
Abstract
Background
Type 1 diabetes requires making numerous daily decisions to maintain normoglycemia. Support is an evidence-based self-guided web application for type 1 diabetes diabetes self-management.
Objective
Evaluate users’ satisfaction with Support and investigate changes in self-reported frequency of-, fear of- hypoglycemia, and diabetes-related self-efficacy.
Methods
Adults from a Quebec type 1 diabetes registry used Support. Data was collected through online surveys or extracted from the registry at 0, 6, and 12 months (number of episodes and fear of hypoglycemia). At 6 months, participants reported satisfaction with Support and diabetes-related self-efficacy. A sub-group of 16 users was interviewed about their experience. Transcripts were analyzed using inductive and deductive approaches.
Results
In total, 207 accounts were created (35% men, 96% White, mean age and diabetes duration: 49.3 ± 13.8 and 25.2 ± 14.7 years). At 6 months, the median [Q1; Q3] satisfaction was 40/49 [35; 45] with a mean decrease in hypoglycemia frequency of 0.43 episodes over 3 days (95% CI: −0.86; 0.00, p = 0.051) and of −1.98 score for fear (95% CI: −3.76; −0.20, p = 0.030). Half of the participants reported increased diabetes-related self-efficacy.
Conclusions
Participants reported a high level of satisfaction with Support. Its use has the potential to facilitate hypoglycemia management and increase diabetes-related self-efficacy.
Trial registration
This study is registered on ClinicalTrials.gov NCT04233138.
Introduction
Digital health tools for health care communication and delivery can be a more accessible and flexible alternative than in-person approaches. 1 Compared to other digital health solutions (e.g., mobile applications [apps], virtual reality, web apps) have lower development costs, can be faster to develop and require fewer updates and technical support over the long-term. 2 This makes them suitable to deliver chronic disease self-management education and support to a larger population, especially when regular content updates are needed. 3
People living with type 1 diabetes (PWT1D) need to make numerous daily decisions to maintain an adequate glycemic level and avoid complications. 4 Factors such as food intake, physical activity, stress, and change of routine3,5,6 need to be considered to maintain normoglycemia. Hypoglycemia is considered one of the main barriers to optimal glycemic management. 7 Frequent episodes can lead to fear of hypoglycemia which can consequently lead to adaptative behaviours (e.g., increasing food intake, avoiding physical activity) which, in turn, potentially increase the risk of hyperglycemia and long-term complications. 7 Therefore, for PWT1D, diabetes self-management education and support (DSME/S) are essential.
DSME/S aims to facilitate long-term diabetes self-care by providing key concepts of diabetes management (e.g., factors influencing glycemic control) and by training individuals to engage in self-management behaviours (e.g., carbohydrate counting, insulin dose adjustments). 8 Compared to in-person DSME/S, online DSME/S allows people to learn at their own pace, 9 and can potentially lead to higher satisfaction. 10 In situations of limited healthcare resources, self-guided tools (i.e., absence of live involvement from healthcare professionals (HCPs)) can further decrease the DSME/S programme maintenance cost and add flexibility to the learning process. 11 Continuous evaluation is essential to understand how people are using such tools in order to an ongoing improvement on the use of the platform and its influence on clinical outcomes. 12 In addition, as behaviour change theories facilitate the understanding of behaviour mechanisms and increase the precision of interventions, their incorporation in DSME/S web apps can potentially lead to better clinical outcomes and intervention engagement.13,14 However, there are limited self-guided DSME/S web apps for type 1 diabetes (T1D) that are informed by behaviour theories or frameworks, in particular for adults 11 and a lack of evidence on web apps’ development to ensure user satisfaction.11,12
Support is a self-guided web app developed with and for adults with T1D with a focus on hypoglycemia. Through a proof-of-concept study, we investigated (a) user satisfaction with Support and (b) changes in the self-reported frequency of hypoglycemia, in the fear of hypoglycemia, in self-efficacy in diabetes self-management (DSM) (in preventing hypoglycemia and in managing glycemia). Potential optimization of the web app to facilitate its use and training in hypoglycemia management will also be discussed. We expected that Support would be appreciated by users since previous digital interventions on chronic health conditions received a high satisfaction score 15 and that its use would be associated with reduced fear and frequency of hypoglycemia and with increased self-efficacy in DSM. 16
Methods
This mixed methods concurrent triangulation study combined a registry-based quasi-experimental and a phenomenological design 17 (ClinicalTrials.gov. registration number: NCT04233138). The study was approved by the Montreal Clinical Research Institute's Research Ethics Committee and participants provided online informed consent. The results are reported based on Mobile Health Evidence Reporting and Assessment Checklist. 18
Intervention
Participants had access to the Support web app (French or English) 19 for 12 months with bi-weekly e-mail newsletters during the first 6 months. Briefly, Support was developed by a team of patient partners, HCPs and researchers specialized in T1D (e.g., certified diabetes educator, dietitian, nurse, psychologist, endocrinologist). All content is based on the most recent literature, and peer-reviewed by patient partners and HCPs. The learning modules are divided into six categories with several courses in each. Categories have three learning levels (basic, intermediate, and advanced) and course lengths vary from 5 to 20 min. Completing the basic level unlocks the intermediate level and so forth. Four learning paths are available based on the diabetes treatment profile (Supplemental information I). Several features are included (such as videos, testimonials, downloadable PDF) to enhance user experience (Supplemental information II). The choice of features was guided by the Behaviour Change Wheel, 20 its related behaviour change techniques, 21 and evidence from previous literature. 11 At onboarding, every participant needs to complete a mandatory module on hypoglycemia.
Recruitment
Recruitment was done using a registry of PWT1D in Quebec (BETTER: BEhaviours, Therapies, Technologies, and hypoglycemic Risk in T1D 22 ). Adults (≥ 18 years old (y.o.)) with a self-reported diagnosis of T1D ≥ 1 year, and daily use of ≥ 4 insulin injections or an insulin pump were invited by email. Other inclusion criteria were having access to the Internet, an active e-mail address, and understanding English or French. People with ongoing pregnancy or illnesses limiting diabetes care or limiting access to educational tools (e.g., dementia and blindness) were excluded.
Data collection
At baseline, socio-demographic information and diabetes history data were extracted from the BETTER registry. Participants completed an online survey asking about their readiness to change for improving glycemic management, their level of health literacy, 23 and the number of hypoglycemia episodes (blood glucose <4.0 mmol/L) in the last 3 days. Participants also completed the 33-item Hypoglycemia Fear Survey-II (HFS-II). 24 Questions related to hypoglycemia were repeated at 6 and 12 months. The presence of elevated fear of hypoglycemia (i.e., a score of ≥ 3 on any of the items in the HFS-II 25 ) was calculated. At 6 months, participants were asked to report on changes in their confidence level in self-efficacy (in preventing hypoglycemia and in managing blood glucose).
At 6 months, the level of satisfaction with Support was measured using a 7-question face-validated satisfaction questionnaire (Likert scale from 1- strongly disagree to 7- strongly agree).26,27 Two questions were purposively formulated in a negative form to ensure participants read questions properly. The score was reversed before analysis for a maximum total score of 49. Thus, data from respondents who answered all “1” or all “7” was removed from the analysis. A single question rating overall appreciation from 1 to 10 was also asked. Participants selected a maximum of three most preferred features from a list of 14 and answered two mandatory open-ended questions on what they liked most about Support and what should be improved. The study-specific questionnaires were administered online through Research Electronic Data Capture 11.1.0.
Web app usage and engagement
Google Analytics was used to track the usage of the web app (number of page views, number of sessions, and average session duration) and of specific embedded features (calculator use, downloaded PDF documents, and submitted quizzes). The number of page views included only pages with specific uniformed resource locator (URL; i.e., learning content, dashboard, media library, frequently asked questions, discussion forum, and news blogs) and included pages seen multiple times. They were reported per period of 6 months and used to describe engagement with the web app. When a user logged in to Support and remained active, a session was tracked. 28 Usage of the calculator was defined as the number of times a result was displayed, PDF documents referred to the number of downloaded documents, and a quiz was considered when the user clicked on “submit.” The number of posts on the discussion forum was analyzed from the front end of Support. Mailchimp tracked the number of opened and clicked newsletters (out of 13 sent). 29
Natural evolution of hypoglycemia within the BETTER registry's participants
Using the BETTER registry, we contrasted the change in the frequency and fear of hypoglycemia observed among the Support participants from baseline to 6 months to the natural evolution observed in the registry over a similar 6-month period. The data included in this description are from participants in the registry not part of the actual study but who met the inclusion and exclusion criteria.
Quantitative data analysis
Descriptive analyses are presented (median and interquartile range or mean and standard deviation). Cronbach's alpha was used to measure the reliability of the satisfaction questionnaire. Pearson correlation, paired t-tests, and independent t-tests were performed. Analyses were conducted using SPSS Statistics version 28.
Semi-structured interviews
At 6 months, semi-structured individual interviews based on a phenomenological design were conducted to deepen the understanding of the participants’ experience using Support (content and format). Of those who completed the satisfaction questionnaire, 16 users were included. To decrease recall bias, four participants were randomly selected, using R Studio, for every 25 participants who completed their first 6 months. To ensure an equal number of men or women, purposive sampling was employed with the last group of 25 participants. Participants were excluded if they explicitly expressed never using Support.
The interviews lasted about 60 min and were conducted in French on Microsoft Teams. A doctoral student (LFX), trained in qualitative data collection and unknown to the participants, conducted all interviews. The interview guide was developed following work from Arnold et al. 30 with guidance from HCPs (dietitians, nurses, and an endocrinologist) and patient partners. It consisted of five sections with a total of 24 questions, including 20 open- and four closed-ended questions. Participants were invited to share their general experience using the healthcare system and then to focus on their experience with Support. Factors influencing their use of Support, feedback on the contents and the features, and the consolidation of knowledge learned from Support into their DSM were explored. Following the interview, participants received a summary of their interview's key points by email and were asked to comment within 2 weeks. Each participant was sent an electronic gift card (40 CAD) for their participation.
Open-ended questions from satisfaction questionnaires were qualitatively analyzed along with the semi-structured interview transcripts using NVivo (QSR International, Melbourne, Australia). Two researchers (LFX and AH) performed the initial inductive coding independently on two transcripts randomly selected. Then, all the interviews were analyzed with the created coding book in an iterative approach. Codes were refined as needed (e.g., through rewording). After independently coding all transcripts, 100% agreement was achieved through discussion. Codes were grouped into themes using a combination of inductive (i.e., using concept mapping) and deductive methods (i.e., guided by the interview questions). 31 Analyses were performed in French and were translated into English using a forward-backward translation process for publication.
Results
Satisfaction and change in hypoglycemia
From October 28th, 2019, to September 30th, 2021, 207 participants consented and created a Support account and were included in the analysis (Supplemental information III). The baseline characteristics are summarized in Table 1.
Baseline characteristics of support users.

HbA1c: Hemoglobin A1c
At 6 months, 169 participants answered the satisfaction questionnaire (Cronbach's alpha of 0.88). The median [quartile 1; quartile 3] score was 40/49 [35; 45], which is similar to the overall rating of Support on a 10-point scale (8 [8;9]) (n = 166) (Supplemental information IV). During the first 6 months, the self-reported frequency of hypoglycemia over 3 days decreased by −0.43 episodes (95% confidence interval [95% CI]: −0.86, 0.001; n = 166) from 2.47 episodes to 2.04 episodes. Self-reported hypoglycemia from 6 to 12 months showed an average additional decrease of −0.51 (95% CI: −1.13 to 0.12; n = 89) (Table 2). In contrast, in the BETTER registry, a sub-group of 244 participants, reported on average no change in the number of hypoglycemic episodes (0.01 episodes per 3 days, 95% CI: −0.22, 0.25) during the same 6-month period.
Changes in hypoglycemia frequency and fear.

A decrease in HFS-II total score (out of 132) was observed during the first 6 months (−1.98; 95% CI: −3.76 to −0.20; n = 170) and by −10.20 (95% CI: −13.84, −6.56; n = 100) during the following 6 months (Table 2). The percentage of users having elevated fear of hypoglycemia at baseline, 6-month, and 12-month were 82% (n = 166/203), 53% (n = 78/146), and 48% (n = 53/111), respectively. In the BETTER registry, there was no change in their fear of hypoglycemia during the same period (mean 0.94 95% CI: −0.64; 2.52; n = 248). The changes in the frequency of hypoglycemia and in fear of hypoglycemia were not associated with satisfaction scores with the web app (respectively r = −0.064; p = .442, and r = 0.021; p = 0.786) during the first 6 months. At 6 months, about half of the users reported an increase in their confidence in managing blood glucose levels (47%, n = 79) and in their confidence in preventing hypoglycemia (51%, n = 85) (Supplemental information V).
Support usage
The use of Support is described in Table 3. No web app usage was tracked by Google Analytics for 25 users due to their privacy parameters and four users did not receive newsletters due to a human error (their email address was not added to the newsletter list).
Web app usage during the first 6 months of intervention.
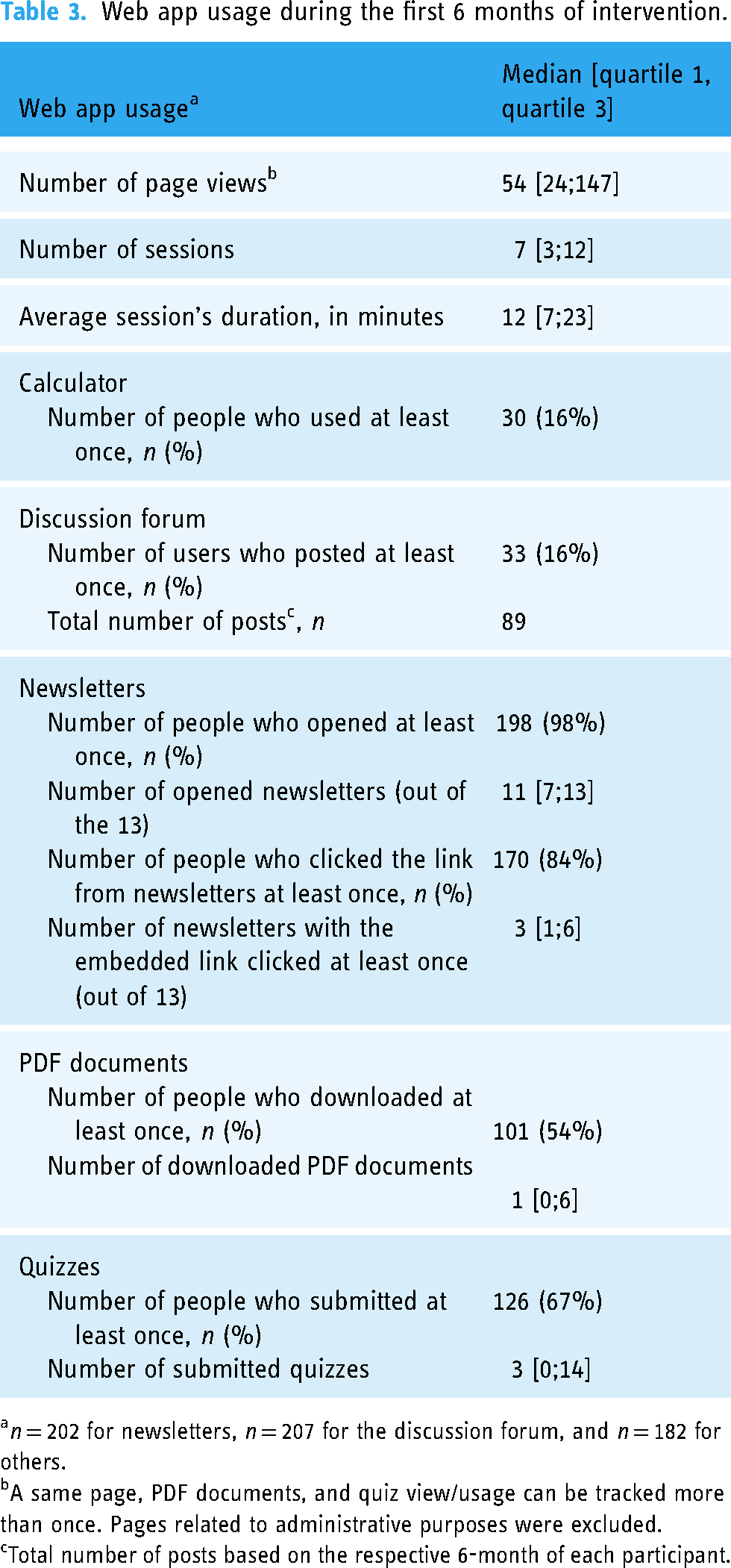
n = 202 for newsletters, n = 207 for the discussion forum, and n = 182 for others.
A same page, PDF documents, and quiz view/usage can be tracked more than once. Pages related to administrative purposes were excluded.
Total number of posts based on the respective 6-month of each participant.
The median number of page views during the first 6 months was 54 [24;147] and decreased to 0 [0;10] in the following 6 months. Based on a stratification analysis with the median split of the number of page views in the first 6 months (n = 90 for lower engagement vs n = 92 for higher engagement), all baseline characteristics were similar except that people with a higher engagement reported a slightly higher readiness for glycemic management's change at baseline (9.0 ± 1.0 vs 8.8 ± 1.1; p = 0.047). The number of page views was not associated with changes in hypoglycemia frequency (r = −0.008; p = 0.917) nor fear (r = 0.004; p = 0.961) during the first 6 months
Among the 14 listed features, the most preferred features were downloadable PDF documents, blog news, newsletters and videos with an equal number of votes, and quizzes. Discussion forums, certificates for course completion, virtual rewards, and glossary definitions were the least frequently selected features.
User's experience with Support
The interviews were held between February 2 to June 30, 2021. Thirty-one invitations were sent. Three participants declined, 11 didn’t respond, and 17 accepted. One participant admitted not using Support despite creating an account and was therefore not interviewed. The mean age of the 16 participants (50% women, 100% White) was 53.8 ± 16.1 years (ranging from 27 to 79) with a mean diabetes duration of 26.5 ± 14.7 years. Among those participants, the median number of page views on Support was 130 [30; 323]. Based on descriptive analyses, the change in the self-reported frequency of hypoglycemia during the last 3 days was −0.4 ± 2.8 episodes and total fear of hypoglycemia was −1.98 ± 11.75 during the first 6 months. Only one participant provided comments after receiving the interviewee's summary (i.e., by highly suggesting the use of a mobile app instead of a web-based one).
Interview code saturation (i.e., information was repetitive and no new code occurred 32 was reached after 14 transcripts. Feedback and suggested modifications are summarized in Supplemental information VI. Participants reported on the factors that could impact their experience with Support and these factors were further divided in relation to the content and the format (Figure 1). Examples of quotes can be found in Supplemental information VII.

Factors facilitating the use of support for diabetes self-management.
Experience with the content
The majority of the participants expressed the importance of having content that is accessible, personalized, and credible. They suggested unblocking all modules to increase accessibility and flexibility in navigating the content. Having information that was concise and easy to understand (e.g., using PDF documents to summarize the information or delivering information with videos) was reported among the main strengths of Support. A few participants stated that the length of the content impacted its accessibility. They appreciated that a written module could be completed within 10–15 min and a video between 2 and 4 min, as lengthy content can decrease their motivation in accessing the information.
Many participants elaborated on the need for having personalized information, that should be level- and need-adapted, and allow them to integrate the new skills into their daily life. A participant suggested having “a knowledge validation questionnaire” (woman, 37 y.o.) at the beginning to guide users to the appropriate level of content. As suggested by our users, diabetes duration can be a potential factor influencing their level of understanding. The feature “Case studies with the six characters” was positively viewed by some participants as it can potentially help users save time by identifying the scenario corresponding to their needs, going beyond the basics, and making direct applications.
The credibility of the information was associated with scientifically up-to-date information and the involvement of HCPs in creating the content and monitoring the forum (e.g., have HCPs involved and supervised the discussion forum).
Experience with the format
Some participants explained that they would need active exposure to the web app's information such as through email newsletters, social media, or reminders from HCPs. Although categorization of the information was mentioned to facilitate information searching, some participants shared difficulties in navigating Support, especially not understanding how each section or feature was connected. To increase accessibility, some participants suggested transferring to a mobile application because “it's easier to log on the phone than on a computer.” (woman, 37 y.o.)
The web app format should be personalized through flexibility in the learning process and the ability to track self-progress. Many participants appreciated that Support is completely online and self-guided allowing them to “stop at any moment and resume where [they] were” (woman, 27 y.o.). Compared to in-person classes where participants might only “retain 25% of what they heard in 4 days” (woman, 67 y.o.), being able to repeat the modules on Support allowed them to revisit information. The dashboard was mentioned as a feature that facilitated self-tracking and personalized the learning progress based on user needs.
Some interactive features received mixed feedback. On the one hand, participants found that the interaction between peers in the discussion forum allowed them to “know that [they are] not alone in [their] situation” (woman, 60 y.o.). On the other hand, some participants expressed that questions asked in the forum by others were not relevant to them and did not feel the need for referring to the forum. Similarly, concerning gamification, some mentioned it might facilitate the learning process (e.g., with the quizzes) and maintain motivation (e.g., through the trophies), though others expressed it had no impact on their use of the web app. Participants appreciated interactive features that align with their expectation or objective of using Support, such as quizzes that helped “confirm whether [they] understood the content”. (man, 75 y.o.)
The aesthetic aspects were also mentioned during the discussion. One participant reported that “I like the visuals because it's attractive and simple. It's nothing too childish nor adultlike or serious.” (woman, 32 y.o.) and another suggested having a greater contrast to facilitate the reading. In addition, a participant suggested the integration of an in-person component to the intervention, as “[an online intervention] is a computer and can’t be compared with a human. It is cold and has no [human] contact”. (man, 42 y.o.) As a future direction, a participant also proposed to expand the web app for family and friends of people with T1D to increase their “medical literacy”. (man, 79 y.o.)
Discussion
Users reported an overall high satisfaction after 6 months of use and our results show the potential of Support in decreasing the self-reported frequency and fear of hypoglycemia. There was also an increased self-efficacy for preventing hypoglycemia and for managing blood glucose levels after having accessed Support. Engagement in Support was greater during the first 6 months than in the subsequent ones and the engagement was similar across people from different socio-demographic backgrounds (e.g., age, gender, number of years of T1D duration). Features supporting information viewing, such as case studies and news blogs, were the most appreciated. When users expected to receive peer-to-peer interaction, they tended to appreciate social support-related features such as testimonial videos and the discussion forum.
The high level of user satisfaction can be related to the development and delivery method of Support compared to other in-person DSME/S interventions. 19 To our knowledge, Support is the first self-guided web app for PWT1D built using a behaviour change framework. The material is evidence-based and peer-reviewed. These characteristics bridge gaps in the development of digital healthcare tools, namely the user's distrust in the information 33 and the lack of an evidence-based design. 34 Its development by a multidisciplinary team includes PWT1D participating in every step of the development can contribute to increased acceptability by the end-users given their shared experiences and needs.12,35 The decrease in self-reported frequency and fear of hypoglycemia after 6 and 12 months of accessing Support is comparable to results reported by other DSM programmes for PWT1D. For instance, in a 6-week in-person intervention, 23 participants were taught about hypoglycemia symptoms, causes, and consequences of impaired awareness of hypoglycemia. The intervention was delivered over three weekly full-day group sessions, homework using home glucose monitoring for two weeks, and one final full-day group session in week 6. Participants reported significant improvement in hypoglycemia awareness after 12 months and a decreased median range rate of severe hypoglycemia. 36 In another in-person programme, 81 PWT1D were gathered in 12 group lessons of 90 min each for a total of 6 weeks. The programme focused on intensive insulin therapy, detection and treatment of acute complications, and prevention and early identification of late complications. An improvement in hypoglycemia awareness and decreased incidence of severe hypoglycemia were reported after 6 months of the programme. The self-guided online delivery format is an alternative to in-person programmes.36,37 It provides the opportunity to reach a greater population that may not have physical access to those programmes and allow users to learn at their pace. 38
Similar to previous online interventions, 39 our results show a decrease in engagement with time and low usage of downloadable PDF documents, calculators, and newsletters in general. This low feature usage can be explained by the method used for measuring it. For example, downloadable PDF documents can be viewed in a browser without being downloaded, whereas only actual downloaded documents were tracked by Google Analytics. The absence of newsletters in the second 6 months may partially explain the lower engagement because our results show that the newsletters were mainly used to obtain information rather than promote engagement with Support. Some participants explained that when receiving sufficient information from the newsletters, they did not perceive the necessity to log in online or click the links; while others only connected to the web app when they received a reminder as an external stimulus. The decreased engagement can also be explained by the fact that users perceived Support as a source of information and once they finished viewing the content relevant to them, they might only refer to it based on their needs. Therefore, a decreased engagement (measured by the number of page views) is to be expected.
Limitations
Our study has some limitations including the absence of Anglophone users for the interview and the lack of ethnic diversity. Our interviewed participants also had a higher engagement than other users, indicating a greater preference for using digital tools for DSM or higher digital literacy. These participants were also included in the second 6 months’ engagement analysis, their interview invitation might have encouraged them to use the web app during this period. Recruitment within diverse cultural communities could improve the sample's diversity and enhance the findings’ generalisability. When responding to the satisfaction survey, some participants might not have explored all the components of Support. This reflects one of the challenges in delivering digital interventions, as it is often difficult to evaluate if the users received the intervention content in the intended way. 40 During the intervention, we noticed that some participants were not receiving the newsletters due to human errors. This lack of fidelity in the intervention delivery highlights the need for having utility and feasibility studies before larger pivotal studies to advocate adjustments needed in future intervention deliveries. We also encountered challenges in tracking the usage data, as 25 (12%) of the users had no usage data from Google Analytics due to privacy settings. The selection bias can also be present due to the timing and method of recruitment. This study occurred during the coronavirus pandemic when people's lifestyles, including the use of digital tools, were affected.41,42 Participants were recruited through the BETTER registry. However, the recruitment for the registry was also slowed down at the beginning of the pandemic having to move from primarily in-person clinic-based recruitment to mainly online. These aspects might restrict the recruitment of people having a greater interest in digital health and research and of those with more time availability. Therefore, future evaluation projects in a non-pandemic situation would be suggested.
Conclusions
In conclusion, our study showed that Support is highly appreciated by PWT1D. This online education and support web app has the potential to decrease the self-reported frequency and fear of hypoglycemia and increase self-efficacy in DSM among adults living with diabetes. Such a web app could be used as an adjuvant tool to DSME/S in clinical settings. Future steps include adjusting the web app based on the suggestions provided by the participants and investigating its clinical implementation and effectiveness for scalability.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231204435 - Supplemental material for Evaluation of Support, a self-guided online type 1 diabetes self-management education and support web application—a mixed methods study
Supplemental material, sj-docx-1-dhj-10.1177_20552076231204435 for Evaluation of Support, a self-guided online type 1 diabetes self-management education and support web application—a mixed methods study by Li Feng Xie, Asmaa Housni, Amélie Roy-Fleming, Aude Bandini, Treena Delormier, Deborah Da Costa and Anne-Sophie Brazeau in DIGITAL HEALTH
Footnotes
Acknowledgements
Authors would like to acknowledge the contribution of Haeli Anderson, Chantal Blais, Sarah Blunden, Inès Boukabous, André Carpentier, Steve Chalifoux, Abigail Collings, Kaberi Dasgupta, Katherine Desjardins, Michel Dostie, Andréanne Fortin, Sarah Haag, Mélanie Henderson, Claudia Gagnon, Annie Gaumond, Catherine Goulet-Delorme, Patricia Kearns, Maude Lafontaine Hébert, Laurence Laplante, Catherine Leroux, Laurent Legault, Fati Merah, Virginie Messier, Meranda Nakhla, Pamela Nakouzi, NaraCreative, Silvia Netedu, Jacques Pelletier, Bruce Perkins, Melinda Prévost, Rémi Rabasa-Lhoret, Marie Raffray, Monia Rekik, Maha Saadé, Stéphane Tardif, Cynthia Turcotte, and Michael Wright.
Contributorship
All authors read and accepted the manuscript. Li Feng Xie designed the study, interviewed the participants, recruitment, data collection, performed the statistical analysis, performed the qualitative coding, drafted, reviewed, and corrected the manuscript. Asmaa Housni was involved in the coding process, translated the quotes, participated in the draft and revision of the manuscript. Amélie Roy-Fleming coordinated the development of Support, study recruitment, intervention and data collection, helped in the data analysis and interpretation, and reviewed the manuscript. Aude Bandini has lived experience with type 1 diabetes. She participated in the study design, development of Support, data interpretation, and reviewed the manuscript. Treena Delormier participated in the study design, data analysis, and interpretation, and reviewed the manuscript. Deborah Da Costa participated in the study design, data analysis and interpretation, and reviewed the manuscript. Anne-Sophie Brazeau is the principal investigator of the project. She co-designed the study, guided the development of the Support web app, participated in data analysis and interpretation, and reviewed the manuscript. The guarantor of this manuscript is Dr Anne-Sophie Brazeau.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Montreal Clinical Research Institute's Research Ethics Committee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LFX holds a PhD scholarship from the Fonds de Recherche Santé Québec. ASB is a Fonds de Recherche du Québec en Santé's research scholar. This study is funded by the Canadian Institutes of Health Research and the Juvenile Diabetes Research Foundation.
Informed consent
All the participants provided online informed consent. The results are reported based on the Mobile Health Evidence Reporting and Assessment Checklist.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.