
Abstract
Background
Perioperative messengers as tools for hospitals to communicate with patients’ loved ones during surgery have been described in form of pagers, SMS, email, and apps. The approach of combining multiple means of communication to create a secure and reliable messenger promises several advantages and has not been investigated to date.
Objective
The aim was to develop and test the technical feasibility and acceptance of a remote hybrid SMS/web-based perioperative messenger that keeps patients’ loved ones informed around the time of surgery.
Methods
Three focus groups were held with six physicians, five nurses, and 11 members of the Austrian Patient Council separately to understand their concerns and needs regarding the perioperative messenger. Their input was used to develop the perioperative messenger. Twenty-five patients and their selected loved one tested the messenger in a feasibility study. Data were collected between September 2021 and August 2023.
Results
Focus groups indicated that the most important characteristics of a messenger were transparent and prompt communication, ease-of-use, data security, and no additional workload for healthcare professionals. Our developed perioperative messenger uses SMS notifications to link to new information on a secure web platform. Participating patients were aged between 18 and 78, their loved ones between 18 and 71. Thirteen patients and 15 loved ones were female. A total of 173 messages regarding the 25 surgeries were sent, 99% of which were read on a mobile device. The median time between sending and reading surgery-related messages was 63s. All loved ones were either “fairly satisfied” or “very satisfied”.
Conclusion
The idea of a perioperative messenger was received positively by physicians, nurses, and members of the Austrian Patient Council. The developed SMS/web-based hybrid messenger system for receiving perioperative updates was shown to be feasible, and of interest and satisfaction to the loved ones.
Keywords
Background
Surgery impacts not only patients, but also all who care about the patient's well-being: immediate or extended family, partners, friends, caregivers (in this paper summarized as loved ones). Waiting times during surgery are considered among the most stressful parts of the hospitalization journey for patients’ loved ones.1–3 The literature suggests that perioperative communication decreases the anxiety felt by a patient's loved one, while simultaneously increasing satisfaction among patients and their loved ones.4–6 In a recent social media study on communication between hospitals and a patient's loved ones, perioperative messengers were discussed as a very positive form of communication strategy and given public approval. 7
The format for perioperative updates has initially evolved from their origin as in person updates in family waiting rooms to phone calls 8 and pager-based texts.5,6,9 With the growth of digital healthcare and anesthesia information management systems, 10 short message service (SMS) or email-based messaging,4,11,12 as well as digital messaging applications capable of sending text, images, and even video messages 13 have become increasingly common. Recently the most commonly implemented are SMS services and digital applications.4,11–14 SMS services are very convenient and widely used, however, SMS traffic is not encrypted and considered an insecure form of communication. 15 Although smartphone applications are highly secure, they are limited to smartphone users, and need to be downloaded onto the user's device. Furthermore, not all the systems mentioned are automated, and some necessitate manual messaging.4,12–14 This strains healthcare resources.
Relating to the World Health Organization (WHO) Classification of Digital Health Interventions, perioperative messengers tackle sections 1.4 Communication roadblocks and 1.5 Lack of access to information or data. 16 However regarding the perioperative messaging in written form, the literature only describes solutions in the United States, Canada, and Malaysia.4–6,8,9,11–13 No literature on perioperative communication with a patient's loved ones could be found for Europe. However, a recent German study notes the importance of developing tools for digital communication within hospitals. 17 Communication is especially challenging in absence of in person visits, which was seen following restricted hospital visiting policies implemented due to COVID-19 resulting in the absence of loved ones in the hospital and drastically reduced (informal) communication. 18
The WHO Global Strategy on Digital Health for 2020–2025 states that digital tools will be of high value if they increase efficiency, are easily accessible and protect the privacy of patients. 19 Furthermore, one of the WHO's seven goals as laid out in its Global Action Plan for Patient Safety 2021–2030 is to involve patients and their relatives in healthcare. 20 Open Innovation in Science (OIS) methods, in which all relevant stakeholders are involved and invited to participate, 21 can thereby be used. Following these recommendations, the aim of this study was first to collaboratively develop a perioperative messenger with nurses, physicians, patients, and their loved ones and second to test the acceptance and feasibility of this messenger in the largest tertiary hospital in Austria.
Material and methods
The methodology of this project was separated into three parts: focus groups, development, and testing. First an OIS approach discussing the idea of the perioperative messenger with the relevant user groups: physicians, nurses, and the Austrian Patient Council as representatives of the patient and loved one perspective. Second the perioperative messenger was developed based on the outcome of these discussions. Third, a feasibility study with 25 elective surgical patients and their loved ones to test the developed messenger in a clinical setting.
Focus groups with the relevant stakeholders
Three focus groups were held with the relevant stakeholders: physicians, nurses, and the Austrian Patient Council. Physicians and nurses working in an Austrian university hospital were recruited using posters and flyers distributed on various information boards within the hospital. Potential participants were also personally invited by members of the research team. To gather the patient and loved one perspective towards the perioperative messenger, the Austrian Patient Council was approached. The Austrian Patient Council is a committee of interested and committed representatives of society with experience as patients or patient's loved ones, a strong interest in health research issues and in contributing their views and opinions. Appraisal, evaluation, and idea generation are its core tasks. They are therefore well placed to voice the patient or loved one perspective regarding the perioperative messenger. The Austrian Patient Council was contacted by email. Participants were asked to register for the focus groups via the email address provided in the flyer.
The focus groups were held between September 2021 and September 2022. A total of 22 people participated in the three focus groups; six nurses in the first focus group, five physicians in the second focus group, and 11 members of the Austrian Patient Council in the third focus group. Both in the first and second focus groups, one registered participant failed to appear and gave no reason for absence.
All focus groups were led by a female qualitative researcher working at the Ludwig Boltzmann Institute Digital Health and Patient Safety with extensive experience of conducting focus groups. Those with nurses and physicians were held in person, while the focus group involving members of the Austrian Patient Council was virtual, due to some of the participants belonging to vulnerable patient groups and/or their geographical location. During each 2-h focus group, all the participants shared their views on the topics discussed. At the beginning of each focus group the reasons for conducting the research were given and the researchers introduced, together with information about their professional backgrounds. The focus group objectives were also communicated and participants invited to ask (critical) questions and share their thoughts regarding the communication between hospitals and patients’ loved ones in the perioperative setting and their opinions on a perioperative messenger (Supplemental Figure S1). The focus groups were held, transcribed, and analyzed in German. The selected quotes were translated into English for this article, with the accuracy of the translation checked by a native English speaker.
Design of the perioperative messenger
The perioperative messenger was developed together with clinical specialists and software engineers based on the feedback received from the focus groups. It was designed as a one-way system of communication. They adhered to best practices for the development of secure web applications (i.e. end-to-end encryption, mobile-first approach, modular architecture). The development of the messenger and the feasibility study were self-funded by the Ludwig Boltzmann Institute Digital Health and Patient Safety and the Medical University of Vienna.
Feasibility study
This prospective observational study took place at the Medical University of Vienna where around 15,000 surgeries are conducted annually. Feasibility testing of the perioperative messenger was conducted by the Section of Neurosurgical Anesthesia, Department of Anesthesia, Intensive Care and Pain Medicine at the Medical University of Vienna. Participants were included between July 17 and August 31, 2023. Ethics approval to include 25 elective surgery patients and their respective loved one was obtained from the Ethics Committee of the Medical University of Vienna (EK 1291/2022). Patients younger than 18 years of age were excluded from the study. Additionally, as the platform was only available in German at the time of the study, non-German speaking patients or loved ones were excluded. Recruiting started on July 17 until all 25 patients had been recruited. All the eligible patients were informed of the option of using the perioperative messenger during the anesthesia consultation routinely held via phone in the days or weeks prior to surgery. After expressing their interest, they were then called by the study team who explained in greater detail how the messenger works. After receiving the patients’ verbal consent to participate, they were issued with a personal code for registering with the messenger via email, and for forwarding to a person of their choice who would function as the recipient of the messages, who then registered to use the messenger with their own phone number. The registration process provided information about the study and obtained the loved ones’ informed consent to participate in written form.
On the day of the hospital admission, usually one day prior to surgery, the patients were visited at the ward to obtain their written informed consent. During that same visit, the patients confirmed that the registered person was indeed the loved one they wished to be informed about the course of the surgery. On the day of the surgery, status updates were sent to the registered contact via the digital messenger. For the purposes of this feasibility trial, messages were manually sent by the study personnel simultaneously to the event being documented into the routine digital anesthesia protocol by the anesthetist.
Data collection
Focus groups
All focus groups were moderated by ME, an experienced qualitative researcher working at the Ludwig Boltzmann Institute Digital Health and Patient Safety. The focus groups with physicians and nurses were held in person in a conference room at the lead research institution and were recorded by two researchers (MH and AT) who observed and transcribed the conversations. The third focus group was held online and was recorded as a video after agreement from the participants. Only the three researchers and the participants were present.
Design of the perioperative messenger
The requirements of the perioperative messenger were captured in a performance specifications list. Based on this, the messenger was developed.
Feasibility study
The web platform logged the timestamps indicating when the messages were sent, as well as every time the messages were accessed by the patient's registered loved one. The type of end device used to read the message was also recorded.
A short questionnaire was attached to the final message to obtain immediate feedback on the loved ones’ level of anxiety, satisfaction, and whether they would recommend the messenger to others or use it themselves. The survey questions were 4- or 5-step Likert Scales, with one open ended question encouraging any additional thoughts or remarks to be shared (full survey available in Supplemental Material S2).
Data analysis
Qualitative data
Qualitative data were analyzed using thematic analysis as described by Braun and Clarke. 22 Two researchers MH and AT independently analyzed the focus group transcripts and defined parts that were relevant to the development of the perioperative messenger. These were then used to identify overarching themes.
Quantitative data
Data are summarized, identifying minimum and maximum, mean with standard deviation (SD), and median and interquartile range (IQR).
Results
Focus groups
In general, all three focus groups viewed the perioperative messenger positively (Table 1). However, concerns were raised in all three groups with respect to a possible additional workload (collecting the contact details, explaining how the messenger works, sending messages) and how these tasks should not fall to the healthcare professionals. The members of the Austrian Patient Council expressed concern that patients might receive less attention if physicians were occupied with manually sending the messages. Both they and the physicians recommended the use of an automatic messaging system integrated into existing digital protocols. There was consensus that no surgery-specific messages should or could be communicated as the system should be applicable to patients undergoing a broad range of surgeries, while arrival at and departure from the operating theatre are events common to all patients. The Austrian Patient Council members stated that the worst-case scenario would be a system failure, leading to a disruption in communication with the patient's loved one, followed by a failure to subsequently inform the contact in person in the event of major complications. Nurses and physicians suggested there should be someone to contact for support with technical problems, and for patients or their loved ones to reach should they have any questions.
Perioperative messenger capabilities required by nurses, physicians, and members of the Austrian Patient Council.

Design of the perioperative messenger
Based on the input of the focus groups, design principles were identified and appropriate messenger features were mapped out (Table 2). The resulting perioperative messenger is a secure web application designed to keep patients’ selected loved ones informed about the status of their surgery. All data are stored on a secure server; loved ones are notified about new messages via a standardized SMS which they can read in a web-based app accessed via their smartphone, tablet, or computer, using their personal access credentials. The study personnel establishes trust with the patients and provides detailed information on how the messenger works and the information which can be expected to be provided during surgery. For the purpose of this study and to test the feasibility, the messenger was designed for manual operation, with additional study personnel tasked with sending the messages. In case of an integration of the messenger into the hospital information system this would be done automatically.
Design principles and the derived messenger features.

Security and privacy
The messenger structure is based on SMS notifications linking to new information on the secure web platform which is hosted on hospital premises (Figure 1). The SMS does not include personalized health information (such as patient name or patient's status) to comply with the European general data protection regulation (GDPR). Therefore, the platform was designed to combine the advantages of SMS with those of an end-to-end encrypted web-based platform, removing the need for an additional medium such as an app that would require downloading, maintenance, and updates.
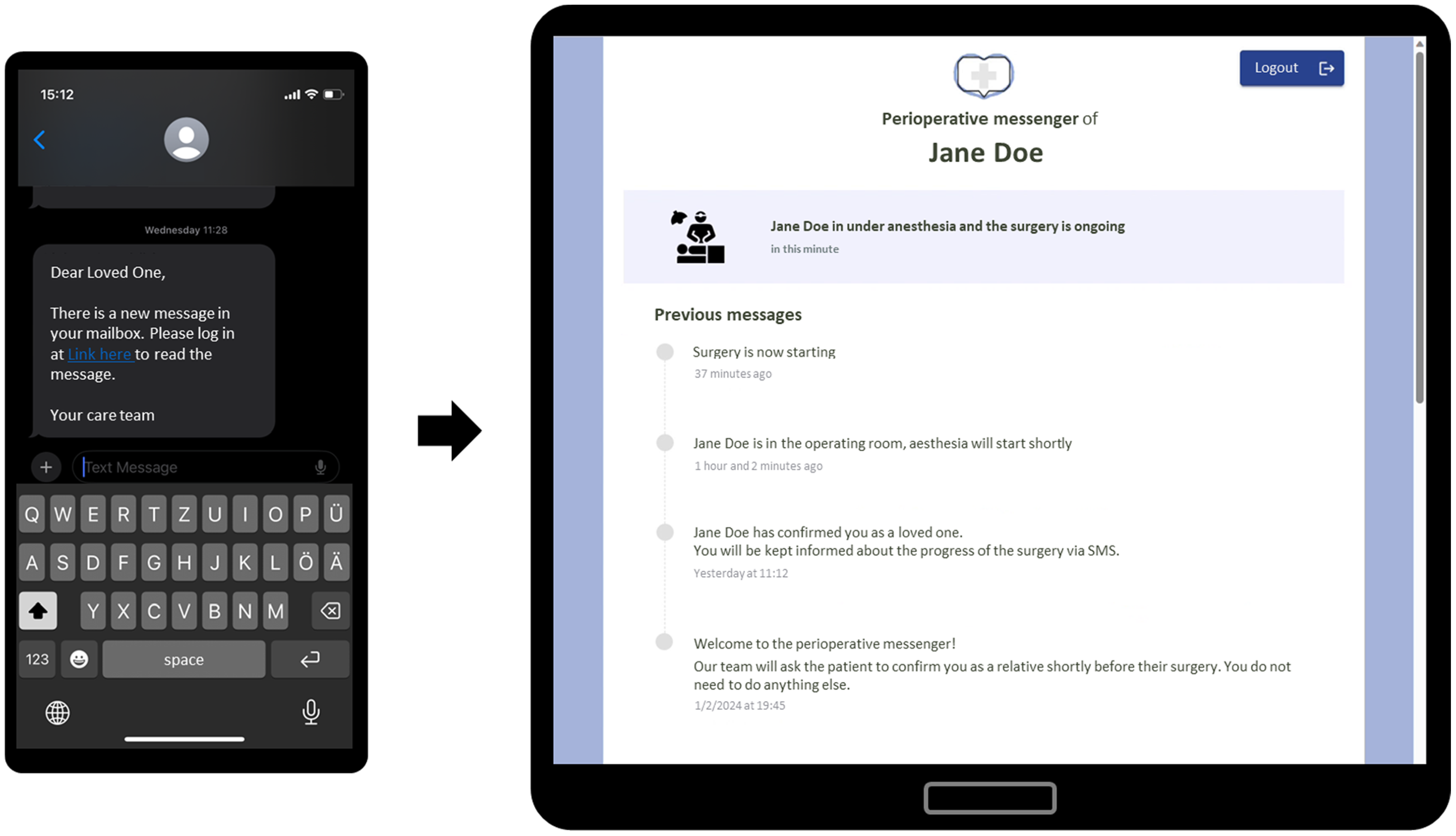
The hybrid SMS/web-based perioperative messenger allows for low-barrier notifications via SMS and secure information access via the web platform (screenshot of our developed perioperative messenger, translated into English for this publication).
Information about the status of the patient's surgery is sent to a selected loved one, who, according to Europe's GDPR, does not have the right to access the data. However, they may be granted access by the patient who has the right to manage access to their own data. Consequently, consent is obtained twice: (1) the patient provides their loved ones with the code and (2) additionally confirms the loved one's data at hospital admission.
Functionality
The workflow of the perioperative messenger has been designed so that the patient and their selected loved one are responsible for organizing and entering their own data. Hospital personnel are tasked only with providing the patient with the access code, and asking the patient to confirm or reject the registered loved one (Figure 2).
The patient receives a registration code for the loved one via email. They share this code with the person they wish to be informed of the progress of their surgery. The chosen loved one registers using the access code. First name, last name, and date of birth are entered to allow later verification by the patient. The phone number and password are used as platform login details to access messages. The phone number is verified via SMS. Once the phone number has been verified, a welcome message (Message 1, Table 3) can be seen on the platform. To check the correct contact person has registered, the patient is asked to confirm (or reject) the registered loved one (using first name, last name, and date of birth) on the day of hospital admission. Message 2 will be dispatched to the loved one to inform them that the messenger is now active. Their login credentials (phone number and password) are required to read the messages. On the day of surgery, messages about the operation are sent to the confirmed loved one. Each new message triggers a SMS notification to the nominated loved one indicating that there is a new message on the platform. To read the message content, the loved one must log into the platform.

Workflow of the hybrid SMS/web-based perioperative messenger.
Messages sent by the developed perioperative messenger.
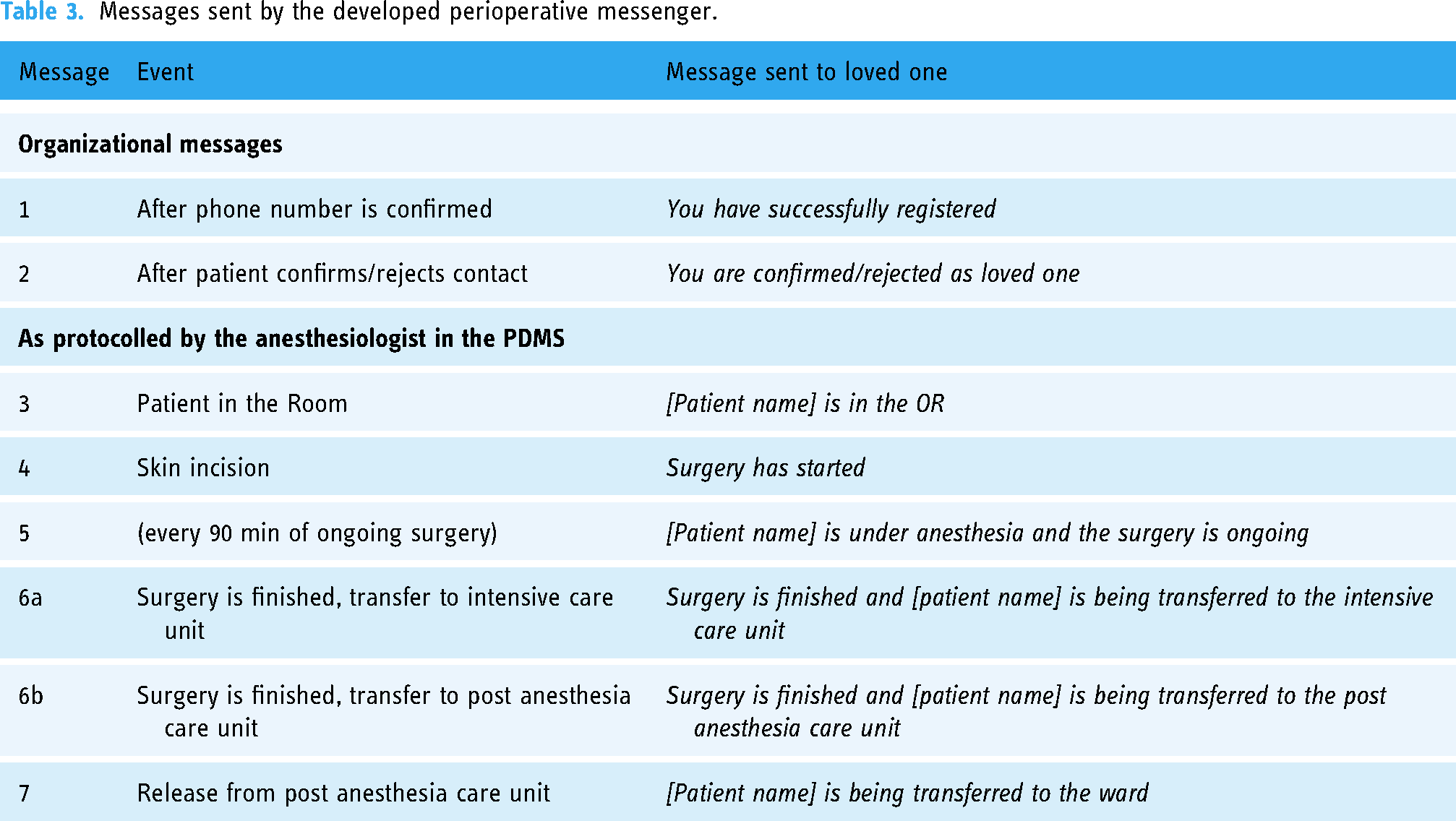
The messages are personalized from Message 2 onwards, using the patient's first and last name for to create a more personalized experience. The messages were designed to be applicable to different surgical settings and state only the status of the patient in the perioperative journey, do not include information about the actual status of the procedure itself, and do not require any additional input from the surgeon. If complications should arise, the surgical team would contact the loved one directly via phone call.
Feasibility study
Participants
Of 36 eligible patients, 27 (75.0%) showed an interest and 25 (69.4%) agreed to participate in the study (Figure 3). Reasons for non-participation were lack of interest from the patient (n = 6), no loved one with time or interest in receiving the messages (n = 3), absence of loved ones (n = 1), and the selected loved one lacking the necessary digital know-how (n = 1). The 25 loved ones selected by the patients all agreed to participate in the study.
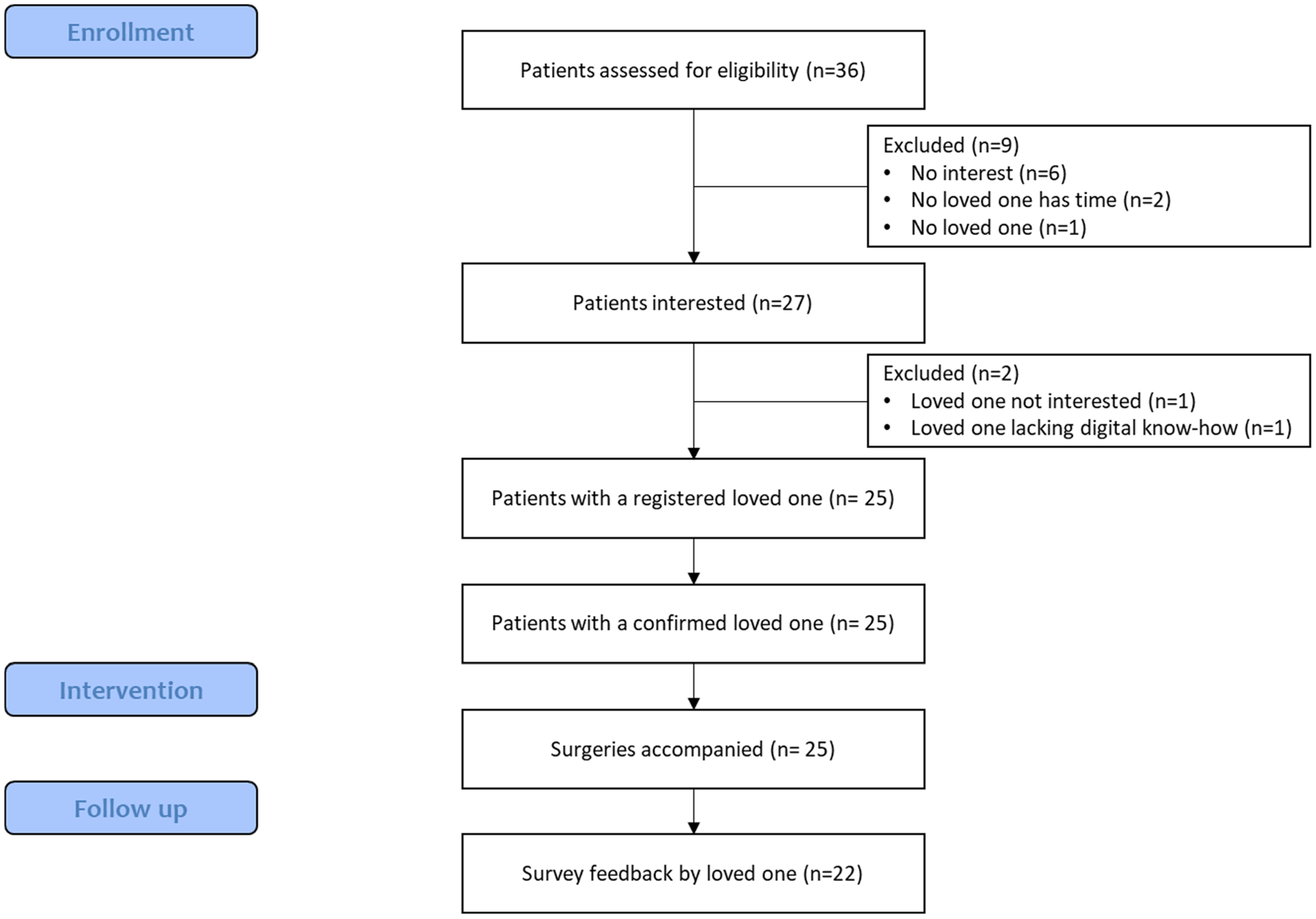
Flow diagram of participant enrollment.
Patient and loved one demographics are outlined in Table 4. The mean age of the patients was 48.5 ± 16.5 years (min: 18 years, max: 79 years), 13 participants (52%) were male, and 13 participants (52%) chose their spouse or partner as their loved one. The loved ones were 46.5 ± 12.5 years old (min: 18 years, max: 71 years), 60% were female. Spinal neurosurgeries were the most common type of surgery (32%). On average, the surgeries lasted 3 h and 51 min ± 1 h and 59 min.
Characteristics of patients, loved ones, and surgeries (n = 25).

Perioperative messaging
A total of 173 messages relating to the 25 surgeries were sent, and 728 accesses to read these messages were logged. New messages were available in 160 accesses, and in ten of these more than one new message was available. The median time between a message being sent and then read was 63 s (19 s–13 min 27 s) for all surgical messages (Supplemental Table S3). The fastest messages to be read were those communicating the end of surgery, both when transferred to the intensive care unit (ICU) or post anesthesia care unit (PACU) (Figure 4, Supplemental Figure S4). 99% (158/160) of new messages were accessed via a mobile device, and only 1% (2/160) via a desktop device. These two accesses were made during registration, whereas all messages relating to the surgery itself were read on a smartphone. A few loved ones had reading latencies of an hour or more for at least one of the messages (5/25), while many (9/25) loved ones read all messages within seconds to minutes of arrival (Supplemental Figure S4).

Time between study personnel sending and loved one reading the messages, stratified by message type and duration. Boxplots represent median and interquartile range.
Immediate post-surgical feedback from loved ones
Loved ones’ feedback was positive. The survey was completed by 22 of 25 participating loved ones (88%). While some (3/22) stated that receiving messages made them rather nervous, all were satisfied with the messenger itself, would be likely to recommend the messenger to others, and to use the messenger if they had surgery themselves (Figure 5).

Questionnaire feedback provided by loved ones after receiving the final message.
The open-ended question encouraging feedback, comments, or suggestions for improvement was answered by 7 of the 22 respondents (32%). The comments were clustered onto four categories and included positive feedback, desire for more information, negative feedback, and software error (Table 5).
Responses provided by loved ones to the survey question: “Do you have any feedback, comments or suggestions for improving HeRo and about your experience with using the messenger?”

Discussion
In the present study, we obtained the needs and wishes of relevant stakeholders: physicians, nurses, and the Austrian Patient Council, serving as the voice of patients and their loved ones. Based on their input, we developed the perioperative messenger which uses a hybrid SMS/web-based system as the loved ones’ key to perioperative updates on the patient's surgical journey. In a feasibility study, we demonstrate that such a hybrid system is not only feasible but also accepted by real-world patients and loved ones.
In addition to demonstrating interest, feasibility, and acceptance, our study revealed three important observations for clinical practice. Firstly, patients were very interested in using the service. Secondly, most messages were read within seconds to minutes of arrival, indicating their relevance to the patient's nominated contact and the system's ease of use. Finally, most nominated contacts reported the messages having a calming effect, while all participants stated that they would recommend the messenger to their loved ones and use it if they ever had surgery.
Inclusion of relevant stakeholders
To the best of our knowledge, this study is the first to describe a perioperative messenger developed with the involvement of all relevant stakeholder perspectives: physicians, nurses, patients, and loved ones. As digital tools should be developed in a way that they increase efficiency, it is imperative to involve the people who will be using these tools in their design.23,24 The focus groups highlighted several areas for consideration: which messages can be expected needs to be explained beforehand to the patients and loved ones, technical support should be available to all users, and all focus groups agreed that use of the system should not add to the workload of hospital personnel (Table 1). The members of the Austrian Patient Council stressed that not specific information on the surgery but rather general information on the status of the patient and outcome of surgery is relevant to them. During development of the perioperative messenger, the use of audiovisual messages, such as done by Hodge et al., 13 therefore seemed superfluous. The clinical feasibility study confirmed that some loved ones wish for a personal update regarding the outcome of the surgery (Table 5), meaning that a messenger in its optimal form requires active input from the physicians.
Technical and organizational aspects
All the messages were read by the loved ones, most within minutes of being sent, suggesting the hybrid nature of the messenger (SMS messaging and a web platform) appears to have been well accepted by both the patients and loved ones. Direct feedback from the loved ones included gratitude for the opportunity to use the messenger, and praise for its ease of use (Table 5). The messenger design favors smartphone use, and our results show that all messages on surgical updates were first read on mobile devices. In Austria, 88% of the population were using smartphones by 2021. Among the older population, however, and especially those over 65 years of age, this figure was only slightly over 50% in 2020.25,26 Although some study participants (both patients and loved ones) were over 65, of those patients who declined to participate in the study, only one stated that they felt overwhelmed by the digital nature of the solution and would use it only if they received SMS notifications. This suggests that while this hybrid approach might benefit many age cohorts, challenges in the older generations remain.
The messenger described here is the first to use a hybrid SMS/web-based messaging service in comparison to the other already published ones.4–6,9,11–14 The messenger from Canada uses a SMS service integrated into the hospital system 11 ; the messengers from the US use either pagers,5,6,9 an app 13 or are web based with SMS and email for updates 4 ; in Malaysia, SMS are sent directly by the staff.12,14 However from the data privacy and security aspect, the benefits of SMS being widely available and also accessible to non-smartphone users are offset by a recognized security problem15,27: SMS messages are not encrypted, and studies have shown that messages can easily be intercepted.27,28 The hybrid approach of integrating SMS notifications and a digital platform in our perioperative messenger system combines the strengths of each communication medium, while mitigating their respective limitations.
As well as its hybrid nature, our perioperative messenger differs from those already described4,6,11–14 in another important aspect: the process of registering loved ones is entirely remote. Most existing messengers require the in-person sign up of loved ones on the day of the surgery as they are designed for loved ones who are nevertheless waiting in the hospital during surgery or are at least present during the patient sign up.6,11–14 Only Gordon et al. 4 describes the registration of the loved ones in advance, namely on site by the patient when the decision on elective surgery is made with the physician. Our registration process was remote via phone call and email, with only the verification step taking place in the hospital. Alternative sign up methods would be directly during or after the surgeon consult or by sending a registration link to the patient's phone number. Unlike in the US and Canada, surgery waiting rooms for patients’ loved ones are not provided as standard in European hospitals. Therefore, it is important that the digital solution is readily available to loved ones irrespective of whether they can be physically present in the hospital, which was also mentioned in the focus groups (Table 1).
Users and experiences
Patients and loved ones of different ages and genders took part in the feasibility study. The gender distribution among patients was balanced, while a slightly higher proportion of the loved ones was female. The patient participation rate was 69%. Despite the small sample, this appears to generally reflect levels of interest in the messenger as a study on the implementation of SMS-based perioperative messengers for 8129 surgeries in Canada determined a 75.6% participation rate among the loved ones. 11 In our study, patients predominantly chose immediate family members as message recipients, although some chose friends or other contacts (Table 4). They received 173 messages in total. The messenger however logged 728 accesses, which seems to be artificially inflated by some web browsers of the loved ones which send repeated requests within seconds to load page elements or refresh content. Therefore, the frequent accesses should not be interpreted as anxious behavior; more reliable data regarding anxiety are the questionnaire filled out by the loved ones after receiving the last message. The majority of the loved ones reported that having access to the messenger had a calming effect, while some reported that the very fact of receiving messages made them more anxious. However, all loved ones reported being “fairly satisfied” to “very satisfied” with the messenger (Figure 5). Loved ones receiving intraoperative messages have already been shown to experience lower levels of anxiety and higher levels of satisfaction compared to those receiving no messages.5,11,13 A significant reduction in anxiety is reported 1 h after commencement of surgery and immediately after completion of surgery, but not one day prior or one day after the surgery. 12 Our data indicate how quickly the messages were read, with the median time between sending and reading of 63 s.
Possible further development
Of all the messengers described thus far,4–6,9,11–14 the SMS messenger described by Mignault et al. 11 from Canada and the pager messenger from the US described by Wieck et al. 6 are the only ones integrated into the hospital system, whereby the messenger by Wieck et al. still needs to be manually operated by the healthcare personnel. The next step in the development of the messenger described here is the integration into the hospital system, including linkage with the digital anesthesia protocol. Once implemented, the manual process of sending messages should then be replaced by automated functionality integrated with these protocols. Thereby, the surgical and anesthesia team will be relieved of any additional work. Additionally, a special functionality will need to be developed for the case when surgery is not proceeding as planned. Our current solution on communicating bad news was by phone call. Of the two messengers integrated into the hospital system, Wieck et al. 6 solve this by allowing a free-text box while Mignault et al. 11 do not state an exit scenario. This free text box could be used to contact the loved ones if the procedure is not going as planned. By using this field, the messenger will disconnect from the anesthesia protocol. At the end of the procedure, a free text box could also be used for the surgeon to give a personal update on the outcome of the procedure, a wish expressed by the Austrian Patient Council (Table 1) and loved ones (Table 5). The content and effect of such messages on the loved ones would be interesting to explore in a follow-up study. To cover all possible scenarios in a perioperative journey, the messenger could also be extended to the ICU setting, as some patients are transferred to the ICU for postoperative monitoring. As demonstrated by Gorman et al., 29 messages such as ICU admission, extubation, morning rounds, decision to discharge, and discharge from the ICU could all be sent. However, a similar setup to the study we present—focus groups with patients, loved ones, nurses, and physicians regarding the content of the messages, followed by an observational study—could be conducted.
Until now, all messengers have been described for elective surgeries,4–6,9,11–14 with the target patients being children,6,13,14 adults,4,5,9 both, 12 or not stated. 11 However their use in non-elective, emergency surgery could be of equal or even higher relevance to the loved ones since those times can be even more stressful and anxiety inducing as planned procedures. In such contexts, patients may lack the capacity to provide informed consent for the sharing of their medical data via digital platforms, whether due to unconsciousness, mental impairment, or other factors. Outside the emergency setting, mentally impaired patients have legally authorized representatives who can make decisions on their behalf. However, in emergency settings, doctors often use the doctrine of implied consent. In further studies it would be of high interest to explore whether the doctrine of implied consent could also be applied to sharing data via digital platforms with patients’ loved ones during medical emergencies.
It is often the case that patients and their loved ones are not familiar with the day-to-day workings of a hospital where schedules can quickly change. In the feasibility study, a loved one stated that they were unsure whether the message timestamps were correct (Table 5). Therefore, as suggested by the nurses in the focus group, in order to manage expectations amongst the loved ones, patients and their loved ones should not only be educated about the information they will receive via the messenger, but also about the perioperative process itself. With regards to the messages, studies show that informative and instructional SMS are associated with higher patient engagement.30,31 Additionally, automated SMS text messaging services designed to support adult patients or parents (caregivers) in preparation for surgery are positively accepted32–34 and can even decrease full time hospitalization in cases where an outpatient procedure was planned. 35 However, the perioperative pathway is not the only scenario in which patients and loved ones can feel left out in terms of organization and preparation: patients and their loved ones expressed a wish for greater support throughout the entire healthcare journey. 7 A perioperative web-based platform can offer a secure and reliable environment for patients and their loved ones empowering them to take an active role in the patient's care and preparation for surgery while also serving as a valuable reference resource throughout the perioperative journey. 36 However, for digital solutions to be accepted, hospital care team members must be included in development and provided with ample training opportunities to foster acceptance of such solutions. 37
Lastly, the messenger was only available in German for the purposes of feasibility testing. However, support for multiple languages was an important concern that was raised within focus groups. Having only a single language available excludes vulnerable groups of patients and loved ones with language barriers. This is particularly problematic because this group is already at greater risk when it comes to navigating the hospital system and communicating with healthcare professionals, as interpreters are not always available.38,39 The use of standardized messages presents an opportunity to offer a digital communication tool relaying (perioperative) information in multiple languages. Decreasing language barriers in hospitals would increase the involvement of loved ones in hospital and care developments. 40
Limitations
A limitation of this study is the positive selection bias for the participants, both in the focus groups and the feasibility study. The sample size of the focus groups was rather small, and while this allowed for more personal and in-depth discussions, together with the positive selection bias it limits the ability to generalize in terms of the attitudes and needs expressed. Nevertheless, the information provided was very helpful in guiding the development of the messenger. The sample size for the feasibility study was also small and only patients from a specific surgical area were included. It was conducted in a semi-isolated setting because the study personnel were those tasked with recruiting the participants and sending the messages. However, this should not have impacted the experience of patients and their loved ones around the day of the surgery. Testing of the messenger in its automated form in various surgical settings is now needed for the findings to allow for generalizability.
Conclusion
We have developed a hybrid SMS/web-based perioperative messenger with the relevant stakeholders: patients and loved ones, nurses, and physicians. The developed messenger is a web platform which sends notifications of new messages via SMS, loved ones however need to log into the platform to read the content of the message. Thereby, our solution upholds the necessary privacy and security standards while being very user friendly by utilizing SMS as the most common notification method. The remote registration of loved ones reduces the workload for the healthcare personnel limiting it to only the verification of the registered loved one. Our results show the high importance of the messages to the loved ones during the time of surgery with the fast reading times of the messages, which were almost exclusively done on mobile devices. Loved ones were satisfied with the messenger. The current limitation of the messenger is that messages can only be sent manually. However, the messenger has been designed with consideration of the digital anesthesia protocol and the steps routinely protocolled there by the anesthetist; in the next step, the messenger can be linked to the anesthesia protocol and the messages sent automatically.
Adopting perioperative messengers into clinical routine holds the potential to streamline communication between hospitals and patients’ loved ones and improve patient and loved one satisfaction.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241288760 - Supplemental material for Development and testing of a remote hybrid SMS/web-based perioperative messenger: A mixed-methods study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241288760 for Development and testing of a remote hybrid SMS/web-based perioperative messenger: A mixed-methods study by Mojca Hriberšek, Daniel Laxar, Fabian Peter Hammerle, Stefan Ulbing, Anna Teufel, Stefan Bartos, Nikola Gauß, Martin Niederle, Oliver Kimberger and Eva Schaden in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241288760 - Supplemental material for Development and testing of a remote hybrid SMS/web-based perioperative messenger: A mixed-methods study
Supplemental material, sj-docx-2-dhj-10.1177_20552076241288760 for Development and testing of a remote hybrid SMS/web-based perioperative messenger: A mixed-methods study by Mojca Hriberšek, Daniel Laxar, Fabian Peter Hammerle, Stefan Ulbing, Anna Teufel, Stefan Bartos, Nikola Gauß, Martin Niederle, Oliver Kimberger and Eva Schaden in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241288760 - Supplemental material for Development and testing of a remote hybrid SMS/web-based perioperative messenger: A mixed-methods study
Supplemental material, sj-docx-3-dhj-10.1177_20552076241288760 for Development and testing of a remote hybrid SMS/web-based perioperative messenger: A mixed-methods study by Mojca Hriberšek, Daniel Laxar, Fabian Peter Hammerle, Stefan Ulbing, Anna Teufel, Stefan Bartos, Nikola Gauß, Martin Niederle, Oliver Kimberger and Eva Schaden in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors are grateful to Magdalena Eitenberger, Ludwig Boltzmann Institute Digital Health and Patient Safety, for her methodological input, leadership, and feedback regarding the focus groups.
Contributorship
The work was conceptualized by MH and ES. The methodology and research were conducted by MH, DL, FPH, SU, AT, SB, NG, MN, OK, and ES. Formal analyses were carried out by MH and DL. The original draft was written by MH. The final manuscript was reviewed and edited by DL, FPH, SU, AT, SB, NG, MN, OK, and ES. All authors have read and agreed to the published version of the manuscript.
Data availability
The data sets generated during and/or analyzed during this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Ethics Committee of the Medical University of Vienna approved the focus groups (EK 2079/2020) on 23 October 2020 and the feasibility study (EK 1291/2022) on 23 February 2023.
Funding
The authors received no external financial support for the research, authorship, and/or publication of this article.
Guarantor
MH.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.