
Abstract
Objective
As a result of the growing access to the Internet, online medical platforms have gained increased popularity in China. However, which strategies doctors should use to improve their online communication with patients remains understudied. Drawing upon the performance-evaluation-outcome (PEO) model, the present study seeks to develop a typology of patient-centered communication (PCC) strategies online and identify those strategies that can increase patient satisfaction.
Methods
We employed the data crawling technique to access text-based patient–provider transcripts through a large medical consultation platform in China and coded 9140 conversational turns of doctors.
Results
Our analysis revealed 15 PCC strategies that Chinese doctors often used online. In addition, several strategies were found to enhance patient satisfaction including information provision, making diagnosis, information appraisal, emotion expression, emotion recognition and support, in-depth discussion of medical treatments, providing coping strategies, and enabling self-management.
Conclusion
Chinese patients may have developed multiple needs, which they expect to fulfill through their interactions with doctors. Technological affordances of online medical platforms may pressure doctors to adapt their communication strategies to patients’ needs. Our findings develop the PEO model from the perspective of patient-provider communication strategies and add a perspective centering on patients’ needs to the scholarship on patient satisfaction. In addition, these results provide practical implications on how to improve patient-provider communication online.
Keywords
Introduction
In China, unequal economic developments have contributed to inequitable distribution of the healthcare resources. 1 Patients from the underdeveloped regions often lack access to medical resources. By enabling patients to visit doctors nationwide, online medical consultations present an opportunity to bridge the gap of medical resources between different regions. Thus, while we acknowledge that online medical consultations are not perfect and can cause a series of problems such as increased workload for doctors, 2 it may still be necessary to promote these services given their potential to benefit average individuals.
The performance-evaluation-outcome (PEO) model contends that individuals’ decision to use a service depends on their evaluation of the service, which is affected by the attributes of this service. 3 Thus, patients may want to use online medical consultations only when they make positive evaluations of and feel satisfied with these services. 4 Previous research has revealed the factors affecting patient satisfaction from at least two perspectives.5,6 While one perspective underscores the importance of experience of patients, the other perspective centers on patient expectations and argues that their medical experiences aligning with or exceeding their expectations lead to heightened levels of patient satisfaction.5,6 Therefore, both perspectives acknowledge that experiences of patients are central to their satisfaction.
Previous research has discovered a range of variables closely related to patient experiences.4–8 One variable consistently found to affect patient experience, and their satisfaction was their communication with doctors, no matter whether it happens online or offline.7–13 However, the self-report measure of patient-provider communication in these studies7,9–13 makes it hard to understand what counts effective patient-provider communication online.
Prior research has offered empirical evidence showing that patient-centered communication (PCC) is positively associated with patient satisfaction. 14 Specifically, one line of scholarship on PCC conceptualized this concept as a type of communication that responds to patients’ needs by informing, engaging, and empowering them.15–18 Prior research has revealed a typology of PCC strategies that address multiple needs of patients such as high-quality advice and treatments, emotional support, relationship building, and involvement in decision making.14,15,19–23 However, most research on PCC strategies is conducted offline,14,19–23 which limits the generalizability of some strategies to the online setting because technological affordances of medical consultation platforms make it impossible to use certain strategies online. 24 In addition, Internet-based technologies may create additional needs that patients expect to be fulfilled by doctors. 25 Thus, it is necessary to examine what PCC strategies are used and can predict patient satisfaction in the online setting.
Broadly situated in the PEO model, 4 the present study aims to answer the questions mentioned above by content analyzing the transcripts of patient-provider conversations via a text-based platform of online medical consultation. Theoretically, our results are expected to develop the PEO model from the perspective of patient-provider communication strategies especially strategies in the online setting. In addition, given the close connections between patient needs, PCC, and patient satisfaction, we seek to offer an approach to developing the scholarship on patient satisfaction which centers on patient needs. Practically, this investigation is expected to offer guidance on how to conduct quality patient-provider communication online for future interventions.
Patient-provider communication and patient satisfaction
Originally proposed to explain consumer behavior, the PEO model posits that individuals’ decisions to purchase certain products are a function of the attributes of these products, mediated through their product evaluation. 3 Subsequent research extended this model to medical services, and their research findings highlighted the positive relationship between patient evaluation and the decision to seek medical consultations.4,7,12 In these studies, patient evaluation was often operationalized as patient satisfaction.4,7,12
Previous research argued that patient satisfaction might vary as a function of patients’ experience or their expectation.5,6 On the one hand, positive experiences tend to make patients more satisfied, which translates into heightened intentions to continue to seek medical consultations.4,7,12 On the other hand, patient satisfaction was argued to result from their expectations.5,6 If the received medical services align with or exceed their expectation, patients are more likely to feel satisfied. 26 Although this perspective underscores the influence of patient expectation, their experience still plays an important role in how they evaluate the medical service they have received.
Systematic reviews revealed a wide spectrum of variables that affected patient satisfaction.5–8 These variables include the quality of medical treatments and advice, the physical environment of the hospitals, as well as interpersonal communication with providers.5–8 Specifically, Dagger and her team found that the quality of patient-provider communication was positively associated with medical service quality, patient satisfaction, and the intention to visit the same clinic. 7 The positive relationship between patient-provider communication and patient satisfaction held after confounding variables were controlled. 9 The same finding was replicated online.11–13 For instance, offering informational and emotional support in patient-provider communication was found to elevate patient satisfaction online. 13
Although these studies established connections between effective patient-provider communication and patient satisfaction, they tended to use self-report measures to assess patients’ evaluation of their interaction with physicians.7–13 Consequently, based on these results, what counts effective patient-provider communication online remains unknown. The present study aims to bridge this gap by drawing upon the concept of PCC.
From physician-centeredness to patient-centeredness
There have been at least three models describing patient-provider relationships. The activity-passivity model compared this relationship as parents and infants, in which patients receive medical treatment from physicians without offering any responses. 27 The guidance-cooperation model described the doctor-patient relationship as cooperative, in which physicians tell patients what to do and patients comply with these guidelines. 27
In contrast, the mutual participation model advocates for respecting and responding to patients’ needs and perspectives. 27 Specifically, this model argues that patients should be granted more opportunities to make decisions about their health and allowed to choose the treatment plan they prefer. 27
Therefore, the relationship between physicians and patients has undergone a transition from physician-centeredness to patient-centeredness. The value of patient-centeredness suggests that patients’ needs and perspectives should be respected and addressed, which provides a foundation for PCC. 17 Many studies have reached consensus that respecting and responding to patients’ needs is key to the conceptualization of PCC.17–19 For example, doctors are expected to explain diseases and treatment plans in a way that patients can understand so their informational needs can be fulfilled.17–19 Patients should also be involved in the decision making process to fulfill their autonomy needs.17–19 Additionally, providers are expected to help patients cope with emotional distress and build a relationship with them characterized by mutual respect and trust so their emotional and relational needs can be satisfied.17–19 Taken together, despite the myriad of the conceptualization of PCC, one important component of this concept is that doctors should respect and respond to patients’ multidimensional needs by informing, engaging, and empowering them.15,17–19
PCC online
Epstein and Street proposed six dimensions of PCC: exchanging information, fostering relationships, responding to emotions, managing uncertainty, making decisions, and enabling self-management. 15 First, patients and physicians should exchange biomedical and psychosocial information to assist the development of medical treatment plans. Second, patient-provider communication should help relationship building characterized by trust and rapport. Next, providers should recognize and respond to their patients’ emotional state, offering emotional support when needed. Moreover, physicians should address the uncertainty of patients and help them manage it. Additionally, physicians should involve patients in making decisions about the treatment plan. Finally, providers should enhance patients’ ability to follow through treatment plans and help them develop a health-enhancing lifestyle.
Subsequent research has provided extensive evidence showing that PCC can enhance patient satisfaction,28,29 increase their trust in doctors, 22 make patients more involved in communication with doctors, 23 and lead to greater medical adherence. 30 In addition, previous studies have revealed specific PCC strategies.14,19–23,30,31 While most strategies align with the six dimensions of PCC, 15 some research found additional strategies such as understanding patients’ preferences, 31 using appropriate humor, 14 listening, 14 empathic communication through nonverbal cues, 14 encouraging health management behaviors, 20 using simple language, 21 and making sure patients understand the information. 21
However, most research on PCC strategies is conducted offline.14,15,19–23,30 Thus, some of these strategies may not be applied online. First, offline research on PCC strategies underscores the importance of emotion expression through nonverbal cues. 14 However, as some online medical consultation platforms are text-based (i.e., the platform the current research analyzed), many nonverbal cues are not available online. 24 Hence, online, emotions may only be expressed through verbal messages.
On the other hand, the affordances of Internet-based technologies likely create opportunities for other PCC strategies. Specifically, the asynchronous nature of online communication affords extensive time for patient-provider interactions, which makes in-depth medical discussions possible. Additionally, online, patients have easier access to medical information, which makes them more prepared for discussions about their health issues. 32 Thus, probing into health conditions, in-depth discussions about the health condition, and shared decision making are likely online, which however are not included in many measures of offline PCC strategies.14,22,23
Furthermore, the Internet may increase the importance of addressing certain needs of patients. For example, the prevalence of misinformation heightens patients’ needs for health information evaluation. 25 Notably, without the Internet, patients can also be exposed to misinformation through their personal network or traditional mass media. However, the Internet offers people easy access to volumes of information, which elevates the chance of exposure to misinformation. Thus, nowadays, patients may need professional advice that helps them distinguish correct health information.
Therefore, online, doctors may leverage different PCC strategies because of technological affordances of medical consultation platforms and patients’ additional needs. We ask the following research questions:
RQ1: What strategies did doctors in China use online to exchange information, foster relationships with patients, respond to patients’ emotions, manage uncertainty, make cooperative decisions, and enable self-management? RQ2: What PCC strategies online are positively related to patient satisfaction?
Method
Overview
The present study employed a content analysis approach to answer the research questions proposed above for the following considerations. While survey research that measured PCC as patients’ self-report perceptions revealed positive associations between PCC and patient satisfaction,14,28,29 this relationship became nonsignificant if PCC was measured by coding the transcripts of patient-provider communication. 33 Social desirability bias may explain this discrepancy. 34 As social desirability is more likely in the survey, a content analysis approach can minimize the chance of this error.
Data collection
We used the data crawling technique via Python to access the communication transcripts between patients and doctors through a large medical consultation platform in China, Spring Rain Doctor. All transcripts are textual, without any visual or audio information. These transcripts, in which personally identifiable information has already been removed, are publicly available to all researchers.
As of August 2020, Spring Rain Doctor had 130,000,000 registered users including 630,000 doctors. 35 In addition, the platform allows its users to evaluate their doctors through three rankings (3 = very satisfied, 2 = moderately satisfied, 1 = unsatisfied). As gynecology and pediatrics are mostly visited via Spring Rain Doctor, our sample focuses on the communication transcripts with doctors in these two departments. Thus, we used a 2 (department: gynecology vs. pediatrics) * 3 (satisfactory level: very, moderate, not) between-subjects design.
We accessed the transcripts between patients and doctors between May 2013, the earliest time when the transcript was available, and December 2020, when the data collection started. It is important to note that Spring Rain Doctor does not make all transcripts publicly available. Therefore, despite the wide time range, we could only access 220 records of complete doctor-patient conversations in the departments of gynecology and pediatrics. We deleted the conversations that were too short to provide sufficient information for coding. In order to minimize the validity and power issue caused by unequal group sizes, we intentionally made the number of conversations equal across all six groups by randomly selecting 25 conversations from each group. Therefore, the final sample size of the current study is 150 conversations.
We divided every conversation based on the turn takings of the patient and the doctor, defined as the period in which one party (patient or doctor) finished the conversation. In other words, turn takings happen in the present study when, for instance, a patient finishes his/her statements and a doctor is about to start talking. During one turn taking, all the word that one party (patient or doctor) spoke was the unit of analysis of this study. The 150 conversations in our sample included 18,800 conversational turns, including 9140 from doctors and 9660 from patients.
Characteristics of sampled doctors and patients
The only demographic information about doctors that was publicly available through Spring Rain Doctor is their gender, department, and title. Most sampled doctors were female (112 or 74.7%). Over half of them were attending physicians (85 or 56.7%), followed by associate physician (37 or 24.7%), physician in charge (15 or 10.0%), and physician (13 or 8.7%).
Spring Rain Doctor does not require patients to provide their demographic information. Thus, the demographics of patients is incomplete. Out of 150 patients in our sample, 144 revealed their gender, with 114 identifying themselves as female (76.0%) and 30 as male (20.0%). Although 106 patients recorded their age, we suspect this information was inaccurate, given its minimum (1) and maximum (117). Therefore, variables about patients’ demographics were excluded from further analysis.
Data coding
Since Epstein and Street provided sufficient details about the definition of PCC, 15 we built our coding scheme on their work. Specifically, we established the six first-level categories of online PCC strategies, following the six dimensions of PCC. 15 Next, we went throughout the transcripts to identify the themes of online PCC strategies in each category. Themes were discussed and revised. The final coding scheme includes 15 online PCC strategies within the six categories.
Table 1 provides the conceptualization and example for all 15 strategies. The first category, information exchange, includes five strategies: information provision, probing into the health condition, making diagnosis, clarifying jargons, and information appraisal. Notably, information provision does not include treatment plans, only medical information that helps patients understand their health problem and other general health questions.
The coding scheme of patient-centered communication strategies
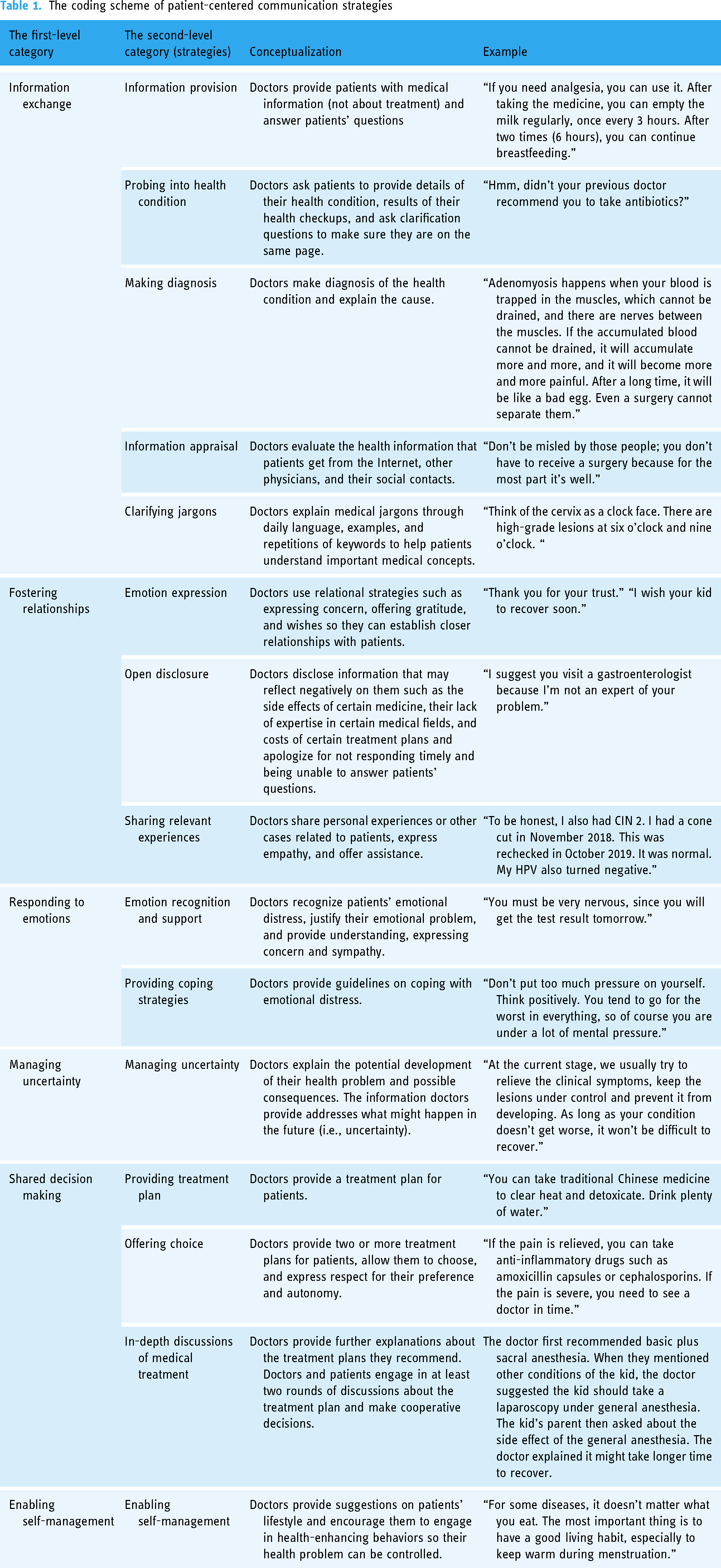
The second category, fostering relationships, includes three strategies: emotion expression, open disclosure, and sharing relevant experiences. These strategies all function for the same goal: to build a close relationship with patients. However, they employ different means. Emotion expression refers to doctors’ verbal expression of emotions such as gratitude, concern, and wishes, usually initiated by doctors rather than as a response to patients’ words. Open disclosure refers to doctors’ disclosure of the information that may reflect negatively on them. Sharing relevant experiences refers to doctors’ sharing of personal or other relevant experiences.
The third category, responding to emotions, is used when doctors address patients’ emotional distress. Two strategies were identified, emotion recognition and support and providing coping strategies. The former refers to the statements showing that doctors have recognized patients’ emotional distress, whereas the latter refers to statements aimed to help patients cope with their emotional distress.
The fourth category, managing uncertainty, includes only one strategy. Notably, uncertainty in this study referred to anything regarding the future developments of the patient's health problem and possible consequences.
The fifth category, shared decision making, involves three strategies: providing treatment plan, offering choice, and in-depth discussions of medical treatments. The information that doctors provide here is all about treatment plans.
Finally, the last category, enabling self-management, includes only one strategy. Here, doctors provide information beyond the patient's specific health problem, which can help them maintain good health condition and live a healthy lifestyle.
Each strategy was coded as absence (0) or presence (1). Two trained graduate students coded 20% of the total conversations. Intercoder reliability was calculated through Holsti's method. The first round of coding led to an average intercoder reliability of .78. They resolved misunderstanding about the coding scheme and procedure through discussions, which increased the average intercoder reliability to .94. They then finished the rest of the coding.
Additionally, patient satisfaction was assessed for each doctor with three levels (3 = very satisfied, 2 = moderately satisfied, 1 = unsatisfied). Therefore, we counted the number of every strategy that each doctor used, which was used as the independent variable in the analysis for RQ2.
Statistical analyses
As a response to RQ1, descriptive statistics were performed. We reported the number of count that each PCC strategy was used as well as its percentage. We also compared whether there was significant difference in terms of the count of several strategies through either Wilcoxon signed-rank test (comparisons between two) or Friedman test (comparisons among more than two).
RQ2 was answered through two statistical methods. First, we compared whether there was any significant difference in terms of the number of PCC strategies used between three levels of patient satisfaction (very, moderate, not). As most counts were not normally distributed, we conducted Kruskal-Wallis H test as an alternative.
As Kruskal-Wallis H test did not consider any control variables, we performed multinomial logistic regression. Control variables include the doctor's gender (0 = male, 1 = female), department (0 = pediatrics, 1 = gynecology), and title (1 = physician, 2 = attending physician, 3 = associate physician, 4 = physician in charge). Physician in charge was set as the reference category. As mentioned before, given the incomplete data of patients’ gender and the inaccurate report of their age, we did not control any variables about patients.
Results
Online PCC strategies (RQ1)
As mentioned above, we identified 15 PCC strategies. Out of 9140 conversational turns from doctors, 7929 (or 86.75%) used at least one PCC strategy. The five most commonly used PCC strategies were in-depth discussions of medical treatments (1236 or 15.59%), followed by information provision (1232 or 15.54%), making diagnosis (1176 or 14.83%), providing treatment plan (1140 or 14.38%), and probing into health condition (976 or 12.31%). These five strategies account for 72.64% of the total PCC strategies. Friedman test revealed no significant difference in terms of the count between these strategies: χ2(4) = 3.87; p = .42.
Apart from these five strategies, enabling self-management was used the most (352 or 4.44%). Wilcoxon signed-rank test revealed significant difference in terms of the count between enabling self-management and probing into health condition: z = -8.49; p < .001. Next was clarifying jargons (337 or 4.25%), followed by emotion expression (292 or 3.68%), information appraisal (283 or 3.57%), offering choice (231 or 2.91%), emotion recognition and support (228 or 2.88%), open disclosure (179 or 2.26%), managing uncertainty (122 or 1.54%), providing coping strategies (80 or 1.01%), and sharing relevant experiences (65 or .82%).
Following the six dimensions of PCC, 10 information exchange was used the most (4004 or 50.50%). Next was shared decision making (2607 or 32.88%). The remaining four categories of patient-centered communication strategies were used less prevalent (fostering relationship, 536 or 6.76%; enabling self-management, 352 or 4.44%; responding to emotions, 308 or 3.88%; managing uncertainty, 122 or 1.54%).
We further categorized these dimensions into socioemotional strategies and instrumental strategies. Fostering relationship and responding to emotions address the emotional and relational needs of patients and are used to develop closer patient-provider relationship. Thus, they were categorized as socioemotional strategies. The other four categories are used to treat patients and promote their health, so they were categorized as instrumental strategies. Wilcoxon signed-rank test shows that instrumental strategies were used significantly more than socioemotional strategies: z = 10.62; p < .001.
Strategies predicting patient satisfaction (RQ2)
Results of Kruskal-Wallis H test revealed significant differences between three groups of patient satisfaction in terms of the frequency of information provision (χ2 (2) = 13.30, p = .001), making diagnosis (χ2 (2) = 10.30, p = .006), information appraisal (χ2 (2) = 14.85, p = .001), emotion expression (χ2 (2) = 19.74, p < .001), emotion recognition and support (χ2 (2) = 14.06, p = .001), and in-depth discussions of medical treatments (χ2 (2) = 16.67, p < .001). Moreover, we found marginal difference in terms of the frequency of providing coping strategies (χ2 (2) = 4.85, p = .088) and enabling self-management (χ2 (2) = 4.75, p = .093). Table 2 presents results of the Kruskal-Wallis H test.
Comparing the usage of patient-centered communication strategies by doctors between very, moderately and not satisfied patients
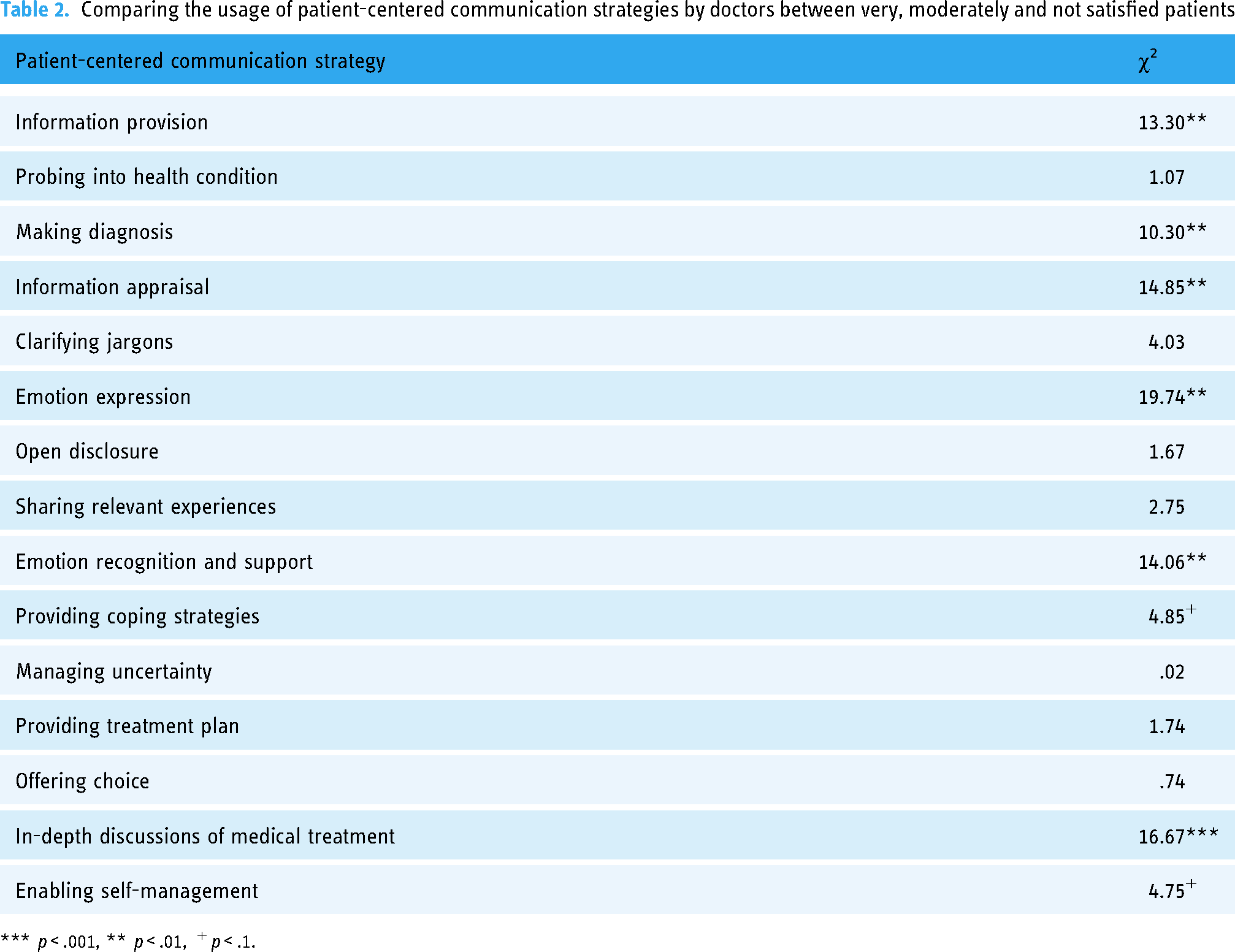
*** p < .001, ** p < .01, + p < .1.
In addition, the multinomial logistic regression model demonstrated a good model fit, χ2 (40) = 108.08, p < .001, Nagelkerke R2 = .33 (Table 3). Controlling for doctor's gender, title, and department, strategies exhibiting a significant relationship with patient satisfaction included information provision (χ2 (2) = 10.86, p = .004), making diagnosis (χ2 (2) = 7.02, p = .03), information appraisal (χ2 (2) = 13.37, p = .001), emotion expression (χ2 (2) = 13.44, p = .001), emotion recognition and support (χ2 (2) = 6.37, p = .041), and in-depth discussions of medical treatment (χ2 (2) = 14.43, p = .001). Providing coping strategies was marginally significantly related to patient satisfaction (χ2 (2) = 5.73, p = .057).
The multinomial regression of patient satisfaction on patient-centered communication strategies

Note: Reference group: female (gender), pediatrics (department), physician in charge (title).
** p < .01, * p < .5, + p < .1.
Furthermore, compared to the patients unsatisfied with their doctor, patients who were moderately satisfied with their doctor reported that their doctor were more likely to use information provision (OR = 1.11, 95% CI [1.01, 1.22], p = .024). As for the other strategies, no significant difference was found between these two groups.
More significantly different results emerged between very satisfied patients and unsatisfied patients. Specifically, after controlling for doctor's gender, title, and department, compared to unsatisfied patients, very satisfied patients reported their doctors were more likely to use the following strategies: information provision (OR = 1.17, 95% CI [1.05, 1.30], p = .005), making diagnosis (OR = 1.15, 95% CI [1.01, 1.29], p = .029), information appraisal (OR = 1.34, 95% CI [1.02, 1.76], p = .035), emotion expression (OR = 1.31, 95% CI [1.05, 1.65], p = .019), emotion recognition and support (OR = 1.71, 95% CI [1.01, 2.89], p = .047), and in-depth discussions of medical treatment (OR = 1.17, 95% CI [1.05, 1.30], p = .003). Taken together, results of Kruskal-Wallis H test and multinomial logistic regression were similar.
Discussions
Online medical consultations exhibit great potentials to bridge the gap of medical resources between different regions. This can be especially helpful for patients in China, where the unequal economic development has contributed to the inequitable distribution of medical resources. According to the PEO model, patients may only want to use these platforms when they feel satisfied with the services they have received through these platforms.3,4 Prior research has offered consistent evidence on the positive association between effective patient-provider communication and patient satisfaction,7–13 but what strategies can improve patient-provider communication remains unclear within the PEO framework. In addition, the majority of PCC research is conducted offline.14,15,19–23 By content analyzing the transcripts of patient-provider communication via Spring Rain Doctor, we summarized 15 PCC strategies that doctors in China used online. We also identified the PCC strategies that positively predicted patient satisfaction. These results underscore the importance of fulfilling patient needs to maintain their satisfaction and encourage them to use online medical consultations. In addition, our findings suggest how patient needs develop as a function of Internet-based technologies. Finally, these investigations provide practical implications for interventions on improving physicians’ communication skills online.
Major findings
Online PCC and patient needs
Our investigation revealed 15 online PCC strategies that doctors in China often used. In addition, our analysis revealed what strategies doctors could use to elevate patient satisfaction. Specifically, information provision, making diagnosis, information appraisal, emotion expression, emotion recognition and support, and in-depth discussion of medical treatments were positively related to patient satisfaction. Providing coping strategies was marginally significantly related to patient satisfaction. As for enabling self-management, Kruskal-Wallis H test found a marginally significant relationship between this strategy and patient satisfaction, but multinomial logistic regression revealed this relationship was not significant perhaps because doctors’ characteristics were controlled.
As reviewed earlier, although most research on the PEO model has established a positive relationship between patient-provider communication and patient satisfaction, these studies did not reveal specific communication strategies that can enhance patient satisfaction. Thus, our findings bridge this gap by identifying effective patient-provider communication strategies.
Furthermore, these findings demonstrate which PCC strategies are valued more by patients. Recall that PCC is essentially the communication centered around patient needs.17–19 Our analysis provides empirical evidence which suggests what patients in China need out of their interactions with physicians. The first and the most basic need is to treat their diseases, as indicated by information provision, making diagnosis, and in-depth discussions of medical treatments. This aligns with findings from the scholarship on patient satisfaction, which consistently demonstrate that the quality of received medical services is positively related to patient satisfaction.3–8
Second, as emotion expression, emotion recognition and support, and providing coping strategies suggest, patients may want doctors to fulfill their emotional needs. Several studies have offered evidence showing the effectiveness of emotional support and relational immediacy to improving patient-provider relationship and optimizing its communication outcome.14,17,20,22,23 However, the current result may need to be interpreted in the context of Chinese medical culture. As the doctor-patient rate in China is far below the average in the world, 36 Chinese patients tend to feel rushed in their offline medical consultations. Moreover, as the primary goal of seeking medical consultations online is instrumental, Chinese patients may not expect their doctors to provide them with emotional support. Consequently, when they receive emotional support from their doctors, they may interpret it as a positive violation of expectancy, which often leads to positive evaluations of the doctor. 37 This finding aligns with a study which showed that emotional support provision was more strongly related to patient satisfaction in China than information support provision. 11
Next, the importance of in-depth discussions of medical treatments shows that patients in China exhibit needs for collaborative decision making. Previous research has found that shared decision making could improve patient-provider communication, but these studies were conducted in the Western countries.19,23 In China, typically, doctors make decisions for patients whereas patients have no choice but comply with doctors’ regimens. 38 However, our results suggest that Chinese patients might have been challenging this communication style and want to be more involved in medical decision making. Therefore, Chinese doctors need to change their perception of treating patients as inferior, respect patients’ autonomy, and give them more power in decision making. Given that the lack of medical expertise may inhibit patients from making appropriate decisions, doctors should use strategies like clarifying jargons to help them understand and make decisions.
Additionally, our results demonstrate that information appraisal could significantly enhance patient satisfaction. This strategy was rarely found in prior PCC research14,15,19–23,30,31 probably because most previous studies were conducted offline. Although people may also receive misinformation offline, the Internet offers them easy access to volumes of misinformation. Thus, informational appraisal may have become a crucial need for patients. Doctors that can help them distinguish correct health information are more likely to receive recognitions.
Furthermore, findings of enabling self-management were inconsistent, and this strategy was not used as often as other strategies. However, prior research on PCC has acknowledged the value of this strategy. 20 Moreover, this strategy demonstrates an additional patient need: health management. Traditionally, patients seek medical consultations because they want a specific health problem to be treated. However, by providing health-enhancing suggestions on patients’ lifestyle, enabling self-management goes beyond treating one particular disease and addresses the question of health management. These two needs—informational appraisal and health management—suggest that doctors are expected to serve as the health consultant for patients.
Taken together, our investigation shows that online PCC strategies heightening the level of patient satisfaction likely address and respond to patient needs. Given the close connection between PCC and patient need,17,19 this finding is not surprising. However, this finding may provide a new perspective that can extend the current research on patient satisfaction. As reviewed earlier, the extant scholarship argues that patient satisfaction varies as a function of either patient experience or their expectation.5,6 Our findings provide a third perspective explaining the dynamics of patient satisfaction, which focuses on patient needs.
This perspective can also explain empirical results on patient satisfaction. For example, as Sun and her colleagues found, patients’ perception of the security of online medical platforms was positively related to their satisfaction with these platforms. 39 This might be because online, patients have a heightened level of needs for privacy protection. Thus, if they thought online medical platforms could protect their privacy, they might feel more satisfied with these platforms.
This need-based perspective provides a potential direction for future research on patient satisfaction. Specifically, future research can employ theories on human needs to better understand what factors may predict patient satisfaction. For instance, as self-determination theory posits, individuals have three fundamental needs: autonomy, competence, and relatedness. 40 Thus, patients are more likely to feel satisfied with medical services that respond to these needs.
Online PCC and technology
It is important to discuss the relationship between technology and PCC strategies. Recent research on user behavior of Internet-based technologies argues that technological affordances of new media may provide users with opportunities to fulfill new gratifications, which affect their subsequent behavior of using new media. 41 Although direct evidence is lacking which demonstrates the relationship between specific technological affordances and PCC strategies online, we argue that at least three findings of the present research might be related to technological affordances of online medical platforms.
First, PCC presents an approach to patient-provider communication characterized by equal relationships between patients and their physicians. This equality is closely related to technological affordances of Internet-based platforms. Traditionally, patients can only choose local doctors. However, online medical consultation services enable them to evaluate and choose doctors nationwide. This obviously adds to the power of patients and pressures doctors to treat them with respect, autonomy, and equality, 42 even in a country where the culture is predominantly characterized by high power distance.
Next, as explained above, the asynchronous nature of online communication affords patients and doctors extended time for interactions. This makes it possible to engage in communication behaviors that require more time such as probing into patients’ health conditions, exchanging extensive health information, and conducting in-depth discussions with patients about medical treatments. Notably, these strategies were among the five most frequently used PCC strategies online. Therefore, doctors might be willing to devote extended time to interacting with their patients if they are allowed to.
Additionally, recall that we categorize PCC strategies into instrumental and socioemotional strategies. Those five most frequently used strategies were all instrumental. Indeed, overall, instrumental strategies were used more often than socioemotional strategies, which differs from previous PCC research, as those studies underscore the value of socioemotional strategies to PCC.14,20,22,23 One possible explanation is that the platform we studied only allows for textual transcripts. In other words, this platform should be considered a type of lean media. 24 Consequently, it can be difficult to have relational conversations between patients and providers, 24 making online patient-provider communication instrumental in nature.
However, we still found evidence on the relational dimension of patient-provider communication via this platform. Specifically, although relational conversation is difficult online, we still found that doctors in China tried relationship building with patients and responding to their emotions. This might be because these doctors recognized the importance of addressing patients’ emotional needs. Thus, although technology limits their ability to engage in relational conversations, they seek other methods to fulfill patients’ needs for emotional support.
Theoretical implications
This study provides important theoretical implications as follows. First, our study demonstrates which PCC strategies can elevate patient satisfaction. Hence, we developed the PEO model from a perspective of patient-provider communication strategies. Second, our results shed light on the relationship between patient needs, PCC, and patient satisfaction. Thus, we developed the scholarship on patient satisfaction by offering an additional perspective which centers on patient needs. In addition, by revealing 15 strategies that were often used by Chinese doctors online, we developed the concept of PCC to the online setting. These findings shed light on the dynamics by which technology and human needs affect PCC strategies.
Practical implications
The present research also provides practical implications for interventions on patient-provider communication. The existing interventions on patient-provider communication online tend to focus on enhancing patients’ or doctors’ skills of using Internet-based technologies.43,44 However, compared to using technology, it may be more important to enhance their communication skills. The typology of 15 online PCC strategies provides a guideline for future interventions.
In addition, our study provides practical implications on the design of online medical platforms. As our finding and prior research11,22,23 show, patients are more satisfied when doctors provide emotional support and try to establish a closer relationship with them. Thus, medical platforms should provide more affordances that can facilitate relational conversations.
Limitations and future directions
Despite these implications, findings of the present study must be interpreted with following caveats. First, our investigation focuses exclusively on doctors’ communication behavior. However, the outcome of patient-provider communication is jointly shaped by doctors and patients. Moreover, patients’ communication behavior can affect doctors’ communication strategies. Therefore, the interaction effect between patients’ and doctors’ communication deserves scholarly attention.
Second, we only analyzed 150 conversations between patients and doctors, so the sample of our study is relatively small. This limits our ability to examine more complicated relationships between patients’ communication, doctors’ communication, and patient satisfaction.
Third, our sample is Chinese and accessed through only one medical platform. These obviously limit the validity of our findings. Investigations are needed to examine whether other patient-centered communication strategies were used in other countries and via other platforms.
Next, our sample is limited to only two departments, and the majority of sampled doctors is female. This lowers the internal and external validity of our results.
Additionally, our coding only focuses on verbal messages. However, nonverbal immediacy is an important component of PCC. Although our transcripts are textual only, future research can analyze visual and audio transcripts, which may be available through other medical platforms.
Furthermore, content analysis makes it impossible to assess patients’ perception of doctors’ communication behavior. For example, although doctors may engage in relational-building conversations, we do not know whether patients perceive these conversations as relational building. Yet patients’ perception can have a critical impact on their satisfaction. Future research should compare the results of content analysis and survey.
Finally, also because of content analysis, we could only measure patient satisfaction by using their overall rating of doctors. However, this measure cannot capture the nuances of patient satisfaction, which according to prior research includes multiple dimensions.4–7
In addition to addressing these concerns, future research can extend the current investigation through following directions. Specifically, future research can examine the relationship between technological affordances and specific PCC strategies online to better understand how technology influences PCC. Additionally, our study provides a need-based perspective of understanding the dynamics of patient-provider communication and patient satisfaction. Thus, future research can incorporate need-based theories to better understand what specific needs patients want doctors to address during their conversations and examine how these needs are related to patient-provider communication and patient satisfaction. Finally, intervention studies through experimental methods are also needed to examine the effect of these strategies.
Conclusion
Through a content analysis of online patient-provider communication transcripts in China, the present study revealed 15 PCC strategies often used by Chinese doctors online and identified the strategies which can elevate patient satisfaction. Our findings suggest that Chinese patients may have developed multiple needs and technological developments in this country may pressure doctors to adjust their communication to these needs.
Footnotes
Acknowledgments
The authors would like to thank Zeliang Li for his assistance in data coding in this research.
Author contributions
JRR and JG researched the literature and designed the coding scheme. JG collected and coded the transcript with ZL. JRR and KY did the data analysis. JG wrote the first draft of the manuscript. JRR and KY revised the manuscript. All authors approved the final version of the paper.
Consent statement
This study is a content analysis, so no participants were recruited. As mentioned above, we used data publicly available to all researchers, so no consent form is needed.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
As this study used data publicly available to all researchers, we did not need ethical approval.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Guangdong Planning Office of Philosophy and Social Science under grant GD21CXW04.
Guarantor
JRR