
Abstract
Objective
Nursing students face increasing challenges, making it crucial to explore innovative teaching methods such as virtual reality simulations to enhance skills. This study aimed to assess their preferences for virtual reality simulation in skills training using a discrete choice experiment.
Method
A discrete choice experiment with six attributes (types of virtual reality, interaction, learning contents, collaboration, frequency, and costs for each additional training module) was used. A mixed logit model and latent class analysis were adopted to analyze data using Sawtooth Software and STATA BE 18.
Result
A total of 518 undergraduate nursing students completed this study. They identified costs for each additional training module, interaction, and types of virtual reality as the three most important attributes. The combination that was most preferred was immersive virtual reality simulation, high-level interaction types, advanced learning contents, mixed learning modules, lower prices, and a practice frequency of once every two weeks. Two classes of students were identified: Class 1 valued the cost for each additional training module, while Class 2 preferred a better immersion experience.
Conclusion
Students’ preference for virtual reality simulation depended on some factors, including types of virtual reality, interaction, learning contents, and costs for each additional training module. Nursing educators should take students’ preferences into account to ensure that their preferences and needs are addressed as fully as possible.
Introduction
Nursing is a discipline focused on practical skill application, in which a nurse's lack of practical skills is perceived negatively by colleagues and managers and will pose a risk to patient safety. 1 As nursing students, they were aware of the importance of practical skills in clinical settings and often felt anxious about proficiency in this area. 1 In the current medical environment, a significant challenge was faced in preparing nursing undergraduate students to become safe practitioners. 2 The scarcity of quality clinical practice was exacerbated and became a pressing issue due to the growing nursing and faculty shortages, increased competition for internships, and the increasing number of acute patients. 2 This placed a challenge on nursing educators to create chances to practice and integrate students’ knowledge and skills, equipping them for the complexities of the modern healthcare system. 3 It was called to identify and evaluate the effectiveness of emerging technologies, such as virtual reality simulation, for teaching nursing skills. 4
Simulation refers to learning in which real-life clinical situations are augmented, simulated, or replaced by simulation. 5 Clinical simulations could take many forms, including role-playing, high- and medium-fidelity manikins, virtual reality, partial task trainers, and standardized patients. Even though mannequin-based simulation labs were widely used in nursing programs, other forms of simulation were becoming increasingly popular, especially for virtual reality simulation. 6 In virtual reality simulations, students were partially immersed in a virtual learning environment (e.g. screen, phone, computer, tablet, etc.), aiming to foster a perceived lived experience and achieve a certain outcome (e.g. learning and entertainment). 7 The results of the meta-analysis indicated that it effectively enhanced nursing students’ practical skills, theoretical knowledge, and skill retention compared to traditional teaching methods. 6 In nursing education, virtual reality simulation could offer an alternative and superior potential to traditional methods that were more expensive and less flexible.6,8 Conventional teaching methods incurred higher costs due to the significant need for consumable resources and environmental construction. Student practice sessions were also hindered by the necessity of reusing materials due to a material shortage. 3 On the contrary, virtual reality simulation had several advantages, including saving material resources without the requirement of any consumables, providing chances to practice nursing skills repeatedly, saving human resources (i.e. teacher supervision), and saving students’ waiting time to practice. 3 Furthermore, the cost-utility analysis indicated that virtual simulation demonstrated a more favorable cost-utility ratio of $1.08 compared to that of mannequin-based simulation ($3.62), 9 while it was also less time-consuming to solve a virtual case (28.73 minutes per student) than a mannequin-based simulation. 10 Nonetheless, in terms of virtual reality simulations, little is known about students’ priorities and needs for virtual reality simulations.
The discrete choice experiment (DCE) is a utility method that is widely used to measure preferences for technology and healthcare services, which allows participants to rank the importance of various attributes of an intervention. 11 The multiattribute choice tasks of DCE can mimic decision-making scenarios in the real world and help to predict individual behavior. Therefore, this study aimed to investigate undergraduate nursing students’ preferences for virtual reality simulations in nursing skills training, which can promote the effective application of virtual reality simulations and provide educators with distinctive references to design skills training programs.
Method
This study used a discrete choice experimental approach to measure undergraduate nursing students’ preference for virtual reality simulations in nursing skills training. The DCE was a stated preference technique that simulates real decision scenarios, which was widely employed for eliciting preferences in the field of nursing.12–14 We conducted the survey design, data collection, and statistics analysis according to the International Society for Pharmacoeconomics and Outcomes Research Guidelines. 15 This DCE was reported according to the DIRECT Checklist (A Reporting Checklist for Discrete Choice Experiments in Health). 16 The whole experiment process is shown in Figure 1.

Process of identifying attributes and levels for the discrete choice experiment.
Survey design
Identifying attributes and levels
Firstly, according to the purpose of this study, we developed the search strategy and conducted a scoping review in PubMed, which yielded a total of 272 publications, the search strategy is shown in Supplemental Appendix 1. Non-peer-reviewed articles, studies not concerning virtual reality simulations, or nursing students’ perspectives were excluded, the screening flow is shown in Figure 1. Sixty-two articles were finally included and these studies provided a wide range of perspectives on nursing students’ views on training using virtual reality simulations. Secondly, qualitative research 17 has already been conducted to richly describe nursing students’ perception and experience with virtual reality simulations in the field of nursing skills training. Then, we selected preliminary characteristics related to virtual reality training after content analysis of the included literature. Thirdly, expert consultation was conducted to discuss the relative importance of characteristics. The expert panel members consisted of nursing faculty from the university, virtual reality technologists, clinical nursing experts, health economics experts familiar with DCE, and nursing student representatives. Their diverse backgrounds had the potential to ensure a comprehensive and objective discussion. All members received a detailed pair of background materials prior to the meeting and an introduction to the study's topic at the beginning of the meeting to ensure a clear understanding of the study's purpose and methodology. They selected the attributes, ensured that each level was clearly defined, and revised the wording to better fit the nursing educational context. This process resulted in the selection of six attributes, each comprising two to four levels (Table 1).
List of virtual reality simulation characteristics and levels.

L1: level 1; L2: level 2; L3: level 3; L4: level 4.
Experimental design and construction of choice tasks
A well-designed DCE is essential for assessing nursing students’ preferences for different attribute levels and understanding their impact on the selection of virtual reality simulations in nursing skills training. Given the numerous possible hypothetical options (i.e. 2 × 34 × 4 = 648), we adhered to the principles of balance and independence to design the choice tasks. Participants were randomly assigned pre-constructed versions of the random tasks. Additionally, two fixed tasks were incorporated to enhance the reliability and accuracy of the responses, administered as the first and 12th tasks for all participants. In total, participants were asked 12 choice tasks (i.e. 10 random and two fixed).
DCEs are designed to simulate real-world decision-making scenarios. Therefore, to introduce participants to the simulation context before presenting the choice tasks, we included the following statement, that is, “Please imagine that your school is now offering virtual reality simulations, and you are considering which one to choose for nursing skills training. We will present you with various types of virtual reality simulations, and you will be asked to select the one you would prefer to use.”
Questionnaires
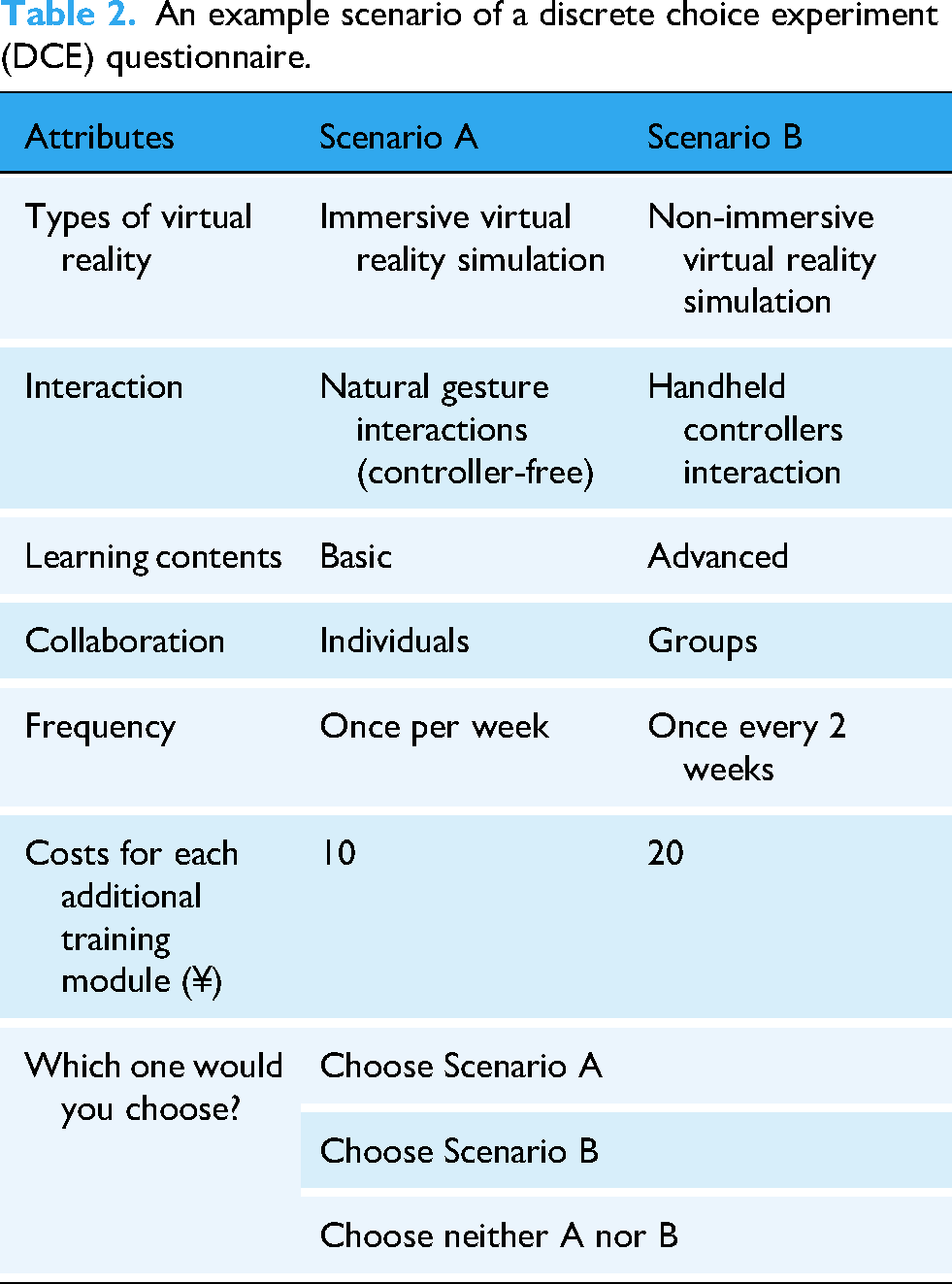
The questionnaire was divided into two sections: the first part was DCE choice tasks and the second part was about basic information including age, gender, and grade point average. We used Lighthouse Studio version 9.15.6 (Sawtooth Software) to generate online questionnaires. A pilot investigation was performed among 11 target participants (i.e. undergraduate nursing students) prior to the formal data collection process to refine language and confirm acceptability. The example scenario of the DCE choice question is shown in Table 2. The full questionnaire can be viewed in Supplemental Appendix 2.
An example scenario of a discrete choice experiment (DCE) questionnaire.
Data collection
This cross-sectional DCE was conducted from April to July 2024. Data were collected from undergraduate nursing students enrolled at two universities in Guangdong Province, China, using convenience sampling. Participants completed an online questionnaire administered by researchers who introduced the study and provided clarifications as needed. The inclusion criteria were (1) undergraduate nursing students and (2) age 18 or older. Participants who were absent for > 10% of the total class hours were excluded from the study. Ethical approval for this study was obtained from the Ethical Review Board of Jinan University (Approval No. JNUKY-2022-034). An online written consent was obtained before proceeding to the DCE tasks.
The sample size for this DCE was determined using the following formula:18,19
The sample size (N) of the DCE main effect was determined by the selection tasks (t = 12), the alternatives (a = 2), and the maximum number of levels for any attribute (c = 4); we calculated that the sample size required for this study had to be > 83.
Statistical analysis
The DCE was chosen to estimate undergraduate nursing students’ preferences for different attributes of adopting virtual reality simulations in nursing skills training and to understand how different levels of these attributes influence respondents’ decision-making. A mixed logit model (MLM) was employed, offering the advantage of accommodating random coefficients, thereby capturing individual-level preference variations more effectively than other models. The estimated parameters (β) in the analysis indicate the direction and magnitude of the effect of each attribute level on the probability of choice. By standardizing the parameter estimates, the relative importance of each attribute was calculated. The willingness to pay (WTP) for non-monetary attributes is estimated by the ratio of the parameter estimates for non-monetary and monetary attributes. We also conducted a subgroup analysis using a mixed logit model to examine differences across academic years. To ensure an adequate sample size, first- and second-year students were combined into one group, while third- and fourth-year students were combined into another. Group differences were assessed by comparing the regression coefficients (β) between the two subgroups. Similarly, the differences between students with and without virtual reality were investigated using a subgroup analysis.
To identify distinct subgroups of respondents with similar preferences, we adopted the latent class analysis (LCA). Each subgroup was assumed to have its own set of parameters, allowing for a more nuanced understanding of preference heterogeneity.
All statistical analyses were performed using Sawtooth Software (Provo, UT, USA) 20 and Stata BE 18 (StataCorp LLC, College Station, TX, USA).
Result
Respondent characteristics
A total of 553 students responded to the link of this online survey (a respondent rate of 97.3%), and 540 completed the questionnaire. Twenty-two respondents were excluded due to the choice of a significantly less attractive option when facing fixed choices.
The mean age of the participants was 20.43 years, with a predominance of females comprising 84.17% of the sample. Additionally, a greater proportion of participants were in their first year of university (40.73%), compared to other academic years. More than half of the students come from rural areas and are balanced in terms of family income. In terms of grades, 42.08% of respondents had a grade point average (GPA) of 3.00–3.49, with the lowest percentage of students having a CGPA ≤ 2.50 (5.21%) and ≥ 4.00 (9.07%). The majority of nursing students (82.82%) wanted to be a nurse after graduation, while 17.18% did not plan to become nurses. Table 3 presents the respondents’ demographic characteristics.
Demographic characteristics of undergraduate nursing students.

SD: standard deviation.
MLM results
Table 4 shows the results of MLM analysis, which indicates that types of virtual reality, interaction, cost for each additional training module, and learning contents were all significantly associated with nursing students’ preference for using virtual reality simulations in nursing skills training, in addition to collaboration mode and training frequency. The relative importance of each attribute was prioritized as follows: costs for each additional training module, interaction, types of virtual reality, collaboration, learning contents, and frequency. A visual presentation of the estimated preference weights is provided in Figure 2.

The visual presentation of the estimated preference weights.
Results of the mixed logit analysis for virtual reality simulation preferences (N = 518).

SE: standard error; 95% CI: 95% confidence interval; p: p-value.
The currency exchange rate of ¥1 = US$0.138 is applicable.
The cost for each additional training module was significantly important to nursing students (β = −0.05, p = 0.000), with the negative coefficient indicating that a lower cost would be preferred. They preferred immersive virtual reality simulation to non-immersive virtual reality simulation (β = 0.37, p = 0.000), and they preferred high-level interaction types (natural gesture interaction: β = 0.24, p = 0.003) rather than interacting through handheld controllers (β = −0.15, p = 0.036) or touches. The students were inclined to use virtual reality simulations for nursing skills training in advanced learning contents (β = 0.18, p = 0.015), instead of moderately complex contents (β = 0.02, p = 0.759). As for collaboration, nursing students seemed to prefer mixed learning modules rather than group-based learning, although it did not reach statistical significance (groups: β = −0.14, p = 0.052; mixed: β = 0.12, p = 0.074), and the preference for frequency showed a similar pattern.
The subgroup analysis was performed using an MLM, with students categorized into two groups: first- and second-year students as one group, and third- and fourth-year students as another. The results of the subgroup analysis are presented in Supplemental Appendix 3. Findings indicate no significant differences between the two groups (p > 0.05). Subgroup analyses revealed divergent preferences between virtual reality experience groups (Appendix 4). While most parameters showed no significant differences (p > 0.05), students with virtual reality experience preferred a group learning approach (p = 0.026), while students without virtual reality experience preferred a mixed approach (p = 0.001).
Latent class analysis
We fitted the models for two to five classes respectively. Bayesian information criterion (BIC) was minimized when categorized into three classes. However, when compared to two-classification, this reduction appears minimal, which means that a suitable number of subgroups has been reached at two-classification; 21 Akaike information criterion (AIC) showed a continuous decreasing trend, and this trend also slowed down as the number of groups increased (Table 5). It is necessary to also evaluate from a practical point of view when determining the number of classifications in an LCA, to ensure that the resulting subgroups are not only mathematically reasonable, but also make sense in practical applications. By comparing the different model fit metrics as well as professional interpretability, 22 the model of two categories was chosen for the best statistical fit.
Performance value of models with different number of classes.
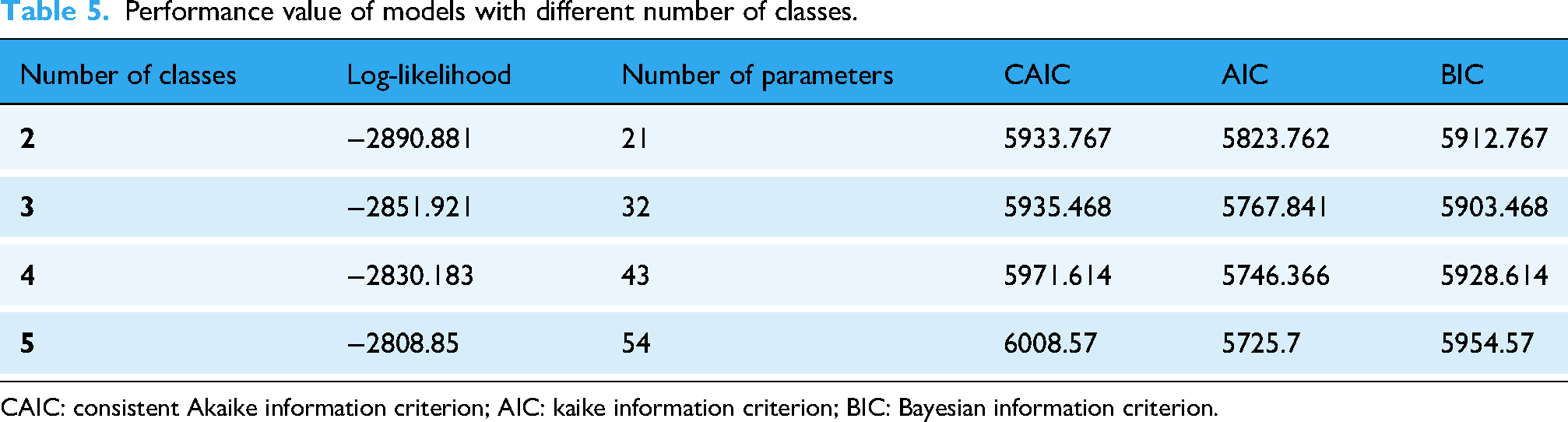
CAIC: consistent Akaike information criterion; AIC: kaike information criterion; BIC: Bayesian information criterion.
Nursing students from Class 2 showed a preference for immersive virtual reality simulation, willing to pay $2.58 (p = 0.000) in exchange for a promotion from non-immersive to immersive virtual reality simulation (Table 6). In addition, Class 2 also showed a greater preference for virtual reality simulations with natural gesture interactions (WTP=$1.98, p = 0.001). In contrast to Class 2's significant preference for immersive experiences, Class 1 had no such preference (p > 0.05, respectively). In terms of learning contents, nursing students from Class 1 respondents needed to be compensated $0.01 before they were willing to accept the advanced level, while Class 2 was willing to pay $1.17 for the advanced level. Overall, Class 1 valued the cost for each additional module, while Class 2 preferred a better immersion experience.
Estimation results of marginal willingness to pay for each class.

WTP: willingness to pay; SE: standard error. All monetary values in this table are expressed in Chinese Yuan (¥).
Discussion
According to our knowledge, this was the first DCE to explore preferences for virtual reality simulation among nursing students. According to the findings of this study, students’ preference for virtual reality simulation depended on types of virtual reality, interaction, learning contents, and costs for each additional training module. The combination that was most preferred was immersive virtual reality simulation, high-level interaction types, advanced learning contents, mixed learning modules, lower price, and a practice frequency of once every 2 weeks.
We found that undergraduate nursing students preferred immersive virtual reality simulation to non-immersive virtual reality simulation. The possible reason was that students rated immersive virtual reality simulation quite positively since, by providing immersive interactivity, immersive virtual reality simulation could effectively eliminate the monotony of traditional teaching and rigid methodologies, increasing nursing students’ enthusiasm for learning and enhancing their practical skills. 23 The increasing popularity of virtual worlds as a tool in nursing education reflected the fact that the current tech-savvy generation of students (i.e. “Net Generation,” born after 1982) was born into a digital era and was accustomed to learning in virtual simulations. 24 It was demonstrated that the operational, immersive, and interactive features of virtual reality were more effective than 3D videos in improving students’ retention and comprehension of knowledge. 25 Virtual reality simulation can be divided into two types, including desktop virtual simulation (also named non-immersive virtual reality simulation) and immersive virtual reality simulation. The former required users to use a mouse, touchscreen, keyboard, or joystick to interact with a computer monitor-based environment, while the latter equipped users with an array of sensory output devices like a head-mounted device. 26 Immersive virtual reality simulation offered a higher level of interactivity than non-immersive simulation by eliminating many real-world visual cues and incorporating sensory stimuli that matched the virtual setting, enabling users to become fully engaged in the experience. 27 Currently, non-immersive virtual reality simulations outnumbered immersive virtual reality simulations. 8 Although undergraduate students preferred immersive virtual simulation teaching, the effectiveness of non-immersive teaching seemed to be better. The meta-analysis results indicated that virtual reality simulations focused on patient management, featuring multiple scenarios with non-immersive experiences, lasting over 30 minutes, and including post-scenario feedback proved to be more effective.27,28 This phenomenon might be caused by technological challenges, cybersickness, 29 and increased cognitive load as students had to pay attention to unrelated immersive stimuli. 30 Although most participants have to stop using fully immersive virtual simulation within 10 minutes, and the symptoms of cyber sickness were significantly higher than in non-immersive environments, immersive virtual simulation was still suitable for situations like nursing skills training that did not require fast movements. Moreover, it is undeniable that immersive virtual simulation is more interesting and enjoyable. 31 And adjusting technical parameters such as field of view, frame rate, image resolution, and bit rate of virtual reality projections also helps improve the issue of cyber sickness in immersive virtual simulations. 31
In this study, we found that undergraduate nursing students were inclined to use advanced learning content in virtual reality simulation, rather than moderately complex content. Practical skills were emphasized in clinical settings, and nursing students understood the importance of these skills as well. 1 Through technologies like artificial intelligence and virtual reality, students hoped to experience cases that were difficult to encounter during traditional internships or observations.17,32 Because of the deterioration of nurse-patient relationships and concerns about patient safety, nursing students have fewer chances for hands-on patient care and clinical practice. 33 With virtual reality simulation, nursing students could engage in immersive and interactive encounters, reenact actual clinical scenarios, and gain hands-on training while avoiding direct contact with patients. 6 In addition to saving clinical nurses’ valuable time, it alleviated the predicaments related to traditional patient interaction in the field of education, thus helping to resolve the shortage of clinical educational materials.6,34 For example, rapidly deteriorating patients are seldom encountered during clinical internships. The students of a mixed study expressed that virtual reality simulations helped them prioritize effectively, improved their anxious symptoms, filled gaps in their learning, and encouraged them to engage in self-directed learning in a “low-risk” environment. 35 Virtual reality simulation not only had the potential to enhance student's ability to manage diverse clinical patients but also offered a safe platform for applying theoretical knowledge to practice through simulated cases. This enables them to provide care for virtual patients within a simulated environment, practicing and enhancing various skills, such as communication behaviors and prioritization.35,36
Future implications for nursing education
As nursing programs continue to adopt innovative teaching strategies, virtual reality-based training offers an interactive, immersive, and safe environment for students to develop essential clinical skills. The findings of this study highlighted that the student's preferences for the type of virtual reality and interaction modes vary, and designing flexible and adaptable virtual reality simulation modules can enhance engagement and learning outcomes if these differences can be taken into account.
Beyond virtual reality simulations, other teaching methodologies, such as distance learning, are on the rise 37 and supported by digital technologies, including virtual reality.38,39 A hybrid approach that integrates virtual reality simulation-based skills training with distance learning modules is demonstrated to positively influence students’ academic performance and diverse educational variables as it allows students to acquire theoretical knowledge remotely while engaging in immersive skill-based simulations for hands-on practice. 38 Future research should assess the long-term impact of virtual reality simulations on clinical competency and patient care outcomes, as well as explore best practices for integrating virtual reality simulation with other active teaching methodologies in different nursing education settings.
Limitations
This study had serval limitations. Firstly, the two universities involved in this study do not currently integrate virtual reality-based learning content or collaboration methods into their standard nursing curriculum. Therefore, students’ responses to these attributes were based on hypothetical scenarios in this DCE rather than direct experience. The stated preferences were explored, but participants might not exhibit the same preferences in real-world situations as they do in hypothetical scenarios, leading to potential discrepancies between stated preferences and actual behaviors. Secondly, the convenience sampling method used might not fully represent the entire population of nursing students, potentially leading to selection bias and affecting the validity of the findings. Finally, only six attributes were selected due to the internal limitations of DCEs. Some students might have difficulty in understanding these attributes. As a result of this limited understanding, some factors might be inadequately taken into account during the trade-off process in the DCE, potentially reducing the importance of these factors in predicting preferences. Hence, future research should incorporate patient-interpretable attributes, like the probability of vertigo or other adverse events.
Conclusion
This DCE attempted to investigate the preferences of undergraduate nursing students regarding virtual reality simulations for nursing skills training. The findings indicated that factors such as types of virtual reality, interaction, and learning contents significantly influence students’ choices, highlighting the importance of designing immersive learning experiences with natural gestures and advanced learning content. As nursing education increasingly incorporates technology, understanding these preferences can guide educators and curriculum developers in optimizing simulation-based training. Ultimately, aligning educational strategies with student preferences may enhance learning outcomes, better prepare future nurses for clinical practice, and contribute to the advancement of nursing education in the digital age.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251339009 - Supplemental material for Undergraduate nursing students’ preferences for virtual reality simulations in nursing skills training: A discrete choice experiment
Supplemental material, sj-docx-1-dhj-10.1177_20552076251339009 for Undergraduate nursing students’ preferences for virtual reality simulations in nursing skills training: A discrete choice experiment by Yanya Chen, Yan He, Xiaochun Zou, Hongya Cai, Hei Hang Edmund Yiu and Wai-kit Ming in DIGITAL HEALTH
Footnotes
Ethical considerations
Ethical approval was obtained from the Ethical Review Board of Jinan University.
Author contributions
Yanya Chen, Yan He, and Xiaochun Zou made contributions equally to this article. Yanya Chen, Yan He, and Wai-kit Ming made contributions to the study conception and design. Xiaochun Zou and Hongya Cai made contributions to data collection. Yan He, Hei Hang Edmund Yiu, and Wai-kit Ming made contributions to data analysis. Yanya Chen, Yan He, Hei Hang Edmund Yiu, and Wai-kit Ming contributed to the draft and critical revision of the article. All authors approved the final article for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 2023 Higher Education Society Higher Education Research Planning Project, 2024 Special Project on Experimental Teaching Reform Research of Jinan University, SIRG-CityU Strategic Interdisciplinary Research Grant, 2023 Guangdong Provincial Young Innovative Talents Project for Regular Higher Education Institutions, Teaching Quality and Teaching Reform Project of Jinan University, 2025 Guangdong Provincial Medical Research Fund (grant numbers 23SZH0208, BZH202403, 7020093, 2023KQNCX006, JG2022047, and *).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HHEY reported receiving research grants from the Health Bureau of the Government of the Hong Kong SAR (HMRF) and Viatris, outside the submitted work.
Guarantor
WKM
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.