
Abstract
Objective
With obesity a major health concern and call on healthcare resources in China, we explored the preferences and willingness to pay (WTP) for obesity OMC, including the influencing factors behind WTP and preferences.
Method
We recruited 400 obese participants to undertake a discrete choice experiment (DCE) and the contingent value method (CVM) survey. We used CVM to measure obese participants’ WTP for one-click services (OCS) and used DCE to estimate obesity participants’ preferences and WTP for OMC with different attributes.
Results
Obese participants were willing to pay more than RMB80 on average for OCS, and more than 50% of participants had a WTP over RMB50 and 5% had a WTP over RMB300, reflecting the strong willingness of Chinese obese patients to pay for OMC. Educational background, income, ethnicity, previous OMC experience and accessibility to offline hospitals with different levels impacted WTP. The relative importance score of attributes in descending order was cost, doctors’ hospital level, doctors’ level, online waiting time, consultation time and consultation form. Obese patients preferred lower cost, doctors from higher-level hospitals, doctors with higher expertise levels, shorter waiting time and consultation duration, and telephone consultation were preferred. 30-min waiting time, 15-min consultation duration and telephone consultation were the most economically efficient set we found.
Conclusion
To maximize health resources, provincial tertiary and municipal hospitals face different paths to developing obesity OMC platforms. We encouraged young doctors to use OMC. OMC regulators should implement consumer protection policies to optimize OMC pricing and address potential ‘unfair’ pricing.
Keywords
Introduction
Online medical services have become increasingly popular in the past decade, especially during the COVID-19 pandemic. 1 Among online medical services, online medical consultations (OMC) are one of the most frequently used professional services.2,3 Existing research has found that OMC improves patient satisfaction, adherence, engagement and access to healthcare, with the potential to improve self-care and patient safety;4–6 in managing chronic conditions, weight loss interventions 7 and individual counselling; 8 and in improving patient communication. Existing research has also pointed to technological challenges, regulatory issues, rural-urban disparities and privacy concerns in OMC treatment.6,9 The benefits and challenges of OMC during COVID-19 have led researchers to call for sustainable strategies for OMC beyond the pandemic.10,11
Obesity is a primary candidate for OMC. While diet, physical activity and behaviour therapy have been found to be effective ways to treat obesity, compliance management has challenged traditional offline treatment, witnessed by an increasing overweight and obese population. As an accessible and convenient obesity treatment, obesity OMC improves the effectiveness of obesity treatment12–14 by addressing the stigma and other psychological burdens that inhibit offline obesity treatments. Previous research has also found that obesity OMC's privacy protections and confidential communication facilitate obesity patients’ compliance with their health management regimes and reduces offline treatment costs, such as travel, transport and loss of worktime costs. 15 Taken together, obesity OMC and obesity offline consultations contribute to the more efficient allocation of total healthcare resources.
While China's online medical consultations are more than 20 years old, the COVID-19 epidemic significantly increased the acceptance and utilization of telemedicine among Chinese residents. With more than half of Chinese adults overweight (34.3%) or obese (16.4%), and China ranking first in the number of obese residents, 16 obesity telemedicine platforms provide unique advantages in treating China's obesity crisis. Obesity OMC can economize health resources, with China's obesity-related medical expenses projected to reach RMB418 billion, accounting for 21.5% of China's medical expenses, by 2030. 17 Existing OMC studies have been mostly qualitative, analyzing industry status quo and regulatory policies18,19 and much of the empirical research and case studies have focused on the OMC supply-side.20,21 Surprisingly, there has been little demand-side research on users’ OMC preferences. To address this gap in the literature, our focus is on preferences and willingness to pay for China's obesity OMC.
The context for OMC in China is shaped by government regulations that apply different pricing and regulatory standards depending on whether the medical services on the OMC platform have been included or excluded from the national medical insurance reimbursement scheme. When included in the national medical insurance reimbursement scheme, prices for offline face-to-face and online consultations follow the same guidelines, usually with OMC platforms operated by public hospitals required to adopt the offline pricing method. When not included in the national medical insurance reimbursement scheme, online platforms determine their own prices based on market demand. The market-oriented online approach is the preferred option for OMC platforms, which have predominantly shaped China's telemedicine industry and are usually operated by private enterprises. Using fee data on China's market-oriented OMC platforms, the Shanghai Health Development Research Center found that there were significant differences in consultation prices across OMC platforms. 22 However, such research has ignored the reasons behind the different OMC fees and the consumer preference factors explaining OMC pricing. Further, the willingness to pay and service demands of patients with different diseases vary across OMC platforms. 23 Many previous studies on China's OMC fail to distinguish between different diseases, with any results subject to selection bias.24,25 We focus on obesity OMC. We analyzed obesity patient preferences for market-based obesity OMC, including fee structure, doctors’ hospital level, doctors’ expertise level and consultation form. 26 In addressing this lacuna in OMC obesity research in China, our results may inform other telemedicine platforms, such as health behaviour and chronic diseases online consultations.
Methods
Framework of experiment
We used the contingent value method (CVM) and discrete choice experiment (DCE) to estimate Chinese obese adults’ willingness-to-pay (WTP) and preferences for obesity OMC. Based on consumer choice economics, 27 CVM and DCE examine consumers’ stated preferences over hypothetical alternative scenarios, a technique widely used in the healthcare management and health economics research. 28 CVM simulates real-life practice, where Chinese OMC suppliers provide One-click Consultation Services (OCS), matching doctors to users, where users can not choose a particular doctor based on their attributes. Although CVM cannot reveal user's preferences and marginal willingness-to-pay (mWTP) for doctors with different attributes, CVM estimates the users’ WTP for obesity OCS. DCE generate a variety of consumer choices for doctors with different attribute combinations via experimental design, so as to estimate users’ preferences and mWTP for doctors with different attributes.
Sample size and data collection
Based on the existing research, the sampling size of a prevalence survey on China's overweight and obese patients should no less than 400 respondents. 29 Figure 1 shows the recruiting, screening and experiment process. We used quota sampling to recruit participants, and the prevalent rates of age, sex and regions of overweight and obese patients in China were defined as the quotas in our survey. The proportion of overweight and obesity in Chinese adults was derived from the Report on Nutrition and Chronic Diseases in Chinese Residents (2020) 30 while Zhang et al.'s 31 survey of 441 thousand adults provided the sex, age, and regional distribution parameters for overweight and obese adults.
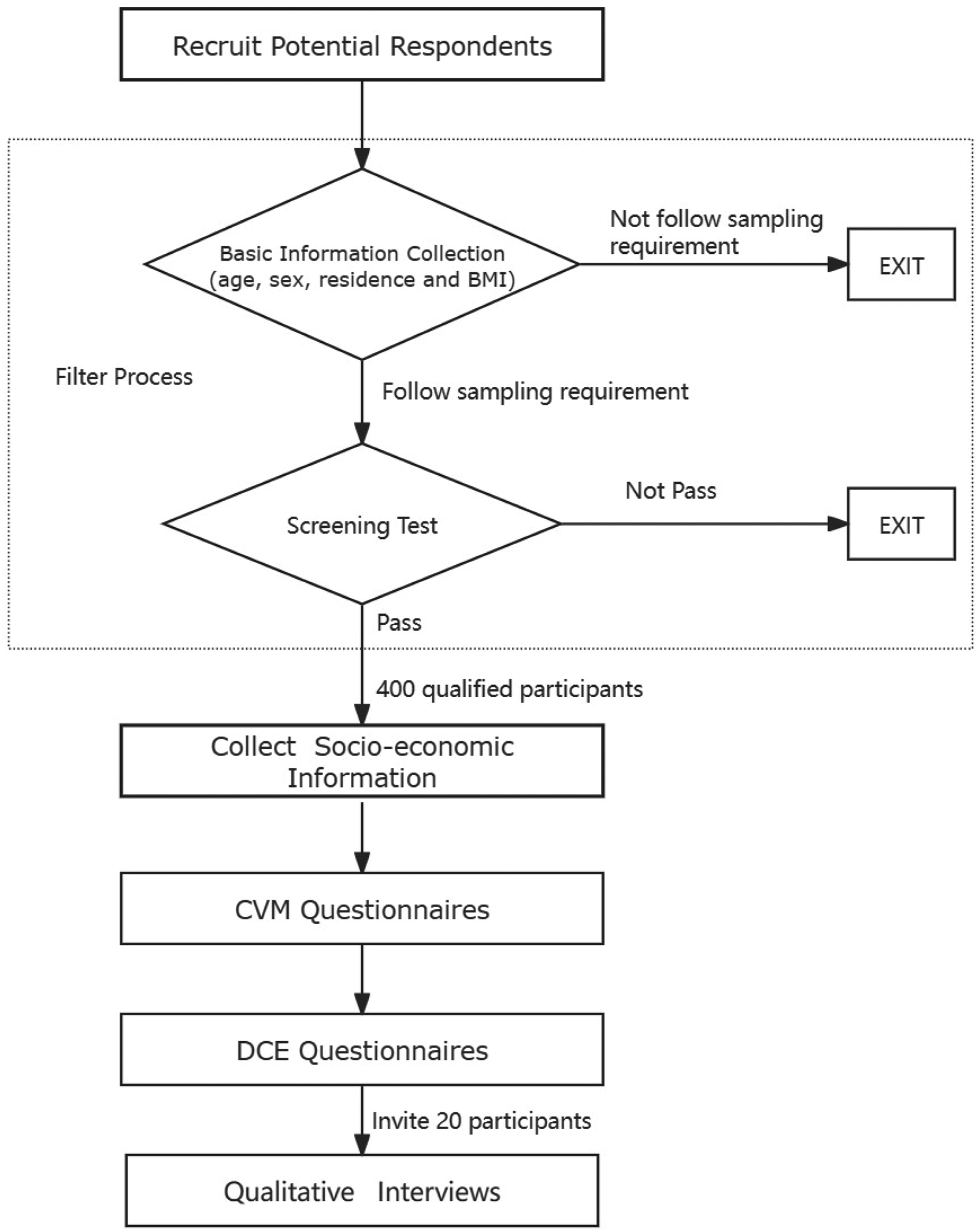
Flowchart of recruitment and experiment.
We designed our online survey platform to recruit eligible respondent's representative of China's national overweight and obese epidemiological characteristics. Second, we required respondents to pass a screening test, which required correct answers to two questions shown in Figure A1, which ensured participants, had a good understanding of how to complete a DCE survey. 32 The recruitment process and survey completion were assisted by a trained medical investigation team with good connections with doctors and hospitals across China. The team recruited obese patients and verified the authenticity of the participants’ information through interviews with the patients and their doctors. After participants completed the surveys, we recruited 5% of the sample, or 20 patients, for in-depth interviews. The interviewees were classified into two types, typical respondents and outliers. Typical respondents had an average WTPA in CVM or preferences consistent with our hypothesis in the DCE, while outliers had too high or too low WTPA in CVM or unusual preference choice in the DCE.
Table 1 displays the data on participants’ predisposing socio-economic and personal characteristics (including age, sex, education, ethnicity, marital status, geographic region and urban-rural location); enabling characteristics (such as monthly income and travel time to hospital); obesity needs (including medical intervention, chronic non-obesity diseases and drug use); and past experience of using OMC.33–35
Characteristics of participants following distribution characteristics of obesity epidemic in China.

Informed consent was obtained from all qualified participants before undertaking the survey and respondents could terminate their participation at any stage of the survey. The project's aims and data collection, usage and storage of information were provided to respondents in the online informed consent agreement. The data collection followed the requirements of Chinese legislation on private information protection. Participants were given sufficient time to understand the informed consent agreement and ticked a box in the online form to give informed consent to participate in the survey. In the informed consent step, participants could also request help from our offline survey team. Our survey ensured anonymity and the data were used only for academic research. Ethics approval was granted by Dong Fureng Institute of Economic and Social Development, Wuhan University. The questionnaire used in our survey was designed by the authors (Supplemental material).
Design of CVM
Our CVM and DCE surveys share the same experimental scenario, which is shown in Figure A2. CVM is one of the main stated preference methods to measure respondents’ WTP and the monetary valuation of new health services. 36 CVM can simulate the experience of OCS where OMC suppliers directly select a doctor for the user. We used the double-boundary dichotomous choice questionnaire to estimate participants’ WTP range and offered an open-ended question to elicit participants’ exact WTPA.37,38 For CVM's binding levels, we used multiples of 5 as shown in Figure A3. The lowest bidding value indicates to participants that the service is not free, while the highest bidding value was set to be unacceptable to most people. We analyzed the pricing of China's major OMC platforms, especially the 95th percentile and maximum prices of obesity doctors on those platforms. 26 Combined with pre-experiment research, expert opinions and previous research, 39 we set the highest value at RMB300.
Design of DCE
Given there were few previous DCE obesity OMC studies, we selected the DCE attributes and levels through a literature search, research on the status quo of OMC in China and industry and academic focus groups. We also undertook a pilot study covering 10 obesity patients with different socio-economic backgrounds to test the attributes and levels in questionnaires. The DCE attributes and levels are listed in Table 2. Doctor ratings or doctor quality were not included as an attribute because our pre-experiment survey, expert advice and focus group study indicated that doctor level and doctor's hospital level proxied doctor ratings and doctor quality; doctor ratings were not available on some platforms; and our concern that doctor ratings could be manipulated on some platforms. The attributes including numerical levels like out-of-pocket cost, waiting time and consultation duration were confirmed following the practices recommended by ISPOR. 40 We did not include video consultation. Not all OMC platforms provide video consultations in obesity treatment. 41 Second, we conducted a focus group study and consulted six OMC experts who reported video consultation was not highly accepted or used by doctors and patients in obesity treatment.
Attributes and levels in DCE survey.

Given the attributes and their levels in Table 2, a full factorial design produced 864 (= 42 × 33 × 21) hypothetical scenarios and 372,816 ((864 × 863)/2) pairwise choice tasks. A D-efficient design 42 was used to generate 16 manageable choice sets. Using Ngene each choice set composed two options and the 16 choice sets were grouped into two blocks.
As an incentive for carefully undertaking the survey, only participants completing the experiment were remunerated for participating in the research. We provided easily available links to explanations of the attributes and levels and also identified potential invalid responses. For example, when respondents chose the same choice option three times continuously, the online experiment automatically alerted respondents to inform, but not to punish, them when they chose the same option three consecutive times.
Statistical analysis
In the CVM questionnaire, we used double bounded dichotomous choice with an open-ended question to estimate the WTPA of the respondents and a TOBIT model to estimate the influencing factors on WTPA. Although some OMC platforms in China provided free consultation services with limited service, such free services were excluded in our study. Therefore, the WTPA of respondents in our CVM research should be greater than zero, which means the dependent variable WTPA should maintain in the positive value region as a censored dependent variable. Commonly used in CVM analysis, we specified a standard TOBIT model:


Based on the random utility theory,
43
the DCE data were analyzed in a mixed logit model (ML model).
44
In stated preference research, the utility that that respondent i obtained from choosing alternative j in choice set s is given by
Results
Willingness-to-pay amount estimation
In the CVM questionnaire, 90% of respondents (N = 360) chose to pay for OCS. In the high WTPA space, we found 12 participants’ WTPA was RMB500, and one participant's WTPA was RMB1000. Table 3 shows the different WTPA results for the full data set and data with outliers (WTPA = RMB1000) removed. Obese residents were willing to pay an average of more than RMB80 for OCS, and more than 50% had a WTPA over RMB50, and 5% had a WTPA over RMB300. Both the average and median WTPA were higher than the outpatient fees of most offline hospitals in China, 41 reflecting the strong willingness of Chinese obese residents to pay for OMC.
Distribution of OCS WTPA using CVM (in RMB).
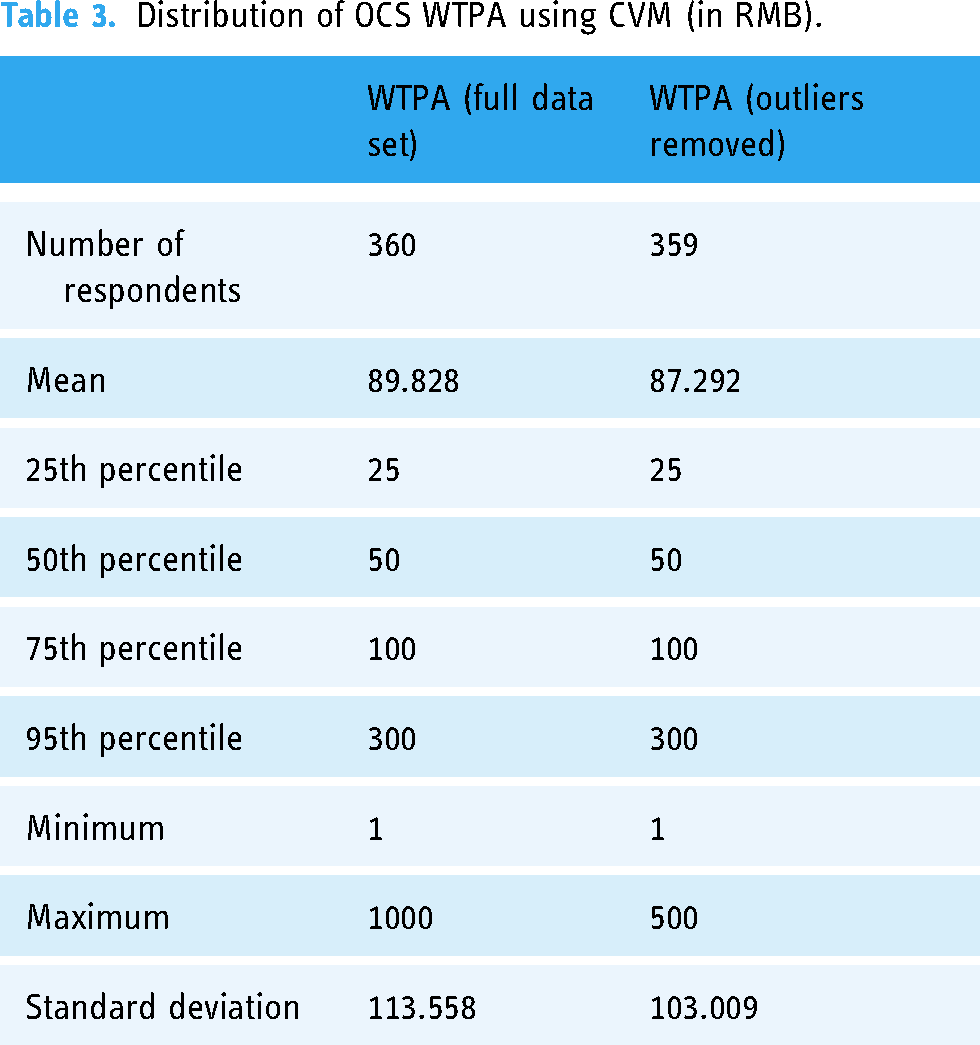
During interviews with the participant whose WTPA was RMB1000, we found the estimation reflected his true WTPA. Considering the truncation effect and the goodness of fit, the truncated data were more in line with bias control and statistical requirements, so we performed TOBIT analysis based on truncated data as shown in Table A1.
For the predisposing characteristics, we found that Han respondents’ WTPA was lower than that of minority respondents (P = 0.001) and compared to those with education level of primary school and below, people with higher educational level had lower WTPA. Based on our qualitative interviews, we found that minorities, usually living in remote and rural areas, had poorer access to high-end medical resources and higher educated respondents had better access to health information and resources than lower educated respondents. For the enabling characteristics, respondents with income level between RMB6001-35,000 per month had higher WTPA (P = 0.033) than those with income below RMB2000 per month (P = 0.027). Compared to within 30 min travel time, when the respondents’ travel time to an offline tertiary hospital was between 0.5 and 2 h, the WTPA for OMC fell, reflecting the reputation of tertiary hospitals, but when the respondents’ travel time to an offline municipal hospital was between 0.5 and 1 h, the WTPA for OMC increased. Obese respondents who had used OMC before were willing to pay more for OMC (P = 0.052). In summary, ethnicity, educational background, income, previous OMC experience and accessibility to offline hospitals of different levels influenced obese patients’ WTPA. Age, sex, marital status, urban-rural location, number of insurance policies and needs were not significant factors influencing WTPA in our analysis.
DCE results
DCE Table 4 shows the results of preferences and WTP space based on the ML model. The mean ASC was significantly positive (3.106), indicating that obese residents preferred OMC over no consultation. From Table 4, participants preferred higher level doctors and doctors from higher level hospitals, where an improvement of the hospital level brought a higher utility than a rise in doctor level. Compared to county-level hospitals, the mean preference coefficients for doctors from provincial-level tertiary hospitals would increase 1.549 times and municipal-level hospitals would increase 1.095 times. Compared to ordinary doctors, the mean preference coefficients of well-known experts increased 1.362 times and general experts 0.418 times. The participants preferred telephone consultation to text consultation and there was no statistically significant preference heterogeneity for this attribute. The respondents preferred lower cost and low waiting time,but the standard deviation of the two attributes indicated significant preference heterogeneity. The mean preference coefficient of consultation duration was negative
Obese residents’ preferences and WTP space for OMC.

Except for consulting duration, all WTP level estimates in Table 4 were significant. Compared with ordinary doctors, participants were willing to pay RMB18.68 more for general experts and RMB72.79 more for well-known experts. Using county-level hospitals as the reference, participants were willing to pay RMB65.55 more for municipal hospitals and RMB87.43 more for provincial tertiary hospitals. Compared with text consultation, participants were willing to pay RMB9.96 more for telephone consultation. The WTP was -RMB1.95 for an increase of every minute of waiting time. We used the WTPA measured by CVM to roughly verify the robustness of the mWTP measured by the DCE. Comparing Tables 3 and 4, the highest mWTP using ML model was RMB87.43 for provincial tertiary hospitals, which is about the average WTPA of RMB87.29 measured by the CVM method.
RIS identifies the relative importance of different attributes in participants’ decisions. Based on ML model, Table 5 indicates importance in descending order was cost (RIS = 48.7%), doctors’ hospital level (RIS = 19.3%), doctor level (RIS = 17%), online waiting time (RIS = 8.3%), consultation duration (RIS = 3.7%) and consultation form (RIS = 2.9%).
Relative importance scores.

Discussion
This is the first quantitative demand-side study of Chinese obese adults’ WTP and choice preference for obesity OMC. We undertook two survey experiments: a CVM OCS model, where the consultation platform matched a doctor to the user, and a DCE where users chose different OMC attributes and levels. The CVM method allowed us to estimate WTPA and the DCE method identified the preferences and mWTP of obese participants.
CVM showed that 90% of respondents (360 people) were willing to choose OMC. The average WTPA was RMB87.29, and the median was RMB50. Our results demonstrate a higher acceptance of OMC than previous non-obese patient studies,48,49 which suggests that obese respondents had a higher demand and WTP for professional OMC advice than non-obese respondents for non-obese online advice. The Tobit regression model indicated the status of doctors from tertiary hospitals was a crucial factor in users’ offline versus online consultations choice. We found that offline tertiary hospital patients may not transfer to online consultation even when faced with increased transportation costs, but offline municipal hospital patients faced with the increased transportation costs would increase their WTP for online service. Compared to previous research on the relationship between accessibility and acceptance of OMC,50,51 our results paint a more complex picture of OMC use, where OMC use is related to different levels of offline hospitals. The preference for offline tertiary hospitals, even with long wait and travel time, over OMC was confirmed in our interviews. Based on our findings, we recommend that tertiary hospitals build robust online comprehensive treatment systems to improve Chinese residents’ access to the benefits of OMC and promote the OMC cost-saving advantages for the health system over offline consultations. With tertiary hospitals promoting OMC, commercial OMC providers will also benefit when users can access tertiary-level doctors online. Since municipal hospital patients prefer OMC, non-tertiary hospitals should take the opportunity to improve their online services. We also found the positive effect of previous OMC use on WTPA formed a basis for building the OMC reuse rate, which OCM platforms should optimize to realize compliance management of obesity treatments.
Our DCE confirmed our CVM results that obese residents had a high WTP for OMC, especially compared with the offline medical consultation fees. 41 The RIS revealed costs, hospital level and doctor level were the three major influencing factors on WTP, with doctors’ hospital level preferred over doctors’ expertise level in selecting OMC. This result points to inefficiencies in the Chinese hospital system, with the over-use of tertiary hospitals and the under-use of county and municipal hospitals, when patients directly choose the ‘best’ hospital. 52 We have argued that tertiary hospitals and municipal hospitals have scope for improving their OMC platforms. Second, given limited high-quality medical resources in China, improving the allocation of medical resources between doctors and users is a key competitive advantage for online suppliers. Finally, our findings suggest that lower level doctors have scope to gain market share by lowering their prices.
Compared to the previous studies,50,52 our detailed findings on waiting time and consultation duration provide practical suggestions to OMC providers. Longer waiting time reduced OMC's utility for obese patients, but when we treated the waiting time attribute as a categorical variable in Table A2, we found that 30 min, rather than 15 min, was the most preferred wait-time level, which suggested that 30 min wait-time was a more economically efficient parameter for OMC platforms. In Table 4, the ML model showed that longer consultation time was not preferred when time was treated as a continuous variable. When the consultation duration was treated as a categorical variable in Table A2, we found that the preference coefficient of 20 min was close to that of 15 min, which suggests when OMC platforms find it difficult to arrange consultation duration in 20 min slots, then 15 min is also acceptable to their users. Combined with our qualitative research, the counterintuitive findings may be related to the diminishing marginal utility effect. Another explanation is that even for the shortest consultation time of 10-min in our DCE set, many respondents reported it was longer than their usual offline consultation and with better communication experience, and 30 min of waiting time was much shorter than their offline transportation and waiting time.
Our findings on consultation form were consistent with previous telemedicine research in China, 50 where telephone consultation was preferred over text consultations, and obese patients were willing to pay RMB10 more for telephone consultations. We recommended OMC platforms perfect their voice technology to provide better services. Our estimated mWTP in DCE study shows that Chinese obese participants’ high willingness to pay for high-quality online consultations. While OMC pricing is higher than that of offline hospitals,25,26 our findings of patient WTP for high-end medical resources online means that OMC providers can develop differentiated market-oriented pricing. With high OMC WTP, we recommend OMC regulators implementing consumer protection policies to optimize OMC pricing and address potential ‘unfair’ pricing.
Our results suggest that young doctors using OMC can gain a competitive advantage. In China, doctor management regulations mean young doctors find it difficult to change their hospital and expertise level in the short run. Also, medical regulations set uniform offline consultation pricing standards where more senior doctors receive a higher fee. Private OMC platforms are not subject to offline price regulation, which means that younger doctors with good OMC experience can charge higher OMC fee. There are opportunities for young doctors to provide cheaper, but better online services with shorter waiting time and telephone consultations.
Our paper has a number of limitations and strengths. Our study is the first to examine obese patients’ stated preferences and WTP for OMC in China. One strength is that our sample size is considered relatively large for DCE studies, while meeting the minimum size for our CVM method. We defined OMC as a paid service without considering free online consultations. We used quota sampling based on the Report on Nutrition and Chronic Diseases in China (2020) and Zhang et al. (2020) cross-sectional study published in 2020 to recruit our participants. Future studies should investigate alternative quota databases providing the latest epidemiological characteristics of China's overweight and obese patients.
In the CVM method, those who had no willingness to choose were not included in our analysis. In the DCE method, we provided respondents exit choice by dual-response design, but did not include free consultations, so our research has more reference value for paid consultations. Even though we selected the DCE attributes based on the commonalities of China's OMC platforms, the uniqueness of some OMC platforms was not considered in our research. Among the first studies to assess overweight and obese patients’ preferences and WTP for OMC, our research also did not measure the effectiveness and efficiency of OMC in the treatment of obesity. While our results provide new insights into online obesity treatment, care should be taken when generalizing our findings to other online disease treatments.
Conclusion
As a quantitative study on China's OMC from the perspective of obesity patients, our research provides new insights into the telehealth industry, which may be applicable to telemedicine platforms generally. The high acceptance and WTP demonstrated the high demand by obese patients for OMC. Our Tobit model identified ethnicity, educational background, income, previous OMC experience and accessibility to offline hospitals of different levels as key influencing factors. Our DCE analyses showed that lower cost, doctors from higher-level hospitals, doctors with higher expertise levels, shorter waiting time and consultation duration, and telephone consultation were preferred. We recommended that obesity OMC platforms pay particular attention to their differential pricing and that 30-min waiting time and 15-min consultation duration were the most economically efficient parameters for OMC platforms. We also recommend the regulation of OCM pricing.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241272525 - Supplemental material for Online medical consultation in China: Demand-side analysis of obese patients’ preferences and willingness-to-pay for online obesity consultations
Supplemental material, sj-docx-1-dhj-10.1177_20552076241272525 for Online medical consultation in China: Demand-side analysis of obese patients’ preferences and willingness-to-pay for online obesity consultations by Yaolin Hu, Jian Wang, Yuanyuan Gu, Stephen Nicholas, Elizabeth Maitland and Jianbo Zhou in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors thank the participants in this study.
Contributorship
All authors have contributed to different work of the article. YH designed the experiment, searched the literature, collected data, did analysis, interpreted data, and wrote the article. JW designed the experiment, supported the whole research, interpreted data and wrote the article. YG designed the experiment, collected data and did analysis. SN and EM did analysis, interpreted data, and wrote the article. JZ participated in the writing and submitting of the article. In addition, YH, SN and EM were involved in revising the article critically for important intellectual content, or in the final approval of the version submitted for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethics approval was granted by Dong Fureng Institute of Economic and Social Development, Wuhan University.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
YH.
Supplemental material
Supplemental material for this article is available online.
Appendix
Obese residents’ preferences for OMC when time were treated as categorical variable using conditional logit model.
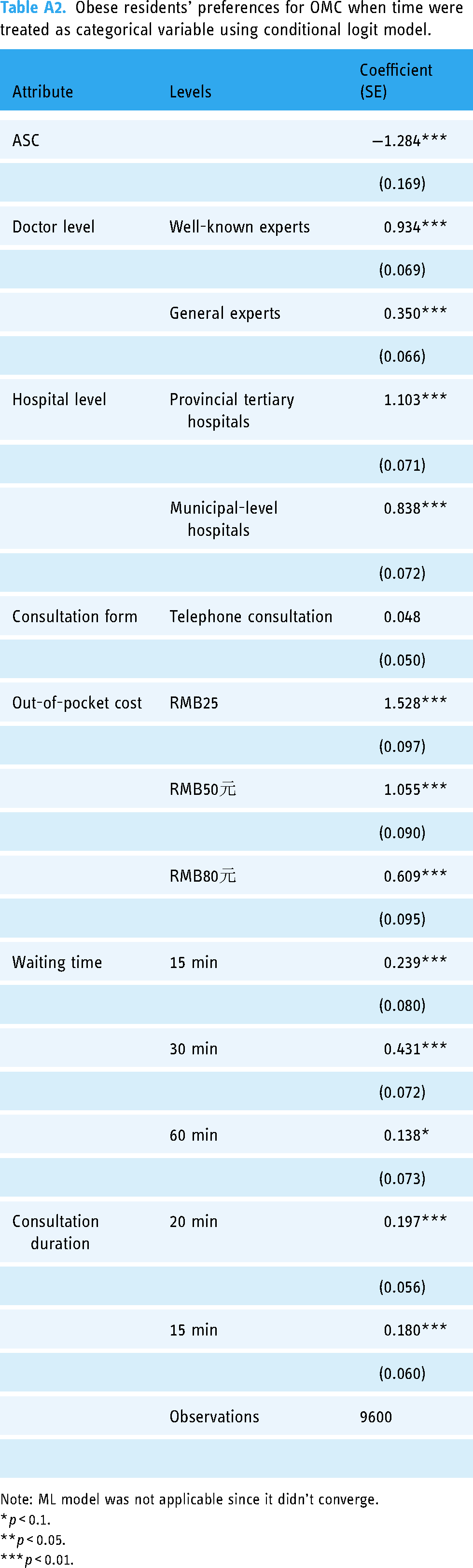
| Attribute | Levels | Coefficient (SE) |
|---|---|---|
| ASC | −1.284*** | |
| (0.169) | ||
| Doctor level | Well-known experts | 0.934*** |
| (0.069) | ||
| General experts | 0.350*** | |
| (0.066) | ||
| Hospital level | Provincial tertiary hospitals | 1.103*** |
| (0.071) | ||
| Municipal-level hospitals | 0.838*** | |
| (0.072) | ||
| Consultation form | Telephone consultation | 0.048 |
| (0.050) | ||
| Out-of-pocket cost | RMB25 | 1.528*** |
| (0.097) | ||
| RMB50元 | 1.055*** | |
| (0.090) | ||
| RMB80元 | 0.609*** | |
| (0.095) | ||
| Waiting time | 15 min | 0.239*** |
| (0.080) | ||
| 30 min | 0.431*** | |
| (0.072) | ||
| 60 min | 0.138* | |
| (0.073) | ||
| Consultation duration | 20 min | 0.197*** |
| (0.056) | ||
| 15 min | 0.180*** | |
| (0.060) | ||
| Observations | 9600 | |
Note: ML model was not applicable since it didn’t converge.
*p < 0.1.
**p < 0.05.
***p < 0.01.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.