
Abstract
Background
Hypnotic intervention for irritable bowel syndrome (IBS), or gut-directed hypnotherapy (GDH), is an effective treatment for improving IBS symptoms with minimal burden and risk in delivery to patients. The Nerva app, developed by Mindset Health, shows promise for dissemination and implementation of evidence-based GDH intervention for IBS.
Objectives
This study aimed to describe the demographic and clinical characteristics of Nerva app users, examine usage patterns, and explore potential factors associated with Nerva app usage.
Methods
A retrospective analysis of data was conducted of 14,898 individuals who downloaded and used the Nerva app between January 2022 and September 2022. Descriptive statistics and Chi-square tests of independence were calculated to examine demographic/clinical characteristics, usage patterns, and their associations to program persistence. Simple linear regression models were used for correlations of GI symptoms severity scores to user persistence.
Results
Users predominantly identified as female (77.2%; n = 11,503) and had a mean age of 38.59 years old (SD = 13.38). Thirty-one percent of users persisted with the program, and a small statistically significant association was found between Nerva app program persistence and age, χ2 (6, N = 6745) = 164.82, p < 0.001, V = .16.
Conclusions
The present study found promising adherence rates for the Nerva app program within the first six weeks of use. Statistics in prevalence estimates of IBS agree with previous literature and significant associations were found between user/clinical characteristics and Nerva app program persistence.
Keywords
Background[19]
Irritable bowel syndrome (IBS) is one of the most common functional gastrointestinal disorders, presenting in approximately 9–11% of adults worldwide with higher prevalence in women than men.1–4 The central symptoms of IBS include recurrent abdominal pain and altered bowel habits.5–7 Individuals diagnosed with IBS often experience higher incidences of psychological distress such as anxiety, depression, and lower quality of life.8–11 The standard medical care for IBS is pharmacological intervention, dietary recommendations, and stress reduction; however, these methods have displayed limited efficacy. 12
Hypnosis is defined as “a state of consciousness involving focused attention and reduced peripheral awareness characterized by an enhanced capacity for response to suggestion.” 13 Hypnotic intervention for IBS, or gut-directed hypnotherapy (GDH), has demonstrated to be effective in improving IBS symptoms with minimal burden and risk in delivery to patients.14–21 However, widespread dissemination of GDH for IBS in adults has not yet been achieved. Potential barriers of implementation include limited accessibility to qualified hypnotherapists as well as limited affordability. 22 Mobile phone applications provide an alternative method of delivering hypnotherapy in an accessible, cost-effective, and convenient way.23–25 Limited studies have empirically examined mobile application–delivered hypnotherapeutic interventions for individuals with IBS. 26 Preliminary research suggests that self-administered and remotely delivered hypnotic interventions for IBS are likely to show therapeutic efficacy equivalent to face-to-face delivery.27,28
The Nerva mobile application is one of the few mobile-based GDH interventions available that includes promising components that would benefit from further investigation. 29 In a recent retrospective study using Nerva app user data, 64% of the sample showed clinically significant changes in the GI symptom of abdominal pain from pre-to-post program, and similar changes were observed across GI symptoms. 29
The Nerva app is a 42-session (6-week) mobile application–delivered GDH program designed and developed by Mindset Health in collaboration with a certified psychophysiologist and gut-directed hypnotherapist. It offers individuals with self-reported IBS a GDH program that can be used to self-manage symptoms. Users are provided with new guided GDH audio recordings approximately 15 min long for daily practice and are encouraged to listen to each GDH audio recording in a quiet, distraction-free setting. The audio recordings are based on the well-established Manchester Protocol 30 and are heavily informed by randomized controlled trial that showed GDH produced statistically significant improvements in overall and individual GI symptoms from pre-to postintervention and proved to be as effective as a low FODMAP die for the treatment of IBS. 19
No known study to date has described the usage metrics of a mobile app–based GDH intervention for IBS. The wider digital health intervention literature provides some evidence that participant-related factors, such as user characteristics (e.g., age, gender identity, baseline symptom severity), can influence mobile app–based intervention (mHealth) engagement. 31 High rates of attrition and nonadherence to real-world mHealth interventions also require greater empirical attention.32,33 The aims of this article are to provide demographic and clinical characteristics of Nerva app users, examine usage patterns, and explore potential factors that could be associated with Nerva app usage to identify factors of engagement with the Nerva app program.
Methods
Participants
The present study involved a retrospective analysis of data collected from 14,898 individuals with self-reported IBS symptoms who downloaded and used the Nerva app between January 2022 and September 2022. Only users who provided their informed consent digitally to the Nerva app's Privacy Policy at the time of download, which included an agreement to have data collected and used for research purposes, were included in the analysis.
Procedure
Throughout their engagement, users are prompted to complete questionnaires that assess user demographics/clinical characteristics, and symptom severity. The Nerva app also collects information about user engagement patterns over the course of the program. The demographics and clinical characteristics questionnaire was presented to each user at the initial download of the Nerva app. The current study restricted analysis to questions specific to users’ age, gender identity, duration of self-reported IBS symptoms, referral by a healthcare provider, self-assessed triggers of IBS symptoms, typical IBS physical symptoms during their flare-ups, and self-identified IBS subtype. Additionally, participants completed the Irritable Bowel Syndrome-Visual Analog Scale to rate the severity for each of their gastrointestinal symptoms34,35 at the beginning and end of the program (day 1 and day 42) and provided a symptom severity rating for overall GI symptoms on a weekly basis. Participants also completed the Four-Item Patient Health Questionnaire for Anxiety and Depression (PHQ-4) on a weekly basis to measure psychological distress.36,37 The questionnaire is a composite measure, comprised of the Patient Health Questionnaire-2 (PHQ-2) 38 and Generalized Anxiety Disorder-2 39 scales.
Nerva Mobile application description
The Nerva mobile application has three core components that users can interact with over the course of their GDH program experience. These components include daily guided GDH audio recordings, psychoeducational readings, and diaphragmatic (“deep”) breathing exercises. Content from these Nerva app components is unlocked one day at time for users to access and engage with; this occurs automatically and is not contingent upon users’ completion of session content from the previous day(s). There is a total of 42 new GDH audio recordings available for listening throughout the Nerva program and they are each approximately 15 min in duration. Users gain access to a different psychoeducational reading each day to review before they listen to their daily guided GDH audio recording. There is a total of 41 unique psychoeducational readings available for review throughout the Nerva program; one reading is provided on each day of the program apart from the last day (i.e., day 42). They are projected to take approximately 5 min each to read. Users are also introduced to a diaphragmatic breathing exercise on the last day of week 3 of the Nerva program (i.e., day 21). This deep breathing exercise can be practiced separate from the GDH audio recordings. There is a total of 21 deep breathing sessions available for completion throughout the Nerva program (i.e., one in week 3, seven in week 4, seven in week 5, and six in week 6) and they are each approximately 5 min in duration.
Statistical analysis
All data and statistical tests were analyzed and performed using IBM Statistical Package for Social Studies (SPSS) Statistics, Version 28 software (IBM SPSS 28.0). The criterion for significance was set at p < 0.05 for all statistical tests, and tests of significance were two-tailed. Descriptive statistics were calculated to describe the demographic and clinical characteristics of the total sample of 14,898 users. Potential factors associated with Nerva app program persistence were explored using a subsample of 6745 users who purchased the full 42-session program. Persistence was marked by completion of postprogram assessment surveys in full at the end of the six-week GDH intervention program.
Additionally, two types of app usage metrics were calculated for each Nerva app program component (i.e., GDH audio recordings, psychoeducational readings, deep breathing). These usage metrics were the number of new sessions completed and the number of total sessions completed. The number of new sessions completed metric represented the total number of distinct sessions completed (i.e., repetitions of an already completed session did not count towards the metric). Conversely, since users could complete a session more than once if desired, the metric observing total sessions included completion of novel sessions and repetitions. An additional metric of “cumulative number of total sessions completed” was calculated to depict the sum of total sessions completed since week one of the program.
Results
User and clinical characteristics
The demographic and clinical characteristics of the total sample of Nerva app users are displayed in Table 1. The program symptom severity scores for the total sample of Nerva app users are reported in Table 2.
Frequencies of demographic/clinical characteristics for users in total sample.

Note. N = 14,898 users who downloaded the Nerva app and completed all preprogram surveys. n = sample size. % = percentage.
Mean and standard deviation of preprogram symptom severity scores for users in total sample.

Note. N = 14,898 users who downloaded the Nerva app and completed all preprogram surveys. M = mean; SD = standard deviation.
Nerva app usage patterns
Paid users completed an average of 18.22 (SD = 14.59) new GDH audio sessions and 19.94 (SD = 16.90) total GDH audio sessions out of the 42 available. They also completed an average of 19.37 (SD = 16.15) new and 20.32 (SD = 17.11) total psychoeducational reading sessions out of the 41 available. For the deep breathing component of the app, paid users completed an average of 0.92 (SD = 1.34) new sessions and 2.97 (SD = 5.76) total sessions out of the 21 available. Given that the deep breathing exercise is introduced after the third week, this subsample includes nonpersisters, which likely consisted of users that stopped engaging with the Nerva program prior to week 4. Therefore, the mean total number of deep breathing exercises is to be interpreted with caution.
The mean number of new and total sessions completed from both the GDH audio recordings and psychoeducational readings components gradually decreased throughout the six-week program (Table 3). The mean number of completed new and total deep breathing sessions increased from the end of week 3 (i.e., when it is first introduced to users in the six-week program) into week 4 before displaying a slight decrease in usage at week 5 and 6 as compared to week 4.
Mean and standard deviation of new, total, and cumulative total sessions completed for paid users.

Note. N = 6745 users who paid for the full Nerva program past the 7-day free trial. M = mean; SD = standard deviation.
Exploring potential factors associated with Nerva app program persistence
User demographic/clinical characteristics and Nerva app program persistence
Of the 6,745 paid users analyzed, 2140 (31.7%) users persisted with the program and 4,605 (68.2%) users did not persist with the program. There were statistically significant differences found between persisters and nonpersisters across user/clinical characteristics (Table 4). The largest statistically significant difference found between persisters and nonpersisters was for age, χ2 (6, N = 6745) = 164.82, p < 0.001, V = .16. Nonpersisters were comprised of a higher percentage of users between ages 10 and 49, whereas persisters were comprised of a higher percentage of users over 50 years of age. Statistically significant differences were found between persisters and nonpersisters for other characteristics such as duration of IBS symptoms (χ2 (3, N = 6745) = 9.36, p = 0.03), IBS subtypes (χ2 (3, N = 6745) = 9.77, p = 0.02), healthcare provider referrals (χ2 (1, N = 6745) = 25.81, p < 0.001), IBS symptom triggers (χ2 (1, N = 6745) = 5.40, p = 0.02), and some IBS physical symptoms (e.g., χ2 (1, N = 6745) = 4.90, p = 0.03). However, these differences yielded trivial effect sizes (V = .03–.06). No statistically significant differences were found between persisters and nonpersisters in the following user/clinical characteristics: gender identity, the endorsed IBS symptom triggers of food, anxiety/stress, medication, exercise, other symptom triggers, and the endorsed IBS physical symptoms of abdominal pain, bloating, wind, and other physical symptoms.
Chi-square test of independence of Nerva app program persistence across user/clinical characteristics for paid users.

Note. N = 6745 users who paid for the full Nerva program past the 7-day free trial. Persisters = paid users who completed postprogram surveys in full at the end of week six. Nonpersisters = paid users who did not complete postprogram surveys in full at the end of week six. n = sample size. % = percentage. df = degrees of freedom. *p < 0.05, **p < 0.01, ***p < 0.001.
Preprogram symptom severity scores and Nerva app program persistence
There were statistically significant differences found between persisters and nonpersisters in symptom severity ratings at preprogram (Table 5). Nonpersisters presented more severe symptoms than persisters for the following ratings: overall GI symptoms, t (6743) = 2.03, P = .04; bloating, t (6743) = 3.36, p < 0.001; nausea, t (6743) = 6.62, p < 0.001; and psychological distress, t (6743) = 5.64, p < 0.001. The results of each independent samples t-test remained statistically significant after FDR-BH correction for multiplicity. However, each significant difference found yielded a d-statistic ranging from .05 to .17. No statistically significant differences were found between persisters and nonpersisters in the preprogram IBS symptom severity ratings for abdominal pain, passage of wind, and stool consistency.
Independent samples t-tests of preprogram symptom severity scores and Nerva app program persistence for paid users.
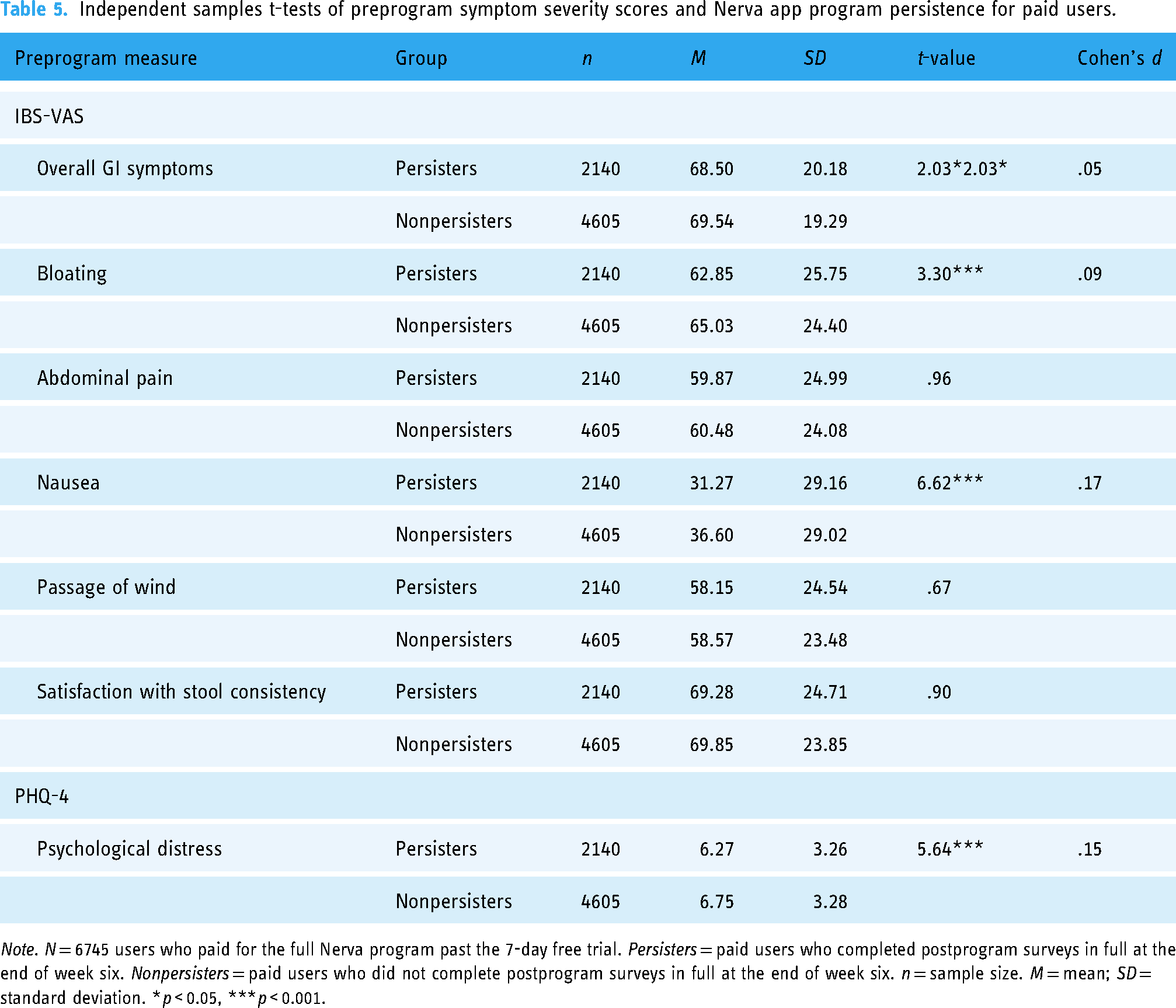
Note. N = 6745 users who paid for the full Nerva program past the 7-day free trial. Persisters = paid users who completed postprogram surveys in full at the end of week six. Nonpersisters = paid users who did not complete postprogram surveys in full at the end of week six. n = sample size. M = mean; SD = standard deviation. *p < 0.05, ***p < 0.001.
Overall GI symptoms changes early in program as potential predictors of Nerva app program persistence
The overall GI symptoms difference score from preprogram to day 6 did not significantly predict user persistence with the program (R2 = <.001, F (1, 2330) = .37, p = 0.54; Table 6). The overall GI symptoms difference score from preprogram to day 13 significantly predicted user persistence with the program and explained 0.3% of the variance (R2 = .003, F (1, 1845) = 5.87, p = 0.02) (β = .06, t (1846) = 2.42, p = 0.02). The overall GI symptoms difference score from preprogram to day 20 significantly predicted user persistence with the program and explained 0.4% of the variance (R2 = .004, F (1, 1533) = 6.58, p = 0.01) (β = .07, t (1534) = 2.57, p = 0.01).
Standardized betas from simple linear regression equations testing overall GI symptoms changes as predictors of Nerva app program persistence.
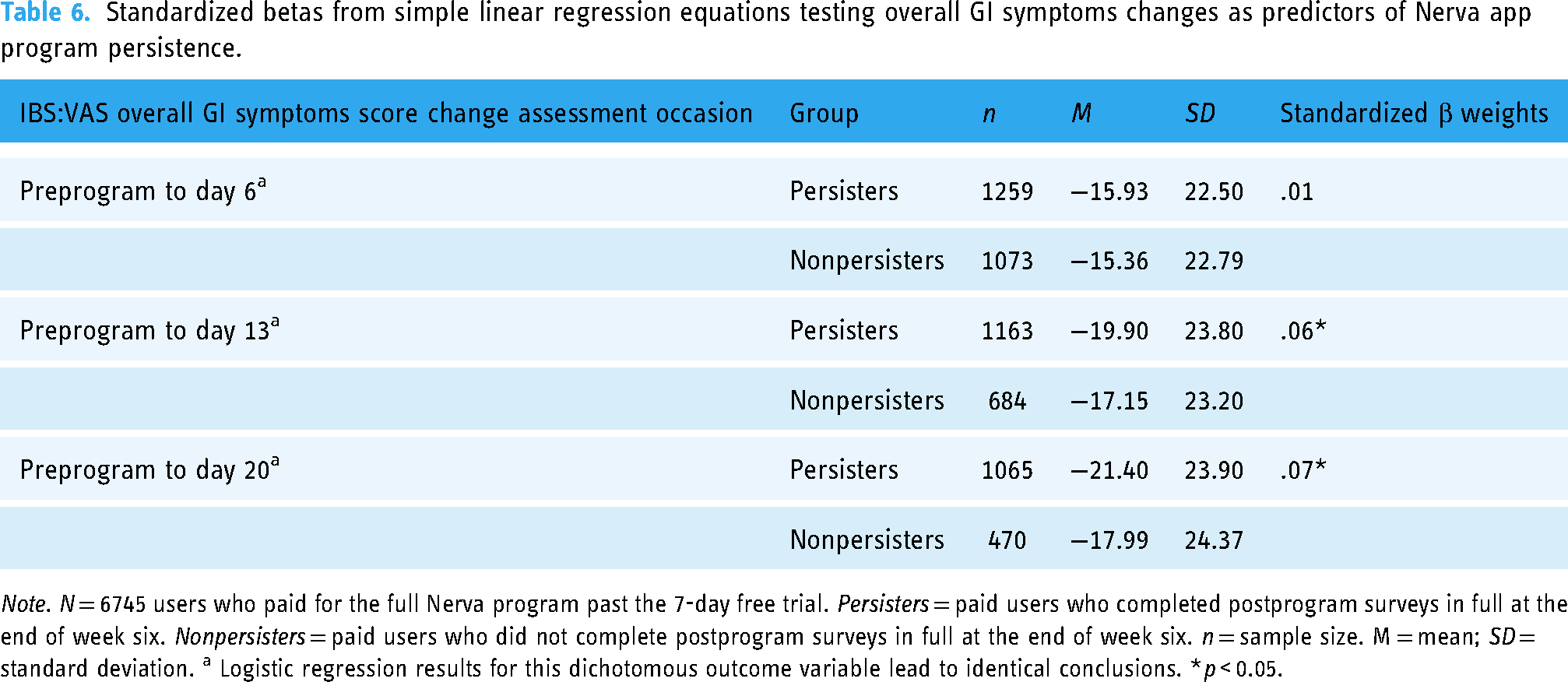
Note. N = 6745 users who paid for the full Nerva program past the 7-day free trial. Persisters = paid users who completed postprogram surveys in full at the end of week six. Nonpersisters = paid users who did not complete postprogram surveys in full at the end of week six. n = sample size. M = mean; SD = standard deviation. a Logistic regression results for this dichotomous outcome variable lead to identical conclusions. *p < 0.05.
Discussion
The user characteristics of the Nerva app sample studied largely mirror previously documented demographic and clinical characteristics of individuals with IBS in the wider empirical literature. For instance, prevalence estimates of IBS across gender identities, distribution of user age, and chronicity of the disorder were consistent with the literature.2,40,41 A vast majority of the sample (90%) was not referred to the Nerva app by a healthcare provider; this was anticipated given that GDH is widely unknown among medical professionals and consumers. 42 One of the primary goals of the Nerva app is to facilitate greater dissemination and implementation of evidence-based GDH. There are data that suggest that the opinion of a healthcare provider can influence a patients’ perception of, and eventual engagement in, a treatment of interest43–45; given this and the low percentage of healthcare provider referrals in the current sample, it may be wise for greater efforts to be made to inform healthcare professionals about Nerva app program and its’ benefits since referral to the Nerva app from a healthcare provider could potentially improve users’ overall adherence rates.
Moreover, total Nerva app usage across users suggest that paid users completed approximately half of the total GDH audio recording and psychoeducational reading sessions available from the program within the first six weeks. These rates are comparable to, or even higher than, the adherence rates displayed by users at the end of interventions of similar study design in the wider mHealth literature in which users’ real-world engagement with an app program, instead of within a controlled setting, is studied.31,46,47 Furthermore, it is possible that Nerva engagement rates could be even higher still if measured at the end of users’ subscriptions. Additional data collection is warranted to gather a better understanding of how users engage with the program throughout their paid subscription.
The mean number of new and total sessions completed within each Nerva app component was very similar for this subsample of paid users. This suggests that they typically moved onto completing another new session instead of repeating a session that they already completed. The gradual decrease in the mean number of new and total sessions completed aligns with adherence rates of mHealth interventions across wider mHealth literature.48,49 Importantly, these data depicting the typical usage patterns across Nerva app users can inform further tailoring of the Nerva application in a way that optimizes users’ Nerva app experience. For example, since users tend to display less engagement with the Nerva app over time, the addition of Nerva app features to later in the program that are specifically designed to increase user engagement (e.g., positive reinforcement in the form of rewards and reminders) might be worthwhile.50,51
Persistence with the Nerva app program was significantly associated with older age (50–70+ years old) and nonpersistence was significantly associated with younger age (10–49 years old). One plausible explanation for this may be that older users are more motivated to engage to achieve treatment benefit since they may have tried more treatments over time. 27 Given this possibility, assessment of user motivation as a potential moderator of treatment response may be a worthy avenue for future studies. Another curiosity emerges when the positive association between Nerva app persistence and age is considered alongside the results from Peters and colleagues’ 29 retrospective evaluation of Nerva app data that suggest a positive association between clinically significant response and increased age. These results suggest Nerva app usage may be an important moderator of response; however, more research is needed since the present analyses do not allow for causal inference.
The trivial associations found between the other user demographic/clinical characteristics and Nerva app program persistence suggest that these variables (e.g., duration of IBS symptoms, IBS subtype, etc.) may have limited ability to differentiate between which users are likely to persist and not persist with the Nerva app program. There may be other user characteristics that better predict Nerva app program persistence that went unmeasured in the present study. For example, treatment credibility, 52 self-efficacy, 53 and motivation 52 have been demonstrated to positively influence adherence in other studies. Taken together, the Nerva app may look to include assessment of these variables across users in the future.
Nonpersisters showed more severe baseline symptoms for overall GI symptoms, bloating, and nausea than persisters, albeit of a trivial effect size. Consistent with findings by Devenney and colleagues 54 who explored predictive factors for a face-to-face, individualized, GDH intervention, it is possible that individuals with more severe IBS symptoms at baseline may require a more individualized approach or potential referral for therapist delivered GDH. Relatedly, nonpersisters presented with more severe ratings of psychological distress at baseline than persisters. This too was a similar pattern depicted by Devenney and colleagues, 54 and suggests that users with high baseline levels of psychological distress may benefit more from a nonspecific, psychological approach rather than a targeted, gut-specific, behavioral treatment like GDH. This is the first investigation known to the authors that has shown these potential associations in a GDH mobile app and provides evidence to suggest that the Nerva app may benefit from further customization of each users’ Nerva app intervention based off of their responses to assessment questions at the onset of their program experience. This seems of additional potential importance given that there are data to suggest that personalized intervention content may also predict higher rates of adherence to online psychological interventions. 55 For example, it is possible that user experience and engagement may be improved if the Nerva app allowed for greater customization, such as the ability to select what voice is used for their guided GDH audio recordings. Relatedly, some data suggest that mHealth interventions with guidance or therapist support show greater rates of adherence compared to those with no support or administrative support. 56 Thus, it may be of interest to explore how app alterations that offer more guidance impacts user experience, engagement, and symptom improvement.
It may be wise to first collect and analyze qualitative feedback from Nerva app users themselves, much like was done by Noble and colleagues 57 in their exploration of patient perceptions of a remotely delivered GDH intervention via Skype. Assessment of how users’ interface with the Nerva app throughout the program, as well as Nerva app users’ satisfaction with the program and obstacles to engagement, could be very informative for Nerva app development. Analysis of other user characteristics and usage patterns collected from the Nerva app users not explored within the present study would be a worthwhile endeavor as it would further contribute to a more nuanced understanding of the Nerva app program, who it can help, and how it can help. For example, it has been suggested that smartphone-delivered GDH skills training may be better suited for individuals “without significant comorbidities” 27 ; however, this has not yet been empirically tested. Future studies may be interested in collecting additional data on comorbidities and how they may influence potential benefit from the Nerva app program.
The self-directed format of the Nerva application and its reliance on self-reported symptoms and self-diagnosis of IBS can potentially waste users’ time and lead to delays in users’ receiving accurate diagnosis and effective healthcare. For example, it is possible that a user may wrongly assume that their symptoms are explained by IBS instead of another, potentially more serious, medical condition and use the Nerva app instead of pursuing medical advice, medical care, or a professional opinion. Thus, it would be prudent for the Nerva app to modify their initial screening process to either attempt to rule out inappropriate users or, if that is not feasible, include a warning or disclaimer to all users at the start of their Nerva app program experience that brings attention to the fact that other medical conditions can mimic or share overlap with the symptom profile of IBS and that it is strongly recommended that they follow up with a healthcare provider first to more formally rule out other medical conditions before proceeding with the program. An additional Nerva app modification of importance is to ensure that parent permission and consent are appropriately obtained from users under 18 years of age. Lastly, given access to symptom and usage patterns data across users and recent interest in the field of GDH in dose–response relationships, future studies may be interested in investigating the potential relationship/association between Nerva app program usage and symptom improvement.
Conclusions
Mobile application delivery of GDH for IBS offers several advantages over face-to-face hypnotherapy, including increased accessibility, reduced health care costs, and decreased clinical provider burden 27 ; thus, Nerva can serve as a viable means to overcome the research-practice implementation gap. The current study explored the user characteristics, patterns of use, and factors of engagement of a mobile application delivery of GDH for individuals with self-reported IBS. Significant associations were found between user/clinical characteristics and Nerva app program persistence. Overall, the results of the current study yield a better understanding of Nerva app users, their usage patterns, and the association between the two, which ultimately can be used to inform dissemination practices and future app modifications so that users’ experience can be optimized. These findings also underscore the importance of user characteristics and app usage as valuable factors of study in evaluation of mobile health interventions for IBS.
Footnotes
Acknowledgements
This project would not have been possible without the generous support of Mindset Health. Specifically, the authors would like to thank the following team members at Mindset Health: Chris Nauomidis, Dr. Simone Peters, and Claire Davidson for their discussions on potential directions for future research as well as their overall guidance and support throughout project implementation and Rafael Mello for his technical assistance with data management. The authors also thank members of the Baylor University faculty, Dr. Alisha Wray, Dr. Sara Dolan, Dr. Keith Sanford, and Dr. Jocelyn McGee, for the invaluable insight and expertise they provided throughout the duration of the project. The authors would like to express our appreciation for all of the users of the Nerva app that consented to contribute their data for scientific research study such as this; it is ultimately their participation that allows for the advancement of our knowledge in this area of research.
Contributorship
LS and GE conceived and designed the study. LS researched literature, gained ethical approval, organized and analyzed the data, and wrote the first draft of the manuscript. VM confirmed analysis of the data. KS researched the literature and made revisions to the discussion section. GE oversaw the study's progress at all phases. All authors reviewed and edited the manuscript and approved the final version.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mindset Health has funded the current research. GE serves on Mindset Health's Scientific Advisory Board and provides consulting services to Mindset Health.
Disclosures
Ethical approval
The study protocol as described was approved by the Institutional Review Board at Baylor University (IRB Reference #: 1997465). All authors approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Mindset Health.
Guarantor
GE.