
Abstract
Background
The Inpatient Telehealth Program permits family to remotely communicate with the patient and care team through secure, live video. We aimed to assess the implementation of this program for family engagement from the perspectives of patients, families, and providers.
Methods
We used a convergent mixed methods design. The quantitative component was a cross-sectional analysis of surveys assessing patient, family, and provider experience. The qualitative component used thematic analysis of patient, family, and provider interviews plus survey free text responses. We performed memo-writing and coding. We developed hypotheses about relationships among categories and identified analytic themes. We used data transformation and narrative discussion to report the integrated findings.
Results
Surveys from 214 individuals (33 patients, 145 family, 36 providers) were evaluated. Mean (standard deviation) experience ratings (1-poor, 5-best) were 4.0 (1.5) for patients, 4.6 (0.8) for family, and 4.0 (1.4) for providers. We received 134 free text responses and conducted 21 interviews. Three themes emerged: (1) inpatient telehealth enhanced patient and family experience through strengthened relationships and increased support; (2) inpatient telehealth enhanced patient care through improved information sharing and engagement; (3) low awareness of the program limited adoption. Quantitative and qualitative data aligned in that participants perceived inpatient telehealth to be valuable; however, surveys revealed that patients and providers have relatively lower satisfaction with the program.
Conclusion
Inpatient telehealth for family engagement was perceived to improve family-centeredness of care. Future work is needed to overcome implementation challenges and to increase awareness of this resource among patients and families.
Background
Family-centered care is a health care delivery approach that recognizes the collaborative partnership among patients, families, and health care providers. The Institute for Patient and Family-Centered Care defines core principles of family-centered care to include respect and dignity, information sharing, shared decision-making, and collaboration. 1 Family-centered care is recognized to improve patient self-management, improved family experience, decreased rates of harmful errors, and reduced length of hospitalization.2–4 For these reasons, family-centered care is recognized as a health care standard by multiple healthcare societies, legislative bodies, and the National Academy of Medicine.5,6
Unfortunately, not all patients and families experience care delivery that is family-centered. Families with low income, public insurance, and from racial and ethnic minority backgrounds are less likely to receive family-reported family-centered care. 7 Family members of minority races report more instances of experienced or observed discrimination.8,9 Also, during a hospitalization, family members of the patient who have a language preference other than English are more likely to report poor satisfaction, lack of knowledge of care plans, and poor family-centered care.10–13
The hospital setting presents unique challenges to experiencing family-centered care. Information sharing, engagement, and shared decision-making with family members of hospitalized patients is often limited due to barriers that prevent family from being physically present in the hospital to communicate with the care team and participate in patient care. Identified barriers include schedule conflicts, other cargiving responsibilities, living far from the hospital, lack of transportation, and high travel costs.14,15
Utilizing telehealth for hospitalized patients is a promising strategy to promote family-centered care. Telehealth permits family members to communicate with the patient and health care team through secure, live video. In this way, telehealth overcomes some barriers by making it easier to share information, support, and collaborate with the patient and family. Importantly, telehealth use facilitates the family-centered aspects that are most important to families: availability, accessibility, and communication. 16 The use of telehealth cannot overcome all factors resulting in non-family-centered care experiences; however, telehealth offers families a resource that can potentially strengthen family-provider communication, trust, and collaboration.
Our hospital implemented an internal inpatient telehealth service line referred to as the “Inpatient Telehealth Program.” This hospital-wide program includes use of telehealth to virtually bring care team providers and family members to the bedside. Although the use of telehealth for hospitalized patients was rapidly adopted across the nation in the setting of the novel coronavirus (COVID-19) pandemic,17–19 research is needed to evaluate these clinical interventions. 20 Furthermore, prior telehealth research has identified threats to longerm sustainability of such programs and highlighted the critical need for further research that focuses on implementation. 21
Qualitative and mixed methods are valuable approaches to understanding implementation outcomes, including intervention feasibility, acceptability, appropriateness, adoption, and sustainability. 22 The Medical Research Council process evaluation framework provides a structured approach to evaluate implementation and outcomes in real-world context. 23 Medical Research Council domains include implementation, mechanisms of impact, and context. Based on existing literature on family-centered care, relevant outcomes to explore mechanisms of impact include information sharing, empowerment, collaboration, and support.16,24–26 We thus employed a mixed methods approach, applying the Medical Research Council framework, to evaluate the Inpatient Telehealth Program. Specifically, we aimed to assess the implementation of the Inpatient Telehealth Program for family engagement of hospitalized patients from the perspectives of patients, families, and care team providers.
Methods
Study design and setting
We conducted a mixed method study using a convergent design to examine the Inpatient Telehealth Program. Data were collected from December 2020 to October 2022. During this timeframe, the program had 372 family engagement encounters. The quantitative component was a cross-sectional analysis of a patient, family, and provider experience survey. The qualitative component was a qualitative descriptive study using thematic analysis of patient, family, and provider interviews plus free text responses from the surveys. We integrated the data using data transformation to convert the quantitative data into qualitative data.
This study was conducted at a 646-bed quaternary care hospital in Northern California. This hospital is the referral center for children and adults across a 33-county region covering 65,000 square miles. Telehealth services have been available at our center since 1992. Telehealth service lines have expanded over recent decades to encompass outpatient general and specialty care, urgent care, remote patient management, e-consults, external inpatient specialty care, and internal inpatient care.
The Inpatient Telehealth Program, an internal inpatient care service and one of our center's recently introduced telehealth offerings, was designed and implemented in May of 2020. This program was developed at the request of the health system during COVID-19 shelter-in-place orders as a service to simultaneously support clinical needs and patient and family needs. It was implemented across every unit in the hospital so that every patient, regardless of clinical service or location, could benefit from this resource. The decision to use the Inpatient Telehealth Program was at the discretion of the care team providers. In-person and virtual trainings were offered by the Health Information Technology Education Department to providers on every unit; most trainings were conducted for unit-based groups of nurse managers and bedside nurses.
We initially used Zoom (San Jose, CA) as the software interface for the program. We added ExtendedCare (Chicago, IL) as our preferred platform in January of 2021; we continued to support the use of Zoom as a secondary platform option during this study. Family members download Zoom or ExtendedCare onto their personal computer or smart device. The hospital care team uses Zoom or ExtendedCare on a tablet or computer with a speaker and microphone, which is mounted on a stand with wheels. Inpatient telehealth can be used 24/7. Care team providers such as bedside nurses or unit clerks inform patients and families of the opportunity to use telehealth for family engagement. Inpatient telehealth is also advertised on the health system's website with instructions and a 24/7 helpdesk number.
Study population and data collection
Surveys
Survey data were collected from patients, family members, and providers from December 2020 to October 2022. This survey was designed and administered by the Information Technology Department; it was not evaluated for validity evidence prior to use in this study. Upon ending an Inpatient Telehealth Program encounter, a pop-up box invited users to rate their experience. Survey questions are provided in Supplement 1 and included: (1) Rate your experience using this visitation technology (1–5 stars), (2) Was the goal of your video visitation met? (Yes/No), (3) Would you use this technology in a hospital setting again? (Yes/No), (4) Rate your audio connection (1–5 stars), (5) Rate your video connection (1–5 stars), (6) Provide any other comments about this technology use (free text).
Interviews
We conducted one-on-one semi-structured interviews with patients, family members, and providers between January and October 2021. Participants had to have English proficiency and be aged 18 years and older. We recruited participants who had used inpatient telehealth for family engagement at least once within one month of recruitment. We initially used convenience sampling, whereby participants were identified by recommendation from providers and from the Inpatient Telehealth Activity Report. We subsequently used purposeful sampling and recruited participants with no experience using the Inpatient Telehealth Program to understand the reasons for not using the program and explore emerging insights regarding program reach. We also hoped to gain insights into how perceptions and experiences might vary under the different condition of no program use. For the latter third of the interviews, we used maximum variation sampling to identify participants with varied use of the Inpatient Telehealth Program and to achieve diversity among participants regarding gender, race, ethnicity, and role. Participants were recruited in-person or by email. Interviews were conducted either in-person in a private location at the hosptial or by videoconference, per participant preference. Sampling continued until we reached thematic saturation. 27
The interviewer (J.W.) was a research assistant with qualitative research expertise; they had no prior relationship with participants prior to the study. They used a question guide that solicited participants’ general perceptions about the program, perceived benefits and harms, usage, facilitators and barriers to adoption, mechanisms of impact, and strategies for optimizing the program. Participants provided verbal informed consent and received a $50 gift card. Interviews were audio recorded, transcribed verbatim, deidentified, and reviewed for accuracy by the interviewer.
Analysis
We analyzed the five quantitative survey items using descriptive statistics. We calculated proportions and means with standard deviations; we examined data by respondant type (patient, family, and provider). For qualitative data, we used thematic analysis27,28 with application of some principles from Grounded Theory, specifically constant comparison, theoretical sampling, and memo-writing.29,30 Our analysis team consisted of four researchers, including a medical student (K.B.), a clinical research coordinator (J.W.), a physician telehealth researcher (J.R.), and a nurse scientist (L.K.).
Qualitative data were analyzed concurrently with data collection. Data were examined iteratively using a framework analysis of concepts pertaining to the Medical Research Council process evaluation framework. 23 Our initial codebook (Supplement 2) included the Medical Research Council domains (implementation, mechanisms of impact, context) merged with variables from existing literature on family-centered care.16,24–26
Three researchers (J.W., J.R., L.K.) used the initial transcript to independently perform analytic memo-writing and coding using a priori codes while identifying emergent codes with open coding. We met to discuss the relevance and definitions of the coding structure and new topics from inductive coding. Subsequently, the researchers independently memoed and coded 1–3 transcripts and then met to discuss memos and application of codes, refine dimensions of existing codes, add new codes, develop tentative concepts using constant comparisons, examine data for patterns and variations, and revise the interview guide. This process was repeated with every 1–3 transcripts.
We developed tentative hypotheses about relationships among categories, revisited prior transcripts in search for negative and qualifying evidence, and identified theoretical direction. We diagramed by drafting a causal network to note the relationships between variables. We created a participants’ role-ordered matrix to explore how the variables related to participants’ role types (i.e., patient, family, nurse, physician, and clerk). Free text responses from surveys were incorporated into the matrix. Recurrent unifying concepts and identified linkages and patterns between the categories became analytic themes. We used ATLAS.ti to organize and store coding and data analysis. 31
This study was approved by the University of California Davis Institutional Review Board. This study had a waiver of the requirements for a signed consent form. The research only involved minimal risk. The level of involvement of the participants was at their own discretion. The beginning of each interview began with an introduction that included reviewing a script with consent elements. The interview only proceeds following verbal consent. For the quantitative data, the study used existing data that were collected for the purposes of clinical services. The risk of loss of confidentiality was minimized by deidentifying the data. The research could not alter the clinical treatment of patients, because data were analyzed after the clinical care was completed.
Integration
To compare the results of the quantitative and qualitative data, we used data transformation. We converted the quantitative data into qualitative data. Rationale for transforming in the direction of quantitative-into-qualitative data was to enrich the analyses that were informed by the Medical Research Council process evaluation framework. 23 We identified to what extent and in what ways the two sets of results converged, diverged, or related to each other. We used a narrative discussion to report our integrated findings. 32 We used the integrated results to create a logic model of the relationships among the Inpatient Telehealth Program's activities and outcomes (Figure 1).
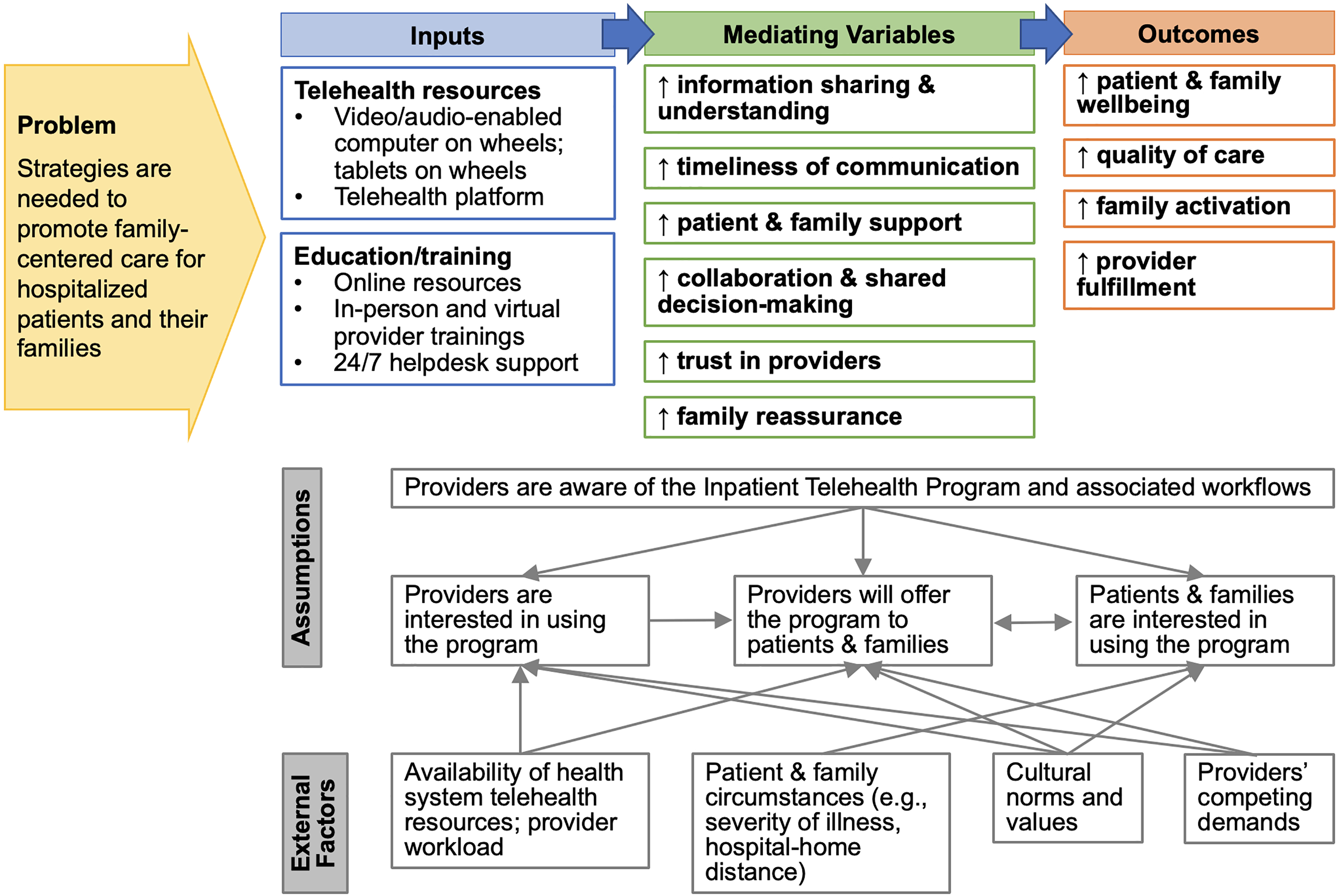
Logic model of the relationships among the inpatient telehealth program and its outcomes. Legend: ↑– increases or improvements. ↓ – decreases or reductions. Inputs include inpatient telehealth program components.
Results
Among the 372 family engagement encounters for the Inpatient Telehealth Program, 214 individuals completed the optional survey. Survey respondants consisted of 33 patients, 145 family members, and 36 providers. Survey results are presented in Table 1. The below sections present the transformed survey data and integrated results in passage format organized by theme.
Inpatient telehealth user experience survey results.

SD, standard deviation.
Response option: 1 to 5 stars.
We received 134 free text responses from surveys and conducted a total of 21 interviews. We interviewed 1 patient, 4 family members, 10 nurses, 3 physicians, and 3 hospital clerks. Two of the family members had not used the Inpatient Telehealth Program; they stated that they were unaware of the program. One interview was in-person; 20 were by videoconference. Interview duration was between approximately 30 and 45 min. Table 2 shows the interview participant characteristics. Three major themes emerged from the data and are explored below. Table 3 provides exemplary quotes supporting each theme.
Interview participant characteristics.

Family members consisted of a wife, a father, and two sisters.
Nurses represented the following clinical roles: neonatal intensive care unit, adult acute care unit, and adult intensive care unit. Four of the nurses were nurse managers; one was a charge nurse.
Years of experience since completed training.
For patients and family members, frequency refers to during the hospitalization. For care team providers, frequency refers to current use.
Type of internet access for patients refers to what they have access to when not in the hospital.
Extemporary quotes by theme.

Theme 1: inpatient telehealth enhanced the patient and family experience through strengthened relationships and increased support
Every interview participant described how telehealth use to virtually bring family to the bedside of hospitalized patients strengthened patient- and family-provider relationships. Nurses and physicians explained how the use of telehealth humanized patients by allowing providers to meet patients’ family. Nurses and family members shared how it strengthened families’ trust in providers. Family members stated how telehealth let them witness providers’ body language with the patient, which instilled trust and reassurance. Multiple nurses and one physician expressed that this increased trust facilitated their ability to communicate with patients’ families, especially for difficult topics such as end of life conversations. One physician, however, stated that a limitation of telehealth is the inability to read body language accurately, which limits the ability to express empathy and recognize family members’ emotions. Despite this concern, they thought telehealth is superior to telephone in that it allows for a “more human touch.”
Interview and survey free text data revealed that telehealth was perceived by family and providers to be a tool that supported family members’ wellbeing and addressed their unique needs. Telehealth allowed family to visit without exposure to risks such as COVID-19. Family members could visit virtually while grieving or expressing emotions privately in their own homes. Family members shared how telehealth gave them “peace of mind” and helped them feel “very cared for” and “included and… more embraced.”
The program supported the patient, too. Participants explained how telehealth made it so patients were no longer isolated from their lives outside the hospital. With telehealth, patients could participate in routines such as family dinners or bedtime rituals. One family member wrote about talking, singing, and playing the piano to calm her son. Nurses shared stories of telehealth use lifting patients’ spirits. Similarly, a patient explained how he was depressed while hospitalized, and telehealth family visits helped encourage him to keep fighting.
While interviewees of all role types expressed that the Inpatient Telehealth Program enhanced the patient and family experience, survey data suggested that some patients did not value this program. Although almost every family member repondant reported that they would use the program again (94.5%), a smaller propoprtion of patients felt similarly (75.8%). Family member survey repsondants also had higher overall experience ratings than both the patients and providers.
Theme 2: inpatient telehealth enhanced patient care through improved information sharing and engagement
Inpatient telehealth was perceived to enhance patient care by providing direct communication lines between providers and family. Nurses explained how telehealth family visits created dedicated time for nurses to update families about the patient's status and care plan. Direct lines of communication helped families make more informed decisions. It also was perceived by providers to improve their ability to gather relevant information. For example, providers could obtain information from telehealth connections about the patient's medical history; family members could show the providers the patient's living situation or home medications.
Providers perceived telehealth to be a tool that connected family members during pivotal clinical circumstances. It enabled large groups of family to gather quickly to discuss and to hear information. The virtual gatherings were easier to coordinate compared with in person gatherings which allowed decision-making to occur sooner. Care decisions that would typically be delayed until family was physically at the bedside were made in real-time via telehealth. This was beneficial, for example, for patients whose clinical status was rapidly declining.
Telehealth helped family members gain increased understanding of the patient's clinical status and care plan. Providers could see family members’ nonverbal cues and thus improve their ability to interpret whether the family member was adequately comprehending the conversation. Family members shared feeling more confident in their ability to make informed care decisions and relay information to other family members. Family members gained improved knowledge, skill, and confidence to care for the patient. This increased activation was perceived to benefit the patient, particularly for the transition from hospital to home. For example, family members received virtual training on discharge instructions such as wound care plans.
This perception that inpatient telehealth enhanced patient care aligns with the survey data in that most provider survey respondants reported that the goal of the telehealth encounter was met (86.1%). However, some providers were dissatisfied with the program, as only 83.3% of respondants reported that they would use inpatient telehealth again. The free text repsonses from providers suggested that the platform is a source of discontent. Providers wrote about poor audio quality, poor video quality, and delays. Also, compared to patients and family, providers reported worse ratings for audio and video quality.
Theme 3: low awareness of the program limited adoption of inpatient telehealth
Multiple providers explained that widespread adoption of inpatient telehealth was hindered by limited awareness of the program. They shared how most patients and families did not know about this resource, but that the program's “untapped potential” must be addressed. One factor contributing to limited awareness of the program among patients and families was that providers inconsistently offered telehealth family visitations. Rather than offering telehealth use to all patient families, providers shared that the program was mostly offered to families of patients with no visitors.
Restricted offering of telehealth was possibly due to the burdens that the program placed on some nurses. Nurses stated that setting up the equipment impeded their workflow at times. Other acceptability issues among some nurses included patient privacy concerns given the inability to confirm all the individuals listening to and seeing the patient. Despite these unanticipated consequences of the program, every interviewed provider participant shared overwhelming desire for the program to continue.
Family interviewees suggested strategies to increase Inpatient Telehealth Program adoption. They advocated for targeted efforts to expand awareness, such as a marketing campaign that broadly advertised the benefits of telehealth family visitations. Multiple participants emphasized that it should be offered to all families at the time of admission. They recommended integrating it into conversations around hospital visitation policies. Some family members and providers articulated the need for additional program resources so that telehealth family visitations could be equitably accessed by all families, including those lacking broadband and smart devices. Another suggestion was to have clerical support for the program to promote expansion while minimizing burdens imposed on nurses. Although uncommon, some participants shared that the clerks in their hospital unit had the responsibility of teaching families how to use the telehealth platform, coordinating the timing of the visits with families, and setting up the telehealth equipment at the bedside. Nurses from these units expressed appreciation for clerical support, and clerks expressed their gratification in supporting the program.
Discussion
This mixed methods study identified patient, family, and provider perspectives of using telehealth in the hospital for family engagement. Inpatient telehealth was thought to strengthen relationships, increased support, and improve information sharing and engagement. Despite these perceived benefits, adoption of the program was restricted, largely due to limited awareness of the program among patients and families. Figure 1 presents a logic model of the relationships among the program's activities and its outcomes. As shown in the logic model, multiple external factors and assumptions influence the use and impact of the Inpatient Telehealth Program. Lessons learned from this study can be used to standardize implementation and optimize the program.
Our finding that telehealth use was perceived to improve patient and family experience is consistent with prior research. A randomized controlled trial identified that the use of telehealth to virtually bring family members to the bedside during family-centered rounds improved parent-reported Child Hospital Consumer Assessment of Healthcare Providers and Systems Survey scores. 33 Similarly, a non-randomized study reported improved family-provider communication with the use of telehealth to virtually transmit family to the bedside, 34 which aligns with our present study's finding that telehealth improved patient- and family-provider relationships and information sharing.
Other prior research has examined unintended consequences of telehealth projects, such as the ten-project evaluation by Alami et al. 35 Some findings aligned with our present study, including concerns that telehealth use increased providers’ workload. Regarding a result that did not align with our present study, Alami et al. found that telehealth sometimes reduced patient and family contact time with providers and made interactions less patient-centered. These results contradict our major finding that telehealth use strengthened relationships, facilitated communication with providers, and enhanced principles of patient- and family-centered care. This difference is likely explained by the way in which we used technology for our program; the focus of our use of telehealth was to support family visitations, not for direct patient care.
Another finding that diverged from prior research was that digital literacy was not a barrier expressed by our study participants. Although we did not specifically evaluate digital literacy in quantitative or qualitative data collection, we explored contextual factors influencing implementation of the Inpatient Telehealth Program. We anticipated that digital literacy might present as an influencing factor, because digital literacy is widely recognized as a significant inhibitor preventing diverse populations from using telehealth services.36,37 Potentially, our platform and workflow for the Inpatient Telehealth Program might be more user-friendly compared to other telehealth programs. Nevertheless, we must continue to evaluate our program reach and impact to ensure equitable access and benefit among diverse populations.
Our study is not without limitations. We limited participants to those with English proficiency. The survey used in this study has not been validated, and we do not have data on survey respondant characteristics. The qualitative phase of our study was also limited by the participation of only one patient. Although patient and family perspectives were well-represented in the survey data, inclusion of additional patient and family interviews could have potentially enriched our understanding with insights not captured in this study. Conversely, despite relatively fewer provider survey respondants, we included a comparatively larger number of provider interviewees. As such, provider perspectives about the Inpatient Telehealth Program are represented with in-depth information.
Our hospital has extensive and established support for telehealth service lines. Thus, inpatient telehealth programs at hospitals with limited resources would likely differ, limiting the transferability of our findings. We conducted our interviews during COVID-19; those results might only be applicable to this circumstance. However, survey data were collected through October 2022 when COVID-19 was a less influential contextual factor. The Inpatient Telehealth Program has continued to remain an active service across the hospital to date. Various adaptations to the program have occurred. Briefly, the Inpatient Telehealth Program now integrates with the health system's video medical interpreter platform, ExtendedCare is the only IT-supported platform for the program, and families are able to join the telehealth connection using a direct-join link without the necessity of downloading an application. Future research is needed that evaluates the current version of the program. Despite these limitations, trustworthiness of this study is supported by the use of investigator triangulation, peer debriefing (i.e., regular team meetings), and negative case analysis.
Conclusion
This study provides valuable information on the use of telehealth for family engagement in the hospital setting, which is relevant to many hospitals aiming to establish and improve innovative family engagement solutions. The Inpatient Telehealth Program is perceived to enhance patient care and the patient and family experience. Future work is needed to identify best practices to overcome unintended consequences of provider workload burden and to enhance equitable awareness of and engagement with the program.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241267374 - Supplemental material for Using inpatient telehealth for family engagement: A mixed methods study of perceptions from patients, families, and care team providers
Supplemental material, sj-docx-1-dhj-10.1177_20552076241267374 for Using inpatient telehealth for family engagement: A mixed methods study of perceptions from patients, families, and care team providers by Jennifer L. Rosenthal, Jacob Williams, Keegan F. Bowers, Sarah C. Haynes and Lori Kennedy in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241267374 - Supplemental material for Using inpatient telehealth for family engagement: A mixed methods study of perceptions from patients, families, and care team providers
Supplemental material, sj-docx-2-dhj-10.1177_20552076241267374 for Using inpatient telehealth for family engagement: A mixed methods study of perceptions from patients, families, and care team providers by Jennifer L. Rosenthal, Jacob Williams, Keegan F. Bowers, Sarah C. Haynes and Lori Kennedy in DIGITAL HEALTH
Supplemental Material
sj-pdf-3-dhj-10.1177_20552076241267374 - Supplemental material for Using inpatient telehealth for family engagement: A mixed methods study of perceptions from patients, families, and care team providers
Supplemental material, sj-pdf-3-dhj-10.1177_20552076241267374 for Using inpatient telehealth for family engagement: A mixed methods study of perceptions from patients, families, and care team providers by Jennifer L. Rosenthal, Jacob Williams, Keegan F. Bowers, Sarah C. Haynes and Lori Kennedy in DIGITAL HEALTH
Footnotes
Contributorship
JLR conceptualized the study design, facilitated the data collection sessions, analyzed and interpreted the data, drafted and revised the manuscript, and approved the final version of the manuscript. JW collected data, analyzed and interpreted the data, revised the manuscript, and approved the final version of the manuscript. KFB assisted with conceptualization of the study design, collected data, revised the manuscript, and approved the final version of the manuscript. SCH analyzed and interpreted the data, revised the manuscript, and approved the final version of the manuscript. LM assisted with the study design, analyzed and interpreted the data, revised the manuscript, and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of the University of California Davis approved this study (IRB number: 1640525).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health [grant number K23HD101550 to Dr Rosenthal]. The project was supported by a University of California at Davis (UC Davis) Clinical and Translational Science Center (CTSC) Pilot Projects Grant [grant number UL1TR001860]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or UC Davis CTSC.
Guarantor
JLR.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.