
Abstract
Objective
This study aimed to assess the effects of older Chinese adults’ online behaviors (including recent access to the Internet and duration of Internet use) on their current health habits and health status. Health status comprised self-rated physical and mental health.
Methods
Interviewees aged over 60 years who participated consecutively in the 2010, 2014, 2018, and 2020 China Family Panel Studies were selected. Ordinary least squares and ordered logit regression analyses were used to analyze the associations between older adults’ online behaviors and their health habits and status. Propensity score matching analysis was employed to mitigate selection bias. Structural equation modeling was conducted to test the robustness of the findings and to explore whether the associations between recent and continued Internet use and their health were mediated by older adults’ prioritization of online entertainment, learning, communication, and lifestyle-related activities.
Results
The results showed that Internet access among older adults was positively associated with health habits, increased self-rated health levels, and improved physical and mental health. Continuous Internet use among older adults may be a predictor of better mental health. While prioritization of online life style could improve physical health, prioritization of online communication might be prejudicial to acquiring health habits.
Conclusion
Internet access may support healthy aging by encouraging older adults to adopt healthier lifestyles. However, the varied effects of different types of online behavior underscore the importance of designing targeted digital interventions rather than blanket promotion of technology adoption.
Keywords
Introduction
The number of Chinese netizens aged over 60 years is increasing. Notably, as shown in Figure 1, the proportion of Chinese netizens aged over 60 years was below 5% from 2008 to 2016. However, the COVID-19 pandemic triggered a sharp rise in Internet use among older Chinese adults, contributing to an increase of over 100 million netizens by late 2020. The network penetration rate among Chinese adults aged 60 years and above was 57.36% in 2023. Nearly all Chinese netizens over the age of 60 years use mobile phones to access the Internet. They use instant messaging, online videos, government services, news, and payments. Interestingly, the usage rate of online news among Chinese netizens aged over 60 years is 3% higher than that among all netizens. 1

Internet penetration rate among Chinese adults aged over 60 years, the number of Chinese netizens aged over 60 years, and proportion to the entire number of netizens.
The digital divide among older Chinese adults became more evident during the COVID-19 pandemic. For instance, some older Chinese adults were unable to use their e-health codes, which limited their daily travel. Those without Internet access are excluded from digital society. 2 In particular, while 57.36% of older Chinese adults (those aged over 60 years) had become netizens by late 2023, nearly half of these older adults still lacked Internet access.
Figure 2 illustrates the motives attracting Chinese non-netizens to become netizens. From 2018 to 2021, the primary factor encouraging non-netizens to adopt the Internet was using it to communicate with family and friends. The motive of accessing specific information (e.g., medical and health information) has also been a major reason for accessing the Internet since 2018, which reflects the development and popularity of online medical services and the increasing demand for accessing online health-related information; this motive was ranked first in 2022 and 2023.

Motives to attract Chinese non-netizens to become netizens.
However, reports on the effects of Internet use on health are inconsistent. Most studies present a positive link between Internet use and health, indicating that Internet use enhances individuals’ physical and mental health status.3,4 Furthermore, the diverse purposes of Internet use by older adults may amplify the positive effects on physical and mental health. 5 However, overuse and Internet addiction are harmful to health. For example, the intensity of Internet use has a reverse U-shape on self-rated health and mental health.6–8 Furthermore, excessive Internet usage and mobile phone addiction may lead to physical discomfort, depression, and breakdown of family and social relationships.9,10 Internet use may also have an impact on health habits, which are highly correlated with health status. For example, digital programs have been employed to promote teenagers’ eating habits. 11 Using online health information can promote older adults’ health habits, including dietary habits and physical activities. 12
This study examined the effects of older Chinese adults’ online behaviors, including recent Internet access and Internet use duration, on their current health habits and health status. Health habits comprised dietary practices, physical activity, lifestyle behaviors, and sleep patterns, whereas health status was assessed using three dimensions: self-rated health, physical health, and mental health. This study selected interviewees who participated consecutively in the panels of the 2010, 2014, 2018, and 2020 China Family Panel Studies (CFPS) and who were aged 60 years and above in the panel of 2020. To investigate the relationships between online behaviors and health outcomes, this study employed both ordinary least squares (OLS) and ordered logistic regression analyses. To address potential selection bias related to Internet access, propensity score analysis was used. Additionally, structural equation modeling (SEM) was conducted for robustness checks and path analysis. The latter was used to analyze whether the associations between Internet behaviors (recent and long term) and health outcomes were mediated by older adults’ prioritization of online communication, learning, lifestyle, and entertainment activities.
Literature review
Internet use and health status
Information seeking and communication are two primary reasons why older adults use the Internet. 5 The Internet is a primary resource for people to acquire health information, and health information is one of the most frequently sought topics on the Internet.13–16 Access to online health information bridges the digital divide concerning Internet access and mitigates the impact of the digital divide concerning Internet use on health issues. 17 Due to high health concerns, older adults are the primary consumers of health information. 18 In particular, health information guides health behaviors, treatments, and decisions. 6 Access to online health information can break the monopoly of medical information providers, reduce asymmetry between professionals and ordinary individuals, and provide opportunities to individuals for self-health management. 19 Exposure to health information plays a crucial role in modifying health-related behaviors, ultimately leading to the adoption of healthier practices. 20 In general, seeking and obtaining trustworthy health information online, even through mobile applications, can help users to prevent diseases, enhance disease cognization, understand the presymptoms of diseases, and take part in physical activities, finally leading to the promotion of health habits and health status.3,4,21,22
Accessing online health information may improve mental and physical health. 23 Specifically, older adults can seek scientific information about mental illnesses and find abundant mental service resources to enhance their mental health status. Additionally, older adults can utilize online health information to prevent specific diseases and promote health management, such as weight control, healthy dietary habits, and immunizations, consequently resulting in a better physical health status.3,6,23 Mobile health applications have spread health information more widely. 6 Furthermore, resocialization theory states that as individuals age, they need to continue training, learn new skills, and update their knowledge to align with societal developments. 24 Using the Internet for learning could enhance older adults’ learning and social abilities, promoting the resocialization of older adults, and improving their mental and physical health status.5,22,24
Older adults gradually face diminishing social participation and interactions. 15 Online communication is a means to expand social networks, connect with friends and family, and reconstruct a supportive relationship to imbue further a sense of community.7,9 For older adults, online communication could help reduce isolation and loneliness and enhance social connectedness.8,12,25 Furthermore, online communication for older adults is a channel for social support. Through online communication, older adults can receive transgenerational emotional support from their families, empowering those with functional disabilities, and ensuring their self-efficacy.26,27 When older adults have higher social cohesion and social connectedness, they may enjoy a better mental and physical health status.10,19
Health status measurements can be categorized as objective and subjective. Mental health status is typically assessed using emotional and depression measures. Physical health status includes metrics such as physical pain, hospitalization, cancer diagnosis, and frequency of poor health affecting daily life.12,19,23,28 Among subjective measures, self-rated health is simple but exhibits good reliability and validity, effectively predicting morbidity and mortality.6,28 Self-rated health is a good indicator of health status among older adults. 29
Internet use and health habits
Internet use can also influence health habits. A health habit has been defined as “a neurologic pattern initially established through repetition, then initiated by a cue resulting in automatic responses (automaticity) that are then manifested and acted upon through conscious recognition of the health impact of the response.” 30 Health habits are automatically learned components of behaviors and perceptions toward promoting health conditions, often established in early life and persisting throughout life.15,31 Positive health habits could protect people from harm and medical threats and prevent disease occurrence.32,33 These health habits include naps, healthy diets, physical activities, no smoking, and no alcohol abuse, for example.15,34,35
Health habits are highly correlated with health status. Lack of physical activity, inadequate eating habits, and other unhealthy habits may harm health and increase the risk of diseases and other complications.11,36,37 Conversely, regular physical activity and dietary plans can significantly promote health status.33,38
The use of the Internet may have positive effects on health habits, and several web-based computer-tailored interventions are helpful for the promotion of health habits. A pilot program based on technological solutions aimed to improve the nutritional habits and physical activities of adolescents to prevent obesity. The results showed that technological applications enhanced health habits and helped with attaining prevention goals in the short term. 39 Another application-based intervention aimed at improving eating habits among patients with type 2 diabetes, with the results showing that healthy eating habits had improved, subsequently influencing sleeping habits and physical activities positively. 36 Digital programs have been employed to promote adolescents’ eating habits. 11 Technological applications designed to improve habit strength in relation to nutrition and physical activities for people who wanted to reduce their cardiovascular risk showed positive effects between technological intervention and habit strength. 33 Another digital solution for intervention in terms of adolescents’ eating habits and physical activities has been shown to work effectively. 39 Furthermore, negative health habits, such as smoking and alcohol abuse, can also be subject to intervention using digital programs. 33 The interventions work effectively because participants’ self-efficacy and planning techniques help increase social cognization, consequently enhancing habit strength. 33
Theoretical approaches and hypotheses
Online communication and information-seeking are among the primary digital activities of older adults. Self-determination theory provides insight into the relationship between online communication and health outcomes, with social support acting as a moderator. According to this theory, intrinsic and extrinsic factors drive human motivation. Online communication serves as a form of social support that transforms extrinsic social context into intrinsic motivation. This process addresses the psychological need for competence, relatedness, and autonomy, thereby fostering greater participation in various social activities and ultimately improving both physical and mental health.40,41
Access to the Internet may offer a better perspective on health issues and help alleviate health concerns. Engaging with online health-related content acts as a form of social reinforcement, strengthening the connections between information and community while enhancing health empowerment. 17 The health empowerment hypothesis explains the mechanism by which online health information influences health outcomes. Accessing online health information helps alleviate health concerns, raises health awareness, and facilitates the sharing of health information. Through this process, users are empowered to cultivate health literacy, increase self-efficacy, accept health products, adopt new health habits, and modify their health behaviors. 17
Empowerment is understood as both a process and an outcome. As a process, empowerment refers to the mechanism through which individuals gain control over their lives; as an outcome, it encompasses the various consequences of this process.42,43 The health empowerment process includes two key actors: individuals who are responsible for their own healthcare and the institutions, organizations, or societies that enable individuals to fulfill these responsibilities, because empowerment is a transactional concept that involves collaborative efforts with others. 42
Empowerment is a proactive concept with the potential to enhance self-esteem and self-efficacy while promoting positive health behaviors. Furthermore, it enables individuals to master their environments, foster self-determination, and initiate changes within themselves, within interpersonal relationships, and within social structures.42,43
Health empowerment involves the responsibilities individuals have in achieving positive health and the impact of social environments on their well-being. 42 In this study, the social environment was limited to various online activities. Empowerment is a crucial factor in intrinsic motivation and comprises four components: expected effects, the degree of skills related to tasks or self-efficacy, idealized goals, and perceptions surrounding one's decisions. 43 The perceived benefits of information and decision-making are prerequisites for health empowerment, 44 which are closely aligned with the four components of empowerment mentioned earlier. These perceived benefits imply that individuals have established health goals and anticipate expected health gains as a result of their self-efficacy. Access to online health information and the acceptance of e-health services have empowered individuals by encouraging them to take control of their health management through informed decision-making.44,45
In addition to self-determination and health empowerment, the digital divide has emerged as a critical area of inquiry. It highlights inequalities in access to, usage of, and outcomes from digital technologies. Understanding these disparities provides a broader perspective on how digital realm inequalities affect individuals’ health, well-being, and overall quality of life.
Digital capital theory helps explain varying patterns of information and communication technology (ICT) use and outcomes across different social groups. Digital capital is a contemporary extension of Bourdieu's concept of capital, one that can be historically accumulated and transformed into different forms of capital, such as social, economic, personal, political, and cultural capital. 46 Among these, personal and cultural capital encompasses aspects such as an individual's health and well-being. Digital capital has been defined as “a set of internalized abilities and aptitudes” (digital competencies) and “externalized resources” (digital technology). Digital capital bridges online and offline capital. The interaction between digital capital and other forms of capital contributes to disparities in ICT usage and outcomes. Individuals with higher levels of social, economic, personal, political, and cultural capital tend to accumulate more digital capital and derive more meaningful online experiences. Conversely, individuals with limited access to these forms of capital may develop weaker digital capital, leading to more constrained digital engagement.46,47
Research examining factors that influence Internet use has frequently considered sociodemographic and socioeconomic variables such as age, gender, educational background, and social status. 48 Digital capital, resources gained through digital engagement, can subsequently be transformed into social resources and ultimately generating disparities in ICT-related outcomes across groups. These digital resources contribute to the production and reproduction of individual advantages, including health, which is a measurable personal outcome.46,47
Digital capital comprises two aspects: digital access and digital competence. Digital access includes elements such as digital equipment, connectivity, time spent online, and support and training. Digital competence encompasses information and literacy, communication and collaboration, digital content creation, safety, and problem-solving. To measure the historical accumulation of digital capital, the concept of time spent online typically refers to long-term engagement rather than daily Internet use. 47 However, for practical reasons related to data availability, this study used daily time spent online for empirical analysis. 47 Greater accumulation of digital capital can yield greater benefits, including improved health outcomes.
In summary, most existing studies have explored the relationship between Internet use and older adults’ health, focusing primarily on self-rated health, physical health, and mental health. However, few have investigated how Internet use influences health habits specifically. Furthermore, research on Internet use among older Chinese adults has largely relied on basic indicators such as recent Internet access and total time spent online. Nevertheless, a more nuanced understanding of Internet use should incorporate both usage duration and the diversity of online activities. 7 Years of Internet use are positively correlated with daily usage, and extended usage tends to foster broader online engagement and stronger digital literacy. 49 Thus, metrics such as daily frequency and duration of Internet access are valuable indicators of the depth of Internet engagement.48,50
According to digital capital theory, both daily time and historical online activity contribute to digital capital accumulation. This accumulated digital capital can be converted into other forms of capital. Consequently, older adults who are proficient in digital health literacy can access a wider array of health resources, gain social capital, and achieve greater prominence within online social networks.
15
Therefore, the following hypotheses are presented:
Materials and methods
Methods
This study is a quantitative analysis focusing on the effects of older Chinese adults’ online behaviors, including recent Internet access and the duration of Internet use, on their current health habits and health status. Secondary data were obtained from the CFPS conducted in 2010, 2014, 2018, and 2020. The CFPS collected comprehensive data from individuals, households, and communities across 25 provinces in China. This study was conducted between March and July 2024 in Changchun, China.
Ordered logistic analysis and the OLS model
This study focused on the relationship between older Chinese adults’ online behaviors and their health habits and health status, with the latter involving self-rated health, physical health, and mental health. Health habits, physical health, and mental health were continuous variables, while self-rated health was a five-item ranked variable. Therefore, ordered logit regression was applied to the self-rated health equation, whereas the OLS model was applied to the equations for health habits, physical health, and mental health.




Propensity score matching analysis
To address potential self-selection bias—where older adults with poorer health may be more likely to access the Internet for health-related reasons, propensity score matching (PSM) was used. Previous research has indicated that the proportion of older adults with health problems accessing the Internet may exceed that of their healthier counterparts, 21 raising concerns about reverse causality.
The treatment effects of recent Internet use on health habits and health status were defined as follows:

Because the treatment effect was a random variable, the average treatment effect (ATE) was measured as

The ATE on the treated (ATT) was measured as:

The ignorability and matching assumptions were satisfied in the selection of the observables. Three PSM steps were conducted. First, control variables were used as covariates that showed an imbalance between the treatment and control groups via logit regression, with the variables of gender, individual social status, and coresidence size found to be insignificant and consequently omitted. The second step entailed matching replacements in the common support region, and the third step involved applying a data balancing check to appraise the match quality.51,52 Propensity score matching involved using one-to-one nearest neighbor matching, radius matching, and kernel matching to measure the propensity score.
Structural equation modeling
Structural equation modeling was first employed to test the robustness of the regression results and subsequently used for path analysis. As shown in Figure 3, the mediating effects were examined among the older Chinese adults who had recently accessed the Internet, focusing on their online preferences related to communication, entertainment, learning, and life style. These effects were analyzed in relation to health habits and health status. Second, a similar analysis was conducted among the older Chinese adults who had long-term access to the Internet.

Path analysis using structural equation modeling (SEM).
Data
The analysis utilized secondary data from the 2010, 2014, 2018, and 2020 CFPS. The CFPS is funded by Peking University and the National Natural Science Foundation of China and reflects changes in Chinese society, economy, population, education, and health by tracking and collecting data from individuals, families, and communities in 25 provinces. The CFPS began in 2010 and is maintained by the Institute of Social Science Survey of Peking University. 53 Interviews in the four panels lasted from April to September 2010, from July to November 2014, from June 2018 to March 2019, and from July to December 2020. The interview guides used in these waves are provided in Supplemental Files 1–4.
The CFPS obtained informed consent from all participants involved in the studies and was approved by the Biomedical Ethics Committee of Peking University. The IRB approval number is IRB00001052-14010. 54 All statistical analyses were conducted using Stata version 15.1. 55
A total of 13,457 interviewees participated in the four panels. This study aimed to explore the relationship among older Chinese adults’ online behaviors, health habits, and health status. Thus, interviewees aged 60 years or older were included from the 2020 panel. A total of 5074 interviewees were included in the sample.
Variables
Explained variables
Health habits: Data concerning the continuous variable were obtained through summing the responses to six questions concerning health habits, which were related to dietary habits, physical activities, life habits, and sleeping habits. The questions were as follows: (1) Have you eaten meat in the past week? Meat includes flesh from pigs, cattle, sheep, chickens, ducks, other poultry, livestock, fish, shrimp, shellfish, and other aquatic products; (2) Have you eaten fresh vegetables or fruit in the past week?; (3) Do you have a napping habit at the moment?; (4) Have you smoked in the past month?; (5) Have you consumed alcohol three times per week in the past month?; and (6) How often have you participated in sports, fitness, and leisure activities over the past 12 months? The responses to the first five questions were binary, with one representing yes for questions 1–3 and representing no for questions 4 and 5. There were eight frequency responses to question 6: (1) less than once a month on average, (2) more than once a month on average, but less than once a week; (3) on average, 1–2 times per week; (4) on average, 3–4 times per week; (5) on average, 5 or more times per week; (6) once a day; (7) twice a day or more; and (8) never. Regular physical activity can significantly promote health status, which shows that within a certain frequency to do physical activity may have positive effects.33,38,56 Therefore, this study transformed categorical responses into a binary response to question 6, with one representing participation counted in a week, including rankings from 3 to 7 for the initial feedback; otherwise, the response was represented by zero for never participating or participating less than once a month. Therefore, the scores for health habits ranged between 0 and 6.
Self-rated health: The responses were obtained from the question “How do you measure your health”, which included five categories ranging from unhealthy to extremely healthy, represented by rankings ranging from 1 to 5.
Physical health: The responses obtained from four questions seeking to determine the interviewees’ physical condition and independence capabilities. The questions were as follows: (1) Have you been unwell and consulted a doctor about any illness in the past two weeks?; (2) Have you had a chronic medical condition diagnosed by your doctor in the past six months?; (3) Have you been hospitalized for illnesses in the past 12 months?; and (4) How many activities can you not perform independently, including outdoor activities, dining, preparing dinner, taking public transport, shopping, doing household chores, and doing laundry? Responses to the first three questions were binary, with one for the event that occurred and zero otherwise. Physical health was considered as a continuous variable that involved counting events that occurred in the four questions.
Mental Health: Response were obtained for this continuous variable through measuring how often the interviewees experienced these feelings: (1) I feel frustrated, (2) I find it difficult to do anything, (3) I do not sleep well, (4) I feel good, (5) I feel lonely, (6) I live happy, (7) I feel sad, and (8) I do not think that life can continue. The possible responses were hardly ever, sometimes, always, or most of the time. Negative feelings were measured from 4 to 1 for answers such as hardly ever, sometimes, always, and most of the time. Otherwise, the responses were measured in the opposite manner for positive feelings, ranging from 1 to 4. Finally, all the responses were summed.
Explanatory variables
Online behaviors
Recently access to the Internet: This variable was considered as binary, with the value being one if the interviewees accessed the Internet in the CFPS 2020 panel regardless of whether the device was a mobile device or computer; otherwise, the value was zero for no access to the Internet.
Online time: This variable measured time spent on the Internet. Responses were based on questions regarding the amount of time the interviewees spent online using a mobile device or computer. There are different devices available to interviewees to access the Internet; therefore, if interviewees had only used one device, either a mobile device or computer, to access the Internet, the Internet time would be shown. If the interviewees had used both mobile devices and computers to access the Internet, this study selected the longest Internet time between these two devices, and if the interviewees did not access the Internet, the Internet time was considered as zero.
Online duration: This variable measured the number of years the interviewees had consecutively accessed the Internet. If the interviewees had consecutively accessed the Internet since the CFPS 2010 panel, the values were 10; if since the CFPS 2014 panel, the values were 6; if since the CFPS 2018 panel, the values were 2; and if since the CFPS 2020 panel, the values were 1. If the interviewees had not accessed the Internet in these four panels or if they had accessed the Internet once but quit in some panels, the values were considered as zero. The online duration was used as a continuous variable.
Diverse applications: This continuous variable measured the number of online activities that the interviewees had experienced, including whether they had played online games, shopped online, watched any live online programs, took part in online learning in the last week, or used WeChat in the past year.
Information resources
Four categorical variables were included as information resources: television, the Internet, paper media, and broadcasting. Responses were obtained from a question regarding the importance of television, the Internet, paper media (e.g., newspapers, periodicals, and magazines), and broadcasting, which was coded from 1 to 5, ranging from no importance to utmost importance. Altogether, four binary variables were generated based on the weights of the responses, with 3–5 coded for the Internet, paper media, and broadcast as important information resources and 4–5 for television as an important information resource.
Control variables
Age range: The interviewees in this study were over 60 years old. To detect differences among ages, the study used four categories: 60–64 years old, 65–69 years old, 70–75 years old, and >75 years old.
Gender: Women may have a better health status than men. 26 Women were coded as one, and men were coded as zero.
Education: Higher educational attainment has positive returns on health.4,22 The educational qualification variable used in this study comprised four categories: illiterate and no schooling, elementary school, middle school, and beyond high school (college, bachelor's, master's, and PhD attainments).
Urban: Due to their typically low educational and material capital, individuals living in rural areas tend to rely on their health capital when investing in the labor market. Therefore, with the rapid depreciation of health capital, people living in rural areas have a poor health status. 27 Participants who living in urban areas were coded 1; those who live in rural areas are coded as zero.
Pension: Pensions are a financial resource for older adults. Greater financial resources not only allow individuals to adopt dietary habits that prevent diseases but also to engage in special health investments, such as vacations and physical activities to help ensure better health conditions, or to undertake regular body checks to help them control health risk factors. 27 Therefore, the annual pension amount was used as a continuous variable. If the interviewees had not yet received a pension, the values for the variable used the interviewees’ income.
Medical insurance: The continuous variable assessed the interviewees’ medical insurance status. Medical insurance included public medical insurance, urban employee basic medical insurance, urban resident basic medical insurance, supplementary medical insurance, new rural cooperative medical insurance, and basic medical insurance for rural and urban residents.
Social status: People of lower socioeconomic status tend to have a poorer work environment in relation to their health.6,27 Conversely, those with a higher socioeconomic status tend to have better health-related work environments. This inequality has been enlarged with the development of the economy and the improvement of medical technology. 38 The responses to the question “How do you measure your social status in the city in which you live?” were ranked from 1 (lowest socioeconomic bracket), 2 (lower middle socioeconomic bracket), 3 (middle socioeconomic bracket), 4 (higher middle socioeconomic bracket), and 5 (high socioeconomic bracket).
Family size: This continuous variable measured how many family members the interviewees had.
Coresidence size: This continuous variable measured the number of family members with whom the interviewees resided.
Mediating variables
Evaluation of online activities: Online activities are heterogeneous in terms of enhancing human, financial, and social capitals. Some Internet activities, such as educational and economic uses, are more capital enhancing than other activities, such as personal and social uses.48,50,57
Four categorical variables were used to measure the importance of online activities: entertainment, communication, learning, and life style. The questions were as follows: “How important are the activities of entertainment, activities of staying in touch with family and friends, activities of learning and getting information, and business activities for you when using the Internet.” The responses were ranked as 1 (no importance), 2 (low importance), 3 (neutral), 4 (some importance), and 5 (utmost importance).
Online activity evaluation was used in the path analysis of the SEM model to measure the mediating effects: first, between the older Chinese adults who had recently accessed the Internet and the effects on their health habits and health conditions; second, between the older Chinese adults with disparities in online duration and the effects on their health and health conditions.
Results
A statistical summary is presented in Table 1. On average, the older Chinese adults had four health habits. Self-rated health responses indicated that most participants perceived their health as either healthy or relatively healthy. Physical health was a negative variable, with the results indicating that the unhealthier the event, the worse the physical condition of the older Chinese adults. On average, the older Chinese adults experienced no more than one unhealthy event. On average, the mental health score was 26.40, indicating a relatively positive mental condition.
Statistical summary.

Concerning the older Chinese adults’ online behaviors, 17.50% of the interviewees had access to the Internet in the CFPS 2020 panel, spent about 20 min a day online, and used no more than one online application.
Specifically, four age cohorts were weighed equally in the sample. Gender was equally distributed in the sample, while 67.6% of the interviewees were illiterate and no schooling, or had elementary schooling. The average annual post-tax pension was 5345.44 yuan. Nearly half of the interviewees could be considered middle class. On average, there were three people in a family, and the older Chinese adults typically resided with one member at home. The average number of medical insurances that these older adults owned was one. Most associations between the control variables and the four dependent variables were statistically significant (p < 0.10), as determined by the correlation analysis and chi-square tests. However, no significant relationships were found between (1) social status and physical health or (2) family size and health habits.
As shown in Table 2, the older Chinese adults who had recently accessed the Internet had positive associations with health habits and health status on average; specifically, they showed enhanced health habits (0.093 units) and mental health (0.403 units) and decreased in the occurrence of negative physical events (0.176 units). Additionally, those who recently accessed the Internet had 1.212 times higher odds of reporting better self-rated health than nonusers. After controlling for control variables, this effect slightly decreased, with 1.077 times higher odds of being in a better self-rated health category.
Estimated OLS and ordered logit regression coefficients concerning the online behaviors of older Chinese adults for predicting their health habits and health status.

Note. *** p < 0.01, ** p < 0.05, * p < 0.10. Robust cluster standard errors are indicated in the parentheses. The reference categories were no access to the Internet, and television, the Internet, paper media, and broadcasting not as important information resources. The complete table (Supplemental Table 1) is provided in the supplementary material.
However, time spent online showed no clear effect on health. Prolonged access to the Internet over many years had insignificant but positive associations with mental health conditions, with an effect size of 0.038 units. The diverse use of Internet applications helped the older adults develop health habits and better mental health, with effect sizes of 0.063 and 0.246 units, respectively. Notably, the four information resources worked differently: if the main information resource was television and broadcasting, these older adults showed positive associations with more health habits, better self-rated health, and improved mental health conditions; however, by relying on the Internet, the older adults showed positive associations with more health habits but decreasing levels in terms of their mental health conditions. In particular, when the older adults’ main information resource was television, their mental condition on average was enhanced by 0.898 units, but decreased by 0.549 units when they relied on the Internet as the main information resource. When the control variables were included in the models, the coefficient of determination increased, which indicated the increased strength of the relationship between the independent and dependent variables. The complete table (Supplemental Table 1) is provided in the supplementary material.
Propensity score matching was applied to assess the relationship between the older adults who had recently accessed the Internet and their health habits and health status, with the results presented in Table 3. The balance diagnostics (Supplemental Table 2) are provided in the supplementary material. In most cases, there were no statistically significant differences in the means of the covariates between the treatment and control groups after matching. The results showed that, compared to the older adults who had not accessed the Internet recently, the older adults who had recently accessed the Internet enhanced their health habits between 0.1889 and 0.2386 units, their self-rated health between 0.0891 and 0.0964 units, their physical health between −0.2083 and −0.0937 units, and their mental health between 0.4234 and 0.6640 units. When considering the results from the OLS and ordered logit regression, the finding that the older adults who had recently accessed the Internet exhibited improved health habits and better health status than the older adults who had not can be considered robust.
Results from propensity score matching (PSM) concerning older Chinese adults who had recently accessed the internet for predicting their health habits and health status.

Note. *** p < 0.01, ** p < 0.05, * p < 0.10.
Structural equation modeling was applied to check robustness and analyze the mediating effects between the older Chinese adults’ online behaviors and their health habits and health status. The results of the multivariate normality test showed that the distribution of the model did not follow multivariate normality. Therefore, the maximum likelihood method was applied to the models, and robust estimates were used.
Table 4 presents the standardized estimates with maximum likelihood and robust cluster standard errors. The model fit evaluations showed that the standardized root mean squared residual was 0.03 (below 0.08), indicating a good fit. Recent Internet access was positively associated with enhancing the older Chinese adults’ health habits and health status. Longer years of Internet access insignificantly enhanced the older adults’ mental health conditions. In summary, the results of the SEM analysis were consistent with those of the OLS and ordered logistic analyses.
Estimated structural equation modeling (SEM) coefficients concerning the online behaviors of older Chinese adults for predicting their health habits and health status.

Note. *** p < 0.01, ** p < 0.05, * p < 0.10. Standard beta coefficient. Robust cluster standard errors are indicated in the parentheses. The reference categories were no access to the Internet, television, the Internet, broadcasting, and paper media not as important information resources, >75 years old, men, and rural living. SRMR < 0.08, is regarded as a good fit.
CD: coefficient of determination; SRMR: standardized root mean squared residual.
The mediating effects were considered separately for the two models. Four online preferences were used to examine how recent or long-term Internet access affected the older Chinese adults’ health habits and health status. Table 5 presents the significant mediating pathways. The Sobel test was used to assess the significance of mediation effects, revealing statistically significant indirect effects at the 10% level. Bootstrapping estimates with 400 replications (Supplemental Table 3) presented these similar significant mediating effects. If the older Chinese adults had recently accessed the Internet, their health habits and health status showed improvement. However, due to a preference for communication and learning, the positive effects of recent Internet access on health habits decreased. The negative mediating effects of online communication and learning on the health habits of the older adults may be due to Internet overuse and its impact on sleep habits, which are closely related to time. However, through preferences for life style activities, the effects of recent Internet access on physical condition were positive. Furthermore, when the older Chinese adults had access the Internet over the long term, the negative indirect effects from the preferences for communication and learning produced an overall negative effect, indicating that prolonged access to the Internet could decrease health habits as online communication and learning activities were prioritized. The negative indirect effects of life style preferences may have helped enhance the older adults’ physical conditions. However, the direct effects of online duration on health habits and physical health were very small. However, large effects are not the only way to demonstrate the effect is important. Small effects may have enormous implications in the practical context, and small effects in ongoing process may accumulate over time to become large effects. 58
Mediating effects experienced by older Chinese adults who had recently accessed the internet and online duration on their health habits and health status.
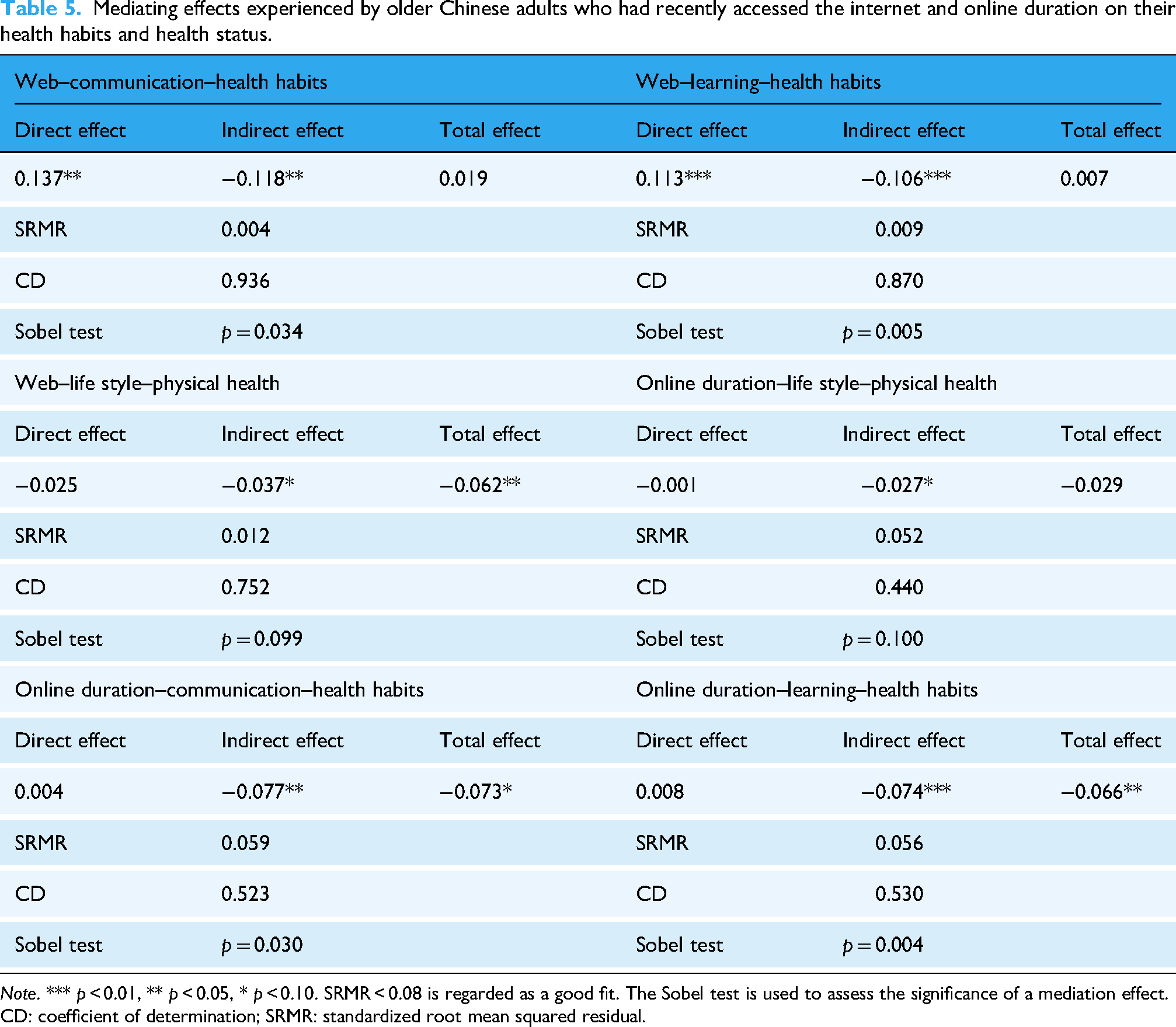
Note. *** p < 0.01, ** p < 0.05, * p < 0.10. SRMR < 0.08 is regarded as a good fit. The Sobel test is used to assess the significance of a mediation effect.
CD: coefficient of determination; SRMR: standardized root mean squared residual.
Discussion
The results concerning the effects of older adults’ access to the Internet, as a measurement of Internet use, on their health status, including self-rated health, physical health, and mental health, were consistent with previous studies.7,10 Furthermore, the older adults’ access to the Internet was positively associated with their health habits, including dietary habits, physical activities, life habits, and sleep habits. However, consecutive access to the Internet counted in years did not yield year-difference effects on health habits or health status, as anticipated. A longer online duration may lead to longer time spent online and diverse use of online applications, highlighting online users’ competency in digital literacy. 49 The main reason for this inconsistent result is that the older Chinese adults’ physical function naturally declines with aging. Therefore, the effects of aging may have obscured the positive relationship of consecutive Internet access.
According to digital capital theory, connectivity and time spent online represent aspects of digital access, while information literacy and communication skills fall under digital competence. As both digital access and competence increase, individuals accumulate digital capital. However, this capital interacts differently with other forms of capital, social, personal, political, economic and cultural, rather than integrating uniformly. Positive interactions between digital and cultural capital allow individuals to access health-related and educational resources online and apply acquired cultural knowledge in social settings, thereby influencing their health status. Similarly, when digital capital interacts positively with personal capital, it has enabled individuals to, first, enhance self-esteems and, second, develop a creative and healthy lifestyle. 46 Furthermore, the study shows that self-determination theory and health empowerment synergistically support psychological motivation in the reuse process.
Positive associations between Internet use and older adults’ health have been reported using multicountry datasets. There was a positive relationship reported between Internet use and the mental well-being of retired older adults in the United States, where Internet use reduced the probability of a depressive state by one third. 59 Using the Internet has been positively associated with decreasing older adults’ loneliness in Alabama, in the United States. 60 In a European study, Internet use has been reported to be a useful way to reduce social isolation and increase self-reported life satisfaction. 61 Compared to non-users, Internet users who are beyond 60 years old in Brazil presented a 21% greater prevalence of positive self-rated health. 29 Findings in Europe have shown that Internet use by older adults has a positive relationship with cognitive functioning and can enhance self-care by online communication with health professionals.62,63 As for the long-term effects of Internet use on health, American older adults’ access to the Internet has been positively associated with promotion of cognitive function at a certain wave length and negatively associated with cognitive decline over time. 64 One study distinguished Portuguese older adults’ Internet use behaviors into two categories: experienced Internet users (more than 10 years) versus nonusers, and frequent Internet users (less than 14 h per week) versus nonusers. The results showed that being an experienced Internet user and a frequent Internet user were positively related to health-related quality of life and physical function over time. 65
However, the negative impact of Internet overuse on health cannot be ignored. A reverse U-shaped relationship found between the intensity of Internet use and health shows that it first increases one's health status, but in the case of overuse, health status deteriorates, and risks of loneliness increase.6–8 In the current findings, the total positive impact of Internet access on habits is offset by the use of online communication. Long-term exposure to online communication may increase the risk of sedentary behavior and decrease opportunities to exercise. While digital capital tends to accumulate through long-term Internet use, the conversion of digital capital into other forms of capital (e.g., social, economic, personal, political, cultural) is uneven. For example, frequent online communication can strengthen social capital. However, excessive use may negatively impact the interplay between digital capital and both personal and cultural capital. Moreover, internet overuse can foster addiction, ultimately resulting in incompatibilities. 47 Incapabilities mean limited chances to enhance self-esteem from using ICTs, develop a healthy lifestyle, and reuse the resources acquired online to the social realm. 47 Therefore, excessive online engagement could negatively affect physical and mental well-being.
Digital technology oriented toward older adults is a viable means to address the negative effects of aging. For example, intelligent systems for older adults facilitate connection to digital technology and care. By utilizing wearables and smart home devices, relevant intelligent systems for older adults can specifically detect their practical demands and provide supply-related and integrated services.66,67 These demands encompass grocery shopping, cooking, cleaning, health care, and other life issues. 68 Furthermore, intelligent systems for older adults can facilitate their home care by saving on institutional care costs and providing psychological, interpersonal, and spiritual services for older Chinese adults to support their emotional needs. 66 Currently, Chinese citizens are familiar with the realities of digital society, and with the increasing rate of Internet penetration among older Chinese adults, intelligent systems for older adults have become an efficient means to enhance healthy aging. The demand for online health-related information and communication among older Chinese adults is increasing, which is likely to attract more older adults to become netizens. However, there are some issues in relation to older Chinese adults’ Internet access. They are slow to adopt online health information, lack digital literacy, and have limited ability to search for online health information.3,23
Therefore, the primary challenge is bridging the digital divide among older Chinese adults. Age is the main factor contributing to the digital divide. Age-related senescence, illness, and a decline in cognitive ability and memory affect older adults’ Internet use.2,69 Anxiety and fear regarding digital knowledge are obstacles for older adults who are otherwise willing to access the Internet. 70 Consequently, policies are needed to encourage age-friendly applications. Design norms for age-friendly websites and relevant mobile applications can be used to guide services and techniques. Based on design norms, age-friendly applications have enlarged fonts, icons, buttons, volume, simplified interfaces, structures, functions, and operations to satisfy the needs of older adults.1,71 Furthermore, social support is essential to encourage older adults to access and use the Internet. 70 Sufficient support from older adults’ children has different effects on bridging the digital divide among older adults. If the acquisition effect works, older adults can access the Internet with the help of their children, bridging the digital divide; otherwise, if the agent effect works, older adults rely on their children to access the Internet, enlarging the digital divide. 2 After removing technical obstacles, older adults could participate in training at universities to enhance their digital literacy.
Online users typically remain unaware of how digital platforms and other users compete for data. Indeed, online users are sometimes unaware of whether their data have been collected and who has collected it. 72 When older Chinese adults access the Internet, they may encounter data protection issues, and due to a lack of digital literacy, they may risk exposing private information. 3 Intelligent systems for older adults are also driven by data; therefore, data protection is essential for the further development of such intelligent systems.66,73 Since 2012, a private information protection system has been in use in China, involving a requirement for legal, justifiable, and informed consent. 72 Strengthening data and privacy protection of older Chinese adults, for example, through guaranteeing such adults’ rights to consent, participation, and development, can promote the development of digital care. 73
The contributions of this study are twofold. First, it analyzed the effects of Internet use by older Chinese adults on their health habits and health status. Second, the study recognized that accessing information is considered a basic skill. 28 Unlike most research, which relies on data from one-time cross-sectional surveys and pays limited attention to the digital divide's trends, 23 this study's measurements of Internet use were extensive in terms of assessing access to the Internet, time spent online, and diverse use of online applications. Notably, to present trends in Internet use, online duration was measured by analyzing the older adults’ Internet access over the last ten years consecutively.
This study had some limitations. First, some measurements were self-reported by the older adults, which introduced subjectivity and possible recall bias. Second, this study selected online behaviors to describe the older adults’ ability to use the Internet. However, the skills involved were basic. Therefore, skills related to digital literacy should be covered in future studies to fully understand the different effects of online behaviors on older adults.
Conclusion
This study examined the relationship between older Chinese adults’ online behaviors and their health habits and health status. These findings indicate that older adults who recently accessed the Internet were more likely to report healthier habits and better health outcomes compared to those who did not have access. These results fully support Hypothesis 1. In contrast, hypothesis 2, which proposed that older adults with longer durations of Internet use would exhibit better health habits and health status, is partially supported. While extended Internet use showed a positive association with mental health. However, older adults who engaged in a more diverse range of online activities were more likely to demonstrate healthier behaviors and improved health outcomes. Notably, the type of online activity mattered. Older adults who prioritized lifestyle-related Internet use experienced improvements in physical health, whereas those who prioritized online communication exhibited weaker associations with health-promoting behaviors.
These findings suggest that Internet access may serve as a valuable tool to promote healthy aging by facilitating access to health information and encouraging health-supportive behaviors. However, the heterogeneous effects of various online behaviors underscore the importance of targeted digital interventions. Rather than promoting general technology adoption, policies, and programs should be tailored to guide older adults toward productive and health-enhancing forms of Internet use.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251359130 - Supplemental material for The effects of older Chinese adults’ online behaviors on their health habits and health status
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251359130 for The effects of older Chinese adults’ online behaviors on their health habits and health status by Shu Liu in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251359130 - Supplemental material for The effects of older Chinese adults’ online behaviors on their health habits and health status
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251359130 for The effects of older Chinese adults’ online behaviors on their health habits and health status by Shu Liu in DIGITAL HEALTH
Supplemental Material
sj-pdf-3-dhj-10.1177_20552076251359130 - Supplemental material for The effects of older Chinese adults’ online behaviors on their health habits and health status
Supplemental material, sj-pdf-3-dhj-10.1177_20552076251359130 for The effects of older Chinese adults’ online behaviors on their health habits and health status by Shu Liu in DIGITAL HEALTH
Supplemental Material
sj-pdf-4-dhj-10.1177_20552076251359130 - Supplemental material for The effects of older Chinese adults’ online behaviors on their health habits and health status
Supplemental material, sj-pdf-4-dhj-10.1177_20552076251359130 for The effects of older Chinese adults’ online behaviors on their health habits and health status by Shu Liu in DIGITAL HEALTH
Supplemental Material
sj-docx-5-dhj-10.1177_20552076251359130 - Supplemental material for The effects of older Chinese adults’ online behaviors on their health habits and health status
Supplemental material, sj-docx-5-dhj-10.1177_20552076251359130 for The effects of older Chinese adults’ online behaviors on their health habits and health status by Shu Liu in DIGITAL HEALTH
Footnotes
Ethical considerations and consent to participate
China Family Panel Studies have obtained informed consent from all participants involved in the studies. For participants aged 15 and above, they signed the informed consent form themselves. China Family Panel Studies have been approved by the Biomedical Ethics Committee of Peking University. The IRB approval number is IRB00001052-14010.
Author contributions
Shu Liu has made all contributions to this research, including conceptualization, methodology, writing the original draft, and reviewing and editing the final version. The author has read and agreed to the published version of the manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets presented in this research can be found on the China Family Panel Studies, Peking University Open Research Data website (http:// 10.18170/DVN/45LCSO).
Permission to reproduce material from other sources
All materials used in this research are publicly available data that have been meticulously cited.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.