of systolic and diastolic blood pressure, consistent with the results of a previous VR study on patients with septorhinoplasty. 41 Virtual reality facilitated hemodynamic stabilization during surgery because of its stress-reducing mechanism. 42
Patients in the VR group showed significantly greater reduction in pulse rates unlike the patients examined a previous study, in which intervention patients exhibited no significant reduction in pulse rates compared with control patients. 43 The discrepant results may be attributed to the difference between the procedures of limb suture and plastic surgery.
The VR group showed significantly higher satisfaction scores regarding pain management and service. Virtual reality is a highly effective distractor and improves patient satisfaction.17,44 Although patients viewed different type of videos, they consistently demonstrated increased levels of satisfaction with pain management and service. This finding supported the idea that VR can increase patient satisfaction.
In some studies, the need for extra local anesthesia consumption was reduced in VR groups compared with control groups, although no statistically significant difference was found between the groups.18,44 This study found that patients in the VR group showed significant decrease in local anesthesia during wound closure. Inconsistent results may be due to the difference in the timing of VR use. Nevertheless, VR would prevent the use of extra local anesthesia.
Although one patient reported mild dizziness after using the VR device, no adverse events were found throughout the whole study, and most of the patients (88.2%) would like to have VR experience in the event of new surgery. Virtual reality is a simple and safe distraction technique that can be used by everyone and everywhere; its implementation can be effective in many surgery centers worldwide. 44
Regarding feasibility of this study, the recruitment rate was high and attrition rate was low in this study, indicating that the patients who were invited to participate in this study needed such an intervention and were excited about using a modern technology. However, only the VR group used VR; the participants in the control group showed eagerness to use VR in their future surgical procedures.
In summary, the study demonstrated a moderate-to-large effect and considerable reduction in anxiety, pain, systolic blood pressure, and diastolic blood pressure in the VR group. The group also showed significant decrease in pulse rates and need for additional local anesthesia and improved patient satisfaction.
Study limitations
This study had several limitations. First, the intervention's effectiveness was evaluated only in a single setting. The experience of patients in other settings might be different. Thus, the generalizability of the study finding may be limited. Second, the Hawthorne effect might have been present in the VR group, which could have affected the results. Third, since we collected subjective data on anxiety and pain perceived by the patients, measurement bias may be possible. Forth, the suturing nurses were not blinded to group assignment because they saw VR goggles for the intervention group. This situation may have affected their decision to increase or decrease local anesthesia. Finally, the patients were required to recall the pain they felt during the procedure, which may have a risk of bias in recall.
Future studies should be conducted in a large-scale multicenter. Procedure time, comments from nurses and cost of the intervention should be considered in determining cost effectiveness.
Implications
This pilot study provides preliminary evidence and insight for future studies related to VR as an intervention or support for adult patients undergoing wound-closure procedures. The findings of this study indicated that VR can effectively alleviate anxiety, pain, blood pressure, pulse rate, and local anesthesia requirement and improve satisfaction in adult patients who are undergoing wound-closure procedures. Virtual reality can be considered a safety and noninvasive adjunctive treatment to manage anxiety and pain in these patients in clinical settings.
Conclusion
This study was the first to examine the effects of VR among Chinese adult patient undergoing wound closure by suturing in EDs in Hong Kong. This pilot study provides insight into the use of VR and the direction of future studies. It may effectively improve psychological and physiological outcomes in adult patients during wound-closure procedures in EDs. The findings suggest that VR significantly reduce anxiety, pain, physiological parameters, and local anesthesia use and enhance patient's satisfaction with service and pain management in patients undergoing wound closure by suturing. Thus, this safe, easy-to-use, and nonpharmacological method should be used in routine care and in wound-closure procedures.
Footnotes
Acknowledgements
The authors would like to thank the Chief of Service for his permission to conduct this study in the ED of Tuen Mun Hospital. Special thanks to all nurses and patients who offered support or participated in this study. Special thanks to Dr Doris Leung for the statistical consultation and support.
Contributorship
SYK designed and implemented the study, data analysis, and drafted the manuscript; EW conducted the analysis, interpreted the results, and revised the manuscript; the others support the implementation of the study and reviewing the manuscript. All authors reviewed the final manuscript and gave their consents.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NTWC Clinical Research Governance Committee (CRGC). The CRGC played no role in the design of the study, data collection, data analysis and interpretation, writing of the manuscript, or the decision to submit the manuscript for publication.
Guarantor
EMW.