
Abstract
Objective
Online medical consultation (OMC) is increasingly used in China, but there have been few in-depth studies of consultation arrangements and fee structures of online doctors in China. This research assessed the consultation arrangements and fee structure of OMC in China by undertaking a case study of obesity doctors from four representative OMC platforms.
Methods
Detailed information, including fees, waiting time and doctor information, was collected from four obesity OMC platforms and analyzed using descriptive statistical analysis.
Results
The obesity OMC platforms in China shared similarities in the use of big data and artificial intelligence (AI) but differed across service access, specific consultation arrangements and fees. Big data search and AI response technologies were used by most platforms to match users with doctors and reduce doctors’ pressure. The descriptive statistical analysis showed that the higher the rank of the online doctor, the higher the online fee and the longer the wait time. Through a comparison with offline hospitals, we found online doctors’ fees exceeded offline hospital doctors’ fees by up to 90%.
Conclusions
OMC platforms can gain competitive advantages over offline medical institutions through the following measures: make fuller use of big data and AI technologies to provide users with longer duration, lower cost and more efficient consultation services; provide better user experience than offline medical institutions; use big data and fee advantages to screen doctors to match users’ consultation needs instead of screening by the rank of doctors only; and cooperate with commercial insurance providers to provide innovative health care packages.
Introduction
Online medical consultation (OMC) is a growing health service trend in China. Although implemented later than other countries, OMC has developed rapidly in China, gaining a reputation for wide coverage compared to many other countries.1,2 Common across many countries suffering from the COVID-19 pandemic, the Chinese government issued a series of regulations to guide citizens to online medical treatment to attenuate the spread of COVID-19. These measures promoted OMC 3 already reliant on remote communication technology, facilitating the transfer of many offline medical needs to online platforms. 4 Given the expansion of OMC platforms, an important issue is online medical service provision and pricing in China. Although an important innovation in health servicing, there has been no in-depth study of the consultation arrangements and fee structure of OMC platforms. This lack of OMC studies is surprising since pricing and service provision are not only of significance for online consultation market participants and doctors but also of interest to government health authorities and hospitals.
To avoid disease selection bias, 5 we selected obesity as a case study since obesity displays both chronic disease management characteristics and common health consultation needs. By studying the structure of online consultations and fee charging by obesity doctors, rather than analyzing the platform-wide fee data of doctors without distinguishing disease types,6,7 the charging characteristics of online doctor consultation platforms can be revealed in a targeted manner. Further, obesity has become an important issue in China's public health and social governance. The Report on Status of Nutrition and Chronic Diseases of Chinese Residents (2020) found that 34.3% of adults in China were troubled by being overweight and 16.4% by obesity.8,9 In terms of disease management, overweight and obesity treatment involves a long treatment cycle, with a high demand for standard procedures during frequent subsequent visits, which can be provided by OMC at low cost. 10 Second, from the perspective of patients’ medical needs, online obesity consultations can promote diagnosis, precautionary behavior and diet and exercise regimes during the process of weight loss and disease treatment. Obesity online consultations are prompt, cheap and convenient and encourage treatment compliance. 11 Third, in terms of psychological needs of patients, obesity patients frequently suffer from social pressure, 12 where online one-to-one doctor–patient communication can reduce the psychological pressure on obesity patients caused by the hospital environment. 13
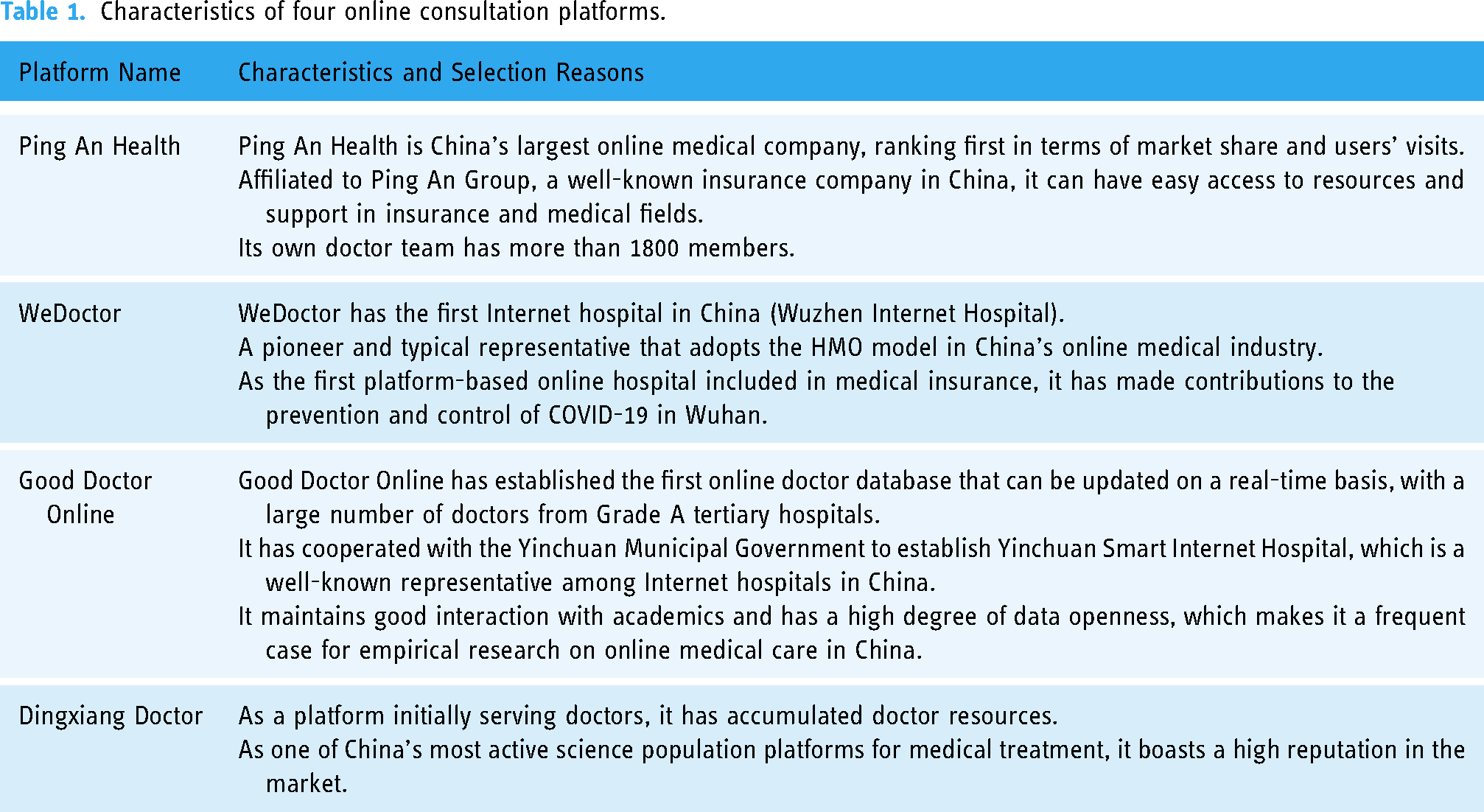
As shown in Table 1, we selected four representative obesity OMC platforms in China and analyzed their consultation arrangements and fee structure. Since some Chinese hospitals have OMC platforms, their pricing is the same as their offline pricing, so our analysis compares offline hospitals and OMC platforms. To fully reveal the online fee patterns, we conducted a detailed descriptive statistical analysis of the fees charged by obesity doctors on three of the online platforms. Besides revealing the consultation arrangements and fee structure of China's OMC, we provide information and make recommendations, for health service regulators of online consultation platforms.
Characteristics of four online consultation platforms.
Methods
Selection of OMC platforms
As set out in Table 1, all our obesity data were selected from the four major OMC platforms: Ping An Health, WeDoctor, Good Doctor Online and Dingxiang Doctor. The four platforms had app portals and were ranked among the top online platforms in terms of the number of active users and market share. 14 Besides market share and user reputation, these platforms had their own operating models and charging arrangements. In addition to app portals, WeDoctor, Good Doctor Online and Dingxiang Doctor also had webpage portals, which allowed more specific data capture and analysis. The largest and best-known online platform in China, Ping An Health, was an exception, without a web portal, which meant that Ping An Health was not included in the statistical tests but was included in the comparisons and discussion. Ping An Health was characterized by a large team of self-employed doctors with standardized fee rules and famous for cooperating with national well-known experts charging high fees. Since different obesity doctors charged differently, except for Ping An Health, we collected specific fee charging data from three online consultation platforms to compare the pricing patterns of obesity doctors.
Data collection
Python technology was used to capture the consultation arrangements, fee structure and related public information on doctors who provided obesity consultation from the webpages of WeDoctor, Good Doctor Online and Dingxiang Doctor in July 2021. There were around 20 Ping An online obesity doctors, and given Ping An Health's small obesity doctor sample size and the absence of a webpage for consultations, Python technology was not suitable for data collection. Ping An Health had unified consultation rules, which are summarized in Appendix A. As shown in Table 2, the type of doctor information disclosed on each platform was broadly comparable across platforms, with the slight differences noted.
Doctor information available on online obesity consultation platforms.

Results
Online consultation arrangements
The consultation arrangements for doctors on OMC platforms shared similarities. As shown in Appendix A, there were three major forms of online consultation arrangements: graphical consultation, voice consultation and video consultation. For graphical consultation, the patient sent consultation-related graph, text and voice records to the doctor, and the doctor responded to the patient after assessing the patient's information. While this communication system allowed both doctors and patients to have more time for assessing the information, there was a time delay. Similar to phone communications, voice consultation used the communication system of the OMC platform. After the doctor confirmed the receipt of consultation request, the patient directly consulted the doctor within the limited allocated time slot, which had the advantage of prompt feedback. As for video consultation, the patient directly communicated with the doctor through the video system of the OMC platform. The doctor and the patient saw each other on a real-time basis through cameras, providing a form of face-to-face consultation, which was close to offline consultations.
Second, Appendix A shows that the OMC platforms had doctors from all professional ranks, comprising chief physicians, deputy chief physicians, attending physicians and resident physicians (ranking from high to low). OMC platforms preferred doctors from Grade A tertiary hospitals, or urban hospitals, with the highest grade medical equipment and best medical staff and research facilities. 15 Given these commonalities, Appendix A shows that the differences in doctors’ consultation arrangements mainly reflected in waiting time, consultation access settings, specific consultation rules and fees.
While the consultation arrangement revealed in Appendix A shared several constituent elements in common, the discussion below sets out each platform's distinguishing characteristics and competitive advantages.
Consultation arrangements for obesity doctors on Ping An Health
Ping An Health obesity consultation services had the following key characteristics. First, the free ‘Quick Consultation’ channel enabled users to have free consultation services within 15 min. The free services ensured a response within three minutes using artificial intelligence (AI) technology. Patients completed personal questions and stated their health needs according to questions raised by the AI system, and the doctor gave advice based on the AI record. Although Quick Consultation is free, doctors usually provided suggestions on drugs and dietary supplements according to the patient's health conditions, which was an important way for Ping An Health to make profits. Second, Ping An Health doctors only worked for Grade A tertiary hospitals or the Ping An Internet Hospital. As shown in Appendix A, the consultation fees for Ping An Internet Hospital online were lower than doctors from Grade A tertiary hospitals.
Consultation arrangements for obesity doctors on WeDoctor
Doctors from Grade A tertiary hospitals were the most important marketing point for WeDoctor. To enable users to have more direct access to tertiary hospital doctors, WeDoctor provided two consultation channels. The first consultation channel was ‘finding a doctor within three minutes’ that linked patient–doctor within three minutes, with uniform fee standards. After users described their health conditions and paid a fee, the platform automatically matched users with tertiary hospital doctors. The second consultation channel was to pay-a-fee and obtain answers from at least five Grade A tertiary hospital doctors. The user described their diseases and problems, and then, the platform matched five to ten Grade A tertiary hospital doctors with the user. This channel took the form of graphical consultation by default. The doctor only gave a one-time brief diagnosis conclusion, and the users could not raise additional questions. This consultation design allowed the user to get answers from different doctors on the same question and compare them. Duration and consultation rules, but not fees, were standardized across doctor categories on WeDoctor, in contrast to Ping An Health, which allowed doctors from Grade A tertiary hospitals to change rules like consultation duration. As shown in Appendix A, graphical consultation was available in an unlimited number of communications within 24 h; voice consultation was fixed at 15 min; and the duration of video consultation was not strictly limited and much closer to the offline experience.
Consultation arrangements for obesity doctors on Good Doctor Online
Good Doctor Online also emphasized access to doctors from Grade A tertiary hospitals, claiming 240,000 real-name certified doctors. As shown in Appendix A, the Good Doctor Online platform provided channels for free and quick consultations. For free consultations, after the user completes their basic information, the platform automatically matched a doctor to the patient. Free consultation was limited to graphical consultations, and the doctor can reply to the user at most three times. The quick consultation service was similar to ‘finding a doctor within three minutes’ on WeDoctor, but not limited to doctors from Grade A tertiary hospitals.
In terms of the doctors’ consultation services, Good Doctor Online mainly adopted graphical consultation and voice consultation, and only a few doctors provide video consultation. Despite non-uniform fees, Good Doctor Online, like WeDoctor, adopted uniform consultation rules. In addition to graphical consultation, Good Doctor Online also provided a ‘Q&A’ graphical consultation service, which had a low fee, but was suitable for simple, conventional medical consultations. Good Doctor Online does not calculate the average waiting time but uses qualitative statements, such as fast, normal and slow.
Consultation arrangements for obesity doctors on Dingxiang Doctor
Dingxiang Doctor provided two access services, one was low-cost consultations, in which users can get a discount of 10–50% on posted consultation fees. This service set limits on the type of doctor and the number of users. The second service matched doctors with users through the platform's AI system. Compared with other platforms that attached importance to chief physician consultations, most obesity doctors on Dingxiang Doctor were attending physicians from tertiary hospitals and only graphical consultation and voice consultation were available. As shown in Appendix A, the consultation adopted unified rules, and the platform provided reference waiting time based on the doctor's previous consultations.
From the above surveys, the current OMC platforms shared four common characteristics: first, big data search and AI response technologies were adopted to match users with doctors; second, doctors from Grade A tertiary hospitals were preferred; three, each platform provided quick consultation services to reduce the waiting time; and four, each platform provided low-cost or even free consultation services according to different consultation scenarios.
Statistics analysis of online obesity doctors
Python technology was used to capture types of doctors, hospital type, prices, wait time, evaluation scores, admission rates and inquiry rate information on 580 doctors who provide obesity consultation services on WeDoctor, 575 doctors on Good Doctor Online and 100 doctors on Dingxiang Doctor. Using STATA16 and Excel, we employed descriptive statistics, mainly means, standard errors, variances, counts, percentages and differences of means to analyze online doctors’ consultation arrangements and fees. As shown in Appendix B, the descriptive statistics results show that obesity doctors from tertiary hospitals account for more than 90% of the total obesity doctors on the three platforms. Second, Appendix B shows that the fees charged were related to the doctor's hospital level, where the fees charged by obesity doctors from tertiary hospitals were higher than those charged by obesity doctors from secondary hospitals. Third, the fees charged were related to the obesity doctor's title, with a descending payment from chief physicians to resident physicians. Fourth, the price of graphical consultation was generally lower than that of voice consultation. Finally, the doctor with a higher rank meant longer waiting time.
Using STATA16 and Excel to compare the pricing advantages between the three platforms, we tested the mean differences between fees on each platform. We found both the graphic and voice consultation fees from Good Doctor Online were higher than those in WeDoctor (Table 3, sections 1–2). To further compare the fee differences of doctors with different titles from different platforms, we compared fees charged by doctors with the same title from each platform. We found that attending and resident physicians’ graphic consultation fees in Dingxiang Doctor were higher than those in WeDoctor (Table 3, section 3), and graphic consultation fees charged by obesity doctors with different titles in Good Doctor Online were higher than those in WeDoctor (Table 3, sections 4–6). For voice consultation fees, only attending and resident physicians’ voice consultation fees in Good Doctor Online were significantly higher than those in WeDoctor (Table 3, section 7). Overall, the fees charged by obesity doctors with different titles from Good Doctor Online were comparatively higher than those from the other platforms, and fees charged by attending and resident obesity physicians from Dingxiang Doctor were higher than those with the same title from WeDoctor.
Significant difference tests of consultation fees.
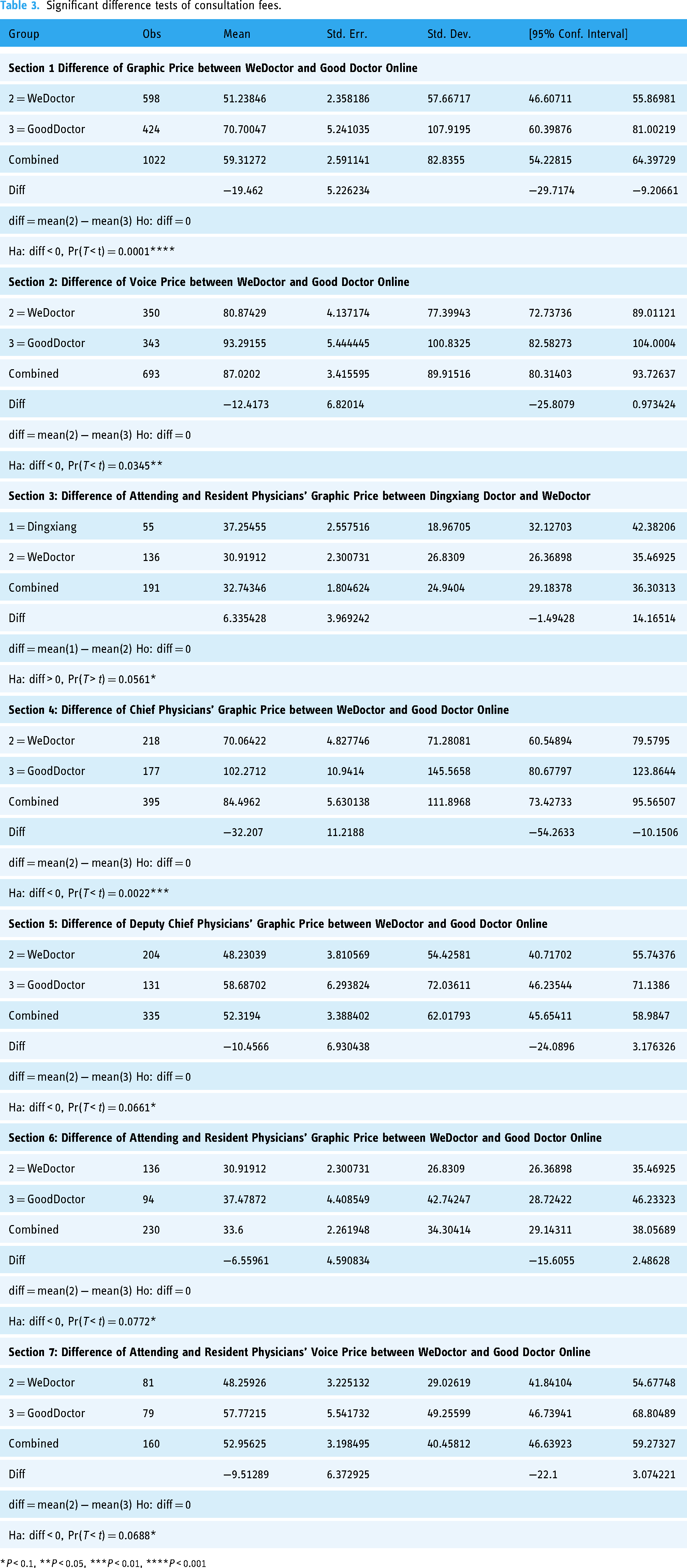
*P < 0.1, **P < 0.05, ***P < 0.01, ****P < 0.001
Since the proportion of doctors from tertiary hospitals was much higher than that from secondary and primary hospitals, for fee comparisons, we selected the average price charged by obesity doctors from tertiary hospitals on the three platforms as shown in Table 4. Although each platform performed slightly differently in graphical consultation arrangements, the prices of graphical consultation on each platform can be directly compared. In voice consultation, WeDoctor consulted within 15 min and Good Doctor Online within 10 min, so we converted voice consultation fees on WeDoctor to within 10 min fees to facilitate the comparison. Considering the platforms selected in our research accounted for a large market in Chinese online consultation industry, we estimated the average online consultation fee charged by obesity doctors by calculating the mean of the different platforms’ average price as shown in Table 4.
Average online consultation fees of obesity doctors from tertiary hospitals.

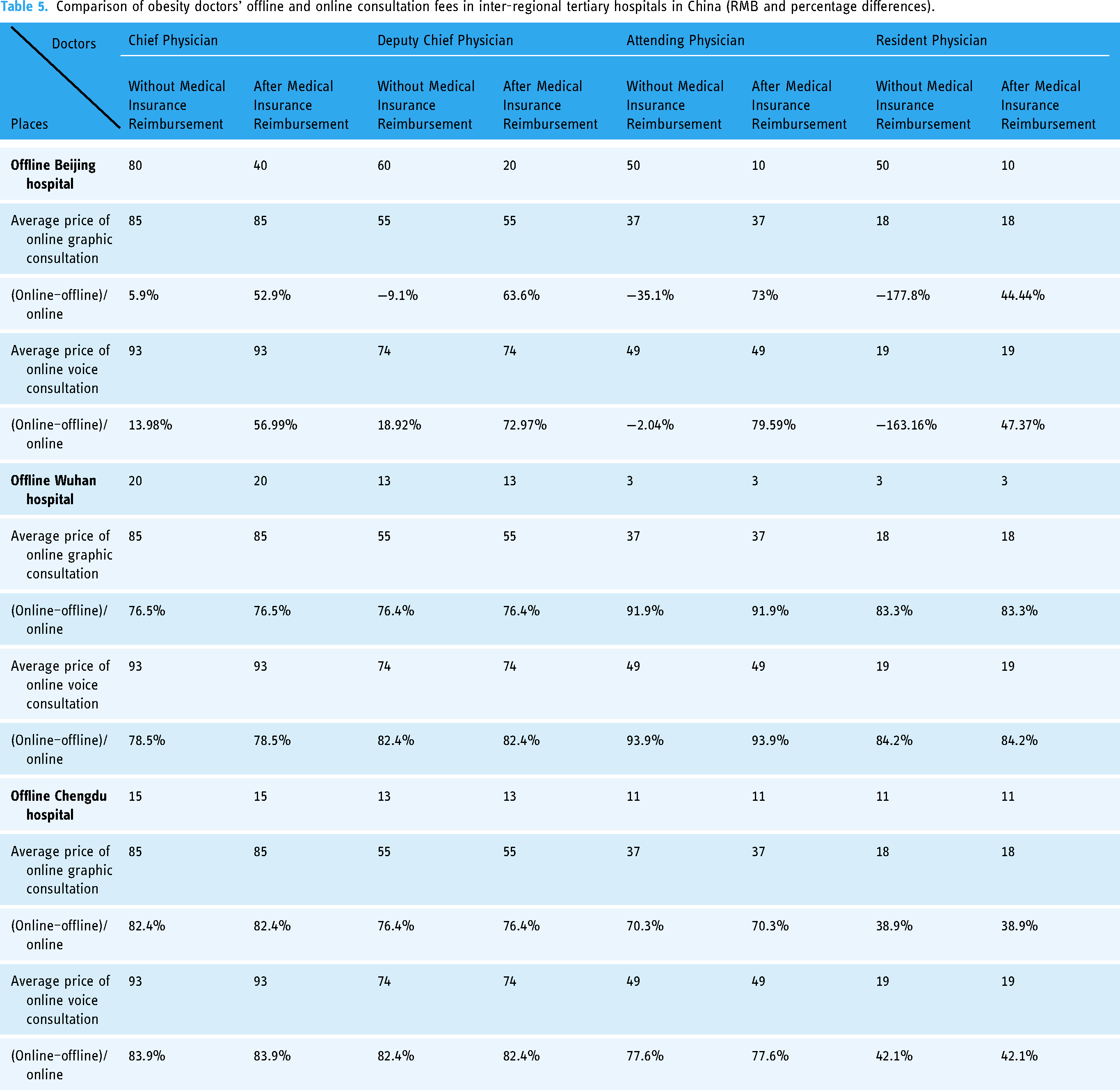
Providing new insights into online consultation fees, Table 5 provides data on inter-regional differences between online and offline consultation fees charged by obesity doctors of different ranks with those from tertiary hospitals in Beijing (eastern China), Wuhan (central China) and Chengdu (western China). In Beijing, offline consultation fees without medical insurance reimbursement charged by obesity doctors with ranks lower than chief physician were higher than average online graphic consultation fees charged by obesity doctors with the same rank, but after medical insurance reimbursement, the offline price was lower than the average online graphic consultation price by more than about 50% for doctors with different ranks. Beijing allowed residents to have instant and convenient medical insurance reimbursements when consulting in offline hospitals. In contrast, no medical insurance reimbursement policies were applicable to the online platforms. As for online voice consultation, the average fee by online doctors with different ranks was also higher than the Beijing offline price, after medical insurance reimbursement, by more than roughly 50%. Offline hospitals in central cities like Wuhan and western cities like Chengdu do not have instant medical insurance reimbursement policies for consultations like hospitals in Beijing. The fees of offline consultation by doctors with different ranks in Wuhan and Chengdu were lower than those in Beijing, reflecting the lower level of economic development in central and western China compared to eastern China. Both average fees for online voice consultation and graphic consultation were higher than offline consultation fees by around 70%, but in some cases 90% in Wuhan and Chengdu as shown in Table 5. The difference percentage shows that residents from central and western China need to pay higher online fees compared to offline hospitals located in their residence places than residents in eastern China.
Comparison of obesity doctors’ offline and online consultation fees in inter-regional tertiary hospitals in China (RMB and percentage differences).
Discussion
In terms of higher fees and the absence of medical insurance reimbursement, online consultations were inferior to hospital consultations. However, the growing popularity of online consultations suggests that online consultations provided advantages over offline hospital consultations. Through the analysis of online consultation fee structure and consultation arrangements of obesity doctors, we recommend the following initiatives to help online consultations develop in the future.
Combine big data and AI technology with initial consultations
The four consultation platforms adopted big data and AI technology in users’ initial access. Although China's recent OMC regulations forbids AI to replace doctors online, OMC should consider AI technology within China's evolving AI legal framework, which allows, for example, GAI-Chatbot techniques to augment online doctor services. By using big data and AI technology to help the online doctors at low, or no, fees, users who do not need further medical consultation services can receive early-stage medical advice. Overweight or obese people are usually concerned about diet and exercise, 16 and such questions can be answered by AI in many cases. The combination of big data technology and AI can not only save on the initial cost of offline medical consultation for obese people but also increase the adherence to physicians 17 and reduce doctors’ time to answer routine questions.
It is not rare for an ordinary outpatient doctor in China to receive 50–100 patients a day, 18 and the duration for each consultation can be less than 5 min. 19 For many conventional diseases, outpatient doctors generally have no time to communicate in detail with patients but simply give patients a diagnosis and prescribe drugs. Under this type of offline consultation scenario, AI plus real doctor consultations provide advantages, 20 especially since this kind of AI consultation services are low cost, or even free. Second, online consultations are highly attractive to patients in regions where medical resources are poor quality and short in supply. Of course, AI consultation services are limited to addressing only conventional straightforward diseases and should be supervised by doctors according to the legal supervision. Based on the online health platform case studies, there is scope to expand the use of AI for consultations, coupled with longer consultation times, more user-friendly AI-based Q&A and more scope for detailed answers to enhance their advantages over offline consultations.
Improving the consultation experience
Although online consultation saved transportation time and offline costs, 21 our analysis shows that the costs for online consultation were generally higher than those of offline medical institutions. To offset online consultation platforms’ higher costs, the platforms need to improve their consultation quality compared to offline consultations. Our findings identified three problems to be addressed by China's online consultation industry: to reduce users’ waiting time; to strengthen the management and tracking of patients; and to supervise the quality of doctors’ answers.
Appendix B shows that the waiting time for online doctors was generally more than one hour. Of course, online wait times allow users to undertake other tasks while waiting, which may not be an option for offline patients, but the online wait time advantages may not be significant for offline users near hospitals. Online consultation platforms must efficiently use big data technology to quickly match users and doctors to reduce waiting time. Second, online consultation platforms should make fuller use of AI technology to quickly match patient–doctor.
For conventional diseases in China's offline hospitals patients, see a different doctor on each subsequent visit. Offline doctors do not generally leave their contact details with patients. This medical treatment process poorly motivates Chinese doctors’ patient management. Patients with non-communicable diseases, like obesity, usually have other comorbidities that demand a doctor's active continuous role in patient management 22 and require frequent visits to physicians. 23 In addition, overweight and obese people are often prone to psychological stress due to their body shape, 24 and it is not easy for them to establish a trusting relationship with multiple doctors. Online consultation platforms can address these problems, with data recording and management systems and matching doctors and patients for long-term interaction at low cost. Due to doctors’ heavy workloads, online consultation platforms can provide doctors with an intelligent auxiliary management system to reduce doctors’ patient management workload. Currently, it is difficult for offline medical institutions to provide meticulous patient management services, a gap that online consultation platforms can fill.
Online consultation platforms can make a continuous record of doctors’ consultation outcomes, which enables the platforms to monitor the quality of doctors’ consultation service. Due to the shortage of doctors in China, patients have no right to evaluate doctors in offline medical institutions. As shown in Table 2, most online health consultation platforms in China allow users to rate and evaluate doctors, and users can assess the previous evaluation and scoring records of prospective doctors. 25 By providing performance information, online evaluations reduce patient uncertainty about a prospective doctor's performance. Given that a doctor's performance requires expert evaluation, in addition to users’ evaluation, we recommend that health platforms employ professionals to monitor doctors’ responses on a regular basis. This professional assessment will also protect doctors against incorrect subjective evaluation made by patients without medical evaluation capabilities.
Screen ‘good doctors’ suitable for users
A high-rank doctor is not equivalent to being a ‘good doctor’. Our analysis showed that selecting a doctor with a higher rank meant higher consultation fees and longer wait times. China's online health consultation industry is focused on consultation for conventional diseases and management of subsequent visits for chronic diseases. Online consultation platforms can match patients with good, but not high rank, doctors, economizing on doctor fees. In the case of Dingxiang Doctor, attending physicians rather than chief physicians accounted for a majority of all online doctors in obesity consultations. By screening doctor performance, online consultation platforms can select lower-rank doctors with a history of high performance through the platform's internal assessment system. This internal assessment of online doctors can improve the matching of users and doctors, reducing users’ costs and waiting time, while ensuring the quality of medical consultation. For example, the treatment of childhood obesity places high priority on the doctor's communication skills, 26 since children and adolescents are particularly sensitive to obesity stigma. 27 Doctors suitable for children and adolescents may not be high-ranked doctors, but doctors who are qualified to respond and communicate sensitively with specific users.
Innovate reimbursements
Offline hospitals in China charge lower consultation fees than online platforms, and some offline fees can be reimbursed by China's national medical insurance schemes. Online profitable consultation platforms cannot receive medical insurance rebates. Currently, commercial insurance companies cooperate with online consultations in two ways. The first is to use online consultation as a value-added service for commercial insurance, with the insured having free access to online consultation services on designated platforms. Second, commercial insurance companies can capture patient data through cooperation with online platforms, which helps in their planning, service provisions and premium schedules. Since well-known experts charge high fees as shown in Appendix A, we recommend that online consultation platforms cooperate with commercial insurers to develop special health insurance packages, including access to well-known experts and enhanced doctor selection options.
With the increase in the overweight and obese population in China, the pressure on medical insurance rebates for online payment for overweight and obese people will increase. 28 Compared with the United States, in China, there is little insurance to cover the treatment of obesity. 29 Online consultation is a potential and effective intervention suitable for obesity, 22 and we recommend that insurance companies and online platforms cooperate to structure obesity online insurance and care packages.
Our analysis of obesity OMC in China provides new insights into the digital health industry. But we acknowledge several limitations. First, our data were collected from the OMC providers. Future studies should collect data to analyze users’ willingness to OMC choose and pay. Second, the prevalence of obesity in China and other countries may mean our results are generalizable to other diseases, but further studies of other OMC diseases are required.
Conclusion
Using four representative online consultation platforms, this paper provided the first analysis of the consultation arrangements and fee structure for obesity online consultations in China. All the OMC platforms attach importance to the application of big data search and AI response technologies, accessing doctors from tertiary hospitals, and providing fast or low-cost consultation services. Through statistical analysis of the fees charged by obesity doctors on these representative platforms, we concluded that the higher the rank of the online doctor, the higher the online fee and the longer the wait time and that online consultation fees charged by online obesity doctors were higher than those by obesity doctors in offline hospitals. Our results inform the future direction of online health consultation platforms, including expanding the use of big data and AI technology to provide low-cost, efficient consultation services; improving the online consultation experience by reducing users’ wait time and providing comprehensive patient management; supervising the quality of doctors’ online consultations; using big data technology to match users with low-rank, but high-quality, doctors; and cooperating with commercial insurance providers to provide innovative health care packages.
Footnotes
Acknowledgements
The authors would like to acknowledge their gratitude to Yunqiao Liu, Leipeng Kou, Jiangwen Li, Meiling Ren and Yue Tian for their help on data collection.
Contributorship
DY and YH were involved in the research idea, design, writing, data collection and analysis and submission. JW was involved in the research idea, design, writing and supervision. SN and EM were involved in revising critically for important intellectual content, analysis and interpretation of data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Guarantor
YH.
Appendix
Descriptive statistics of obesity doctors’ online consultation and fee arrangements.

| WeDoctor | Cases: 580 Doctors | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Doctors from Tertiary Hospitals | |||||||||
| Job Title | Observation (Proportion) | Items | Mean | Median | Mode | Variance | Minimum | Max | Observations |
| Chief Physician | 214 (35.79%) | Waiting time (within hours) | 2.72 | 2 | 1 | 3.76 | 1 | 6 | 69 |
| Graphic consultation price (RMB) | 70.78 | 50 | 30 | 5148.43 | 5 | 500 | 214 | ||
| Voice consultation price (RMB) | 104.73 | 80 | 100 | 8728.94 | 0 | 500 | 132 | ||
| Evaluation score (percentage) | 0.99 | 1 | 1 | 0.00 | 0.5 | 1 | 177 | ||
| Admission rate | 0.91 | 1 | 1 | 0.04 | 0.18 | 1 | 103 | ||
| Inquiries (cumulative) | 203.28 | 35 | 1 | 424,964.51 | 1 | 7231 | 201 | ||
| Deputy Chief Physician | 199 (33.28%) | Waiting time (within hours) | 2.64 | 2 | 1 | 3.72 | 1 | 6 | 59 |
| Graphic consultation price (RMB) | 48.64 | 30 | 30 | 3027.73 | 0 | 500 | 199 | ||
| Voice consultation price (RMB) | 81.97 | 50 | 30 | 5516.65 | 0 | 500 | 118 | ||
| Evaluation score (percentage) | 0.99 | 1 | 1 | 0.00 | 0.66 | 1 | 165 | ||
| Admission rate | 0.93 | 1 | 1 | 0.02 | 0.25 | 1 | 94 | ||
| Inquiries (cumulative) | 212.27 | 21 | 1 | 1,476,349.89 | 1 | 16,100 | 186 | ||
| Attending Physician | 114 (19.06%) | Waiting time (within hours) | 2.27 | 1.5 | 1 | 3.18 | 1 | 6 | 44 |
| Graphic consultation price (RMB) | 32.68 | 30 | 30 | 756.34 | 0 | 200 | 114 | ||
| Voice consultation price (RMB) | 49.46 | 40 | 30 | 864.00 | 0 | 159 | 72 | ||
| Evaluation score (percentage) | 0.99 | 1 | 1 | 0.00 | 0.75 | 1 | 106 | ||
| Admission rate | 0.96 | 1 | 1 | 0.01 | 0.5 | 1 | 66 | ||
| Inquiries (cumulative) | 286.29 | 26 | 1 | 807,449.39 | 1 | 5930 | 114 | ||
| Resident Physicians | 16 (2.68%) | Waiting time (within hours) | 2.00 | 2 | – | – | 2 | 2 | 1 |
| Graphic consultation price (RMB) | 17.81 | 15 | 5 | 178.03 | 5 | 50 | 16 | ||
| Voice consultation price (RMB) | 29.83 | 30 | 20 | 76.17 | 20 | 40 | 6 | ||
| Evaluation score (percentage) | 0.99 | 1 | 1 | 0.00 | 0.93 | 1 | 13 | ||
| Admission rate | 0.83 | 1 | 1 | 0.08 | 0.5 | 1 | 3 | ||
| Inquiries (cumulative) | 638.00 | 11 | 2 | 5,601,576 | 1 | 9192 | 15 | ||
|
|
|||||||||
| Chief Physician | 8 (1.34%) | Waiting time (within hours) | – | – | – | – | 0 | 0 | 0 |
| Graphic consultation price (RMB) | 52.38 | 30 | 30 | 3865.13 | 0 | 199 | 8 | ||
| Voice consultation price (RMB) | 110.00 | 50 | – | 14,800.00 | 30 | 250 | 3 | ||
| Evaluation score (percentage) | 1.00 | 1 | 1 | 0.00 | 0.97 | 1 | 8 | ||
| Admission rate | 1.00 | 1 | – | – | 1 | 1 | 1 | ||
| Inquiries (cumulative) | 105.13 | 68.5 | – | 11,292.13 | 12 | 288 | 8 | ||
| Deputy Chief Physician | 11 (1.84%) | Waiting time (within hours) | 1.75 | 2 | 2 | 0.25 | 1 | 2 | 4 |
| Graphic consultation price (RMB) | 32.73 | 30 | 30 | 81.82 | 20 | 50 | 11 | ||
| Voice consultation price (RMB) | 26.25 | 27.5 | – | 422.92 | 0 | 50 | 4 | ||
| Evaluation score (percentage) | 1.00 | 1 | 1 | 0.00 | 0.96 | 1 | 11 | ||
| Admission rate | 1.00 | 1 | 1 | 0.00 | 1 | 1 | 5 | ||
| Inquiries (cumulative) | 52.73 | 44 | – | 2350.22 | 1 | 152 | 11 | ||
| Attending Physician | 11 (1.84%) | Waiting time (within hours) | 1.00 | 1 | 1 | 0.00 | 1 | 1 | 3 |
| Graphic consultation price (RMB) | 31.67 | 30 | 30 | 137.88 | 20 | 50 | 12 | ||
| Voice consultation price (RMB) | 46.00 | 30 | 30 | 1030.00 | 20 | 100 | 5 | ||
| Evaluation score (percentage) | 1.00 | 1 | 1 | 0.00 | 0.97 | 1 | 12 | ||
| Admission rate | 1.00 | 1 | 1 | 0.00 | 1 | 1 | 6 | ||
| Inquiries (cumulative) | 183.42 | 25.5 | 5 | 142,838.99 | 2 | 1340 | 12 | ||
| Resident Physicians | 2 (0.33%) | Waiting time (within hours) | – | – | – | – | 0 | 0 | 0 |
| Graphic consultation price (RMB) | 15.00 | 15 | – | 50.00 | 10 | 20 | 2 | ||
| Voice consultation price (RMB) | 12.50 | 12.5 | – | 12.50 | 10 | 15 | 2 | ||
| Evaluation score (percentage) | 1.00 | 1 | 1 | 0.00 | 1 | 1 | 2 | ||
| Admission rate | 1.00 | 1 | – | – | 1 | 1 | 1 | ||
| Inquiries (cumulative) | 66.50 | 66.5 | – | 8064.50 | 3 | 130 | 2 | ||
|
|
|||||||||
| Attending physician | 5 (0.84%) | Waiting time (within hours) | – | 2 | – | – | 2 | 2 | 1 |
| Graphic consultation price (RMB) | 11.72 | 10 | 20 | 62.79 | 3.6 | 20 | 5 | ||
| Voice consultation price (RMB) | – | – | – | – | 0 | 0 | 0 | ||
| Evaluation score (percentage) | 0.99 | 1 | 1 | 0.00 | 0.97 | 1 | 5 | ||
| Admission rate | 1 | 1 | – | – | 1 | 1 | 1 | ||
| Inquiries (cumulative) | 45.20 | 5 | – | 4128.20 | 2 | 149 | 5 | ||
|
|
|
||||||||
|
|
|||||||||
| Chief Physician | 256 (42.95%) |
Graphic consultation price (RMB) | 102.27 | 60 | 30 | 21,189.40 | 0 | 1360 | 177 |
| Voice consultation price (RMB) | 116.07 | 94 | 150 | 11,951.65 | 1 | 799 | 142 | ||
| Evaluation score (five-point) | 3.55 | 3.6 | 3.8 | 0.10 | 2.9 | 5 | 256 | ||
| Deputy Chief Physician | 174 (29.19%) | Graphic consultation price (RMB) | 57.98 | 35 | 30 | 5094.48 | 6 | 500 | 129 |
| Voice consultation price (RMB) | 92.69 | 54.5 | 50 | 12,962.60 | 9 | 1000 | 104 | ||
| Evaluation score (five-point) | 3.35 | 3.4 | 3 | 0.11 | 2.8 | 5 | 174 | ||
| Attending Physician | 109 (18.29%) | Graphic consultation price (RMB) | 40.71 | 30 | 9 | 2007.47 | 2 | 299 | 82 |
| Voice consultation price (RMB) | 64.64 | 50 | 50 | 2536.26 | 9 | 288 | 67 | ||
| Evaluation score (five-point) | 3.21 | 3.1 | 3 | 0.09 | 2.6 | 4.7 | 108 | ||
| Resident Physicians | 19 (3.19%) | Graphic consultation price (RMB) | 15.50 | 12 | 9 | 61.39 | 9 | 30 | 10 |
| Voice consultation price (RMB) | 18.50 | 19 | 19 | 100.94 | 9 | 40 | 10 | ||
| Evaluation score (five-point) | 3.06 | 3 | 3 | 0.03 | 2.8 | 3.4 | 19 | ||
|
|
|||||||||
| Chief Physician | 3 (0.50%) | Graphic consultation price (RMB) | 41.67 | 15 | – | 2558.33 | 10 | 100 | 3 |
| Voice consultation price (RMB) | 165.00 | 165 | – | 36,450.00 | 30 | 300 | 2 | ||
| Evaluation score (five-point) | 3.20 | 3.3 | – | 0.13 | 2.8 | 3.5 | 3 | ||
| Deputy Chief Physician | 6 (1.01%) | Graphic consultation price (RMB) | 13.50 | 9 | 9 | 123.00 | 6 | 30 | 4 |
| Voice consultation price (RMB) | 19.00 | 19 | – | 100.00 | 9 | 29 | 3 | ||
| Evaluation score (five-point) | 2.87 | 2.8 | 2.7 | 0.04 | 2.7 | 3.2 | 6 | ||
| Attending Physician | 8 (1.34%) | Graphic consultation price (RMB) | 19.50 | 19.5 | – | 73.67 | 9 | 30 | 4 |
| Voice consultation price (RMB) | 29.00 | 29 | – | 162.00 | 20 | 38 | 2 | ||
| Evaluation score (five-point) | 2.75 | 2.7 | 2.6 | 0.03 | 2.6 | 3 | 8 | ||
|
|
|
||||||||
|
|
|||||||||
| Chief Physician | 11 (11.00%) | Waiting time (minutes) | 71.60 | 44.5 | 180 | 4190.27 | 12 | 180 | 10 |
| Graphic consultation price (RMB) | 81.00 | 69 | 49 | 4123.80 | 10 | 229 | 11 | ||
| Evaluation score (five-point) | 5.00 | 5 | 5 | 0.00 | 5 | 5 | 9 | ||
| Inquiries (monthly) | 21.91 | 11 | 7 | 630.09 | 1 | 81 | 11 | ||
| Deputy Chief Physician | 31 (31.00%) | Waiting time (minutes) | 68.37 | 30 | 120 | 9359.69 | 4 | 360 | 30 |
| Graphic consultation price (RMB) | 57.97 | 39 | 39 | 7018.83 | 19 | 499 | 31 | ||
| Evaluation score (five-point) | 4.92 | 5 | 5 | 0.08 | 4 | 5 | 25 | ||
| Inquiries (monthly) | 27.74 | 10 | 1 | 2912.46 | 0 | 217 | 31 | ||
| Attending Physician | 51 (51.00%) | Waiting time (minutes) | 60.46 | 30.5 | 120 | 6644.04 | 4 | 360 | 48 |
| Graphic consultation price (RMB) | 38.49 | 39 | 39 | 365.61 | 19 | 99 | 51 | ||
| Evaluation score (five-point) | 4.96 | 5 | 5 | 0.03 | 4 | 5 | 38 | ||
| Inquiries (monthly) | 22.02 | 6 | 1 | 1696.26 | 0 | 220 | 51 | ||
| Resident Physicians | 4 (4.00%) | Waiting time (minutes) | 134.00 | 107 | – | 17,405.33 | 22 | 300 | 4 |
| Graphic consultation price (RMB) | 21.50 | 19 | 19 | 25.00 | 19 | 29 | 4 | ||
| Evaluation score (five-point) | 5.00 | 5 | 5 | 0.00 | 5 | 5 | 4 | ||
| Inquiries (monthly) | 13.00 | 8 | 8 | 146.00 | 5 | 31 | 4 | ||
|
|
|||||||||
| Attending Physician | 1 (1.00%) | Waiting time (minutes) | 35 | – | – | – | – | – | – |
| Graphic consultation price (RMB) | 29 | – | – | – | – | – | – | ||
| Evaluation score (five-point) | – | – | – | – | – | – | – | ||
| Inquiries (monthly) | 4 | – | – | – | – | – | – | ||
|
|
|||||||||
| Attending Physician | 2 (2.00%) | Waiting time (minutes) | 68.5 | 68.5 | – | 5304.5 | 17 | 120 | 2 |
| Graphic consultation price (RMB) | 69.5 | 69.5 | – | 840.5 | 49 | 90 | 2 | ||
| Evaluation score (five-point) | 5 | 5 | 5 | 0 | 5 | 5 | 2 | ||
| Inquiries (monthly) | 7 | 7 | – | 8 | 5 | 9 | 2 | ||