
Abstract
Background and Objective
To preserve cardiovascular health in persons with spinal cord injury (SCI), it is important to promote physical activity programs adapted to them. Home-based exercise programs allow patients to perform clinician-prescribed physical activity without going to a hospital. However, they make it difficult for the clinician to guide and monitor the patient. To face this issue, this paper proposes a novel smartphone-based mobile application (Fisiofriend), and evaluates its feasibility with a pilot study in a real clinical intervention.
Methods
Fourteen SCI male subjects were involved in a 6-weeks home-based intervention, based on upper limbs exercises: 7 subjects (APP group) used Fisiofriend, and 7 subjects used traditional pictorial instructions on paper (PAPER group). At the beginning (t1) and end (t2) of the study period, we measured: (i) biceps and triceps brachii strength and endurance parameters with an isokinetic dynamometer (Biodex System 4), (ii) O2 maximal consumption with a crank ergometer stress test (VO2000, Medgraphics). Moreover, we collected subjective data about subjects’ perception of the support (app or paper) in the home-based program.
Results
Physiological results were encouraging for both groups. Questionnaire data suggests a possible advantage of the app in terms of pleasantness, engagement and perception of positive effects. Practical clinical experience with the subjects and their informal reports highlighted which features of the app could be of particular benefit in real interventions, as we discuss in the paper.
Conclusions
The study showed the feasibility of using a mobile app in home-based exercise programs involving SCI patients. We discuss implications of introducing such kind of apps into clinical practice.
Keywords
Introduction
Ageing entails a progressive reduction of physical performance, with increased risk of re-hospitalization and reduced quality of life. While this general issue affects every individual, it becomes more serious with spinal cord injured (SCI) persons, because of their much greater risk of cardiovascular disease and comorbidity. Physical inactivity and marked deconditioning are highly prevalent among SCI patients. Moreover, ordinary everyday activities that SCI patients perform appear to be inadequate to maintain cardiovascular fitness. Several studies have shown that physical inactivity is a major independent risk factor for cardiovascular diseases (CVD) and premature mortality,1,2 and regular physical activity can reduce the onset and/or prevalence of various chronic diseases (including CVD, type II diabetes, and osteoporosis) in SCI patients, 3 maintaining good quality of life. It is thus important to promote long-term physical activity interventions adapted to the SCI population and tailored to characteristics and needs of each patient. Such programs should accompany SCI persons throughout life aiming at maintenance of muscular strength and cardiovascular performance. The literature provides evidence of the positive effects of exercise programs in SCI patients:4–6 long-term home-based programs based on continuous training ensure an increase in oxygen consumption, and an improvement in strength and endurance parameters, while programs based on interval training improve respiratory capacity. Undergoing any of the two treatments also improves quality of life.4–6
Unfortunately, compliance with home-based exercise programs tends to be lacking, patients may not comprehend the exercises correctly or they may not perform them at all, and it is impossible for clinicians to guide and monitor the patient at home. Indeed, the percentage of patients who perform the exercises correctly at home is estimated 7 to be only between 34% and 62%. Patient's compliance with the exercise plan depends on several factors, including the clinical characteristics of the patient, the specific exercises and the relationship between clinician and patient. The most important patient's factors are motivation, lifestyle, and pathology, while the most important program factors are type of exercises, clarity of instructions and effectiveness of exercises.7–9 For all the reasons above, it is essential to find strategies to support long-term, home-based exercise treatment. This paper proposes a novel smartphone-based mobile application (Fisiofriend), and evaluates its feasibility with a pilot study in a real clinical intervention. Potential advantages of using a mobile app include the possibility of better instructing patients about the exercises, providing real-time feedback during the execution of the exercise based on data collected by the smartphone accelerometer, and providing the clinician with reports about program compliance.
Materials and methods
The Fisiofriend application
Fisiofriend is a mobile application we created (in Java for Android smartphones) to support SCI persons in home-based exercise programs. The app requirements have been elicited through meetings of a multidisciplinary team, composed by two computer scientists, two medical doctors, and three physiotherapists. Both the doctors and the physiotherapists work with SCI patients in their daily clinical activity. The app provides patients with three main functions. First, it illustrates instructions for each exercise in the program, with text, pictures and video (Figure 1).

Fisiofriend illustrates exercises with pictures, text, and video.
Second, all exercises that include movement on the frontal or sagittalis plane can additionally provide real-time monitoring and feedback based on accelerometer data: if the user moves the upper limb outside the correct range, the app produces a warning sound. To monitor movement, users wear the smartphone on their wrist using a band (Figure 2).

In the intervention, users wore the smartphone with a band.
Third, the app includes some game-like features as a motivating feature: users receive points for carrying out exercises, and medals for “perseverance in the program”. Points and medals are given separately for each exercise, remain stored in the phone, and users can visualize them whenever they like (Figure 3).

The app gives points for carrying out exercises, and rewards progress in the program by assigning “perseverance medals” (bronze, silver, gold, platinum). The screen on the left shows points and medals received for an exercise. The screen in the center shows how many times and when an exercise was performed. The screen on the right shows a summary of all performed exercises and the medals received.
Two additional functions are reserved to clinicians. They can tailor parameters of the exercise program to the clinical profile of the patient, setting loads to be used in exercises, number of exercise repetitions, recovery time, number of exercise sessions per week (Figure 4). Moreover, clinicians receive a periodic report about user's activity: the file contains exercise plan, number of sessions performed by the user, start and end time of each exercise, load in kilograms or resistance of elastic band used, number of exercises completed.

Clinicians can define the patient profile and select exercises (a). For each exercise, they can adapt parameters to the patient's needs (b).
Subjects
From a patient acceptability point of view, we did not expect specific issues in recruitment or in intervention, because one of the groups was going to follow the standard approach to home-based exercise programs, which is known to be well accepted by patients in the field of rehabilitation. Moreover, in the other group, the addition of the mobile app to the same exercise program was specifically meant to support patients in more easily performing the home-based program to further improve acceptability and compliance.
Our pilot study involved 14 male SCI patients, discharged by the Spinal Unit of the Institute of Physical Medicine and Rehabilitation “Gervasutta”. Study inclusion criteria were: spinal cord injury in chronic phase (at least 1 year after lesion), lesion at the cervical or thoracic level with a motor score for the biceps and triceps brachii of at least 3/5, no involvement in competitive sports after lesion. In terms of physical activity, the lifestyle of all subjects was similar: they were not performing it regularly, and they all used a wheelchair for locomotion. They were all classified as low active at baseline. Participants in the group who were going to use the app had to own an Android smartphone, to be able to run the app.
All subjects were assigned to the same exercise program, which was appropriate for their conditions: 7 of them (APP group, mean age 43.43 ± 10.11, BMI 24.23 ± 4.77) used Fisiofriend, while the other 7 (PAPER group, mean age 50.14 ± 17.99 years, BMI 24.05 ± 3.60) used traditional pictorial paper instructions. Figure 5 shows how the paper instructions presented the exercises. All subjects signed an informed consent form to participate in the study.

Presentation of an exercise in the paper instructions. The empty tables were meant for manual recording of date of exercise, number of repetitions, used weights. Such data was automatically recorded in the app.
To prevent the risk of confounding variables due to possibly unbalanced groups, which might arise in randomization with small samples, we followed a nonrandom assignment aimed at minimizing differences on individual characteristics that could become confounds if significantly different between the two groups. In particular, we focused on completeness/incompleteness of the spinal cord injury and lesion level (cervical and thoracic). Lack of control over these variables can lead to critically biased results. For example, if participants’ cervical lesion level had been different between groups, the quality of physical performance would have been inevitably biased in favor of one of the two groups.
Methods
The 6-weeks home-based exercise program in the pilot study consisted of strengthening (38 different exercises, performed with 1–2 Kg overloads and elastic bands) and stretching (8 different exercises), addressed to the upper limbs. The strengthening exercises involved the major muscle groups of the shoulder and elbow joints. The stretching exercises took into account the muscles and tendons that most often undergo shortening in the SCI population.
The traditional instructions that illustrated exercises to subjects in the PAPER group were based on guidelines from the international literature. 10 In addition to text descriptions, we included photographs of a person performing the exercises to improve clarity. The APP group received the instructions from Fisiofriend. The app was installed on their personal smartphones. All participants in the two groups had to perform 3 sessions per week, and the load they had to use was personalized in the same way, based on an initial evaluation with an isokinetic dynamometer and a stress test with Heart rate (Hr) monitoring.
Subjects were tested at the beginning (t1) and end (t2) of the program, focusing on strength of upper limbs and aerobic performance. The clinical evaluation took place in the Spinal Unit of the Institute of Physical Medicine and Rehabilitation “Gervasutta”.
We performed the isokinetic test using System4 Biodex dynamometer (Biodex Medical Systems, New York, US), focusing on the movements of flexion and extension of elbow to obtain an objective performance evaluation of the muscles that have a key role in determining the functional abilities of a SCI patient. In particular, we tested the parameter of force (Torque: peak moment of force) and work. These parameters for flexors and extensors were measured while the subjects performed 4 repetitions of the movement in concentric/concentric modality at 60°/s. We evaluated also subject's endurance (a measure of fatigue during exercise) examined on 20 repetitions in concentric/concentric modality at 120°/s. The Biodex System used a fatigue index defined as the ratio between the first third and the last third of work in the test bout. Normative parameters set the index between 20% and 30%.
We evaluated aerobic performance with a portable VO2000 Medgraphics (Medical Graphics Corp., St Paul, Minnesota, US) breath analyzer. We evaluated peak oxygen uptake VO2 (VO2peak) during a maximal incremental stress test to exhaustion at the crank ergometer (beginning from 15 Watts, 1-min steps, increasing by 15 Watts per step). Peak oxygen uptake is the oxygen that the subject is able to use as his maximum in a unit of time during maximal exercise; it is expressed in ml/kg/min (milliliters per kg of body weight per minute). The higher is the VO2peak value, the better aerobic performance.
After the measurements at t1, each subject received a two-hour instruction session by a physiotherapist. In the APP group, the physiotherapist installed the application on the subject's phone, and asked him to perform the exercises with the app. In the training session for the PAPER group, the physiotherapist asked the subject to perform the exercises with the paper instructions.
All subjects were told to follow the home-based program assigned to them for 6-weeks. They were provided with a number to call for any possible issue, difficulty or symptom during the study period. Two subjects in the APP group suffered a biceps tendinitis episode (very common in SCI patients) during the study period and had to skip a few exercise sessions for that reason.
At the end of the 6-weeks, all subjects came to the hospital for the strength and aerobic performance tests. After measurement, they were asked to fill a questionnaire about their subjective perception of performing physical activity with the support (app or paper) used at home. The questionnaire began with “When I perform physical exercise with Fisiofriend” (APP group) or “When I perform physical exercise with the paper instructions” (PAPER group). The 18 items that followed were taken from the Physical Activity Enjoyment Scale.1,11 They were subjected to an exploratory factor analysis with principal component extraction and Varimax rotation, that revealed the presence of three components in the subjective perception questionnaire. The three components were respectively related to pleasantness of the experience (5 items), engagement (5 items), and perceived positive effects (8 items). Subjects expressed their level of agreement with each item on a 7-level Likert scale (1 = completely disagree, 7 = completely agree). Ratings of negative items were reversed to make it possible to average items in each of the three components. Two subjects in the APP group left the hospital without filling the subjective questionnaire, due to an error in the organization of the appointments.
Results
Low incidence of SCI patients in the population, and impossibility for a considerable number of SCI patients to perform home-based exercise programs (due to insufficient motor control or strength), did not allow to recruit a large sample of subjects from persons followed by the hospital. For this reason, we provide results in terms of descriptive statistics.
In both groups, we observed a general maintenance of the original peak torque value for the elbow flexor and extensor muscles of the right and left upper limb, and an improvement of fatigue and power on the extensor muscles.
Figures 6 and 7 illustrate the results obtained with the crank ergometer stress test. In APP, we observed a greater workload in Watts (a 25% increase in Watts at t2 vs. t1), while there was no change in PAPER. Moreover, in APP we observed a 19% increase of VO2peak in the stress test, while the increase in PAPER was 8%.

Percentages of change (POpeak).
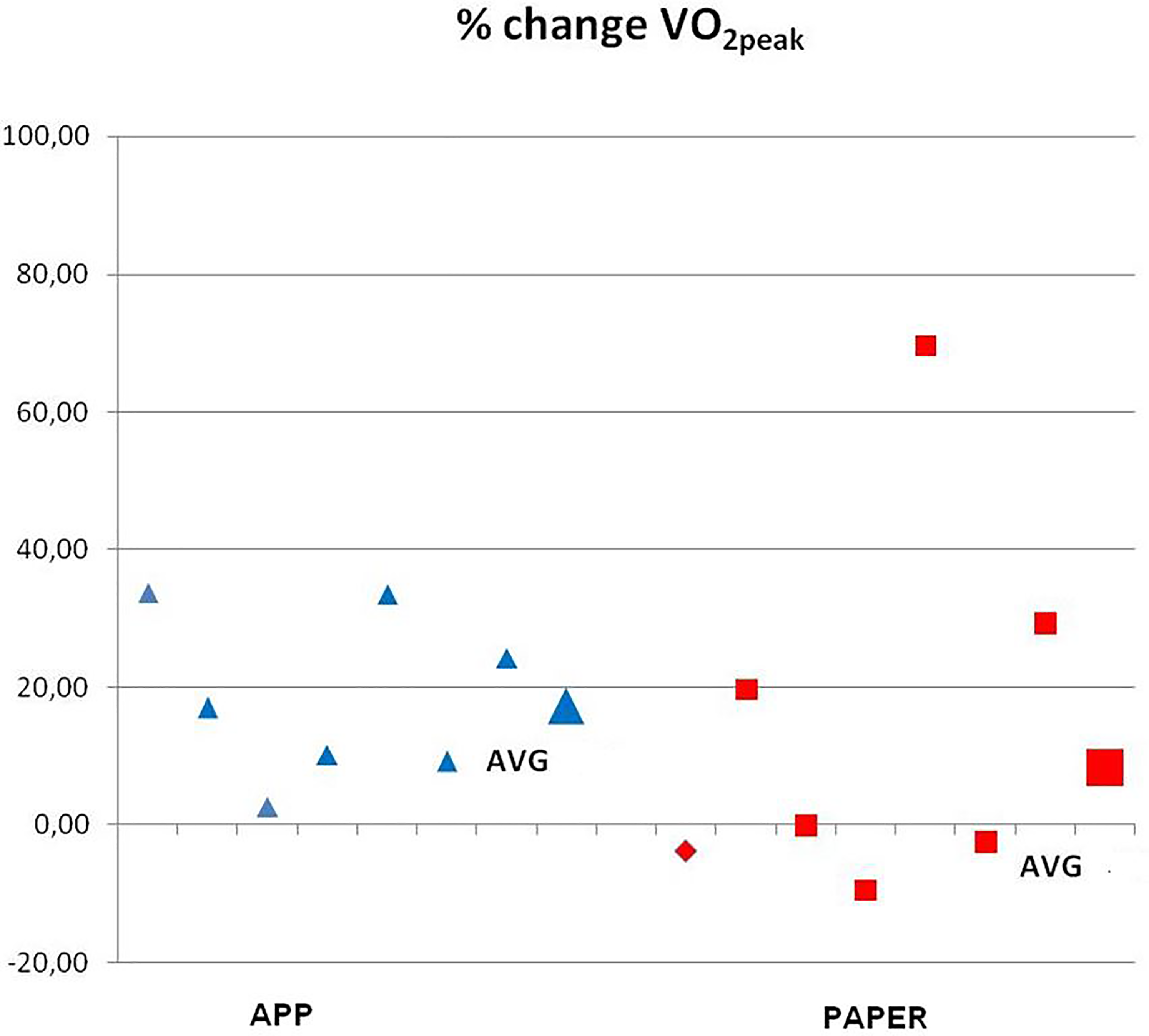
Percentages of change (VO2peak).
Table 1 provides the results of the subjective perception questionnaire, with higher values in the APP group for each of the three questionnaire components (pleasantness, engagement, and positive effects).
Subjective perceptions.

Discussion
This paper proposed a smartphone-based application to support SCI patients in home-based exercise programs, and evaluated it in a real clinical intervention, also comparing it with paper instructions traditionally given to patients.
To assess possible changes in performance obtained during the 6-weeks study, we used an isokinetic dynamometer, and an expired gas analyzer. In both patients groups (APP, PAPER), we observed changes of only a few Newton per meter between the beginning and end of the period. There was an amelioration of the fatigue index for the extensor muscles of the elbow, which returned to normative values. This improvement can be useful in daily life activities, such as execution of transfers and postural changes.
The incremental test at the crank ergometer suggests that both groups had similar improvement in exercise tolerance, although the exercise program was not focused on improving aerobic capacity. This might be explained by the fact that some subjects reported that being engaged in the program lead them to autonomously engage in additional physical activities.
While the physiological results are encouraging for both groups, the questionnaire data indicated a possible subjective advantage in the APP group. The app received better ratings in terms of pleasantness, engagement and perception of positive effects. Moreover, APP subjects verbally reported that the use of the application was simple and useful, and the feedback provided by game-like features contributed to motivation. The results of the subjective perception questionnaire were also consistent with the expectations about patient acceptability, showing good patient's satisfaction in both groups, with higher values in the APP group.
The practical experience with subjects and their informal reports suggests that a possible advantage of using a mobile app in this medical context is better instruction about exercises. Subjects considered videos to be particularly useful. However, to adopt the app in a clinical program, an important practical aspect is to perform a first training session in which the clinician gives instructions about the correct placement of the wristband and supervises the initial and final position of the shoulder, arm and hand as the patient performs each exercise. In our clinical experience, it turned out that 2 h was an appropriate length for such initial training, making all patients in the APP (resp. PAPER) group autonomous in performing the home-based program with the app (resp. paper instructions).
Another advantage for the patients was the app real-time feedback, which allowed them to monitor how well they were following the instructions, and the possibility of keeping track of their progress and achievements.
From the clinical perspective, the data collection function of the application was useful, because it allowed us to check patients’ compliance with the exercise program, and keep track of subjects’ achievements. This is particularly important, considering that the number of patients who do not perform exercises in home-based programs is large, and estimated to be one to two thirds of patients. 1
Practice with the application also highlighted its limits: only the 13 exercises that require movement on the frontal or sagittalis plane can be monitored through the accelerometer. Second, the exercise program turned out to be difficult to complete by tetraplegic subjects: two subjects (one in APP and one in PAPER) had a C6 lesional level and they both gave lower scores than non-tetraplegic subjects in the subjective questionnaire.
Finally, only patients who own a smartphone can use mobile apps. Lending a smartphone to patients who do not own one would solve this limitation only partially, because they would not be familiar with the device and could thus find the support more difficult to adopt than the other patients.
Conclusions
Physical inactivity is a major independent risk factor for CVD and premature mortality.1–6,12 Unfortunately, physical inactivity and marked deconditioning are highly prevalent among SCI patients. 6 Moreover, ordinary daily living activities are not adequate to maintain cardiovascular fitness in SCI patients. 13 Low levels of physical activity increase adiposity and reduce aerobic fitness. 14 In addition, a reduction in cardiovascular fitness may lead to a vicious circle of further decline, reducing functional capacity and ability to live an independent lifestyle. The literature highlights that effective exercise interventions are required to slow the progression of multiple risk factors in the SCI population. The objective of this paper was to propose a mobile application to support SCI persons in home-based programs, and to evaluate its feasibility in a 6-weeks pilot study that considered also traditional printed instructions. The application allows clinicians to select the appropriate exercises for each subject and at the same time allows the user to have a personal guide explaining the movements to be performed, and monitoring some of the exercises with the in-built accelerometer.
Although the study was carried out on a small number of patients, its results are encouraging. There was consensus among users that the application is easy to use and accessible to a large number of SCI patients, while different advantages of the app were noticed at the clinical level, as summarized in the previous section. This suggests that the introduction of mobile apps into SCI home-based programs could be valuable and accepted by patients and clinicians as well.
Our feasibility study lays the foundation for larger studies that could involve more patients over longer periods of time, including also intermediate measurements. Using the application over longer periods of time might lead to a wear off effect of the motivational game-like features. The monitoring capabilities of the app can be extended through new wireless sensors that are appearing on the market. In particular, we have just added a new function to the app to keep user's heart rate monitored through a wireless connection with an external Zephyr HXM BT Bluetooth sensor: if the HR threshold (set by the clinician based on patient's status) is exceeded, an audible alarm and a message on the screen informs the patient that the exercise must be temporarily stopped. Moreover, we are implementing notifications that could be managed by the physiotherapist and automatically sent to the patient on a periodic specific basis according to the user's needs and the time elapsed since the exercise program beginning, working as tailored prompts to promote compliance.
In terms of measurements, the study could be further developed with the analysis of the correct muscle recruitment during exercise through surface electromyography, in particular the physiological timing in the recruitment of agonist and antagonist muscles and the parameters relating to fatigue. An additional assessment that could be considered is the evaluation of Fat-Free Mass before and after the exercise program with bioimpedance analysis.
Footnotes
Acknowledgments
None
Author contributions
Author’s note:
Agostino Zampa, Rehabilitation Center “Comunità Piergiorgio”, Udine, Italy.
Ethical approval
Not applicable.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/ or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written consent was obtained from all participants prior to the commencement of the research.
Trial registration
Not applicable, because this article does not contain any clinical trials.