
Abstract
Background
Undergraduate students are particularly vulnerable to mental health problems due to academic pressure, financial concerns, and interpersonal stressors. Nature-based virtual reality (VR) technologies, which replicate natural settings, may offer psychological benefits by compensating for limited access to real-world natural environments in urban contexts.
Purpose
This study aimed to evaluate the effectiveness of a nature-based VR relaxation program in improving mental health and sleep outcomes among Korean undergraduate students.
Method
Participants from five Korean universities were randomly assigned to one of three groups: VR relaxation, progressive muscle relaxation (PMR), or wait-list control. Self-reported measures of depression, anxiety, perceived stress, and sleep patterns were collected at baseline, post-intervention, and follow-up. Objective sleep efficiency was assessed using wrist-worn actigraphy devices. Data were analyzed using generalized estimating equations to examine changes over time and between groups.
Results
A total of 41 participants completed the study. The VR intervention group showed significant reductions in perceived stress levels (p = .001) and improvements in subjective sleep patterns (p = .046), with these effects sustained at follow-up. Notably, sleep efficiency measured via actigraphy improved significantly in the PMR group compared to the other groups (p = .033).
Conclusions
A nature-based VR relaxation program appears to be an effective digital intervention for reducing stress and enhancing subjective sleep quality among undergraduate students. These findings highlight the potential of nature-simulating digital environments to support mental health and wellness in settings with limited access to natural spaces.
Introduction
As undergraduate students transition from late adolescence to early adulthood, they encounter various challenges related to academics, employment, finances, and interpersonal relationships. 1 These stressors contribute to increasing rates of mental health issues such as depression, anxiety, behavioral addictions, substance use, and sleep disturbances.2,3 A mental health survey conducted at a South Korean university among 1242 students found that approximately 60% reported experiencing depressive symptoms. Nevertheless, only 23% had accessed the university's mental health services, underscoring a considerable gap between mental health needs and actual service utilization. 4 This highlights the urgent need for accessible, stigma-free, and scalable interventions tailored to the unique needs of undergraduate students who are vulnerable to mental health problems.
Relaxation-based therapies are widely used to alleviate negative emotional states and enhance sleep quality. These behavioral interventions aim to activate the parasympathetic nervous system, reduce physiological tension, and foster psychological comfort.5–7 A variety of relaxation techniques have been demonstrated to be effective, including abdominal breathing, yoga, progressive muscle relaxation (PMR), massage therapy, and music-based interventions. 8 PMR systematically induces deep relaxation by alternating muscle tension and release. 7 This technique is based on the principle that muscle tension arises as a physiological response to cognitive stimulation. Notably, PMR shares similarities with virtual reality (VR)-based relaxation programs, as both function as self-management tools that can be easily integrated into daily life without requiring a specific environment or schedule. 8
As relaxation therapy gains traction as a mental health intervention, VR has emerged as a promising modality for delivering immersive relaxation experiences.9,10 Initially developed in the 1980s with the advent of head-mounted displays (HMDs) and interactive controllers, VR has since evolved into a multimodal, interactive, three-dimensional computer-generated environment that provides tactile, positional, and multisensory feedback. 11 These features enable users to engage in lifelike simulations that can induce relaxation and reduce psychological distress. VR has been shown to be highly effective in reducing stress and anxiety by modulating physiological functions, including blood flow, heart rate, sleep patterns, and muscle tension, through visual and auditory feedback. 9 In particular, immersive VR environments that simulate natural scenes—such as mountains, skies, underwater scenes, and animals—have been found to enhance mental well-being and promote emotional regulation.12–15 These interventions may be especially beneficial for individuals with limited access to nature due to physical disabilities, time constraints, or public health restrictions such as those experienced during the COVID-19 pandemic. Emerging evidence suggests that immersive VR experiences using HMDs are more effective in promoting relaxation and positive affect compared to non-immersive, screen-based alternatives. 16 Veling et al. 17 developed an immersive VR relaxation program that provides 360-degree views of natural environments and demonstrated its effectiveness in reducing negative emotions among individuals with psychiatric disorders. Moreover, while immersive VR relaxation programs have also shown promise in promoting relaxation among the general population, further research is needed to strengthen the evidence supporting their effectiveness. 10
Most prior studies evaluating immersive VR relaxation interventions have relied predominantly on self-report questionnaires. While such subjective assessments offer valuable insight into participants’ perceived experiences, they are also susceptible to recall bias and other forms of response distortion.18,19 To address these limitations and enhance the robustness of the findings, incorporating objective physiological measurements can provide a more comprehensive understanding of intervention effects. 18 Therefore, this study aimed to evaluate the effectiveness of an immersive VR relaxation program, designed to replicate natural environments, on mental health and sleep outcomes among undergraduate students. To improve measurement accuracy, both self-report tools and actigraphy were employed, with actigraphy being a validated method for assessing sleep and wake cycles.
Methods
Trial information
This study was registered with the Clinical Research Information Service (CRIS) of Republic of Korea (KCT0009185), which is a member of the WHO International Clinical Trials Registry Platform (ICTRP), on 20 February 2024.
Study design and participants
This study employed a randomized controlled design with repeated measures across three groups. Participants were allocated using simple randomization with a 1:1:1 ratio. The required sample size was calculated using G*Power version 3.1.9.7. Although a prior meta-analysis reported large effect sizes for VR-based interventions targeting anxiety (Hedge's g = 0.79) and depression (g = 0.73), 20 a moderate effect size was adopted for this study. Based on an assumed effect size of 0.25, a power of 0.80, a significance level of 0.05, three measurement time points, and a correlation of 0.5 among repeated measures, a total sample size of 45 participants (15 per group) was determined to be sufficient for a repeated-measures ANOVA. This calculation also accounted for an anticipated dropout rate of 20%.
Participants were recruited from five universities located in the metropolitan area of the Republic of Korea. These universities were selected based on the research team's ability to access each university's online community platform, through which recruitment announcements could be directly posted. Eligible participants met the following criteria: (1) currently enrolled as an undergraduate student in Korea; (2) able to understand and operate the VR program and equipment with moderator guidance; (3) capable of sitting in a chair with armrests and back support for at least 20 min without physical discomfort; and (4) possessing sufficient visual and auditory capacity to engage with the VR content. However, individuals were excluded if they had a current diagnosis of a mood disorder, anxiety disorder, or sleep disorder and were receiving psychiatric medication or psychotherapy. This study was reported in accordance with the CONSORT checklist, as detailed in Supplementary File 1.
Procedure
Those who consented to participate were randomly assigned to one of three groups: the immersive VR relaxation group (VR), the attention control group (AC), or the wait-list control group (WLC). Randomization was performed by the first author using Excel's RAND function, and identification numbers were assigned to each participant. In accordance with the study protocol, participants completed assessments at three time points: pre-intervention (pre-test), immediately post-intervention (post-test), and at a 4-week follow-up (follow-up test).
Participants in the VR group received the immersive VR-based relaxation program in a simulation room located at the researchers’ affiliated institution. They were instructed to attend six sessions over a 2-week period, excluding weekends, with at least 1 day between sessions. Each session consisted of 20 min of engagement with the VR-based relaxation program. To reduce attrition, participants received reminder messages the day before each scheduled session.
The AC group received PMR training as an alternative intervention. Participants were individually instructed by the research team and then asked to perform PMR at home, following a structured manual and video tutorial. They were instructed to complete six sessions within the two-week period.
The WLC group did not receive any intervention during the study period. However, upon completion of all study procedures, participants in this group were granted access to the same VR relaxation program provided to the VR group.
Adherence to the intervention was monitored differently across groups: For the VR group, session participation time was directly measured and logged by the research team. For the AC group, participants were asked to self-report their session completion.
Intervention
Virtual reality relaxation group: nature-based virtual reality relaxation program (vRelax)
VRelax (version V3) is a scientifically validated VR-based relaxation program developed by Veling et al. 17 for individuals experiencing mental or physical distress. The program provides immersive virtual environments depicting a range of natural scenes, such as beaches, coral reefs with tropical fish, dolphins, rivers, night skies, meadows with animals, alpine landscapes, and ocean cliffs. Users can select preferred environments and engage in interactive elements designed to promote relaxation. The program includes two main features: the Overview mode, which allows 360-degree exploration of natural environments, and the Themes mode, which enables users to navigate between different spaces and engage in interactive activities by moving their head. 17 In this study, the Overview mode was used during sessions 1, 3, and 5, while the Themes mode was used in sessions 2 and 4. For the sixth session, participants were allowed to choose either mode based on personal preference. All VR sessions were delivered using a Meta Quest 2, providing fully immersive experience in a controlled simulation environment. A screenshot of the nature-based virtual environments implemented in the VRelax program is provided in Supplementary File 2.
Attention control group: progressive muscle relaxation
The AC group received PMR as a relaxation-based intervention. PMR is a technique designed to alleviate tension and anxiety by systematically tensing and relaxing skeletal muscles while focusing on controlled breathing. 21 Participants were individually trained in the procedure by the research team and were provided with a standardized manual and instructional video for home-based practice. To promote adherence, participants worked with the researchers to develop a personalized practice schedule. They also received reminder messages prior to each scheduled session and were asked to confirm the completion of their exercises to ensure compliance with the intervention protocol.
Measurement
Depression, anxiety
Depression and anxiety were assessed using the Korean version of the Patient-Reported Outcome Measurement Information System-Short Form (K-PROMIS), which was culturally adapted and validated by Choi et al. 22 This instrument is derived from the PROMIS Short Form, developed by the National Institutes of Health. 23 The K-PROMIS assesses the emotional distress subdomain of mental health within the PROMIS framework and includes eight items each for depression and anxiety, rated on a five-point Likert scale. Raw scores are converted to standardized T-scores with a mean of 50 and a standard deviation of 10, where higher scores indicate greater symptom severity. In this study, the K-PROMIS demonstrated excellent internal consistency, with Cronbach's alpha coefficients of 0.94 for depression and 0.91 for anxiety at post-test.
Perceived stress levels
Perceived stress levels were measured using the Korean version of the Perceived Stress Scale (K-PSS), which was originally developed by Cohen et al. 24 and later translated and validated for Korean populations by Park and Seo. 25 The instrument consists of 10 items divided into two subscales: Negative Perceptions (5 items) and Positive Perceptions (5 items), with the latter being reverse-scored. All items are rated on a five-point Likert scale, and higher total scores indicate greater levels of perceived stress. In the present study, the K-PSS demonstrated good internal consistency at post-test, with a Cronbach's alpha of 0.85.
Subjective sleep patterns
Subjective sleep patterns were assessed using the General Sleep Disturbance Scale (GSDS), originally developed by Lee 26 and adapted for Korean populations by Choi et al. 27 The GSDS evaluates sleep disturbances over the past week and consists of 21 items across six subscales: sleep onset, sleep maintenance, sleep quality, sleep quantity, fatigue and alertness at work, and use of substances to induce sleep. Higher total scores reflect greater levels of sleep disturbance. In this study, the GSDS demonstrated good internal consistency at post-test, with a Cronbach's alpha of 0.85.
Objective sleep patterns
Objective sleep patterns were assessed using a wrist-worn actigraphy device (ActiGraph wGT3X-BT accelerometer), which detects sleep and wake states based on movement patterns. The device also includes ambient light sensors, allowing for analysis of environmental context in relation to sleep activity and enabling objective measurement of sleep parameters. 28 Wearing the device on the nondominant wrist is considered a reliable method for monitoring sleep and activity levels. 29 A 3-day monitoring period was chosen based on prior research indicating that compliance tends to decline when actigraphy is worn for more than 7 days. 30
In this study, participants wore the actigraphy device on their nondominant wrist for 3 days before the intervention and 3 days after the intervention to measure total sleep duration and sleep efficiency. Sleep efficiency was calculated as the percentage of total sleep duration relative to the total time in bed, using the formula: (total sleep duration / time in bed) × 100. 31 To supplement the objective data, participants also recorded their self-reported bedtimes and wake times throughout the monitoring period.
Statistical analysis
Data were analyzed using SPSS 26.0 and R 4.4.1. Chi-square tests were conducted to assess the homogeneity of general characteristics and outcome variables among the three groups: VR, AC, and WLC. To evaluate the longitudinal effects of the intervention, generalized estimating equations (GEEs) were employed. GEE allows for the assessment of interaction effects between groups and measurement periods by analyzing differences in changes in outcome variables over time. This method is robust to violations of normality assumptions and provides reliable population-level estimates, making it well-suited for repeated-measures data. 32 As a significant difference in grade level was observed among groups at baseline, it was included as a covariate in the GEE models to control for its potential confounding effect. When the GEE analysis conducted in SPSS revealed a statistically significant group-by-time interaction, post-hoc pairwise comparisons were subsequently performed using the “emmeans” package in R to explore differences between groups. Tukey's method was applied to adjust for multiple comparisons. In addition, the usability of the VR intervention was assessed by calculating the mean and standard deviation for each item.
Ethical considerations
Ethical approval for this study was obtained from the Institutional Review Board of the authors’ institution (IRB No. 2305/004-009). Prior to participation, all participants received detailed information about the study objectives and procedures and provided informed consent. They were informed of their right to withdraw at any time without any disadvantages. As compensation for participation, each participant received a voucher. To ensure confidentiality, all collected data were anonymized prior to analysis.
Results
General characteristics of the participants
A total of 45 undergraduate students were recruited, and enrollment was closed upon reaching the target sample size. All participants provided informed consent. Prior to baseline assessment, four participants (two in the VR group and two in the WLC group) withdrew from the study due to lack of time (n = 2), illness (n = 1), or travel commitments (n = 1). The final sample comprised 41 participants who completed the intervention and follow-up assessments in the VR, AC, and WLC groups. Retention at the 4-week follow-up was 100%. All participants in both the VR and AC groups completed the prescribed number of sessions. A CONSORT flow diagram illustrating participant progression is provided in Figure 1.
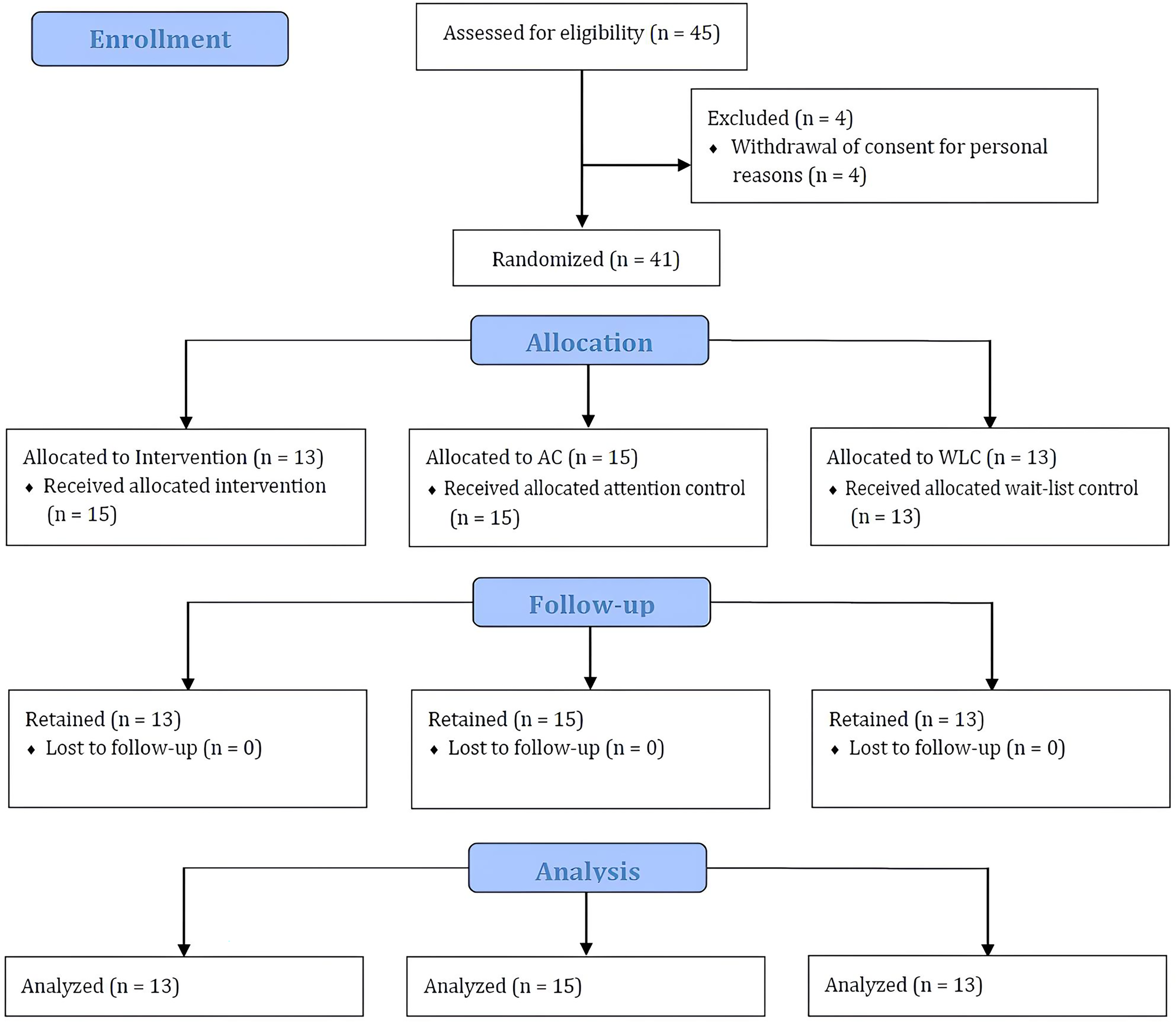
Flow diagram of participants through each stage of randomized controlled trial.
The mean age of participants was 21.34 years, with the majority being juniors (87.8%). The sample was predominantly female (73.2%), and more than half (58.5%) lived with their families. A total of 29 participants (70.7%) reported no prior experience with VR. General characteristics were comparable across the three groups, except for grade level. No significant differences were observed in pre-test scores for depression, anxiety, perceived stress levels, or subjective sleep patterns, indicating adequate group homogeneity (Table 1).
Homogeneity test of general characteristics and outcome variables among groups.
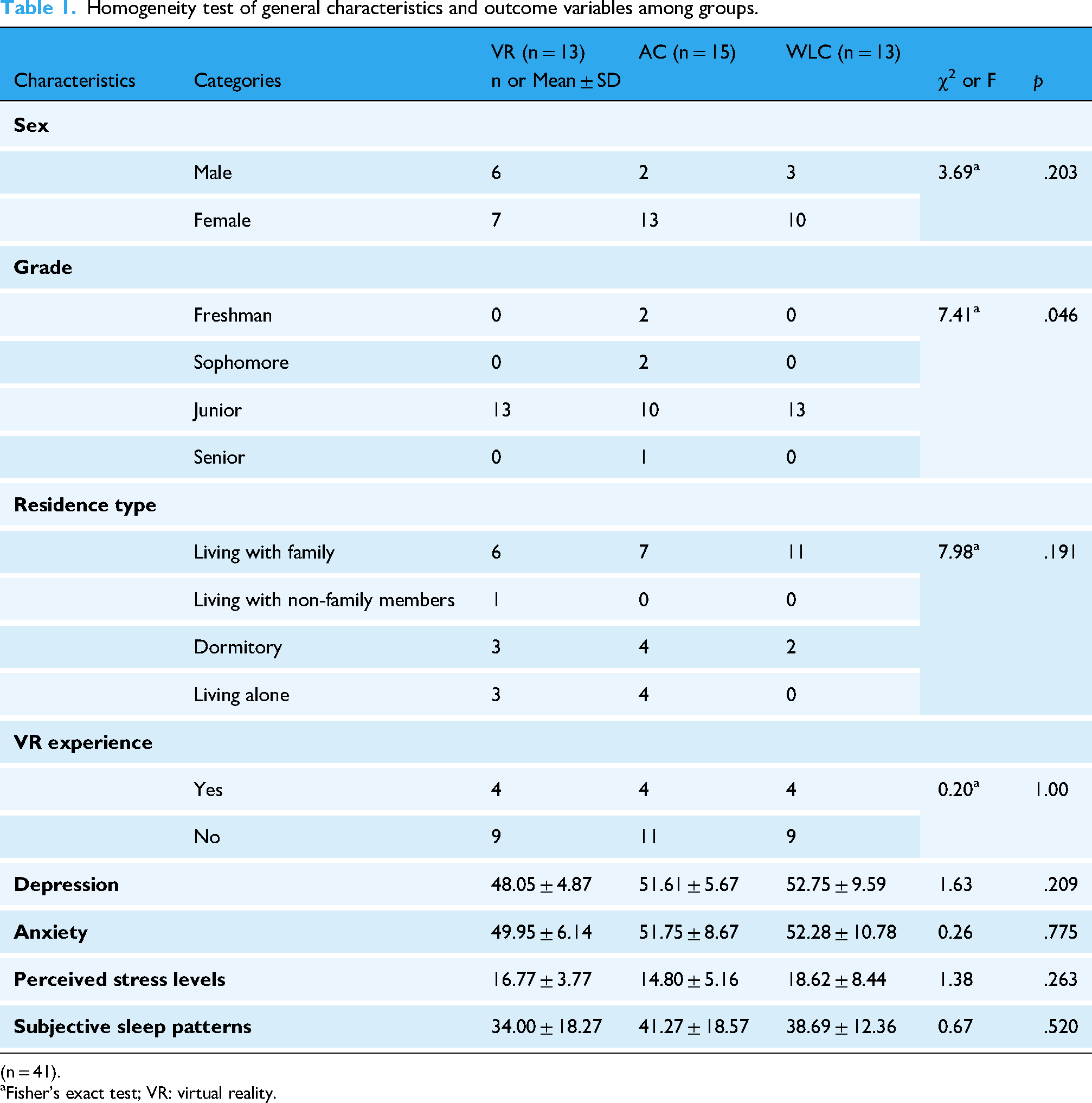
(n = 41).
Fisher's exact test; VR: virtual reality.
Efficacy of the virtual reality-based relaxation program
GEE analyses, adjusted for grade level, revealed significant group-by-time interaction effects for perceived stress levels (p = .001) and subjective sleep patterns (p = .046) (Table 2). The VR group demonstrated greater improvements in both outcomes over time compared to the AC and WLC groups. Post-hoc pairwise comparisons following the significant group-by-time interaction in the GEE analysis indicated that, at the post-test time point, the VR group exhibited significantly lower perceived stress levels compared to the WLC group (estimate = −9.35, SE = 1.85, 95% CI [−13.69, −5.00], p < .001), and marginally lower levels compared to the AC group (estimate = −3.74, SE = 1.65, 95% CI [−7.66, 0.18], p = .065). In terms of subjective sleep patterns, the VR group reported significantly greater improvement than the WLC group (estimate = −15.43, SE = 5.14, 95% CI [−28.2, −2.60], p = .014). Among participants on the VR group, the pre-to-post change in perceived stress levels yielded a large effect size (Cohen's d = −1.55), whereas the change in subjective sleep patterns showed a moderate effect size (Cohen's d = −0.75).
Comparison of outcome variables across groups over time.

(n = 41); VR: virtual reality.
Perceived stress levels in the VR group significantly decreased from pre-test to post-test (estimate = 6.31, SE = 1.24, 95% CI [3.85, 8.77], p < .001) and remained significantly lower at follow-up test compared to pre-test (estimate = 5.62, SE = 0.98, 95% CI [3.67, 7.56], p < .001). No significant difference was observed between post-test and follow-up test (estimate = −0.69, SE = 0.97, 95% CI [−2.61, 1.23], p = .477), suggesting that the intervention effects were sustained over 4 weeks. In contrast, no significant changes in stress levels were found in either the AC or WLC groups across time points (Figure 2).
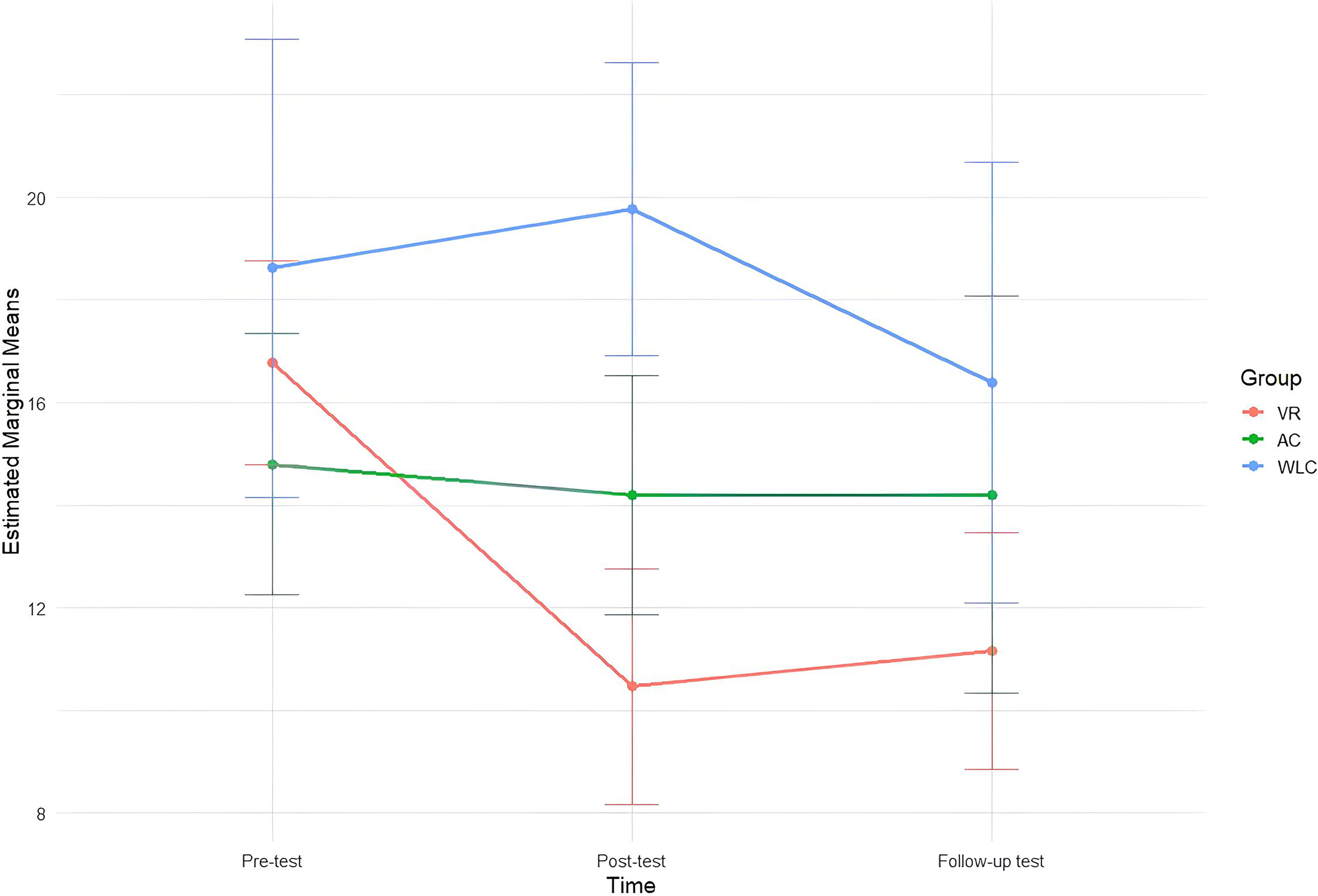
Estimated marginal means of perceived stress levels across time points.
In the VR group, subjective sleep patterns significantly improved from pre-test to post-test (estimate = 12.94, SE = 3.26, 95% CI [6.46, 19.38], p = .001) and from pre-test to follow-up test (estimate = 8.54, SE = 4.04, 95% CI [0.53, 16.55], p = .037). The difference between post-test and follow-up test was not statistically significant (estimate = −4.38, SE = 2.35, 95% CI [−9.03, 0.27], p = .064), indicating that the improvement was largely maintained at follow-up. No significant time effects were observed in the AC or WLC groups regarding sleep outcomes (Figure 3).
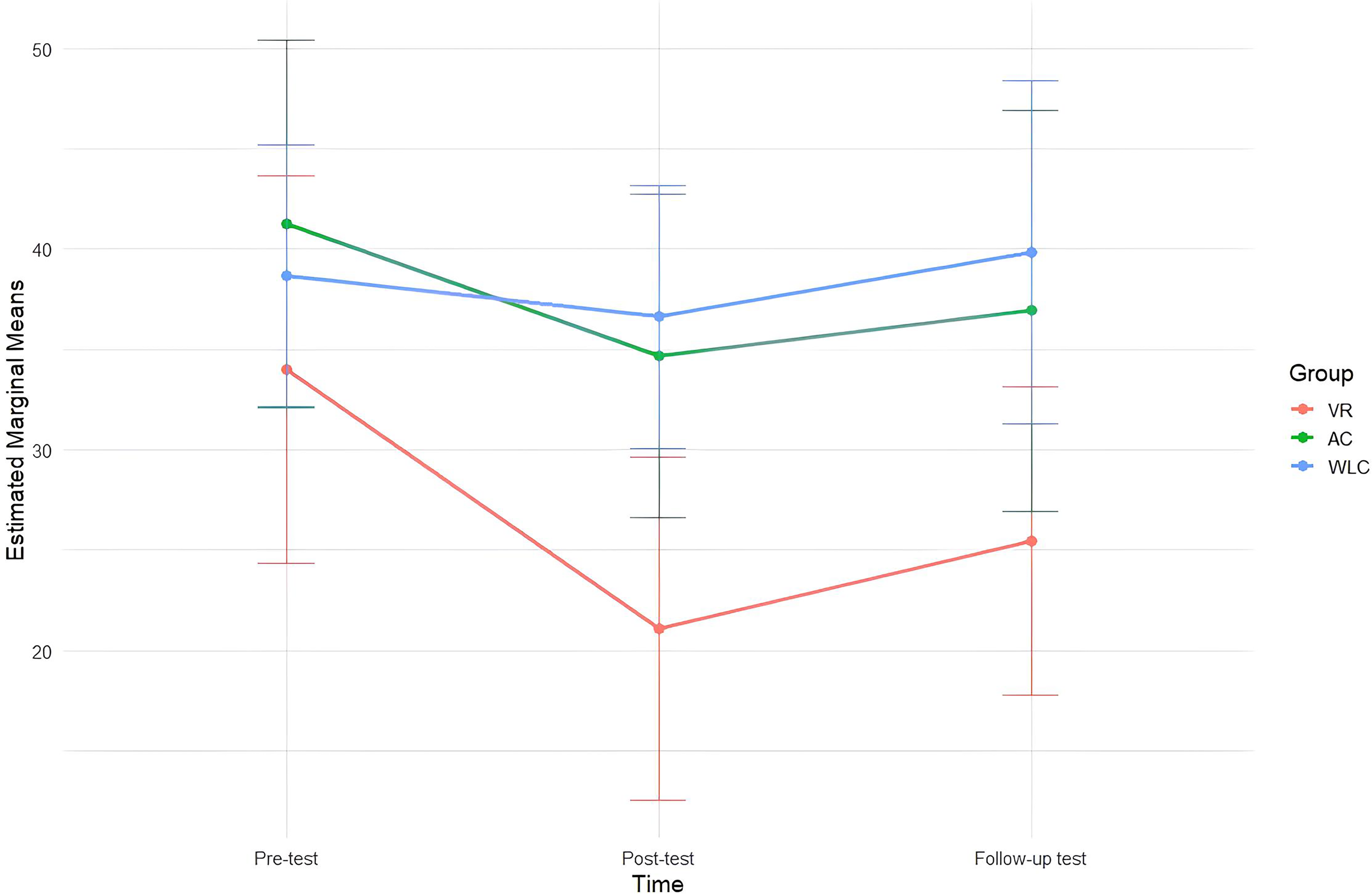
Estimated marginal means of subjective sleep patterns across time points.
Objectively measured sleep efficiency, assessed via actigraphy at pre- and post-intervention, differed significantly among groups (F = 3.73, p = .033). Post-hoc analysis indicated significantly greater improvements in sleep efficiency in the AC group compared to the VR group (p = .035). No significant group differences were observed in total sleep duration (Table 3).
Group differences in objective sleep patterns.

(n = 41).
Post-hoc comparisons were conducted using the Bonferroni correction; VR: virtual reality.
The average usability score for the VR intervention was 8.75 out of 10 at post-test, indicating high overall satisfaction. Participants reported particularly high satisfaction with the clarity of instructions (9.85 ± 0.55), the pacing of the program (9.69 ± 0.85), ease of operation (9.54 ± 1.20), and the visual quality and resolution of the program (9.46 ± 0.66), suggesting that the technical performance of the intervention was well-received. The lowest satisfaction rating was for discomfort associated with wearing the VR headset (6.85 ± 3.31).
Discussion
This study investigated the effects of a nature-based immersive VR relaxation programs on mental health and sleep patterns among Korean undergraduate students. The findings indicated a significant reduction in perceived stress levels and improvement in subjective sleep patterns, with effects sustained at 4-week follow-up.
Perceived stress levels
The effectiveness for stress level was consistent with prior research. In a study of 90 undergraduate students, an immersive VR intervention featuring a calming river scene significantly reduced perceived stress levels and heart rate. 33 Similarly, a systematic review of VR-based stress management interventions for adults without psychiatric disorders found that these interventions were effective in reducing perceived stress levels, with most utilizing immersive VR to simulate natural landscapes. 34 Exposure to natural environments in VR through audiovisual stimulation has been shown to enhance positive affect, reduce negative emotions, and increase emotional arousal.35,36 These psychological benefits may be explained by the restorative properties of undisturbed natural settings, which meet fundamental human needs for safety and psychological recovery. 37 Additionally, immersive engagement in virtual nature environments has also been shown to activate the parasympathetic nervous system, inducing relaxation and supporting mood regulation, which may contribute to stress reduction. 10
Sustained stress reduction observed at the 4-week follow-up may be attributed to immersive VR's activation of the parasympathetic nervous system, which promotes relaxation and emotional regulation. 38 The sense of presence and mindfulness induced by VR may also help reduce rumination and support adaptive coping strategies. 39 Furthermore, repeated exposure to restorative virtual environments may enhance positive emotions and psychological recovery, contributing to the durability of the effect. 40 Notably, during the sixth session, participants were allowed to select their preferred virtual environment, introducing a personal preference effect. This autonomy and individualized engagement may have further enhanced the perceived restorativeness of the experience, as environments aligned with personal taste are more likely to elicit positive emotional responses and foster a deeper sense of psychological restoration. 41
Therefore, nature-based immersive VR environments may function as emotionally engaging coping tools for stress management by enhancing the sense of realism and presence. By simulating tranquil natural settings, these interventions offer a psychological escape from stress-inducing situations and facilitate a restorative mental state, thereby effectively reducing perceived stress levels.
Sleep patterns
The nature-based immersive VR relaxation program was effective in improving subjective sleep patterns. Although no significant changes were observed in objective sleep indicators, participants reported improvements in their subjective sleep patterns. This divergence may reflect the fact that subjective perceptions of sleep are influenced not only by physiological parameters but also by psychological factors such as stress, mood, and cognitive appraisals. 42 In real-world settings, subjective sleep quality can have meaningful implications for daily functioning and well-being, potentially even more so than objective metrics. Therefore, improvements in subjective sleep assessments should be considered an important outcome of the intervention.
The AC group demonstrated a significant improvement in sleep efficiency, which is measured by actigraphy. However, no significant changes were observed in objective sleep parameters, as measured by actigraphy, in the VR group. This differential effect may be partially explained by variations in total sleep duration and time in bed, potentially influenced by the delivery context of each intervention. While participants in the AC group practiced PMR independently at home, those in the VR group were required to attend sessions in a simulation room at the affiliated institution due to limited availability of HMDs. Conducting the VR sessions in a non-home environment may have reduced the ecological validity of the intervention and limited participants’ ability to achieve a relaxed state prior to sleep. Moreover, most VR sessions were scheduled during the daytime, whereas PMR could be practiced at night before bed, possibly contributing to improved sleep efficiency in the AC group. To enhance the generalizability and real-world relevance of VR-based interventions, future research should prioritize enabling home-based implementation by securing an adequate number of HMDs. This may more accurately reflect the potential of immersive digital interventions to enhance sleep.
In this study, actigraphy was worn for three consecutive weekdays to maximize adherence. However, prior research suggests that a minimum monitoring period of 5 days—including both weekdays and weekends—is required for accurate assessment of sleep and activity patterns. 43 Extending the actigraphy monitoring period in future studies would allow for a more comprehensive and representative evaluation of objective sleep efficiency. Notably, in this study, actigraphy data were limited to pre- and post-intervention assessments and were not collected during the follow-up period. Given the emphasis on sustained improvements in sleep, the absence of objective sleep measurements at follow-up restricts our ability to fully assess the long-term effects of the interventions. Consequently, interpretations regarding the persistence of sleep benefits should be made with caution, and further studies are warranted to include extended objective monitoring to better understand the durability of sleep improvements.
Despite these limitations, the VR intervention had a significant impact on subjective sleep patterns. Previous research has demonstrated that nature-based meditation via immersive VR can enhance psychological stability and concentration, ultimately improving perceived sleep quality. 44 As subjective sleep experience is a critical component in evaluating overall sleep health, 45 this finding is particularly relevant for undergraduate students living in urban environments, where direct access to natural settings is often restricted. In this context, immersive VR may serve as a digital proxy for nature, compensating for limited access to real-world natural environments and fostering psychological restoration. Moreover, interacting with nature through VR has been shown to reduce anxiety related to outdoor environments and enhance familiarity with natural settings, potentially encouraging increased engagement in real-world outdoor activities. 41 These behavioral changes are significant, given that greater exposure to outdoor environments supports circadian rhythm regulation, which is essential for optimal sleep health.
Depression and anxiety levels
A previous study examining the effects of a VR-based relaxation program among individuals diagnosed with mood, anxiety, or psychotic disorders reported significant reductions in both depression and anxiety following the intervention.17,46 In contrast, the present study did not observe significant changes in depression or anxiety levels in the VR group compared to the AC or WLC groups.
This discrepancy may be attributed to key differences in study population and baseline symptom severity. Unlike prior research focusing on clinical populations, this study recruited general undergraduate students without screening for psychological distress. In the current study, pre-intervention T-scores for both depression and anxiety levels were below 55, suggesting that the majority of participants fell within the normal range. Given this low baseline symptomatology, the VR-based intervention may not have yielded statistically significant effects on these measures due to a floor effect. Nonetheless, in the VR group, average depression and anxiety scores showed a consistent downward trend across all time points (pre-test, post-test, and follow-up). Although these changes were not statistically significant, the observed pattern suggests that VR-based relaxation interventions may hold therapeutic potential for individuals with elevated baseline symptoms. Future studies should consider recruiting undergraduate students with moderate to severe depression and anxiety to more accurately evaluate the clinical effectiveness of the program.
Strengths and limitations
This study has several limitations. First, stress was measured solely via self-report, without incorporating physiological indicators such as heart rate, which could have provided more objective evidence of stress regulation. Second, the use of repeated assessments at three time points introduces the possibility of testing effects. Participants may have become familiar with the assessment content or process, which could have influenced their responses independently of the intervention. Third, while the observed improvements may reflect the intervention effect, it is also possible that non-specific factors, such as providing the VR group with a quiet space and dedicated time for relaxation, contributed to the outcomes. Fourth, limitations were identified in the usability evaluation. The lowest rated item concerned physical discomfort, such as dizziness or stuffiness, experienced during the VR sessions. Future VR-based interventions should address these issues through ergonomic and hardware improvements. Nevertheless, the highest rated usability item pertained to the clarity of instructions for VR device operation, underscoring the importance of clear guidance in minimizing user discomfort. Fifth, the study did not apply inclusion criteria related to levels of depression, anxiety, stress, or sleep disturbance, which may have reduced the likelihood of detecting intervention effects. Moreover, individuals with a current diagnosis of a mood disorder, anxiety disorder, or sleep disorder who were receiving psychiatric medication or psychotherapy were excluded from participation, which may limit the generalizability of the findings. Sixth, while participant anonymity was maintained during analysis, group allocation was not blinded to analysts. This introduces a potential risk of detection bias, as knowledge of group assignment may lead analysts to interpret outcomes more sensitively in the treatment group. Seventh, the study did not include formal attention or validity checks in the self-report questionnaires. Given that data collection was unsupervised, the accuracy of participants’ responses may have been influenced by factors such as inattentiveness or rushed completion.
Despite these limitations, this study has several notable strengths. The three-arm randomized controlled trial design enhances methodological rigor. The use of both subjective and objective sleep measures, combined with short-term and follow-up assessments, provides a comprehensive evaluation of the intervention. Moreover, by targeting a non-clinical population, this study demonstrates the potential of immersive VR-based relaxation as a scalable and accessible self-care strategy for promoting mental well-being and sleep quality among undergraduate students. In addition, common issues that often affect immersive VR performance in typical studies—such as unreliable Wi-Fi connections, poorly designed setups, and users’ unfamiliarity with VR—are usually present. 47 These challenges, however, were carefully addressed in the present study. The Meta Quest 2 headset was preloaded with the nature-based immersive VR relaxation program by the research team, ensuring that the intervention could operate independently of Wi-Fi connectivity. Participants received pre-session training on VR usage, and one-on-one support was provided throughout the intervention period. Sessions were conducted in a quiet, comfortable setting to ensure an optimal user experience. These design considerations helped mitigate performance-related concerns and contributed to the methodological rigor of the study.
Conclusions
This study demonstrates that nature-based immersive VR relaxation programs can effectively reduce perceived stress and improve subjective sleep patterns among undergraduate students. These findings underscore the potential of simulated natural environments delivered through immersive technologies as accessible, technology-enabled self-management tools for promoting mental well-being and sleep health in non-clinical populations.
To enhance the scalability and real-world applicability of such interventions, future research should address barriers such as VR-induced discomfort and explore home-based delivery models that preserve the ecological validity of the virtual nature experience. Further studies are also warranted to evaluate the effectiveness of nature-based VR interventions among individuals with higher baseline levels of psychological distress and sleep disturbances, thereby expanding their clinical relevance and contribution to digitally mediated environmental therapeutics.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251365140 - Supplemental material for Nature-based virtual reality relaxation to improve mental health and sleep in undergraduate students: A randomized controlled trial
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251365140 for Nature-based virtual reality relaxation to improve mental health and sleep in undergraduate students: A randomized controlled trial by Junggeun Ahn, Jiu Kim, Youngeun Park, Riah Kim and Heeseung Choi in DIGITAL HEALTH
Supplemental Material
sj-png-2-dhj-10.1177_20552076251365140 - Supplemental material for Nature-based virtual reality relaxation to improve mental health and sleep in undergraduate students: A randomized controlled trial
Supplemental material, sj-png-2-dhj-10.1177_20552076251365140 for Nature-based virtual reality relaxation to improve mental health and sleep in undergraduate students: A randomized controlled trial by Junggeun Ahn, Jiu Kim, Youngeun Park, Riah Kim and Heeseung Choi in DIGITAL HEALTH
Footnotes
Acknowledgement
We sincerely thank all individuals who participated in this study for their willingness to share their time and experiences, which were essential to the success of this research.
Ethics approval statement
This study was approved by the Institutional Review Board of Seoul National University (IRB No. 2305/004-009). All participants provided written informed consent before participation. The study was conducted in accordance with the Declaration of Helsinki and relevant ethical guidelines.
Consent to participate
Written informed consent was obtained from all participants prior to their enrollment in the study.
Author contributions
JA contributed to conceptualization, validation, formal analysis, investigation, data curation, writing—original draft, writing—review & editing, supervision, project administration, and funding acquisition. JK contributed to conceptualization, validation, formal analysis, investigation, data curation, writing—original draft, writing—review & editing, and supervision. YP contributed to investigation, data curation, and writing—original draft. RK contributed to investigation, data curation, and writing—original draft. HC contributed to conceptualization and writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Institute of Nursing Science, Seoul National University, (grant number Student Research Grant in 2023).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Due to ethical concerns and the absence of participant consent for public data sharing, the anonymized data are not openly available. However, they may be provided by the corresponding author upon reasonable request, subject to review of the research purpose.
Guarantor
Junggeun Ahn (first author) and Jiu Kim (corresponding author) serve as the guarantors of this work. They take full responsibility for the integrity of the data, the accuracy of the analyses, and the overall content of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.