
Abstract
Background
Diabetes self-management education and support (DSME/S) are central in type 1 diabetes (T1D) where individuals are responsible for 95% of care. In-person DSME/S programs have been proven clinically effective (e.g. optimizing glycemic management, improving diabetes-related behaviors) but are limited by a lack of accessibility and long-term follow-up. Self-guided digital tools such as web applications (web apps) can be an alternative for delivering DSME/S.
Objective
This article describes the development of Support, a behavioral theory-based, self-guided, web application for adults living with T1D in the province of Quebec, Canada.
Methods
A multi-disciplinary team developed Support. Patient partners first proposed its focus, learning topics, and expressed barriers to using digital tools for DSME/S. These barriers were analyzed based on the Behaviour Change Wheel. A group of healthcare professionals (HCPs) drafted the evidence-based learning content which was reviewed by external HCPs and by patient partners.
Results
Support is a bilingual (English and French) web app accessible at any time via the Internet. It has four learning paths focusing on hypoglycemia and based on the user's method of diabetes treatment. Learning modules are divided into six categories with a maximum of three learning levels. It contains features such as a discussion forum, videos, and quizzes to ensure interactivity, provide social support, and maintain the motivation and long-term engagement of users.
Conclusions
To the best of the authors’ knowledge, Support is the first self-guided evidence-based web app for adults living with T1D. It is currently under study to evaluate its feasibility and clinical impacts.
Introduction
Type 1 diabetes (T1D) is a chronic autoimmune health condition characterized by an insulin deficiency due to the destruction of beta-cells in the islets of Langerhans, leading to hyperglycemia. 1 Based on a modelling study published in 2022, from the sum of mid-year prevalence estimates, for people born in 1922 up to 2021, in Canada, the prevalence of people living with T1D (PWT1D) was 276,284 in 2021. 2 Daily insulin administration and blood glucose monitoring are required starting at diagnosis. A sub-optimal blood glucose management can lead to short-term (e.g. hypoglycemia and coma) and long-term (e.g. retinopathy and stroke) health complications, 3 and a reduced life expectancy. 4 Diabetes self-management (DSM) is complex and further challenged by life stage changes, daily factors (e.g. stress, medication, food intake, social stigma), and the development of diabetes-related complications and comorbidities. 5
Diabetes self-management education and support (DSME/S) are central for PWT1D who are responsible for 95% of their own care. 6 DSME/S programs contain people-centered learning components (e.g. case management) aiming for behavioral changes and are traditionally delivered in group settings.7, 8 Positive outcomes include lowering of hemoglobin A1c, a key indicator of blood glucose management.9–11 For instance, the Programme for diabetes education and treatment for a self-determined living with type 1 diabetes (PRIMAS) contains 12 lessons (twice a week for 6 weeks) of 90 min each with materials (e.g. worksheet for carbohydrate estimation) to be completed between lessons. 9 It aims to help PWT1D adjust their insulin dosage, detect, and treat acute complications such as hypoglycemia. The Dose Adjustment for Normal Eating (DAFNE) is another program and is delivered over five consecutive days or one day per week for five weeks. 12 DAFNE aims to teach PWT1D skills for adjusting insulin to increase their dietary freedom and has been extensively supported by research evidence with positive clinical outcomes.10, 12, 13 However, despite the positive impact of these in-person DSME/S programs, their fixed schedule, required on-site presence of care receivers and health care providers, and group delivery format can decrease their accessibility, increase delivery cost, and limit personalization of the learning content.7, 14 In addition, the lack of sustained follow-up can be an obstacle for PWT1D to maintain long-term behavioral changes. 15
Digital tools, such as mobile applications (apps) and responsive websites (web apps), are feasible and accessible alternatives for delivering DSME/S. The idea of using digital tools for DSME/S emerged around 2013 and was accelerated by the coronavirus pandemic where in-person consultations were limited. 16 The number of mobile apps related to DSM increased rapidly in recent years. However, there is still a lack of evidence regarding their clinical effectiveness17–20 and their use over time. 16 For example, in a meta-analysis published by Wu et al. in 2019 there is inconclusive evidence on the efficacy of mobile apps for lifestyle modification in T1D. 21 Similarly, in the Mobile Applications for Self-Management of Diabetes report published by the Agency for Healthcare Research and Quality in 2018, hundreds of commercial mobile apps for DSM were identified but only 11 apps were evaluated for impact on health outcomes, and 5 (2 in T1D and 3 in type 2 diabetes) showed a clinically significant reduction of hemoglobin A1c of 0.5%. 22 Furthermore, compared to web apps, mobile apps require more resources for development and maintenance due to the multiple and rapidly evolving operating systems. 23 Therefore, it could be beneficial, both clinically and financially, to have a self-guided (i.e. absence of live and individual contact between the user and healthcare professionals [HCPs]) web app for DSME/S that is based on behavior change theories and scientific evidence. 24 For instance, the Behaviour Change Wheel (BCW) is a framework based on 19 behavior change theories, it proposes a 3-layer behavior system with the capability, opportunity, and motivation (COM-B) model at its core, followed by nine interventions, and seven policies. 25 This model has previously been identified as a key factor for digital health tools in diabetes to facilitate behavior changes and increase adherence to the intervention. 26 Therefore, considering these gaps, our research team developed Support, a DSME/S self-guided web app guided by the BCW for adults living with T1D. This article describes its development process.
Methods
The Support web app was designed by a multi-disciplinary team, based on a people-oriented participatory approach, and the BCW to meet the needs of its intended users (adults with T1D living in Quebec, Canada). Description of its development is reported based on Template for Intervention Description and Replication checklist 27 (Supplemental material I).
People-oriented development process
Patient partners, a multi-disciplinary team of HCPs, an e-health intervention specialist, and external information technology and design agencies were involved in the development of Support.
In 2017, an initial group of patient partners was recruited through T1D clinics and networking to discuss their needs and research priorities, and to draft the outline of a research proposal to submit for funding. Our patient partners were formed by a mixed group of Anglophones and Francophones from various age ranges. The number of patient partners varied during the development of Support from 9 to 11 with a similar number of men and women. During an initial in-person meeting with researchers and HCPs, they expressed their interest to have access to more educational resources, mainly related to the use of new medical technologies (e.g. insulin pumps). They also felt that access to education and training varied across regions and therefore alternative means of delivering DSME/S should be explored. The patient partners have been involved in every step of the web app development (e.g. brainstorming of the digital tool design, content creation, tool testing). In 2019, two in-person meetings were organized as well as phone/videoconference discussions with patient partners and researchers every six weeks to gather their impressions and suggestions throughout the process. E-mail communication was used for content revision in between the meetings. Patient partners each decided their degree of involvement which could vary throughout time. Financial compensation was given for their involvement, as recommended by the Canadian Institutes of Health Research. 28
Content creation
Content refers to the learning information within Support. The focus of the content was first identified after a brainstorming session between the researchers, HCPs, and patient partners. A list of topics to be included was then drafted and categorized based on patient partners’ suggestions. The initial list of content topics was completed following a review of clinical guidelines for diabetes29–31 and an assessment of educational programs.32–34 It was circulated for external review by seven dietitians, three nurses, and one endocrinologist. Additional topics were added based on their suggestions.
Clinical literature review and writing of educational content were performed by T1D specialists including two dietitians/certified diabetes educators, one kinesiologist, one psychologist, and one nurse and overviewed by one dietitian and one endocrinologist To develop the learning content, the team used guidelines published by the diabetes organizations,29–31 provincial diabetes association website (e.g. Diabète Québec), reference books,35, 36 consensus guidelines,37–39 health centers’ publications,32, 33 and user manuals (e.g. for insulin pumps). When scientific evidence was not available (e.g. what to do in case of insulin dose errors, dose of insulin needed for alcoholic beverages containing carbohydrates), a discussion between the core team took place until consensus was obtained. The content was reviewed by patient partners and a team of external HCPs specialized in T1D including two dietitians, two nurses, three endocrinologists, and one psychiatrist.
The words’ choice was inspired by The Use of Language in Diabetes Care and Education to ensure a neutral, nonjudgmental message transfer. Content underwent a linguistic revision and was professionally translated from French to English.
Web app format development
Format refers to the skeleton of the web app, including the visual design, method of presenting the content, and features. In this context, a feature is defined as functionality that facilitates the user's learning and navigating experiences such as the discussion forum and videos. 24
The initial web app format emerged from discussions with patient partners, HCPs, and researchers. It was suggested that the app regroup an education component, including at least videos, textes, a discussion forum to facilitate peer support, and a blog section for scientific news. The team requested a visual design adapted to an adult population, showing cultural diversity, having an appealing color scheme, and being coherent to facilitate the learning process. The web agency also suggested relevant features based on their expertise. In parallel, a literature review on features used in digital interventions for chronic health conditions was conducted. 24 Given the early developmental phase of this web app and to ensure a long-term engagement in the intervention, a brainstorming session with patient partners was conducted to understand the barriers related to the use of self-guided digital tools for DSME/S compared to in-person sessions. The identified list of barriers was returned to patient partners by e-mail and they were invited to return their comments after the meeting throughout the development process. The web agency, patient partners, and researchers discussed methods and behavioral change techniques (BCTs) version 1 using the BCTs taxonomy 40 that can be used to reduce these barriers based on the COM-B model and associated with interventions from the BCW, 25 to be finally translated to various features. Before the web app development, the feature list was reviewed again by the patient partners to confirm that these features were related to barriers previously identified.
Confidentiality and data safety
For confidentiality and navigation safety, the web app was built on WordPress.ca and hosted on a Canadian server (HostPapa.ca). Usage data is tracked through Google Analytics with an anonymous identifier attributed to every user.
Results
This project resulted in the development of the Support bilingual (English and French) web app. 41 The initial brainstorming session was held in September 2017, research funding was awarded in March 2018 and the web app was launched in January 2020 as part of a proof-of-concept study.
Content
The educational content is divided into six main categories (medication, blood glucose monitoring, diet, physical activity, hypo- and hyperglycemia, health and other situations). Each category is subdivided into courses, each taking 5 to 20 min to complete (length labelled on each course). Topics are divided into a maximum of three levels: basic, intermediate, and advanced. The basic level introduces participants to some key concepts of DSM (e.g. understanding insulin action, understanding continuous glucose monitors, and identifying foods with carbohydrates). The intermediate level is an extension of the previous level and involves specific situations (e.g. counting carbohydrates and downloading continuous glucose monitors). The advanced level requires more mathematical calculation (e.g. how to calculate an insulin-carb ratio, how to adjust insulin) or deeper analysis (e.g. understanding the ambulatory glucose profile). Content is updated or new material is added according to the publication of new clinical guidelines, expert consensus, or access to new medical therapies and technologies for T1D.
To personalize the learning experience, four learning paths were developed based on the individual's diabetes treatment and each path has its specific learning content: (1) multiple daily insulin injections (MDI) with capillary blood glucose (CBG) monitoring; (2) MDI with continuous glucose monitoring (CGM); (3) continuous subcutaneous insulin infusion (CSII) with CBG monitoring; (4) CSII with CGM.
Users are prompted to do a mandatory course on hypoglycemia at their first log-in to the app. This initial focus on hypoglycemia is related to the important daily burden and was voiced by patient partners as a limiting factor for health behavior change. After completing this basic mandatory course on hypoglycemia, users have access to the basic level of all categories. If multiple levels are available within a topic, completing the basic course is required to unlock the course of the following level. A summary of courses offered in learning path four is provided in Supplemental material I.
Web app format
The web app was built using a desktop-first responsive design. The web agency proposed a cartooned visual design with six pastel colors (blue, green, orange, red, pink, and purple), one for each learning category. Human characters with different ethnic backgrounds were incorporated. A visual presentation of the home page is available in Figure 1.

Screenshot of the support web app (home page).
Throughout the content development, the team varied the format of educational material and used features such as quizzes, videos, downloadable PDF documents, news blogs, case studies, and glossary definitions to enhance user experience and overcome the potential barriers of using self-guided digital tools for DSME/S compared to in-person sessions. These features also aim to facilitate comprehension, adapt to different learning types, and increase interactivity between users and the digital tool. In addition, a list of potential barriers was established by researchers and patient partners and was categorized based on the COM-B model (Figure 2). Each of the barriers was associated with interventions from the BCW, 25 to BCTs, and then translated into characteristics or features included in the web app.

Barriers to use self-guided digital tools for DSME/S compared to in-person sessions: analysis and categorization from the COM-B model to web app building.
Users were able to choose their focus DSM behavior (e.g. carry glucagon, carbohydrate counting, and increase the frequency of physical activity) while navigating on Support. BCTs were incorporated within Support to facilitate the practice and integration of DSM behaviors. Inspired by the previous literature, 42 BCTs were integrated to increase the enablers (e.g. “feeling empowered by new knowledge and skills”) and decrease the barriers of DSM (e.g. “discomfort in managing diabetes in public”), mainly through problem solving, information about health consequences, demonstration of the behavior, instruction on how to perform the behavior, identification of self as a role model, and social support. For instance, videos included the demonstration of glucagon injection performed by a nurse to facilitate the use of glucagon and an explanation of its use from PWT1D to their family members. The health consequences of not carrying a glucagon with self are also given in the same video. In the social discussion forum, users can exchange with their peers regarding the DSM topic of their choice, and act as role models. It allows for social comparison.
Based on these methods of selection, a total of 17 main features were included in Support. They are described below.
Personal username and password
At the moment of this article publication, only people invited to the Support research study were allowed to create an account. To ensure user's confidentiality, users log-in with their e-mail address and personal password. They can choose their pseudonym showed in the discussion forum and change it at any time.
Welcome e-mail
Once the user creates a Support account, a welcome e-mail is sent with the template below (Textbox 1):
Textbox 1 Welcome e-mail send to users

Introductory session
When users first log-in to the Support web app, they are directed to an introductory slideshow (6 slides, takes 2 min to view) explaining how to use the app. After viewing these slides for the first time, users are directed to the mandatory course on hypoglycemia. They can come back to these slides at any time under “Guided tour” displayed on top of the home page.
Avatar/profile picture
Users can choose their own avatars from an avatar database. The more the user completes courses, the more avatars are unblocked.
Personal dashboard
The user's personal dashboard displays a summary of their recent activities (e.g. the last date of connection, goals, completed courses, number of trophies and certificates) and the latest updates on the app (e.g. post on the discussion forum and news blogs).
Goal setting
A textbox is available in the user's personal dashboard for them to set personal goals. They are introduced to set a specific, measurable, attainable, relevant, and time-bound goal 43 in the physical activity learning category.
Videos
Videos are embedded within courses and available in the media library once users have finished the course. Three types of videos can be found: narrated animations (Figure 3), technical manipulations (e.g. insulin injection technique) by HCPs, and PWT1D testimonials. Narrated animations repeat the main written information and aim to increase the accessibility for people with a lower literacy level and for those who prefer watching over reading. Technical manipulations and testimonials were filmed to facilitate self-identification. The content coordinator prepared the video scripts for the first two video types and led the testimonial interviews. Narrated animations and technical manipulations are available in English and French. The testimonials are in the individual's preferred language, and subtitles in the other language were added (e.g. if the video was in English, a subtitle in French would be added).

Example of a narrated animation video.
Quizzes
At the end of each course, users are prompted to answer two to three multiple choices or True/False questions to validate their understanding. Correct answers are given once the quiz is submitted. Virtual points are attributed to completed quizzes, regardless of the answers given. These questions aimed to help users integrate the learned knowledge and increase interactivity with the app.
Downloadable PDF documents
Downloadable PDF documents are available to summarize information and facilitate future reference. They are at the end of each course and can be found in the media library once the related course is completed.
Glossary definitions
Medical jargon and technical words are underlined in their first appearance in each course. When the user places their cursor on the word, a definition bubble appears. These definitions can also be found in the “Glossary” section at all times.
Calculators
A series of automated calculators are available in courses when relevant, and at all times in the media library. They aim to simplify calculations such as calculating the number of carbohydrates in food using a carbohydrate factor, assessing the accuracy of a CBG meter when compared to a laboratory value, and establishing a sensitivity factor.
Case studies with different PWT1D profiles
To facilitate the integration of knowledge and self-identification, six fictional characters with different profiles (e.g. age, gender, ethnicity, diabetes treatment) were created (Figure 4). They are found as case studies throughout the courses and provide practical application of DSME/S.
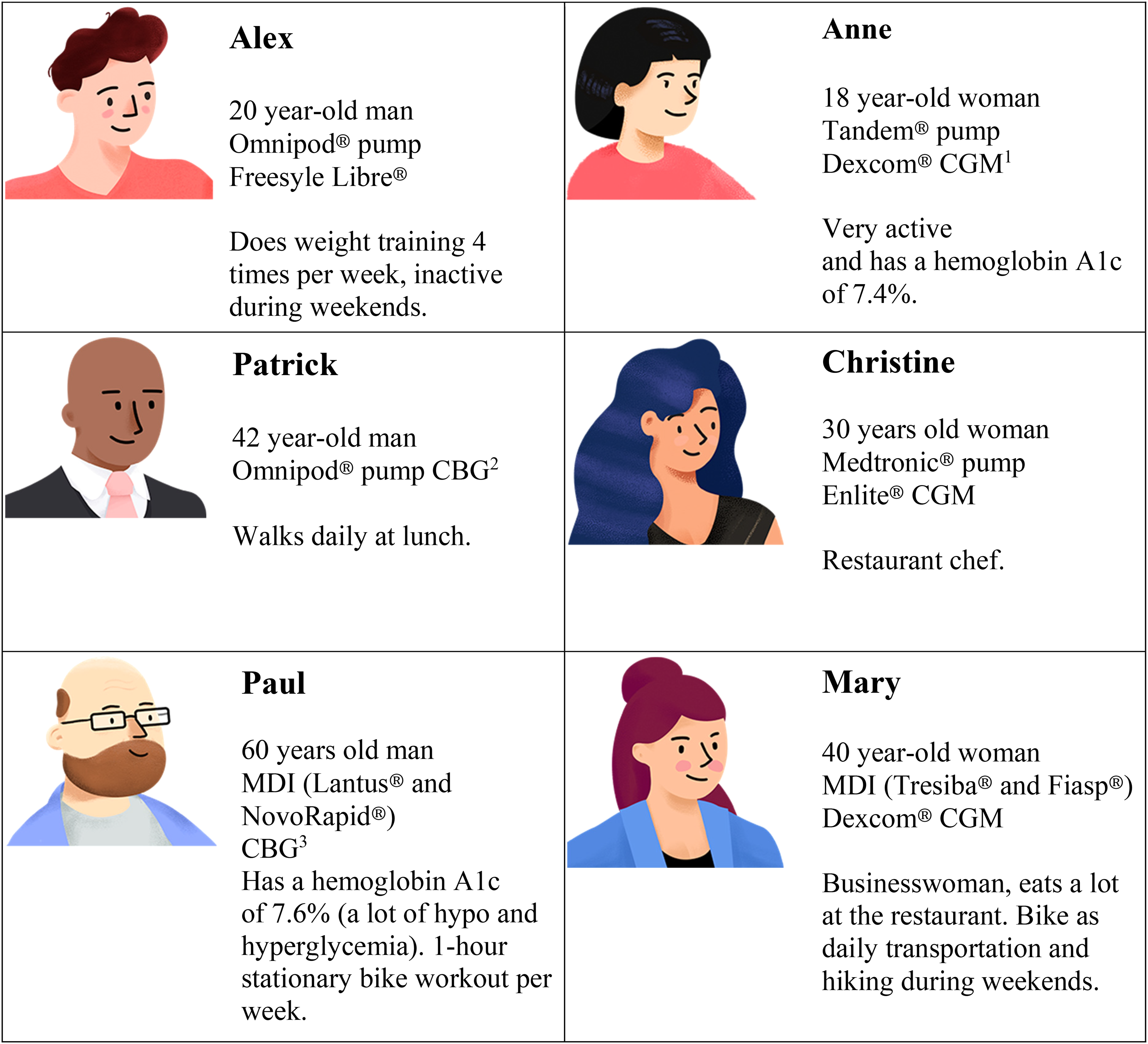
Case study characters.
Virtual rewards and trophies
Users receive virtual points for different aspects of their use of the web app (e.g. completing a quiz, completing a course, participating in the discussion forum) and virtual trophies are unblocked at the accumulation of virtual points.
Certificates
A completion certificate is available in the user's dashboard after completing mandatory courses in each category. Mandatory courses are defined as information applicable to most PWT1D and need to be completed to advance to a further level. Optional courses are related to specific needs (e.g. driving with diabetes). A final certificate is also given when completing all the mandatory courses in Support.
Discussion forum
Users from the four learning paths in the English and the French version of Support share the same discussion forum and can post in the language of their choice. Posts on the discussion forum are classified as the following: in addition to the six main learning categories, there are sections for weekly news blogs, general discussion, frequently asked questions, and technical support. The Support coordinator (who is a bilingual registered dietitian and certified diabetes educator) is in charge of moderating the forum daily. Patient partners are invited to post on the forum to encourage a flow of conversation and the research team also created four user accounts to promote discussions. All the users can participate in the online forum (make a new post, respond or “like” other posts). At all times, the moderator can modify or delete a post (e.g. if it contains confidential information).
News blog
The Support coordinator posts bilingual news blogs once to twice weekly. The topic of the news blogs is based on current events (e.g. how winter cold affects blood sugar), recent scientific publications (e.g. Diabetes Canada's position on ketogenic diets), updates from the research team (e.g. upcoming webinar), and T1D topics that are not currently covered in any courses (e.g. hormonal therapy and T1D). Users from the four learning paths have access to the same news blogs.
E-mail newsletters
Biweekly newsletters are sent to users by e-mail. They contain a preview of the latest news blogs with a link to read more and two suggested basic courses (common to the four learning paths). These newsletters are also used as reminders for users to log-in on Support.
Other
Once the user ends a learning course, related courses are proposed at the end of the page. Users can also find the contact information (including for technical support) and condition of use page at the bottom of every page of the Support web app.
Discussion
To reduce the risk of developing diabetes-related complications, PWT1D need to adequately manage their blood glucose which is affected by multiple factors (e.g. nutrition, physical activity, insulin adjustments, stress). Regrouping these aspects in a cohesive manner within one digital tool can facilitate DSME/S. 42 This article describes the Support web app development process for adults living with T1D. It was created by a multi-disciplinary team using a people-oriented approach. Unlike existing in-person DSME/S programs for PWT1D, the Support web app is self-guided, combines up-to-date evidence-based information (Supplemental material II), enables interactive learning based on the BCW with learning paths specific to the user's treatment modalities, includes opportunities for peer support, and is accessible at any time on any device with an Internet connection.
The educational content offered through Support and its accessibility has the potential to bridge the gap between current DSME/S programs and the needs of PWT1D. Indeed, despite the presence of multiple DSME/S programs, a number of them only focus on specific aspects (e.g. physical activity 44 or nutrition 45 ) or cover multiple aspects only in a basic manner.9, 10, 46 For instance, HypoAware is a group-based diabetes education program that combines in-person and online components on hypoglycemia management. Although it has a broad spectrum of learning curriculum (recognition of hypoglycemia symptoms, nutrition, medication, physical activity, and stress management), it lacks real-life applicability and is offered in the same way to individuals living with type 1 and insulin-treated type 2 diabetes. 46 Despite commonalities in the hypoglycemia symptoms and health complications, these two populations encounter different daily challenges and should receive tailored information respective to their health condition. 47 Different from HypoAware, PRIMAS and DAFNE are two programs designed specifically for PWT1D. They elaborated on many topics of DSM (e.g. the impact of diabetes on partnership, on quality of life) 9 but the information is only offered at a specific moment (e.g. at diagnosis). When people transit from the program to everyday life, they tend to encounter new barriers and decrease the recall of information, which can increase difficulty in applying DSM behaviors.48, 49 Support is different from these in-person programs in the way that it is exclusively online and self-guided, thus accessible over time and at the user's own pace. The ease of access to Support makes it a potentially effective method of providing ongoing DSME/S with continuous up-to-date learning content and the opportunity to exchange their concerns at all times with peers via the discussion forum.
Indeed, social interaction is one of the most apparent differences between an in-person and a self-guided digital program. The in-person group programs have the advantages of providing timely dialogue between people and direct support from HCPs. This human interaction has been reported by studies as a potential factor to increase engagement and acceptability of the intervention, 24 and to improve people's motivation in DSM. 50 However, it can further increase the program's cost 24 To compensate for this lack of social support and human contact inherent to the digital world, interactive features, such as a discussion forum and quizzes, have been added to Support, since these have shown to be effective methods of providing feedback and social communication. 51 As demonstrated by previous literature, 48 virtual points, trophies, and certificates were also included to increase motivation and confidence in DSM. In addition, compared to in-person programs, digital tools might also increase the engagement of people who have confidentiality or stigma concerns as users can choose to stay anonymous during their learning process. 49
The inclusion of different stakeholders is one of the main strengths of the development process of Support. Patient partners were involved in each step and contributed their perspectives. Including the end-users within the development process generates valuable ideas and helps to produce an intervention that is practical rather than only theoretical.42, 50 The identification of a target focus (i.e. hypoglycemia) based on their reality can also increase the long-term engagement of end-users with the digital tool. 50 Participation of HCPs from different areas ensured that the learning content was evidence-based and clinically relevant. Outsourcing information technology teams optimized the design quality of the digital tool.
The development of Support was further strengthened with the use of the COM-B model, BCW, and BCTs. They served as frameworks for intervention development by facilitating the understanding of target behaviors (e.g. use of the digital tool) and providing an explanation for why a BCT can be effective or ineffective. 20 In addition to promoting an increased engagement to the web app, our BCTs can also potentially foster the sustainment of DSM behaviors. Hamilton et al. 42 used the COM-B model and BCW to investigate barriers and enablers to sustained self-management among PWT1D based on the DAFNE program and found barriers such as “difficulty incorporating DAFNE principles [learning content] into everyday life and challenges,” “feelings of failure and hopelessness,” and “didactic culture of healthcare inhibiting independent decision.” These barriers could be reduced by incorporating the BCTs such as “demonstration of the behavior” (e.g. case studies), “social support” (e.g. discussion forum), and “problem solving” (e.g. able to solve their DSM problems by independently learnt information) which can all be found on Support. Hamilton et al. 42 also reported on enablers namely “having clear targets and guidelines” and “feeling empowered by new knowledge and skills.” Support incorporates these enablers with its learning content available under diverse format (e.g. videos, PDF documents, quizzes) translated from BCTs such as “credible source,” “information about health and social consequences,” and “demonstration of the behavior.”
Furthermore, when the same in-person program is given by multiple facilitators, any update of the literature implies extra hours of training and increases the possibility of inconsistent content delivery. Providing the learning content through digital tools facilitates content update and ensures consistency in its delivery. 52
To the best of the authors’ knowledge, Support is the first self-guided web app for DSME/S in PWT1D. Because of the proof-of-concept phase of its development, the research team had to prioritize the selection of features and some potential features impacting on DSM behaviors were not integrated. For instance, a feature enabling self-monitoring might increase positive clinical impact and self-awareness, 24 but it is excluded in the current version due to the development cost and goal setting was used as a proxy. E-mail and text message reminders were integrated into Support and were then replaced with a newsletter due to technical difficulties. Our patient partners also proposed the idea of expanding this tool to family and friends of PWT1D through shareable links on social media channels or subscriptions to newsletters. As Support is currently only accessible through a research study targeting PWT1D themselves, this feature was not integrated. However, the format of web apps provides the developers with the possibility of making modifications and easy updates. 23 Despite the current lack of certain features and content, the research team can make adaptations continuously depending on the needs of the population. Another improvement that can be made would be the composition of our patient partners group, as they were composed of Whites in the majority, efforts to include people from other ethnic groups would be needed in the future. Given the early developmental phase of our web app, only barriers to the use of digital health tools were explored with potential users and content was developed based mainly on the current literature after discussion with our multi-disciplinary team. In the future, content can be further elaborated from user feedback, identify areas of DSM behavior changes that should be prioritized and refined based on the BCW and BCTs.
Conclusion
In conclusion, this article describes the development of the self-guided web app Support for DSME/S in PWT1D. This web app was developed by a multi-disciplinary team with patient partners and is based on the BCW. Support provides evidence-based and periodically updated content with a variety of features to facilitate DSM. It is now under research study to evaluate its clinical impacts, usability, and feasibility among PWT1D in the province of Quebec, Canada. These results will guide the improvement of this web app and suggest methods for integrating it as part of routine diabetes care.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231152760 - Supplemental material for Development of the Support self-guided, web application for adults living with type 1 diabetes in Canada by a multi-disciplinary team using a people-oriented approach based on the Behaviour Change Wheel
Supplemental material, sj-docx-1-dhj-10.1177_20552076231152760 for Development of the Support self-guided, web application for adults living with type 1 diabetes in Canada by a multi-disciplinary team using a people-oriented approach based on the Behaviour Change Wheel by Li Feng Xie, Amélie Roy-Fleming, Sarah Haag, Deborah Da Costa and Anne-Sophie Brazeau in Digital Health
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of Aude Bandini, Chantal Blais, Sarah Blunden, Inès Boukabous, André Carpentier, Steve Chalifoux, Kaberi Dasgupta, Treena Delormier, Katherine Desjardins, Michel Dostie, Andréanne Fortin, Mélanie Henderson, Claudia Gagnon, Annie Gaumond, Catherine Goulet-Delorme, Patricia Kearns, Maude Lafontaine Hébert, Laurence Laplante, Laurent Legault, Fati Merah, Virginie Messier, Meranda Nakhla, Pamela Nakouzi, NaraCreative, Silvia Netedu, Jacques Pelletier, Bruce Perkins, Melinda Prévost, Rémi Rabasa-Lhoret, Marie Raffray, Monia Rekik, Maha Saadé, Stéphane Tardif, Cynthia Turcotte, and Michael Wright.
Contributorship
Li Feng Xie co-designed the web app, drafted the manuscript, and revised the final version. Amélie Roy-Fleming co-designed the web app, coordinated the development of the web app and its content and revised the manuscript. Sarah Haag participated in the development of the content and revised the manuscript. Deborah Da Costa advised the development of the web app and revised the manuscript. Anne-Sophie Brazeau co-designed the web app and developed this project. She contributed to the manuscript preparation and revision.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
As this is the development of a web app, ethical approval does not apply.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the Canadian Institutes of Health Research and the Juvenile Diabetes Research Foundation. Li Feng Xie received a PhD scholarship from Fonds de recherche du Québec. ASB is a Fonds de recherche du Québec en santé's research scholar (junior 1).
Guarantor
ASB
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.