
Abstract
Background
Although a number of studies have investigated the effects of internet use on the health status of middle-aged and older adults (MAOAs), there has been surprisingly little research exploring whether the use of internet among MAOAs has a positive association with the health of their family members.
Objective
This study aims to explore the relationship between MAOAs’ internet use and the health of their family members, including spouses, siblings, and children.
Methods
The datasets were extracted from the China Health and Retirement Longitudinal Survey conducted in 2015 and 2018, comprising 15,946, 37,565, 31,057 individuals who were spouses, siblings and children of MAOAs, respectively. The binary logistic models combined with individual-, household-, community-, and time-level random intercepts were constructed to estimate the association between MAOAs’ internet use and the health of their family members. A series of sensitivity analyses was conducted to assess the robustness of the study findings.
Results
Internet use by MAOAs was associated with a rise in the odds of reporting to have a good health status by an average of 209.29%, 23.12% and 85.71% for their children, spouses, and siblings, respectively. The positive association of internet use by MAOAs and health were found to be most pronounced among children, especially those from less affluent backgrounds. While internet use contributed to improved health among female siblings, statistically significant positive association was only observed for male spouses.
Conclusions
Effective strategies and action plans aimed at promoting internet use should account for the holistic impact of family engagement in addressing the health needs of both MAOAs and their family members in the era of rapid population ageing.
Introduction
With the recognition that information and communications technologies present new opportunities and challenges for the achievement of all 17 Sustainable Development Goals, there has been a growing consensus in the global health community that the strategic and innovative use of digital and cutting-edge information and communications technologies serves as an essential enabling factor for improving population health. 1 In line with the international trends, how to effectively bridge the digital divide to create an inclusive digital society, wherein the rapidly growing elderly population has equal access to and fully utilizes the potential of digital technologies to improve their quality of life and to achieve sustainable development of an ageing society, has become a grand mission for China. On the one hand, the Chinese government has been proposing strategies to address the challenges arising from the intersection of digitalization2–5 and population ageing.6–10 On the other hand, the Chinese government has issued specific action plans11–16 to improve access to digital goods/services, to enrich the content of digital products/services and improve their affordability, to improve the quality of digital products/services, and to foster digital literacy in the elderly. Consequently, the proportion of internet users aged 50 and above in China increased from 31% in 2022 17 to 34% in 2024, 18 indicating that the internet has further penetrated among the middle-aged to elderly age group. A study conducted in 2023 among 1686 Chinese elderly residents in rural areas across four provinces found that, on average, participants watched short videos five times per day, with a mean daily usage time of one hour. 19
Plenty of studies have delved into the health effects of using the internet among middle-aged and older adults (MAOAs), especially in countries where digital technologies are advancing and spreading rapidly. Some studies have investigated the effects of internet use on the health of MAOAs, concluding that the use of internet was effective in improving their self-assessed health,20–23 physical health (measured by their abilities to perform daily living activities), 22 mental health (assessed through indicators such as depression,22,24–29 cognitive functions,26,30 and loneliness 31 ) and subjective well-being (measured by indicators such as life satisfaction29,32,33), although other studies have also demonstrated no association34,35 or a negative association36,37 between internet use and the health. In contrast to the relatively extensive literature examining the effects of internet use on the health of MAOAs, there has been surprisingly little research on whether internet use among these individuals has a positive association with the health of their family members. Family members are regarded as a vital source of informal caregiving for older adults, particularly in developing countries where formal care systems are lacking and in societies where traditional cultures emphasize family responsibility over institutionalized care. A substantial body of research has shown that the health behaviors of older adults had spillover effects on their family members’ health behaviors, such as decisions regarding long-term care insurance enrollment, 38 vaccination uptake, 39 and healthcare service utilization. 40 These findings underscore the interconnectedness of family relationships (particularly, marital relationships 41 ) in later life and their influence on the health of family members, suggesting a potential link between internet use by MAOAs and the health of their family members. However, while some studies have highlighted the role of family members in value co-creation behaviors (such as providing emotional support and guidance to facilitate internet adoption among MAOAs42,43), very limited research has examined whether the interdependence within families in later life may contribute to an association between internet use by older adults and the health outcomes of their family members. Meanwhile, numerous studies have highlighted that informal caregiver of MAOAs faced significant risks of both physical and mental health challenges,44–48 particularly in Asian countries like China, where informal caregivers play a crucial role in providing care for MAOAs. 48 Specifically, it is estimated that each year in China, 53 million MAOAs received informal care from their spouses, children, and other family members. 49 With increasing life expectancy, changes in family structure and the continuous relaxation of the hitherto strict family planning policies in recent years, 50 informal caregivers in China are expected to bear a significantly heavier burden in meeting the complex care needs of MAOAs in the future.
As such, it is crucial to investigate whether internet use by MAOAs has the potential to generate health benefits for their family members. This study aims to address this knowledge gap by examining whether internet use among MAOAs is positively associated with the health of their family members. The structure of this manuscript is as follows: the methods section introduces the data sources, measures of study variables, and statistical approaches applied; study findings were reported in the results section before being discussed in the discussions section; the conclusion section concludes with key study findings and suggestions for future reforms.
Methods
Sample and data collection
This study adopted a repeated cross-sectional study design. Specifically, the datasets used in this study were extracted from the China Health and Retirement Longitudinal Survey (CHARLS), a nationwide survey conducted to gather microdata representing Chinese individuals aged 45 years and older. The CHARLS was launched in 2011 and is conducted every two or three years, capturing data from approximately 17,000 individuals from 10,000 households in 28 provinces across China. 51
The CHARLS did not collect data on the health of MAOAs’ children and siblings in 2011 and 2013, nor on the health of MAOAs’ spouses and siblings in 2020 (further details on the availability of data on dependent variables across the CHARLS waves are provided in Supplemental Table S1). Based on the availability of data on key study variables (i.e. MAOAs’ internet use and their family members’ health status), we extracted data from the third wave (conducted in 2015) and fourth wave (conducted in 2018) of the CHARLS.
As the CHARLS surveyed different characteristics of family members, we created three separate datasets comprising the spouses, children and siblings of MAOAs. After excluding observations with missing values either on MAOAs’ internet use or their family members’ health status (more details on the inclusion and exclusion criteria for sampling can be found in Supplemental Table S2), we finally obtained three separate repeated cross-sectional datasets comprising 15,946, 37,565, 31,057 individuals who were spouses, siblings and children of MAOAs in 2015 and 2018. Due to data unavailability, we were unable to distinguish between informal caregivers and noncaregivers in our study, which suggests that our estimates of the association between internet use by MAOAs and the health of their family members may be systematically larger if the sample were restricted to family members who were informal caregivers of MAOAs.
Measures of dependent and independent variables
The health status of family members was included as the outcome variable and was measured by a self-rated health status variable, with the response being rated on a five-point scale ranging from 1 representing “very good health status” to 5 representing “very poor health status.” As our study included a set of categorical variables as independent variables, we transformed the five-category dependent variable into a dummy variable that contains two responses (with 1 representing “very good health status” or “good health status” and 0 otherwise) 52 to prevent the presence of multicollinearity and complete separation (sometimes referred to as perfect prediction in the literature). Internet use by MAOAs was measured using a binary variable indicating whether the sampled MAOAs used the internet within the month prior to the interview (with 1 representing “yes” and 0 representing “no”).
When estimating the association between internet use by MAOAs and their family members’ health, we also controlled for the effects of the demographic and socioeconomic characteristics of MAOAs’ family members. Prior studies have demonstrated that age,53–56 gender,53–56 education,53,54,56 marriage,54,56 income,53,55,56 employment,54,56 Hukou,57,58 living region,53,55 political participation 59 and social contact 53 were determinants of self-rated health. In our study, we attempted to account for all relevant covariates identified in the existing literature and theories when estimating the association between internet use by MAOAs and the health of their spouses, children, and siblings. However, due to some covariates having a large number of missing values, we excluded these covariates from the regression models to reduce potential bias from their inclusion. Specifically, when estimating the association between internet use by MAOAs and the health of their children, we excluded living region (with more than 30% missing values) and education (with more than 74% missing values); for spouses, we excluded marital status, political membership and contact with MAOAs, due to 100% missing values; and for siblings, we excluded Hukou, employment, contact with MAOAs, living region and education, due to 100% missing values. For covariates with fewer missing values, we imputed missing continuous variables with the sample mean and missing categorical variables with the sample mode. Consequently, when estimating the association between internet use by MAOAs and the health of their children, we included age, gender, Hukou, marriage, income, employment, political membership, contact with MAOAs as covariates; for spouses, we included age, gender, Hukou, income education, employment and living region as covariates; and for siblings, we included age, gender, political membership and marriage as covariates. To fully assess the implications of the missing data processing strategy, we constructed regression models with and without covariates to ensure the robustness of the association between MAOAs’ internet use and the health of their family members.
Statistical analysis
A set of statistical and econometric techniques were used to investigate the association of internet use by MAOAs on their family members’ health. We first compared variations in family members’ health, demographic, and socioeconomic characteristics across groups classified by MAOAs’ use of internet. Specifically, we performed student t-tests (or chi-square tests) to assess differences in family members’ health, demographic, and socioeconomic characteristics between the groups based on MAOAs’ internet use. Subsequently, as family members’ health status was measured by a dummy variable, the logistic regression was considered superior to linear regression as it was specifically designed for binary classification problems. 60 Meanwhile, since our study used three separate repeated cross-sectional datasets comprising 15,946, 37,565, 31,057 individuals who were spouses, siblings and children of MAOAs in 2015 and 2018, for the purpose of adjusting for the effects of unobserved factors, we included individual-, household-, community-, and time-level random intercepts into the regression model. 61 This means that we constructed binary regression models combined with random effects estimator to quantify the association between internet use by MAOAs and the health of their family members.
To check the robustness of our study findings, a set of sensitivity analyses were conducted. First, to check whether our classification of responses (1 representing “very good health status” or “good health status” and 0 for all other responses) affected our study findings, we instead grouped the categories of “very good,” “good,” and “fair” into one group when creating the dummy variable to measure family members’ health status. Second, to check the heterogeneity in the association between internet use by MAOAs and their family members’ health, we conducted subgroups analyses based on datasets of subgroups classified by family members’ demographic and socioeconomic characteristics. Third, although using self-reported binary health variables as the primary measure of health allows for comparable results regarding the association of internet use by MAOAs and the health of their siblings, children, and spouses, it may be subject to reporting bias and fail to capture other aspects of health. Therefore, we conducted an additional analysis to explore whether internet use by MAOAs has an association with both mental and physical health for MAOAs’ spouses. Specifically, mental health was measured using the Center for Epidemiologic Studies Depression Scale, 10-item version (with its score ranging from 0 to 30), while physical health was assessed by whether having difficulties performing activities of daily living, including dressing, bathing and showering, eating, getting in and out of bed, and using the toilet. We used the Chi-Square Test to check for the presence of significant patterns in the residuals and hence informing the overall performance of the fitted regression models. The McFadden's pseudo R-squared was used to examine the goodness of fit of all the regression models. All of the analyses were conducted using the open-source programming language R. A two-sided p < .05 was considered statistically significant.
Results
Sample description
Table 1 reports the results of the descriptive analysis. Out of 31,057 sampled children, 15,946 sampled spouses, and 37,565 sampled siblings, 13%, 19%, and 20% of their parents, spouses and siblings used the internet within the month preceding the survey. The average age of the sampled children, spouses, and siblings of MAOAs was 38 (SD = 11), 60 (SD = 9), and 60 (SD = 11), respectively. The sampled family members of MAOAs who used the internet within the month preceding the survey were more likely to report having a good health status than those of MAOAs without internet use (children 77% vs 51%, p < .001; spouses 36% vs 23%, p < .001; siblings 54% vs 42%, p < .001). Most of the sampled children were male (52%; N = 16,090), had an agricultural “Hukou” (74%; N = 22,841), were married (72%; N = 22,295), had an annual income exceeding 10,000 CNY (56%; N = 17,352), were employed (80%; N = 24,706), were not a member of the China Communist Party (92%; N = 28,486), and did not visit their parent biweekly (75%; N = 23,328). Most of the sampled spouses were female (52%; N = 8282), lacked a secondary school or higher-level education (87%; N = 13,846), had an agricultural “Hukou” (68%; N = 10,908), had an annual income of less than 10,000 CNY (86%; N = 13,654), and were employed (69%; N = 10,925). Most of the sampled siblings were male (56%; N = 20,969), not a member of the China Communist Party (93%; N = 34,992), and married (84%; N = 31,462).
Comparisons of family members’ characteristics between groups classified by middle-aged and older adults’ internet use.

Results of main regression analyses
The association between MAOAs’ use of internet and their children, spouses and siblings’ health was reported in Table 2. Internet use by MAOAs was found to have a positive association with their family members’ health in both the models with and without adjustment for covariates. Specifically, after controlling for the effects of a set of covariates, MAOAs’ use of internet led to a rise in the odds of reporting to have a good health status by an average of 209% (95% CI [150% to 283%]; p < .001), 23% (95% CI [10% to 38%]; p < .001) and 86% (95% CI [62% to 112%]; p < .001) for their children, spouses, and siblings, respectively.
The association between middle-aged and older adults’ internet use and their family members’ health.

a OR: odds ratio.
b SE: standard error.
Children who were older (OR 0.06; 95% CI [0.05 to 0.07]; p < .001), were males (OR 0.91; 95% CI [0.84 to 0.98]; p = .014), had a nonagricultural “Hukou” (OR 0.65; 95% CI [0.58 to 0.74]; p < .001), were married (OR 1.23; 95% CI [1.12 to 1.36]; p < .001), had an annual income exceeding 10,000 CNY (OR 1.34; 95% CI [1.22 to 1.47]; p < .001), were employed (OR 1.74; 95% CI [1.56 to 1.95]; p < .001), had the China Communist Party membership (OR 1.56; 95% CI [1.34 to 1.81]; p < .001), and visited MAOAs biweekly (OR 1.12; 95% CI [1.02 to 1.23]; p = .014) tended to report to have a good health status than their counterparts.
Similarly, spouses who were older (OR 0.21; 95% CI [0.15 to 0.28]; p < .001), were males (OR 0.77; 95% CI [0.71 to 0.83]; p < .001), had a nonagricultural “hukou” (OR 0.84; 95% CI [0.75 to 0.95]; p = .003), had an annual income exceeding 10,000 CNY (OR 1.17; 95% CI [1.03 to 1.32]; p = .01), had a secondary school or higher-level education (OR 1.32; 95% CI [1.16 to 1.50]; p < .001), were employed (OR 1.65; 95% CI [1.48 to 1.83]; p < .001), and lived in urban areas (OR 1.50; 95% CI [1.31 to 1.73]; p < .001) tended to report having a good health status than their counterparts.
Siblings who were older (OR 0.13; 95% CI [0.10 to 0.16]; p < .001), male (OR 0.73; 95% CI [0.68 to 0.78]; p < .001), were married (OR 2.23; 95% CI [2.03 to 2.45]; p < .001) and were a member of the China Communist Party (OR 1.61; 95% CI [1.41 to 1.84]; p < .001) had a higher probability of reporting to have a good health status than their counterparts. The p-values from the Chi-Square tests for all regression models exceeded .05, indicating good model fit. Compared to models using spouses’ health status as the dependent variable, those with children's or siblings’ health as the dependent variable exhibited higher explanatory power (with Pseudo R-squared values of approximately 0.2).
Results of sensitivity checks
Figure 1 reports the results of subgroup analyses. The positive association between MAOAs’ use of internet use and their family members’ health was found to be more pronounced among children who had an annual income of less than 10,000 CNY (OR 9.96; 95% CI [7.65 to 12.98]; p < .001), male spouses (OR 1.93; 95% CI [1.66 to 2.23]; p < .001), and female siblings (OR 2.75; 95% CI [2.25 to 3.35]; p < .001) of MAOAs.

Results of subgroup analyses.
Table 3 reports the results of sensitivity analysis where a different grouping strategy was adopted to generate the dummy dependent variable. The results show that MAOAs’ use of internet was still positively associated with the health of their children (OR 4.21; 95% CI [3.29 to 5.37]; p < .001), spouses (OR 2.11; 95% CI [1.86 to 2.39]; p < .001) and siblings (OR 2.21; 95% CI [1.95 to 2.50]; p < .001).
The results of sensitivity analysis using a different grouping strategy.
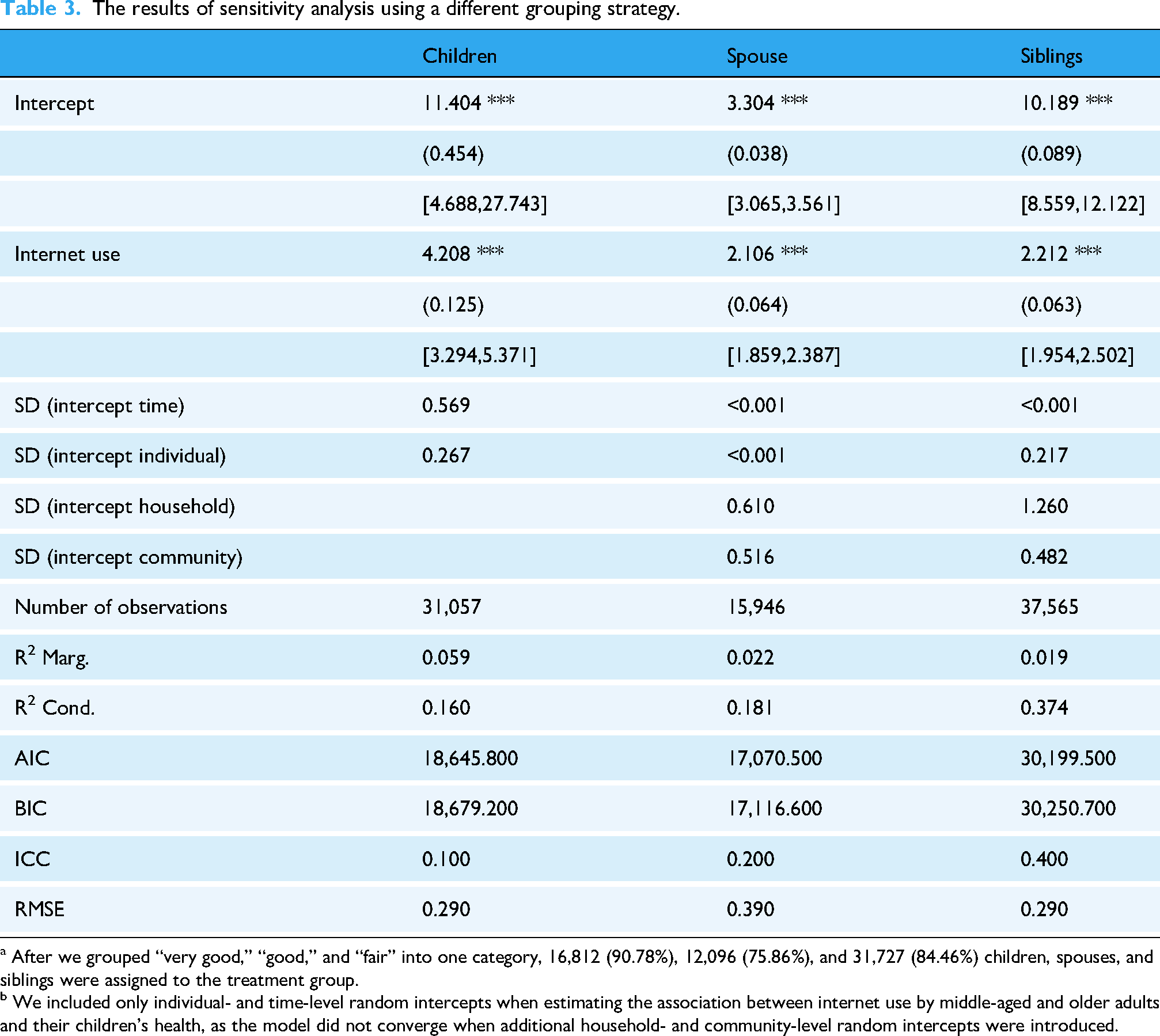
a After we grouped “very good,” “good,” and “fair” into one category, 16,812 (90.78%), 12,096 (75.86%), and 31,727 (84.46%) children, spouses, and siblings were assigned to the treatment group.
b We included only individual- and time-level random intercepts when estimating the association between internet use by middle-aged and older adults and their children’s health, as the model did not converge when additional household- and community-level random intercepts were introduced.
Table 4 presents the association between MAOAs’ internet use and the mental and physical health of their spouses. The results indicate that internet use by MAOAs was associated with a decline in the odds of feeling depressed (IRR 0.91; 95% CI [0.88 to 0.95]; p < .001) and experiencing difficulties in performing activities of daily living (OR 0.70; 95% CI [0.58 to 0.84]; p < .001) for their spouses. These findings jointly suggest that our key findings on the positive association between MAOAs’ use of internet and their family members’ health generated in our main analysis were robust.
The association between middle-aged and older adults’ internet use and the mental and physical health of their spouses.

a IRR: incidence rate ratio.
b SE: standard error.
c OR: odds ratio.
Discussion
Principal findings
This study constructed logistic regression models combined with random intercepts to investigate the association between MAOAs’ internet use and the health of their family members (including their children, spouses, and siblings). The key findings indicate that internet use by MAOAs improved the health of their family members, with this positive association being more substantial among nonrich children, male spouses, and female siblings.
This study demonstrated that internet use by MAOAs was associated with better health outcomes for their family members (including their children, spouses, and siblings), stressing the potential external positive effects of internet penetration among MAOAs. These findings are consistent with previous studies conducted in China20–26,28–30,33 and other countries,27,31,32 which have highlighted the health benefits of internet use among MAOAs. The potential underlying mechanisms through which internet use among MAOAs affects the health of their family members likely involve resource-sharing behaviors and strengthened social connections within the family. Due to resource-sharing within families, internet and internet-based interventions provide opportunities for both MAOAs and their family members (especially those living together and/or having frequent contact) to gain greater access to health information and services as well as become more involved in health self-management.62–65 Additionally, internet and internet-based interventions facilitate easy and affordable ways (such as video calls, social media, and messaging applications) for MAOAs to connect with and develop supportive relationships with their family members.31,32 Resource-sharing and strengthened family connections not only directly enhance the mental and physical health of MAOAs’ family members but also ease their caregiving burden, thereby amplifying the health benefits associated with MAOAs’ internet use.
Our study also found that the positive association between internet use by MAOAs and health was more noticeable among their children than on their spouses and siblings. Children take a predominant role in offering informal care for their ageing parents in China, where the filial piety that emphasizes the moral obligation of respect and care for ageing parents has been recognized as a common virtue. 66 This is very likely to occur within a care system for MAOAs that still faces pressing challenges, including a shortage of long-term care workforce, weak quality assurance, and insufficient public financing. 67 These younger generations, born and raised in the digital age and well-versed in internet use, often engaged with older adults through internet-based technologies, such as intergenerational digital programs.68,69 Meanwhile, recent reresearch 70 has highlighted the phenomenon of “digital feedback” among the younger generations, where young family members have shown a willingness to assist older adults in accessing the internet, guide them in using digital technologies and new media, and ultimately shape the digital technology use behaviors of the elderly. These findings suggest that children, by offering support, guidance, and encouragement to help MAOAs use the internet and by connecting with MAOAs through digital means, were actively engaged in the digital lives of MAOAs. This may explain why the positive association between internet use by MAOAs and health was more pronounced among their children than among their spouses or siblings.
As shown by the results of subgroup analyses, this study found that the positive association between internet use among MAOAs and health was more substantial among children who were less affluent. This finding may be explained by the fact that young adults with a less privileged background were more likely to use internet for social activities (for instance, using social applications to communicate with their parents), while those with a more resource-rich background tended to use the internet for more “capital-enhancing” activities. 71 Another essential finding is that although internet use among MAOAs was positively associated with the health of male spouses, its association with the health of female spouses did not reach statistical significance. There has been a sharp gender division in family caregiving patterns in China. In a society deeply influenced by Confucian culture, Chinese women have historically been constructed as family caregivers, characterized by traits such as endurance and selfless devotion. These caregiving responsibilities have been further reinforced since China's transition from a socialist centralized economy to a market economy since the 1980s, 72 along with the introduction of the one-child policy and epidemiological transitions. 73 In the context of the absence of a formal care system, 74 these changes weakened socialist collectivist norms and fostered new attitudes toward individualization, which led to the emergence of a “sandwich generation,” where women are required to care for multiple senior family members (including their husbands) 74 while also facing competing demands for care between elderly parents and young children. 75 Meanwhile, many prior studies have revealed gender differences in family caregiving,76,77 concluding that: (1) females often dedicated more time to caregiving than males; (2) females were more likely to encounter caregiving stressors and tended to perceive, report, and cope with these stressors differently than males; and (3) females tended to experience higher levels of mental and physical strain while providing care compared to their male counterparts. Based on these facts, it is expected that while internet use by MAOAs may offer potential health benefits for females, it may not be sufficient to improve the health of female spouses.
Our study findings offer essential practical implications for policy initiatives aimed at promoting internet use and internet-related health interventions to address the growing demand for healthcare among the elderly population. Policymakers in both developed and developing countries should prioritize accelerating the adoption of internet use as the first step toward digital transformation, which could bring huge health benefits to both older adults and their family members. In recent years, China has implemented a series of policy initiatives aimed at improving access to, enhancing utilization of, and promoting digital literacy for older adults to bridge the digital divide faced by MAOAs (more details on these policy initiatives are summarized in Supplemental Table S3). One potential optimization of these policies is to emphasize the role of family engagement in their design and implementation. For example, when developing digital literacy promotion programs, including family members as part of the intervention population, rather than solely targeting older adults, could be a more cost-effective strategy, particularly when older adults face physical or mental health challenges. Similarly, policies encouraging digital commerce companies to develop elderly-oriented digital products could introduce incentives to promote family-inclusive features, enabling family members to interact with and support older adults through these digital tools. With continued efforts from the government and relevant stakeholders, the health benefits of internet and internet-based digital technologies are expected to be realized and widely disseminated.
Strengths and limitations
While there has been an increasing number of research exploring the health effects of internet use by MAOAs, this area is ripe for new research that brings more focus to the role of health and well-being as antecedents and outcomes of using the internet. 78 Our study added to the existing literature by exploring, for the first time, the association between internet use among MAOAs and the health of their family members using a nationally representative sample from China. Additionally, our study demonstrated the positive association between internet use among MAOAs and the health of their family members, while simultaneously identifying the groups that benefited the most. These findings have practical implications in terms of guiding the design of intervention programs that utilize digital technologies to improve the health of both older persons and their informal caregivers in countries characterized by rapidly expanding digitalization and population ageing. Furthermore, our study has methodological strengths in terms of adopting a repeated cross-sectional study design with a nationally representative sample, which minimizes bias in estimates and enhances the generalizability of our study findings.
Some limitations should be recognized when interpreting the findings of this study. The first limitation is the lack of data on certain variables, which prevented us from exploring the association between internet use by MAOAs and other health outcomes and understanding the underlying mechanisms through which these associations occur. Our main analysis focusing on the self-reported health of MAOAs’ family members offers the advantage of being a simple and easy-to-implement measure, but self-reported data carries the risk of recall bias. We tried to overcome this shortcoming by conducting an additional sensitivity analysis of the association between internet use by MAOAs and the mental and physical health of their spouses. We provided results on how internet use may influence the overall health of MAOAs’ family members by impacting both their mental and physical well-being of their family members. Future studies with a detailed tracking of more information on family members are suggested to explore the association between internet use among MAOAs and a wide range of health outcomes (including physical health and mental health) for their family members. Further studies are also recommended to explore factors that moderate or mediate the association between internet use and health, which would greatly contribute to the existing literature by providing a more comprehensive understanding of how internet use among MAOAs yielded health benefits of their family members. Second, we failed to handle the imbalance in the demographic and socioeconomic characteristics of family members between groups classified by MAOAs’ internet use, which may bias the estimates of the spillover health effects of internet use. To correct for such confounding bias, we attempted to use the matching method to create a balanced dataset for estimation. However, a large number of observations were excluded after matching, resulting in the nonconvergence of the regression models. Nevertheless, the bias would have been greater if we had neither estimated the association between internet use by MAOAs and the health of their family members in models with and without adjustment for a set of covariates, nor constructed logistic regression models combined with random intercepts to adjust for the effects of unobserved individual-, household-, community-, and time-level confounders. Future studies with larger datasets are recommended to adopt econometric techniques (such as the propensity score matching method) to correct for potential confounding bias in nonrandomized studies. Another limitation is that, due to data unavailability, we were unable to provide a more detailed analysis of the association between specific types/modes of internet use by MAOAs and the health of their family members. We highly recommend that future studies include information on the purposes of internet use (such as digital health, digital finance, digital government, digital entertainment, etc.) and the methods of internet use (such as via laptops, mobile phones, etc.) in relation to the health of family members. Such an analysis has the potential to identify actionable factors that policymakers and practitioners can use when designing internet-based intervention programs.
Conclusions
This study demonstrated that internet use by MAOAs contributed to health improvements for their family members, particularly among children who were less rich, male spouses, and female siblings. Considering the potential positive external effects of promoting internet use among MAOAs, the society, equipment manufacturers, and family members of MAOAs are recommended to work together to reap the benefits of internet penetration. Particularly, policy decision-makers are suggested to be cognizant of the power of integrated and collaborative management to fulfill the tremendous potential of digital technologies in improving population health in the era when digital transformation is shaping the future of the healthcare sector. Specifically, while the diffusion of internet use among MAOAs holds the potential to generate health benefits, it is essential to consider the influence of family dynamics on health outcomes and to develop thoughtful implementation strategies tailored to vulnerable groups. This approach has the potential to improve the effectiveness of internet and digital-based interventions, ultimately reducing costs for health systems.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251382849 - Supplemental material for Association between internet use by middle-aged and older adults and the health of their family members: Nationally representative longitudinal survey in China
Supplemental material, sj-docx-1-dhj-10.1177_20552076251382849 for Association between internet use by middle-aged and older adults and the health of their family members: Nationally representative longitudinal survey in China by Zixuan Peng in DIGITAL HEALTH
Footnotes
Abbreviations
Ethical considerations
Ethical approval for all the CHARLS waves was granted from the Institutional Review Board at Peking University. The protocol of field work of the main household survey was approved (IRB 00001052-11015).
Consent to participate
During the fieldwork, each respondent who agreed to participate in the survey was asked to sign two copies of the informed consent.
Author contributions
ZP: writing—original draft; writing—review and editing, methodology, formal analysis, data curation, and conceptualization.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Startup Research Fund of Southeast University (Grant No. 4025002402) and the Jiangsu Health Economics Association (Grant No. JSWSJJ202507).
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.