
Abstract
Objective
Parkwood VIP4SCI platform is a virtual e-health solution adapted from a version created for Spinal Cord Injury Ontario (SCIO) that focused on self-management skill development for persons with spinal cord injury (SCI) transitioning between stages of care, in partnership with caregivers and clinicians. This evaluation of the platform informs the usability and feasibility of a model to facilitate service care aims postrehabilitation.
Design
Results
VIP4SCI was viewed as usable and feasible. Platform satisfaction assessed on a −3 to +3 scale ranged from +0.9 to 2.5, demonstrating positive agreement. Self-efficacy related to self-management ranged from 5.4 to 7.6 out of 10. The educational resource hub was identified as the most beneficial feature. Lack of clinician uptake was a barrier to integration into day-to-day practice.
Conclusions
Platform usage was low among all groups despite the perceived need for facilitating care coordination with consistent and intentional self-management programming. Despite the lack of uptake, partly due to challenges associated with the pandemic, conclusions on platform features and barriers to implementation will help to inform future programming.
Introduction
Persons with spinal cord injury (SCI) face challenges as they navigate transitions across the care continuum.1,2 Minimal coordination between SCI specialists and community services coupled with shorter lengths of stay can result in poorer outcomes postdischarge and less time to develop self-management skills.3–14 In navigating this disjointed care system, needs often go unaddressed and difficulties re-integrating into the community are exacerbated, representing a gap in care transitions. Therefore, an e-health system employing a theory-based approach was designed to overcome these needs and empower persons with SCI by promoting self-management skill development. The following work represents a demonstration of the usability, feasibility, and effectiveness for this e-health solution with features that enable a novel theory-based care service delivery model.
“Self-management” is defined as the “ability to manage aspects of symptoms, treatment, physical and psychosocial consequences, and lifestyle changes inherent in living with a chronic condition.”15,16 It reflects a dynamic process in which effective monitoring and goal-directed behavioural regulation work in tandem to maintain quality of life.15,16 A recent environmental scan indicated that self-management skill development was acknowledged as an important goal to Canadian SCI rehabilitation centres, despite a lack of understanding of approaches to achieve it. 17 In addition, there was a lack of expertise with only 3 of 12 programs reporting access to specialists to support the embedding of active methods for skill-building. A strategy for improving outcomes in persons with SCI may be the adoption of an integrated program for self-management, facilitating the “expert patient” as an effective knowledge mobilization agent. 17
Approaches to self-management may benefit from the embedding of evidence-informed behavioural strategies to facilitate uptake. A review on self-management interventions focused on enhancing physical activity in persons with SCI concluded that the use of behaviour change techniques, theories, and/or constructs were related to significant improvements in and maintenance of leisure time physical activity outcomes. 18 Also of note, recent self-management trials focused on preventing secondary conditions have been explicit about the embedding of behaviour change strategies, with action planning, problem-solving, and goal-setting being common approaches.19–22 In line with these results, the Health Action Process Approach (HAPA), a stage- and continuum-based behaviour change model, was considered for this initiative based on its successful employment in previous interventions.23–25 Key constructs in the HAPA include self-efficacy, action-planning, coping, and meaningful intentions. 23 Self-efficacy is defined as the perceived capability to perform a desired action. Action planning details the when, where, and how of an intended action. 23 Coping refers to the anticipation of barriers and design of alternative actions to help with goal attainment despite impediments. 23 The facilitation of meaningful intentions during goal-setting describes the idea of one's intention to perform a behaviour being in alignment with personal goals. 23 These constructs were operationalized and embedded in the design of the e-health solution. For example, action-planning was incorporated via the goal-setting feature of the platform, facilitating the user in taking a structured approach to identify the when, where, and how of the intended action.
The platform, Virtual Integrated Platform for SCI (VIP4SCI), was developed as an extension of a version created by ForaHealthyMe Inc. (Toronto, Canada) for Spinal Cord Injury Ontario (SCIO). It was created to facilitate the coordination of care with intentional self-management programming, such that persons with SCI would be equipped with tools and resources to navigate a fragmented network of health services and maintain health by managing secondary complications and improving participation.
The following work represents an evaluation of the usability, feasibility, and effectiveness of VIP4SCI. Usability was operationally defined using constructs of the Mobile App Rating Scale (MARS), specifically quality of information, subjective quality, and perceived impact. 26 Feasibility was operationally defined using the Bowen framework, however the present study only included 4 of the 8 constructs associated with Bowen et al.'s overall concept of feasibility (acceptability, practicality, demand, and limited efficacy). 27 Effectiveness was operationally defined using the limited efficacy construct of feasibility, where the evidence determines if the intervention (i.e. the platform) worked under real-life circumstances. 27 It was hypothesized that the platform would increase self-efficacy related to symptom management, foster goal-setting behaviours related to self-management, and be deemed usable and feasible for use by both patients and clinicians.
Methods
Study context
Parkwood Institute (PI) is an academic rehabilitation hospital located in London, Ontario, Canada that provides care to persons with SCI and other conditions. Following admission, patients participate in therapeutic interventions and educational programming to restore function and re-integrate into the community. As persons with SCI are often at risk of secondary conditions, practicing self-management skills are a core component of care. Following discharge, patients are directed to services as needed, such as outpatient/community rehabilitation services and/or community agencies such as SCIO.
Phase 1: Platform development
Stakeholder involvement was a key aspect of platform development. Stakeholders included: hospital clinicians, persons with lived experience (persons with SCI), caregivers, a SCIO representative, hospital leadership (SCI program coordinator), and the research team. During the development phase, this stakeholder group identified priorities related to features, outcomes, and design elements to incorporate into the prototype e-health solution (Figure 1A). Establishing these priorities involved an initial program retreat, followed by deliberations within the SCI Program Council (i.e. decision-making body of the SCI programs at PI).

Governance structure and current state process map. (A) Governance structure diagram showing the various groups that collaborated throughout the development of VIP4SCI. (B) Process map of current state activities within the SCI inpatient and outpatient programs that informed the creation of platform features during the development phase. SCI: spinal cord injury.
A current state process map of the overall SCI program was developed to identify potential features to support within the platform. This resulted in the identification of seven areas of focus: (1) evaluation, (2) care transitions, (3) education, (4/5) clinical tools/processes, (6) resources, and (7) peer support (Figure 1B). The map helped brainstorm specifics for how features might be operationalized within VIP4SCI. After prioritization, it was determined that there would be customized approaches for goal-setting and action-planning within the following domains: Pain, Keeping Skin Healthy, Feeling Good, and Staying Active.
The vendor (ForAHealthyMe.com) used feedback from initial stakeholder consultations to develop a prototype. At multiple points, the core project working group and the broader stakeholder group provided additional feedback, resulting in a workflow of iterative prototyping. Additionally, the vendor consulted with institutional and organizational experts in information technology (IT) and privacy and risk management to ensure the platform met organizational requirements related to security and privacy and risk. Secure login practices were embedded into the platform, and users were required to answer two security questions whenever logging in from a new device. The platform was made live only once vetted and approved by the organization's IT and Privacy and Risk management departments.
Throughout the development phase, the project working group asked the broader stakeholder group to share their most frequently utilized patient resources to aid the vendor in the creation of a resource library on VIP4SCI. The platform underwent further changes, internal testing, and validation before it was piloted by four persons with lived experience, at which point focus group feedback informed final modifications. As well, prior to deployment, the platform underwent a final round of bug fixes for the purposes of a more fulsome trial of usability and validation.
The features of the platform were centered around communication, self-management and education (see Supplemental Appendix A for overview of Platform Features). In the area of communication, the platform housed multiple tools including Contact lists with contact information of members of the patient's Care Team, Calendar reminders and notifications to track goals and appointments, as well as Messaging and Virtual call features to communicate with members of the patient's Care Team. These communication tools were designed to allow clinicians to support their patients throughout their rehabilitation journey and empower patients to reach out to their Care Team when questions arose.
In the area of self-management, a personal goal setting tool was created to allow patients to track their progress and goal attainment throughout their rehabilitation. Other tools, such as Coping with Pain, Keeping Skin Healthy, Feeling Good and Staying Active, were designed to promote integration of self-management strategies after spinal cord injury in the areas of pain, skin health, emotional wellbeing and physical activity. As patients selected strategies they wanted to integrate into their daily life, the Care Team could monitor those entries, and provide feedback and encouragement as needed. An accessible voice to text journaling tool was also available to patients wanting to track their rehabilitation journey or any other important notes. Additionally, a Medication Tracker tool was created to allow patients to enter in a detailed list of their medications, dosages, side effects and additional information.
In the area of educational resources, patients had access to a virtual library of reliable resources related to spinal cord injury. This educational resource hub was meant to afford patients opportunities for self-directed learning, as well as allow clinicians to direct patients to helpful resources all in one place. The resources were grouped into categories of common interest for persons with Spinal Cord Injury (e.g. Bladder and Bowel Care, Mobility, Skin Care, Pain Management, Sexual Health, etc.) and patients could use a search bar or index to explore areas of interest.
Phase 2: Pilot trial
Participants
Patients met the following criteria: (1) ≥18 years; (2) sustained an SCI (any severity level); (3) admitted to the PI SCI rehabilitation program; (4) access to reliable high-speed internet and a usable device (i.e. tablet and laptop); and (5) intact cognitive function. Caregivers were enrolled if the patient granted access to their platform account. An interdisciplinary mix of clinicians enrolled in the study voluntarily.
Study design
This pilot study underwent institutional Research Ethics Board (REB) evaluation and received approval. This study was intended to follow a pragmatic design involving a convenience sample that represented the flow of inpatient and outpatient admissions into the SCI Rehabilitation Program. Therefore, anticipated sample size based on feasibility and patient flow were estimated to be 30 inpatients and 30 outpatients. However, given significant constraints brought upon by the COVID-19 pandemic as described later, the sample size was underachieved. Clinicians were oriented to VIP4SCI via information sessions prior to study commencement, with a refresher offered to staff if needed throughout the trial. Clinicians determined if a patient under their care was appropriate for the study based on the study inclusion criteria, and provided a general introduction. If a patient expressed interest in receiving further information about the study, the clinician contacted the Research Coordinator and provided them with the patient's contact information to arrange for follow up/consent. After speaking with the Research Coordinator and all questions were answered, patients provided written informed consent early in their inpatient stay or throughout outpatient rehabilitation (Figure 2). At the outset, block randomization was completed using a numeric system to determine which patients would have a delay to starting platform use. In attempt to control potential confounders, patients were additionally categorized based on age and impairment to facilitate balanced groups. At the appropriate time, participants were provided with a 20- to 30-minute orientation to VIP4SCI by a member of the research team known as a VIP coach. Orientation consisted of an explanation on how to navigate the platform, use various features/tools, and of examples of information found within the resource library. Throughout the study, VIP coaches remained available for questions and troubleshooting, and provided reminders to complete study surveys.

Study design. Flow diagram of study design for inpatient and outpatient groups, including timepoints of platform access and check-ins by VIP Coaches. D/C: discharge; IP: ; OP: outpatient; wk: week.
Clinician focus groups were held at the midway point of the study to identify facilitators and barriers to platform implementation. Based on feedback, the role of VIP coaches was enhanced to include a more facilitatory approach involving weekly check-ins (∼30 minutes, in-person, or virtual) to monitor goal progress and facilitate the use of self-management tools. Through these weekly check-ins, patients were given reminders to utilize VIP4SCI to track therapy goals and search for educational resources, and were provided an opportunity to ask any questions related to platform navigation. VIP coaches also interacted with patients via communication features to provide encouragement and support.
Quantitative methods
Outcome measures were collected as part of a pre–post evaluation (Table 1). Surveys were administered via an online application (REDCap). Given the participants included persons with neurological injury/deficit, some participants had decreased hand function and required assistance for completing the surveys. Options were therefore provided to facilitate survey completion as inpatients or outpatients (e.g. in-person with physical assistance of a study clinician/VIP coach (paper or virtual), or via email link for self-administration). All survey data was entered into REDCap for analysis.
Participant demographics.
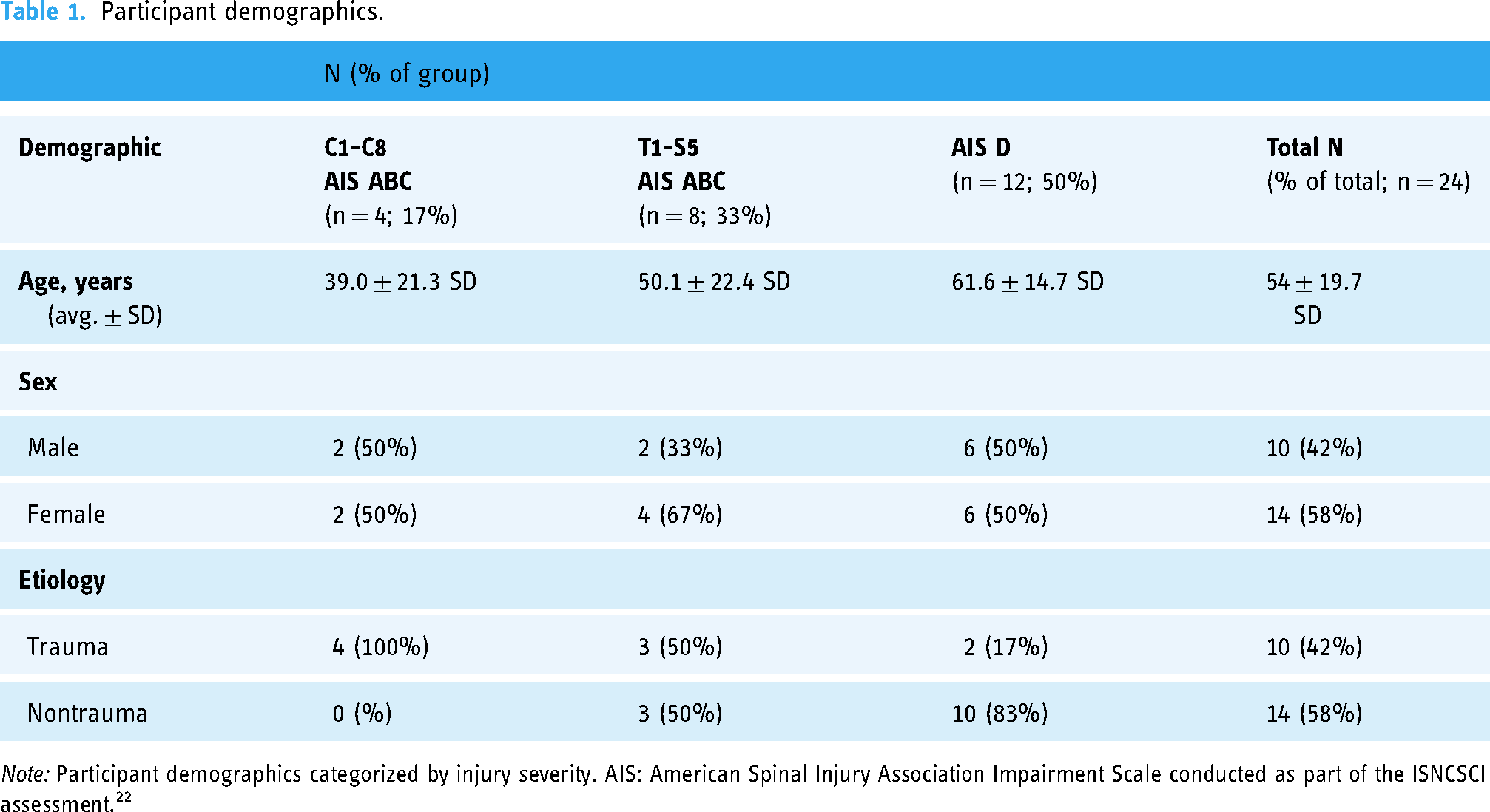
Note: Participant demographics categorized by injury severity. AIS: American Spinal Injury Association Impairment Scale conducted as part of the ISNCSCI assessment. 22
Chosen measures included:
MARS(measuring application quality, functionality, aesthetics, content, subjective quality, and perceived impact)
26
Health Care Provider/Patient/Caregiver Feasibility Questionnaire (assessing acceptance, demand, implementation, practicality, integration, and limited efficacy)
27
Patient-Reported Outcome Measures (PROMs; adaptation of SCI Quality of Life Short-Forms: Social Roles & Activities – Ability to Participate, Independence, Pressure Ulcer Interference, Pain Interference & Behaviour, Resilience; and measures of Self-Efficacy for Managing Chronic Disease 6-Item Scale & Health Utilization)28,29 SCI Secondary Conditions Scale (frequency of secondary complications)
30
Data analysis involved simple descriptive statistics applied to subgroups. Differences between timepoints related to platform analytics, usage of features on the platform, and outcome measures were assessed.
Qualitative methods
Core members of the team (LN, CG, HA, and DW) conducted three focus groups near study conclusion to explore perspectives on the platform, specifically related to the most helpful features, and factors that facilitated or hindered use. Two focus groups were held with clinicians (n = 5) and one focus group was held with patients (n = 4). Clinician focus groups were conducted in-person at PI while the patient focus group was conducted virtually via Microsoft Teams. All focus groups were facilitated using an interview guide, and were recorded and transcribed with consent. The phases of thematic analysis were used to interpret data. 31
A single data coder (MS) began analyses with multiple readings of the transcripts and noting of initial impressions. Preliminary codes were developed systematically, in which related data were grouped. Codes that belonged together were combined into themes that were reviewed in relation to the dataset and discussed with the research team. The final step involved connecting the analysis and refined themes to the research question, the aims of the study, and the broader literature.
Results
Quantitative
The MARS and Feasibility Survey showed that VIP4SCI was viewed as usable, feasible, and useful (Figure 3). Perceived impact averaged around 3.5 to 4.0, with the highest score of 5 corresponding to “excellent.” Platform satisfaction assessed on a −3 to +3 scale ranged from +0.9 to +2.5, demonstrating positive agreement. Self-efficacy related to self-management assessed via PROMs ranged from 5.4 to 7.6 out of 10, with higher scores corresponding to increased confidence. Related to platform usage, clinicians and patients logged on a total of 463 and 393 times, respectively. The lowest amount of login attempts was 1 for both patients and clinicians, indicating that these participants only logged on during onboarding and did not utilize the platform thereafter. The highest amount of login attempts was 87 and 106 for patients and clinicians, respectively. These two numbers reflect outliers, as the vast majority of participants logged in <20 times throughout the study period. In terms of specific platform features, a total of 16 virtual calls were conducted using the platform. Most notably, the resource library received the most clicks, having been accessed 171 times.

Quantitative feasibility and MARS results. Comparisons between outpatient and clinician quantitative data at appropriate timepoints. Results were categorized into respective domains (i.e. feasibility: acceptability, practicality, demand, limited efficacy; MARS: quality of information, subjective quality, perceived impact). Inpatient data is not represented in this diagram due to low n (<5). MARS: Mobile App Rating Scale.
Qualitative
Theme 1: Maintaining a connection
Patients mentioned the necessity to maintain a connection to the hospital postdischarge, emphasizing the feeling of being a short distance away from support. The ability to contact clinicians helped patients feel less alone, which was a common experience when first arriving home and throughout the COVID-19 lockdowns. It appears that VIP4SCI made this transition smoother and helped with staying motivated to therapeutic journeys. Laura: “Being able to know that I still have my umbilical cord to the hospital was an awesome feeling. So, the platform was great for that – making me never feel like I was more than a short distance away.”
Clinicians discussed how the platform helped facilitate the transition from inpatient to outpatient. They noted that the virtual sessions were ideal and helpful for patients who could not come in-person for various reasons (e.g. transportation). In addition, clinicians discussed that since the platform had embedded educational resources, it was ideal for outpatients to work through the resources on their own time as they transitioned back to the community. This made it time-efficient for both clinicians and patients, so treatment time was not spent looking for and/or going through resources but rather on other therapeutic activities.
Subtheme: Communication features
Patients appreciated the communication feature, as it enabled virtual calls with clinicians. The type of messaging tool was not important (i.e. no preference over platform or email), as long as the communication line was open.
Patients also noted that virtual calls as part of therapy were also helpful to ensure that postures and exercises were done correctly. The advice and feedback received from clinicians during virtual calls had a significant impact on patients’ recovery and motivation. They noted that the encouragement they received through virtual therapy was critical for their recovery and progression. Virtual calls were especially important for those patients who could not come to PI in-person. Laura: “I [had a] virtual call with my physical therapist, and that was helpful to make sure that I was doing postures correctly and just being able to show progress and get more advice.”
Clinicians acknowledged that the communication feature may be most valuable for outpatients to continue supporting them in the community; however, they preferred alternative video calling tools (e.g. Webex) based on convenience, existing organizational integration, and higher quality compared to the platform. Clinicians noted that the messaging function worked well but suggested that it could be improved by including pop-up notifications, as otherwise the platform may be forgotten.
Subtheme: Connecting with VIP coaches
Patients in this study appreciated that VIP coaches took the time to introduce the platform to them prior to discharge. Having the VIP coaches thoroughly walk through different aspects of the platform contributed to making the patients feel more comfortable and at ease while using the platform at home. This was especially helpful for patients with low function. Thus, having VIP coaches explain the platform made the platform more accessible for patients. It appears that VIP coaches taking the time to introduce the platform to each patient contributed to building rapport and increased patients’ motivation and comfort to use the platform.
Theme 2: Resources facilitating learning
Patients noted that working through resources on the platform helped address needs and was a great starting point in their therapeutic journey. Specifically, patients reported that the resources helped them gather information on their own, enhancing their sense of autonomy. Independently browsing for information also maintained privacy, because in some cases, patients did not want to share questions with a clinician. John: “The variety of resources available was amazing and I went through a lot of them just for interests’ sake. It was very educational, and I felt it was a great way…to find information [privately].”
Because the library consisted of reliable and highly educational material, patients saved time and energy from using search engines (i.e. Google) and evaluating the quality of information independently. Patients commented on the convenience of having information in one place, for which they described the library as the best feature for learning.
Clinicians noted the importance of referring patients to one trustworthy hub of information. Embedded resources were ideal for outpatients to work through independently at their own pace, which promoted self-management behaviours and freed up valuable therapy time.
Subtheme: Inspiring a holistic outlook on recovery
Patients noted the importance of self-management to recovery. One patient mentioned that VIP4SCI broadened her view of recovery to include domains outside of physical functioning such as emotional wellbeing and stress reduction. John: “I concentrated so hard on sort of the physical aspects of my recovery for a while, and then I found the features that had me think about my emotional and mental well-being and what I was doing to relieve stress and those kinds of things…That part of the program was also helpful to me.”
Theme 3: Barriers to platform use
Subtheme: Goal-setting feature
One limitation mentioned by patients was related to the goal-setting feature (part of self-management tool) within the platform. Patients reported experiencing frustration caused by limited dropdown box options. Some described the goal-setting feature as “funky” and “least helpful.” Overall, patients would have preferred if they could add their own goals instead of choosing from a dropdown menu. Specifically, they noted that being able to add their own goals in the goal-setting feature would make it more individualized to the specific needs of each person.
Subtheme: Too many features
While patients appreciated that VIP4SCI had many features designed to address a variety of needs, some noted that it had “too many,” making it overwhelming to explore efficiently. As a result, some patients did not know certain features existed and failed to explore VIP4SCI in-depth. David: “One of the things just in regard to features was I found there's a lot of features. I didn’t even know there was a feature for contacting clinicians or journal entries, so that's one thing I actually found overwhelming using the VIP system, just that there were so many features. It's kind of hard to navigate through them all.”
Clinicians found some features to be redundant, noting that having “too many” features may discourage patients from use due to the energy and effort required to navigate the platform. They noted a feature was less likely to be used if it accomplished the same goal as an existing process. For example, patients already used a care binder for goal setting. It would be overwhelming and repetitive to record goals on the care binder and on the platform. Lilian (Clinician): “Any time it was a duplication from something else (an already existing system), then it was maybe less likely to be used.”
Subtheme: Technical and practical barriers
Patients described login issues that prevented them from using VIP4SCI regularly. Specifically, they noted the platform did not “remember them” on their personal device, meaning two security questions had to be answered with every login attempt. Related to the communication tools, patients found it frustrating having to re-login to see a new message. It was noted that email would be more convenient and time-efficient, as it is easy to open and read right away. It should be noted that the security precautions built into the platform were implemented in alignment with organizational policy, so the only strategy available would be to better educate participants on the rationale for this issue.
Clinicians noted that having to constantly login to the platform decreased their motivation to use it. Since the platform was viewed as optional, it was not integrated effectively into workflow, and was not a priority when juggling between patients. Clinicians expressed that more time was needed for VIP4SCI to become integrated into practice.
Clinicians in this study reported additional practical issues that interfered with the platform use. They reported that the platform was “optional” to use compared the care binder which was integrated already into clinicians’ workday flow. That simply meant that they used the platform less because it is not as integrated in their day-to-day flow. They also noted that it was challenging to make the platform part of regular work schedule because of added effort and energy required to use it (i.e. logging in). This demonstrates that a platform needs to be easily accessible to improve usability by clinicians. In addition, clinicians noted that the platform was simply not a priority when they are juggling between patients and have more important assessments to conduct.
Theme 4: Platform improvements
Subtheme: Peer discussion forum
Patients noted that a peer group/discussion forum, similar to the /SCI subreddit on Reddit, would strengthen VIP4SCI. They reported that being able to communicate with others, postquestions and answers regarding different topics, and exchanging ideas with others about topics such as recovery and workout plans would be beneficial for them, demonstrating the importance of peer support.
Subtheme: Easier access through a mobile app
Another recommendation made by patients was using the platform as a phone app which would make it easier and more accessible to use since people typically use their phones on a regular basis. Similarly, clinicians noted that a mobile app would be more user-friendly. Clinicians felt it would be easier to introduce VIP4SCI to patients as an app during therapy to prevent the need for a laptop. They noted that having the option to use the platform as both a desktop and mobile app may be ideal for clinicians who do not wish to use phones for clinical purposes. Furthermore, clinicians noted that having the option to connect with other clinicians on the platform may encourage usage.
Subtheme: Reminders and prompts to use the platform
Clinicians needed more prompting to use the platform such as an icon you can easily see/click on and more notifications when patients use the platform, set goals, etc. In addition, clinicians noted that the more patients use the platform; the more reminder emails will encourage clinicians to log in and see what's happening. Clinicians also noted that a reminder at the time of a patient's admission to hospital may help incorporate the platform into schedule. Another way to prompt clinicians and improve the communication feature is to notify the clinician of messages, otherwise they are less likely to check the platform regularly for messages. This is due to other priorities and the added time/energy required for clinicians to regularly check the platform. Katie: “I think that would be more convenient for people from the perspective of like, everyone's looking at their phones all the time. If you had a red blinking thing on it, you’re more likely to go into the app to see what notification you have on it.”
Discussion
Principal findings
VIP4SCI was viewed as usable, feasible, and useful by both patients and clinicians despite low uptake and barriers to adoption in practice. The study is unique in that it captures the experiences of both persons with SCI and clinicians to gauge the feasibility of a virtual e-health solution to be implemented into day-to-day clinical practice and/or be used as a self-management tool to facilitate care transitions. It is also one of few studies that report on both the potential benefits and setbacks to developing, implementing, and maintaining an e-health platform to support persons with SCI across the care continuum in promoting self-management. 32
Patients and clinicians perceived the platform as valuable to maintain a connection postdischarge from rehabilitation and support independent learning. VIP4SCI provided opportunities for patients to connect with therapists virtually to address health concerns and consult on treatment plans, providing an alternate care method during the unpredictable time of the COVID-19 pandemic. Additionally, it was noted that VIP4SCI contributed to more efficient therapy provision in having a singular hub of reliable resources to share with patients, rather than independently searching and vetting for such information during therapy sessions as per current state practice. The remainder of the discussion is organized into three broader themes identified by patients and clinicians related to their experiences using VIP4SCI and how it compares to existing work in the field. The three themes include: (1) fostering a sense of connection; (2) promoting independent learning and self-management skill development; and (3) barriers to integration into practice.
The COVID-19 pandemic resulted in numerous service interruptions and changes in the way care was delivered at PI. It was difficult for patients to feel connected to the rehabilitation program in the midst of hospital capacity restrictions and unexpected disruptions to therapy sessions. In alignment with studies evaluating the psychosocial impact of the COVID-19 pandemic on the SCI community, several participants mentioned experiencing feelings of loneliness and disconnectedness.33–36 Following the use of VIP4SCI, participants noted a newfound sense of connection to the rehabilitation program at PI, and many felt reassured knowing that there was a means of receiving support if needed at any point during their care journey. This is consistent with findings on a mobile app for pressure injury prevention that speak to the comfort felt in knowing that clinicians and evidence-based knowledge are easily accessible to provide support. 32 Unanticipated benefits postintervention, particularly related to a sense of relief knowing that needs were being meaningfully addressed, was a similar finding in the current study. 20 Notably, a participant mentioned that the use of VIP4SCI broadened her view on recovery, suggesting that the effects of such a platform can stretch beyond objective measures in providing additional individualized benefits related to support, connection, and empowerment. 20
Findings from this study are consistent with similar initiatives evaluating virtual-based platforms, particularly related to the role of coaches in motivating and encouraging participants as well.19,20,32,37 Houlihan et al. found that coaches played a critical role in empowering patients to manage their own health conditions in acting as a facilitator to self-management behaviours, similar to the effect of VIP coaches in the present study. 20 While the platform enabled connections between patients, clinicians, and coaches, participants noted that a suggestion for improvement may be to incorporate more peer support opportunities within the platform. Peer support has been shown to play a pivotal role in promoting life satisfaction, participation, and the facilitation of unmet SCI-related needs. 33 Particularly during widespread crises such as the COVID-19 pandemic, it would have been beneficial to have had incorporated peer support features within the platform to combat feelings of social isolation between patients as well. 20
For persons with chronic illness or disability, promoting behaviour change in the context of self-regulation can help prevent further morbidity and mortality. Using the HAPA behaviour change model to inform platform features was intentional to promote self-management skill development in persons with SCI, as such to increase confidence in being able to manage one's own condition independently. Greater emphasis on self-management can remove feelings of reliance and dependency on clinicians, thereby having a downstream effect on the efficiency of rehabilitation programs and the broader healthcare system overall. 37 As reflected in both the quantitative and qualitative data, participants found that VIP4SCI increased self-efficacy related to self-management and increased interest in learning about ways to effectively manage their condition. Amann et al. expressed how patient participants benefitted from having a complementary means of patient education consolidated in the form of a mobile app to enable the processing of information at their own paces, ultimately fostering feelings of self-determination and autonomy. 32 These findings are consistent with VIP4SCI, as participants highlighted how having access to the resource library through the platform enabled independent learning. While the facilitation of goal-setting via weekly check-ins with the VIP coaches helped promote behaviour change, the long-term maintenance of such behaviours could not be evaluated as a result of the platform shutdown. A longitudinal study of self-management-related behaviour change enacted by an e-health solution similar to VIP4SCI would be beneficial to understand whether the incorporation of HAPA constructs and facilitation by VIP coaches would have a lasting effect. 23
While VIP4SCI was received positively by those that did use it, barriers to implementation and accessible use made it challenging to form significant conclusions. Findings related to barriers are consistent with current literature, with a study on an app for pressure injury prevention reporting on similar challenges related to a lack of organization and clinician engagement. 32 Potential strategies for better integration into clinical practice, might include a more enhanced alignment of the platform with existing processes and technologies already used by the Care Team. A challenge to doing this was related to some aspects of these care processes being mandated across the entire organization, with some barriers to change associated with customization within a singular program. Clinician engagement may be improved by eliminating the burden of adopting a new technology and minimizing the potential for duplication of work. This strategy may help mitigate the potential increase in clinician workload. Similarly, improving ease of access to the platform (e.g. consider an app version) may also contribute to improved clinician uptake. Additionally, while the hospital supported the integration of the study into clinical care, clinician participation in the study was optional. This meant there was no corporate expectation for clinicians to engage with patients on the platform. As such, when clinicians may have been faced with competing workload priorities, this may have led to a reduction active participation on the platform.
Finally, there were no formal incentives for physicians or other members of the Care Team to utilize platform. The hope was that by providing additional means of communication with members of the Care Team, patients would benefit from more fulsome and timely access to care. However, given that physicians were the only members of the Care Team working in a fee for service care delivery model, this may potentially have acted as a disincentive to using the platform since they could not bill for communications on the platform.
Limitations
This study provides insight into the effectiveness of an e-health platform; however, data should be interpreted with caution as the small sample size limits generalizability. It was anticipated that the sample size would reflect current inpatient and outpatient admission rates, however participant recruitment was difficult due to the unpredictable, changing hospital climate brought upon by COVID-19 (study conducted November 2020 to April 2022). Toward the end of the study, due to COVID-19 constraints, we were unable to continue the block randomization process. Multiple outbreaks in patient units hindered communication with current and potential participants, resulting in challenges finding appropriate times for onboarding and delays with completing the questionnaires if done in-person. At some points, VIP coaches were unable to conduct weekly check-ins and effectively facilitate goal-setting behaviours with patients. In addition, using VIP4SCI alongside patients was not a priority for clinicians who were navigating changes to program policies as a result of the pandemic. These factors contributed to a small participant pool and low response rate to the surveys, thereby limiting the representativeness of the quantitative results to the larger SCI population. More rigorous statistical analyses could not be performed due to the lack of available survey data, making it difficult to form firm conclusions on the study findings as a whole. In terms of barriers to platform development and integration, the use of an external IT developer was a core roadblock. Several issues arose with accessibility (i.e. having to answer security questions with every login attempt) and platform function (i.e. glitches and response delays). In addition, certain external applications (i.e. WebEx) were used over the platform because of organizational policy. These applications were not used prior to the study, but were deployed in response to COVID-19. Frustrations related to accessing the platform negatively impacted platform usage, as participants would resort to more familiar tools. As such, partnering with an in-house developer and/or leveraging applications with existing organizational approval may have streamlined platform uptake. This would enable a more functional tailoring of the platform features to better meet the needs of clinicians and their patients. As a result of not having VIP4SCI embedded within day-to-day practice by mandate, its utilization was not effectively integrated by clinicians. Whereas active facilitation from VIP coaches facilitated use with patients, clinicians were not trained in a similar fashion. We were in the midst of studying the effect of enhanced facilitation when VIP4SCI was terminated by the vendor due to business closure. The enhancement of training for effective implementation and culture shift is an important consideration for future studies (Table 2).
Lessons learned.

Potential directions for future research
Despite the low uptake and unexpected closure, learnings from the platform provide meaningful considerations for future initiatives. Specifically, the appreciation for a platform that enables the coordination of care and desire for increased access suggests promise in the field of e-health. Further research, using principles rooted in behaviour change with a focus on transitions of care and self-efficacy promotion, is needed to evaluate the impact of self-management skill development and virtual care on promoting improved quality of life in persons with SCI. Moreover, there is an urgent need to explore the usage of e-health interventions on facilitating transitions of rehabilitative care, thereby leveraging the current digital age to coordinate and streamline service delivery. A longitudinal follow-up study may be beneficial to assess the sustainability and long-term effectiveness of the platform.
The results of the evaluation of the platform have been very instructive, and have informed existing and future work in this domain. Findings from the study are in the process of being incorporated into the development of current e-health studies and clinical implementation. The next iteration of the development of a self-management application for persons with mild traumatic brain injury 38 is underway, and design features will be embedded to more effectively align with existing clinical processes to promote uptake.
Conclusion
Although quantitative findings were limited, the qualitative results show that e-health solutions have potential value for coordinating care transitions and promoting self-management skill development in persons with SCI, as demonstrated by the general positive agreement shared by both patients and clinicians. VIP4SCI helped patients feel connected and provided opportunities for self-directed learning, thereby contributing to a sense of personal autonomy and strengthening independence in information-seeking. Both patients and clinicians appreciated the purpose and goals underlying VIP4SCI, and as such viewed the platform with positive regard even when providing suggestions for change. The limited sample size and low response rate prevent the formation of firm conclusions in this domain, however future virtual-based programming can be informed by learnings to ensure subsequent initiatives address limitations to uptake and accessibility and consider facilitators to promote sustained use. With the world becoming increasingly digital, more research is needed to understand whether an e-health solution can promote the development of sustained self-management behaviours and effectively facilitate care transitions for persons with SCI across all stages of the rehabilitation journey.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241272618 - Supplemental material for Parkwood's VIP4SCI platform: A virtual e-health self-management solution for persons with spinal cord injury across the care continuum
Supplemental material, sj-docx-1-dhj-10.1177_20552076241272618 for Parkwood's VIP4SCI platform: A virtual e-health self-management solution for persons with spinal cord injury across the care continuum by Luxshmi Nageswaran, Charlie Giurleo, Merna Seliman, Heather K Askes, Zeina Abu-Jurji, B Catherine Craven, Anna Kras-Dupuis, Julie Watson and Dalton L Wolfe in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241272618 - Supplemental material for Parkwood's VIP4SCI platform: A virtual e-health self-management solution for persons with spinal cord injury across the care continuum
Supplemental material, sj-docx-2-dhj-10.1177_20552076241272618 for Parkwood's VIP4SCI platform: A virtual e-health self-management solution for persons with spinal cord injury across the care continuum by Luxshmi Nageswaran, Charlie Giurleo, Merna Seliman, Heather K Askes, Zeina Abu-Jurji, B Catherine Craven, Anna Kras-Dupuis, Julie Watson and Dalton L Wolfe in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241272618 - Supplemental material for Parkwood's VIP4SCI platform: A virtual e-health self-management solution for persons with spinal cord injury across the care continuum
Supplemental material, sj-docx-3-dhj-10.1177_20552076241272618 for Parkwood's VIP4SCI platform: A virtual e-health self-management solution for persons with spinal cord injury across the care continuum by Luxshmi Nageswaran, Charlie Giurleo, Merna Seliman, Heather K Askes, Zeina Abu-Jurji, B Catherine Craven, Anna Kras-Dupuis, Julie Watson and Dalton L Wolfe in DIGITAL HEALTH
Supplemental Material
sj-pdf-4-dhj-10.1177_20552076241272618 - Supplemental material for Parkwood's VIP4SCI platform: A virtual e-health self-management solution for persons with spinal cord injury across the care continuum
Supplemental material, sj-pdf-4-dhj-10.1177_20552076241272618 for Parkwood's VIP4SCI platform: A virtual e-health self-management solution for persons with spinal cord injury across the care continuum by Luxshmi Nageswaran, Charlie Giurleo, Merna Seliman, Heather K Askes, Zeina Abu-Jurji, B Catherine Craven, Anna Kras-Dupuis, Julie Watson and Dalton L Wolfe in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank our partners, Spinal Cord Injury Ontario, and the University Health Network for their continued support in this and other initiatives. We would also like to acknowledge the contributions of ForaHealthyMe Inc. related to platform development and maintenance for the duration of the study, and most importantly, thank all the patient, caregiver, and clinician participants who dedicated their time to this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was generously funded through Craig H Neilsen Foundation (grant #533045).
Guarantors
LN and DW
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.