
Abstract
Objective
This study aimed to summarize the characteristics of the Internet hospital services of the Seventh Affiliated Hospital of Sun Yat-sen University (SAHSYSU), describe diagnosis and treatment patterns in each department, determine SAHSYSU Internet hospital's role in pandemic control, and explore development strategies in non-pandemic situations.
Methods
Mixed-methods was used in this study. Qualitative organizational behavior analysis was conducted on hospital meeting records and semi-structured interview records to determine the research analysis indicators. We quantitatively analyzed online consultation record data of SAHSYSU Internet hospital from January to December 2020, and conduct classification analysis on departmental case studies using K-means clustering algorithm.
Results
29,944 patient data items were retrieved. Internet hospital services synchronized with COVID-19 pandemic development in China and Guangdong province. The service volume peaked during the period of January to March, which coincided with the height of the pandemic. Out of the total visits, 58.90% were conducted during office hours while 41.10% were conducted during non-office hours. The majority of the patients came from Guangdong (19.67%) and Hubei (9.09%) provinces. The cluster analysis identified three clusters, each with different change rates and magnitudes of change for various departments.
Conclusion
Internet hospitals complemented conventional medical services, providing crucial medical care during the COVID-19 pandemic. Internet hospitals are the future trend of medical services and should be improved based on each department's treatment characteristics.
Introduction
The coronavirus disease 2019 (COVID-19) outbreak in China in late 2019 and early 2020 rapidly attracted global attention. Following the initial COVID-19 outbreak, a series of variants emerged such as Delta and Omicron, as well as subvariants, which were more infectious and prolonged the pandemic, with multiple outbreaks in China and a new round of COVID-19 outbreaks in Shanghai, Guangzhou, and other cities after 2020. The Chinese government implemented a series of administrative measures to stop the spread of infection and to protect people's lives and health through establishing both portable and Internet hospitals. Nonetheless, the COVID-19 pandemic had a huge impact on China's healthcare system. Safeguard measures during the pandemic, such as restrictions on human activities and lockdowns, made it difficult for medical organizations to operate in their previous manner at a time when the pandemic required medical organizations and Chinese institutions to play an even greater role. As such, Internet hospitals emerged as the main form of telemedicine services for the public to meet the demand for medical treatment during the COVID-19 pandemic. Exploring the operation mode of Internet hospitals in response to sudden major crises is of great practical significance to strengthening the healthcare system in China as well as for the sustainable and continuous development of Internet hospitals during normal times.
Internet hospitals, as an online extension of brick-and-mortar hospitals’ offline services in China, offer new ways to provide outpatient healthcare services based on Internet technology that enables patients to receive medical and healthcare services across space.1,2 In addition, China's current Internet hospitals can also provide offline outpatient appointment registration, examination report inquiry, medical science and other diversified services. Patients access the Wechat official account of Seventh Affiliated Hospital of Sun Yat-sen University (SAHSYSU) through mobile phones, tablets, and other mobile electronics to use SAHSYSU's Internet hospital service (The system does not recognize and record its device type). Compared with offline hospitals, Internet hospitals offer advantages such as higher efficiency, lower costs, optimal resource allocation, and non-contact treatment, while transcending spatial limitations. 3 However, technical support issues, limitations of clinical care (limitations of physical examination), insufficient physicians available for such services, and the lack of trust between patients and physicians remain as disadvantages.4–8 Prior to the COVID-19 pandemic, telemedicine, as an important function of Internet hospitals, was mainly limited to providing care to populations in remote areas.9–11 During the COVID-19 pandemic, Chinese healthcare providers still provided essential medical support to the public through Internet hospitals, given the strict social distancing requirements to promote self-care and self-protection, as well as performing epidemiological screening, making it an important component of infection prevention and control measures.12–15 Given the background of normalized prevention and control in the post-COVID-19 era, Internet hospitals can provide a variety of medical services to overcome geographical and temporal barriers and assist in pandemic control through providing equitable and inclusive online services, while mitigating the effect of strained medical resources and the increased burden of chronic diseases as a result of virus transmission.13,16,17 However, all diseases have their own characteristics in terms of diagnosis and treatment. The diagnosis and treatment modes of Internet hospitals may play different roles in different departments. An assessment of disease characteristics concerning each hospital department to identify differences in the role of Internet hospitals in terms of the diagnosis and treatment of each department may facilitate the optimization of the operation mode and improve the quality of Internet hospitals in a normal situation.
The SAHSYSU is a tertiary hospital directly affiliated to Sun Yat-sen University, which was constructed by the Shenzhen Municipal Government and is operated and managed by Sun Yat-sen University. It is a key development project within a three-goal strategy, namely, to introduce and nurture leading medical specialists, to establish reputable hospitals, and to develop clinics as centers of excellence in Shenzhen. After the COVID-19 outbreak, SAHSYSU rapidly launched an “Internet hospital” platform using digital technology to provide online medical services to facilitate medical care access for older adults as well as for patients who were frail or who had impaired mobility during the pandemic. Moreover, it reduced non-essential offline medical visits for patients with minor illnesses and educated the general public concerning COVID-19. More importantly, the Internet hospital platform reduced the potential for cross-infection when patients and their families visited hospital as well as the possibility of disease spread, thereby reducing the burden of COVID-19 prevention and control.
In this study, statistical methods and cluster analysis using machine learning were integrated to process Internet hospital consultation data, online communication texts between physicians and patients, patient evaluation of physicians, and desensitized personal patient data. We aimed to describe and summarize the characteristics of SAHSYSU Internet hospital services in terms of patients’ usage time, sources, and physician–patient interaction during consultation through extracting diagnosis and treatment patterns in each Internet hospital department to determine the role of the Internet hospital in COVID-19 prevention and control, and elaborate and explore the development strategies of Internet hospitals in a normal situation.
Methods
The objectives of this study were to investigate how an Internet hospital undertook prevention, diagnosis, and treatment during the COVID-19 pandemic, and to determine how the disease characteristics of different departments affected diagnostic behavior. We undertook to analyze the diagnosis and treatment processes involved in Internet hospital services and physician–patient interactions. Therefore, adopting mixed-methods, this study drew on the research paradigm combining case studies with machine learning and performed exploratory data analysis with embedded case studies to establish a study approach combining theory and machine learning. 18
Setting and participants
In accordance with the Chinese government's requirements for COVID-19 prevention and control to reduce non-essential offline medical visits for patients with minor illnesses, SAHSYSU launched an emergency “Internet Hospital” platform on 26 January 2020, which opened up online outpatient services of text consultations for various departments, such as internal medicine, surgery, gynecological, pediatric, dermatological, and pharmaceutical departments, to all users in China. In total, > 300 volunteer physicians and pharmacists were recruited to provide remote online services for patients.
Data collection and analysis
The data for the exploratory analysis in this study included the time and source location of online service users of the Internet hospital, online communication texts between doctors and patients, patient evaluation data of physicians, and desensitized personal data of patients. The data were collected from 26 January 2020 to 31 December 2020. Among them, the system launched and mainly held consultations concerning COVID-19-related symptoms from 26 January to 7 February 2020, and the consultations were mainly on certain specific disease types from 8 February to 31 December. Offline consultations resumed on 1 March, and both online and offline consultations were undertaken thereafter. In this study, 29,944 valid doctor–patient interactions were screened from all the data (excluding the texts in which consultation was not performed on any specific disease type or only on COVID-19-related information at the beginning of the Internet hospital, and the low quality text including fewer than three doctor–patient interactions or where the patient's description of the condition is too vague to elicit an effective response from a medical professional), obtaining a total of approximately 7 million words of interaction texts.
In this study, archived data from each department during the COVID-19 pandemic were collected, including meeting minutes, internal communications, and discussion records. The Internet hospital records of the case study departments during the COVID-19 pandemic were also coded and analyzed. Moreover, patient evaluations of the physicians were collected. Semi-structured interviews with the president and vice-president of the SAHSYSU as well as the department head in charge of the Internet hospital were performed to explore the development of the Internet hospital. Semi-structured interviews were also conducted with the directors of the departments analyzed in this study, the physicians who participated in the Internet hospital in the departments, and physicians who did not join the Internet platform. The interviews included identifying department strategies that had been developed to cope with changes during the COVID-19 pandemic, how to familiarize with and use the Internet treatment platform, difficulties identified during the use of the platform, how to overcome difficulties and develop diagnosis and treatment modes, and differences between the diagnosis and treatment using the Internet hospitals compared with conventional outpatient clinics. One research team member headed the Internet hospital project of the SAHSYSU and was familiar with the development of the project, the key time points during development, and the operation of each department, which assisted the research team in conducting in-depth departmental interviews (Table 1, Supplementary Material 1).
Data source and content.
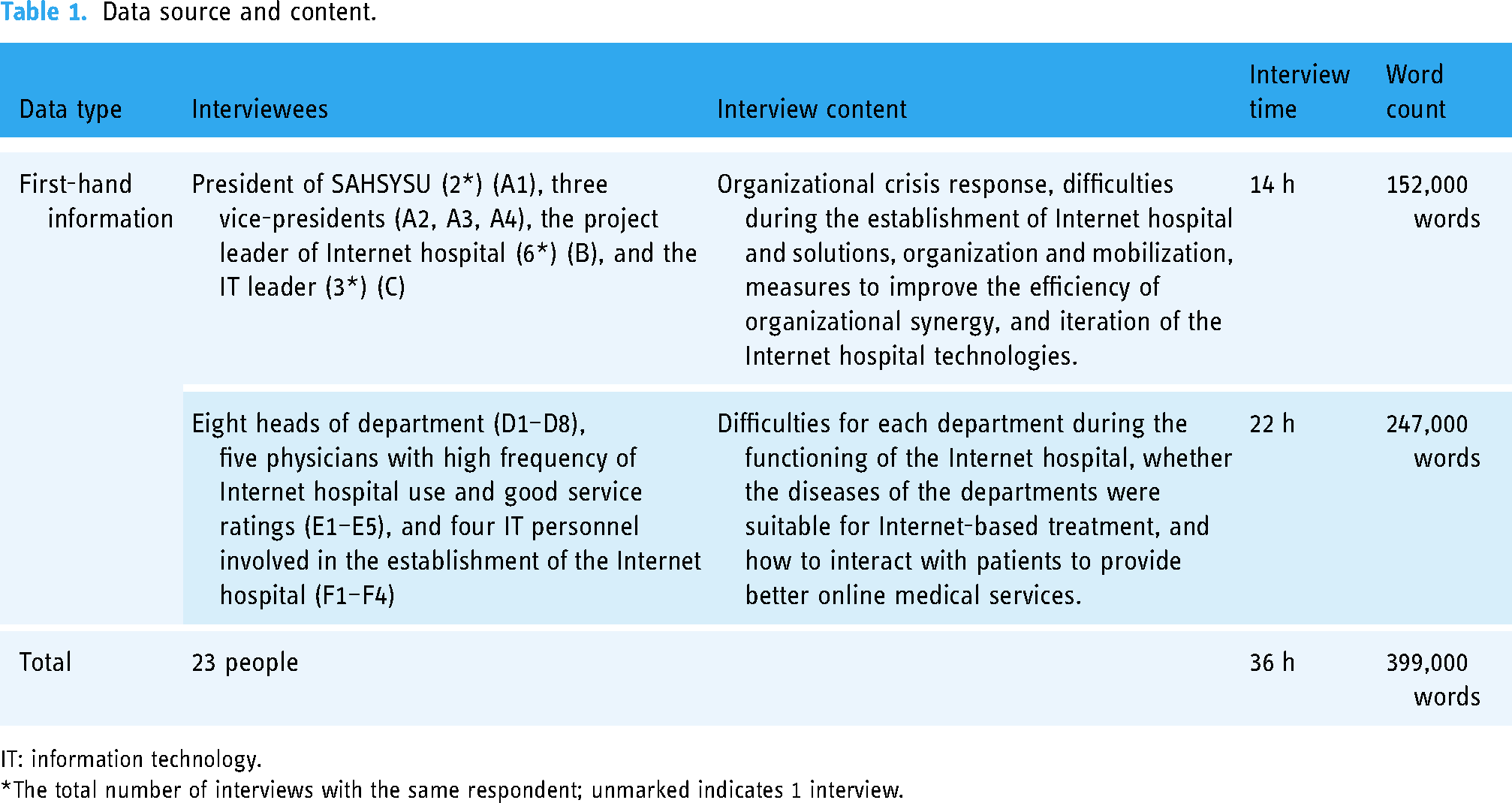
IT: information technology.
The total number of interviews with the same respondent; unmarked indicates 1 interview.
In addition to the online service data of the SAHSYSU Internet hospital from January to December 2020, data from the public platform of the National Health Commission of the People's Republic of China, the public platform of Guangdong Provincial Health Commission, the China Health Statistical Yearbook 2021, and the China Statistical Yearbook 2021 were also extracted to obtain the number of confirmed cases of COVID-19, the number of tertiary hospitals in each region of China, the number of outpatient and emergency visits at each department, as well as the population and gross domestic product (GDP) of each region in China to perform correlation analysis with the online service data.
Application of machine learning techniques
Step 1. Organizational behavior analysis: establishment of departmental diagnosis and treatment modes for the Internet hospital
The COVID-19 pandemic resulted in sudden changes to social production and lifestyles. In response to the pandemic, medical institutions urgently initiated Internet hospital platforms to diagnose and treat patients as well as provide health-related consultations. The speed and magnitude of organizational change are important indicators of an organization's ability to respond to sudden and profound changes. For Internet hospitals, it is more appropriate for a department to develop Internet-based medical services if the treatment mode of the department can rapidly adapt to the sudden changes in diagnosis and treatment methods brought about by the COVID-19 pandemic. Based on the practice of Internet hospitals, this study first selected indicators that represented the “speed of change” of the organization, including the response time of physicians’ consultations and the number of patients per week. Second, indicators that represented the “magnitude of change” of the organization were selected, including the number of messages sent by physicians during consultations and whether the consultation conversation ended in a standard manner (Discussions concluded smoothly without any disruptions due to technical or network issues which indicates that the patient gained a clear understanding of the information they sought, and they ended the conversation after engaging in thorough communication with the healthcare provider.). These two indicators were used in relation to the responses of the departments during the pandemic and formed the basis of analysis concerning Internet-based diagnosis and treatment modes in each department.
Step 2. Analysis unit selection: inductive case study
Case studies are often based on the principle of theoretical sampling, in which cases that would better answer the research questions are selected as research objects. 19 Therefore, this study adopted an inductive case study approach with an embedded single-case study design. We performed cross-case analysis through using different departmental activities in the Internet hospital as embedded cases as well as comparisons between sub-cases. 20 The departmental diagnostic and treatment mode involved considerations of flexibility and speed of response. Research on departments in the same organization may be used to control for the impact of irrelevant variables and also facilitate in-depth analysis of the establishment process and method of the departmental diagnosis and treatment modes of the Internet hospital. Moreover, the embedded single-case study design enabled this study to comply with the requirements of the theoretical establishment of multiple cases, thereby enhancing the generalizability of the findings.21,22
Based on the findings of the previous exploratory data analysis, theoretical sampling was first performed in this study. Specifically, this study identified three department types based on different modes derived from exploratory data analysis. The first category included departments with rapid but small changes, such as the neurology department. The second category included departments with slow but large changes, such as the traditional Chinese medicine (TCM) department. The third category included departments with both change speed and magnitude that were higher than average, such as the gastroenterology department (Table 2). Among the three types of departments above, we selected specific departments for case studies in this study. First, the departments with the highest number of medical visits and the departments with the lowest number of visits in each category were selected for case studies. Such theoretical sampling would ensure the representativeness of the cases as well as data availability. Second, one department among the remaining departments in each category was randomly selected as a case study to improve the robustness of the cases. In this study, the above method was repeated in all three department types (i.e. three cases were proposed to be selected in each type of department). However, since the departments with both rate and magnitude of change higher than average only included the gastroenterology and thoracic surgery departments, a total of eight cases were selected for analysis in this study.
Brief introduction of cases.

TCM: traditional Chinese medicine.
Step 3. Machine learning applications: k-means clustering
Finally, machine learning was applied to improve the scale and precision of theory construction. Machine learning methods may help to discover patterns from the data and select the most predictive models. 23 Commonly used machine learning methods mainly include supervised and unsupervised learning. Supervised learning may be used in cases where a particular dataset (training set) has a certain attribute (label) while the rest of the data are not labeled or require a predict label. Unsupervised learning can be used in cases where the dataset does not have a given label (data is not pre-assigned) and where an algorithm is required to identify potential relationships between the data. 24
In this study, unsupervised learning cluster analysis was performed. Clustering is the process of classifying different types or clusters based on data features, resulting in high similarity among objects in the same cluster and large differences in the objects between different clusters. Cluster analysis is an exploratory analysis in which a classification criterion is not necessarily provided in advance. Cluster analysis is able to classify automatically from the sample data. Therefore, clustering can be used as an independent tool to obtain data distribution and to observe the characteristics of each cluster, thus enabling further analysis on a specific set of clusters. In this study, the classical k-means clustering algorithm was used, where the input of the algorithm was a sample set (or point set) in which the samples were clustered. The first step was to select the number k of categories to be clustered, namely, to select k centroids. The second step was to identify the nearest centroid for each sample point (find the classification), and classify the closest point to the same centroid as one cluster. One clustering process was completed through the above steps. The third step was to determine whether classification of the sample points before and after the clustering was the same. If it was the same, the algorithm was terminated. Otherwise, a fourth step was performed, which involved calculating the centroids of the sample points in each cluster as new centroids of the cluster, and the second step was then performed. The above process was cycled until no change was observed for the clustering before and after two iterations. Therefore, in this study, k-means clustering was suitable for the theoretical construction of the treatment characteristics of the Internet hospital departments through exploring the text concerning physician–patient interactions.
Statistical analysis
In this study, SPSS was used for data analysis to correlate the monthly service volume of the SAHSYSU Internet hospital with the number of confirmed cases of COVID-19 in China and Guangdong province in each month of 2022, the number of tertiary hospitals in each province, as well as provincial GDP and the total population in each month of 2022, so as to comprehensively explore the characteristics of the Internet hospital services. The existence of a statistically significant relationship (P < 0.05) between the two data sets was first tested, and a P-value ≤0.05 was considered statistically significant. Pearson correlation analysis was performed on two datasets with statistical significance. The two sets were considered to have a strong correlation if the absolute values of the correlation coefficients were >0.8, a weak correlation if the absolute values were between 0.3 and 0.8, and no correlation if the absolute values were <0.3.
Results
The SAHSYSU Internet hospital received a total of 29,944 patient data items, which represents the number of complete consultations (considering that the same patient may visit multiple times), from January to December 2020, which were analyzed in terms of date and time of use, patients’ geographic location, and specific patient–physician interactions.
Characteristics of temporal distribution of the consultations
The service volume of the SAHSYSU Internet hospital reflected the development of the COVID-19 pandemic in China, with the distribution of Internet hospital services according to month synchronized with the pandemic. In January 2020, the sudden onset of the COVID-19 pandemic promoted online medical services. January (3772 items of patient data, 12.60%), February (15,378 items of patient data, 51.36%), and March (2894 items of patient data, 9.66%) were the most serious time periods of the COVID-19 pandemic in China, and the consultation volume in these three months was also the highest in 2020. The number of consultations increased dramatically in February (a dramatic increase might have been expected to have occurred in January, but the number of consultations was low in early January when COVID-19 had not yet developed on a large scale). From April to June, the pandemic flattened and offline consultations gradually resumed. The number of consultations dropped, with the number of users being approximately 1300 per month. From July to September, the pandemic slowed, and a significant decrease was observed in consultation volume. However, a sudden and dramatic increase was observed in consultation volume in October, which then dropped rapidly in November and December. A strong correlation with high significance was observed between consultation volume according to month and the number of confirmed cases in China and Guangdong province in each month (Table 3, Figures 1 and 2).

Number of confirmed cases in China and the number of consultations at the SAHSYSU Internet hospital from January to December 2020.
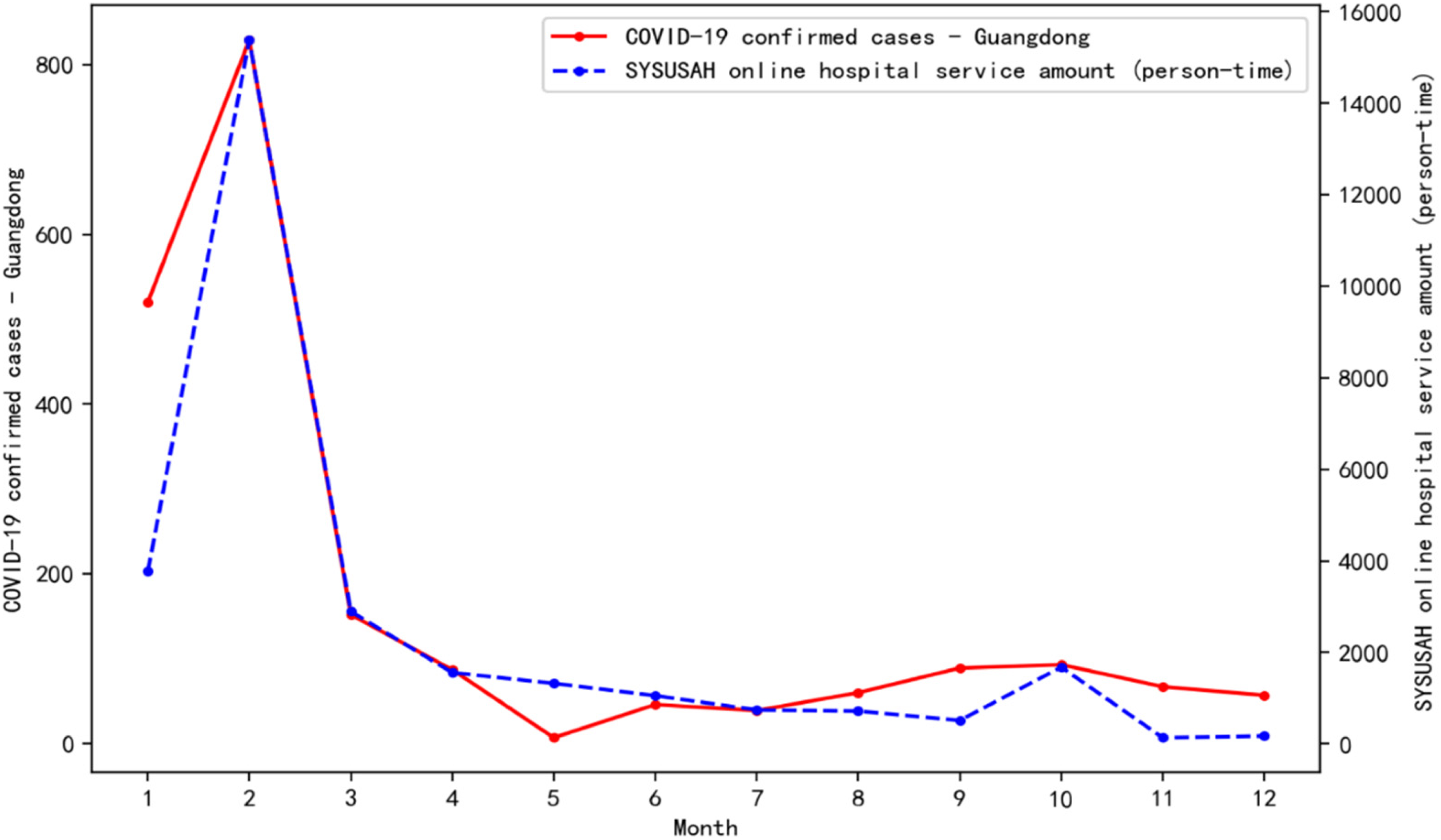
Number of confirmed cases in Guangdong province and the number of consultations at the SAHSYSU Internet hospital from January to December 2020.
Correlation coefficients between the number of confirmed cases in China, the number of confirmed cases in Guangdong province, and the consultation volume at the SAHSYSU internet hospital from January to December 2020.

Data source: National Health Commission of the People's Republic of China, Health Commission of Guangdong Province.
*** represented 1% significance levels, respectively.
In terms of consultation time, there were 17,638 (58.90%) consultations during office hours (8:00–18:00 h) and 12,306 (41.10%) consultations during non-office hours. The dynamics of daily reported service volume per hour showed that during business hours, the number of consultations per hour was similar, whereas during non-business hours, the peak of consultations occurred between 18:00 and 22:00 h (Figure 3).

Number of consultations according to time at the SAHSYSU Internet hospital from January to December 2020.
Geographical distribution of patients
A total of 29,348 data items contained geographic location (596 missing data) from 31 provinces (autonomous regions). Among these, high usage was observed in Guangdong (5774, 19.67%), Hubei (2668, 9.09%), Henan (2143, 7.30%), Hunan (2052, 6.99%), and Zhejiang (2028, 6.91%) provinces, while Shandong, Sichuan, Hebei, Anhui, Jiangxi, and Guangxi provinces had >1000 consultations. This high usage shows the key role of the Internet hospital in cross-regional healthcare and the expansion capacity of healthcare services. Due to the virtual treatment services provided, the SAHSYSU Internet hospital served more patients from Hubei, the province most severely affected by COVID-19, among patients from outside Guangdong province (Figure 4).

The number of consultations at the SAHSYSU Internet hospital according to province (region) in China, January to December 2020.
In terms of temporal trends, the overall trend in each province was that a certain number of patients emerged in January, with a dramatic growth in February, which then reduced in March, with May and September being two clear turnaround points. Guangdong province was the main source of patients for the SAHSYSU both online and offline as well as prior to and after the pandemic, with little decline in the number of visits. Despite a decrease in demand in September, consultations from Guangdong province still maintained a double-digit number and a certain level of demand was retained. From May 2020, as the work and life of people, including those involved in offline medical care, returned to pre-pandemic conditions, all five provinces of Hubei, Henan, Hunan, Shandong, and Sichuan, which had a high overall service usage, saw a decrease in demand from May and a sharp decline from September. Other provinces with fewer visits overall saw a substantial drop in demand from May (Table 4).
The number of consultations in different provinces (regions) at the SAHSYSU internet hospital in China, Jan-Dec 2020.

Data source: National Health Commission of the People's Republic of China.
Characteristics of treatment in the departments
In this study, quantitative data on consultation response times and the number of patients a physician saw per week were first analyzed to establish the diagnosis and treatment modes of the Internet hospital departments. Second, texts involving physician–patient interactions were mined to determine whether conversations ended in a standard manner. Table 5 shows the descriptive statistics of the indicator variables mentioned above. Furthermore, based on these indicators, this study performed statistical analyses according to departments for comparison. The analyses showed three different types of characteristics during the operation of different departments. The first type included departments where the change rate was higher than average, but the magnitude of change was lower than average. The second type included departments where the change rate was lower than average, but the magnitude of change was higher than average. The third type included departments where both the rate and magnitude of change were higher than average.
Statistical analysis results of variables.

Based on the findings of the exploratory data analysis, this study analyzed the interview data of eight selected cases to extract two core constructs that characterized the rate and magnitude of change in a department, namely, the convenience level of physician–patient interaction and the level of standardization of the treatment mode. In addition, in the exploratory data analysis, the physicians’ consultation response time and the number of patients they saw per week were used as variables to measure the “rate of change” in the department in the adaptation to online consultation. The number of messages sent during consultation and whether the conversation ended in a standard manner were used as variables to measure the “magnitude of change” in the department during adaptation to online consultation. In the case studies, two variables were further extracted, namely, “whether the physician received patients on weekends” and “the rounds of consultation,” where the former was a measure of how quickly a physician responded to patients’ requests, while the latter characterized the magnitude of the change of the diagnosis and treatment mode of the physician, that is, whether the physician could grasp and respond to the patients’ consultations rapidly. The faster the “convenient interaction,” the faster the department adapted to online treatment. A higher level of “mode standardization” indicated that a department had changed considerably to adapt to the changes in online diagnosis and treatment. Based on the case studies, this study further refined the clustering metrics of machine learning (Table 6).
Results of variable analysis.

In this study, text analysis on physician–patient interaction data with >7 million words was first performed to extract organizational variables from unstructured text data through natural language processing. Based on these findings, a classical k-means clustering algorithm was used to analyze the data of 35 departments that carried out online diagnosis and treatment during the COVID-19 pandemic, and the number of clusters K was set as 3. According to the iteration results, three different types of diagnosis and treatment patterns were observed in the Internet hospital departments. The first type included departments where the rate of change was higher than the mean and the magnitude of change was smaller than the mean. The second type included departments where the rate of change was lower than the mean and the magnitude of change was higher than the mean. The third category included those where both the speed and magnitude of change were higher than the average. The three mode types were consistent with the hypothesis in the statistical analysis above. The cluster characterization indicators of each variable specific to the three types of departments are shown in Table 7. Variables characterizing the rate and magnitude of organizational change were extracted based on the combination of exploratory data analysis and embedded case study results to identify three organizational reconfiguration modes of Internet hospitals, thereby obtaining three different types of diagnosis and treatment characteristics of the departments in the Internet hospital. Furthermore, the eight cases selected for analysis in this study were included in the cluster analysis to derive different reconfiguration modes and the values of each variable for the eight departments (Table 8).
Clustering results.

Internet treatment mode in different departments.

Discussion
The COVID-19 pandemic led to an unprecedented “lockdown” of countries and societies worldwide.25–27 While mandatory restrictions and extensive lockdowns may have limited the spread of this highly infectious disease, they also inevitably disrupted the routine treatment of patients with other diseases or normal access to medical care, limiting the capacity of healthcare systems to serve and treat uninfected populations. Without continuous medical care, tens of millions of patients with a variety of chronic conditions may have suffered from potentially worsening health conditions, and patients with new health issues would have faced challenges receiving appropriate treatment. 3 Internet hospitals were necessary during COVID-19 outbreaks in China, providing continuous medical care to the public while limiting nosocomial transmission of the virus, and remain essential not only for dealing with COVID-19 but also for future infectious disease outbreaks. 3
This study described the initial construction and implementation of an Internet hospital in response to the COVID-19 pandemic. Through a comprehensive analysis of patient data from the SAHSYSU Internet hospital service in 2020, this study found that the SAHSYSU Internet hospital service contributed to providing continuous medical care during the COVID-19 pandemic and promoted cross-regional healthcare services. Analysis of the diagnosis and treatment characteristics according to each department provided evidence-based references and insights for future construction of Internet hospital platforms in general hospitals.
The efficacy of Internet hospitals
Internet healthcare guaranteed continuous medical care
The study findings indicated that the data volume of the SAHSYSU Internet hospital services in 2020 was strongly correlated with the number of confirmed cases of COVID-19 in China as well as in Guangdong province, indicating an association between the demand for Internet hospital services and the development of the COVID-19 pandemic, which is consistent with previous studies. To stop transmission of infectious diseases so as to protect people's lives, restrictions and quarantine measures for prevention and control of COVID-19 in China related positively to the scale of the COVID-19 outbreak; however, strict restriction measures affected the performance of conventional medical services. The volume of Internet hospital services has also been shown to positively correlate with the scale of the COVID-19 outbreak, indicating the effectiveness of Internet hospitals in supplementing conventional offline medical services during the pandemic as well as ensuring continuous healthcare services during the pandemic.
The utilization rate according to time, “forward triage”, and the effectiveness of Internet hospital services in providing comprehensive services were described through balanced services between office and non-office hours, indicating that the Internet hospital guaranteed the continuity of medical services. 1
Internet healthcare promoted cross-regional healthcare equity
The geographic origin data of patients at the SAHSYSU Internet hospital also showed that Internet hospital services took full advantage of digital technology to enable accessibility in remote areas. Internet hospital services also remotely supplemented healthcare human resources in the most affected areas of the pandemic to ensure the capacity of medical service provision. 4 Through a comprehensive analysis of the two dimensions of “month” and “geographical distribution” in the patient data, the total number of patients and the number of patients outside Guangdong province were found to be higher during the development of the pandemic when control measures were strict. The number of patients decreased when the pandemic eased, with higher sensitivity and magnitude of the decrease observed in relation to the number of patients outside Guangdong province in line with a decrease in the scale of the pandemic. As pandemic prevention and control policies directly affected standard face-to-face medical visits, it was evident that Internet-based healthcare and conventional healthcare complemented each other.
Tertiary hospitals in China provide medical and health services across regions, provinces, and cities as well as to the whole country, and are medical prevention technology centers with comprehensive medical, teaching, and research capabilities. As high-quality medical resources, the distribution of tertiary hospitals strongly correlated with regional economic development level and population. Some of the areas with lower economic development levels as well as remote areas had lower medical care levels (Table 9). The SAHSYSU Internet hospital services radiated to remote areas as well as to counties and cities within China that lacked medical services, which enabled more people to access timely and efficient medical resources and helped to resolve difficult and costly access issues in relation to medical care in these areas, having been shown to serve as an option to narrow the gap between the capacity and quality of urban and rural medical services. 28
Correlation coefficients between the number of tertiary hospitals in 2020, regional GDP in 2020, and regional population in 2020 according to region in China.

*** represent 1% significance levels, respectively.
From a policy perspective, it is a feasible policy direction to utilize the Internet hospital to provide training platform for medical personnel in rural areas who are difficult to receive updated and advanced medical knowledge training in a timely manner, which is conducive to improving the professional quality of rural medical personnel. Actively building the communication and consultation mechanism of urban and rural hospitals through the Internet hospital platform can also effectively play the supporting role of Internet hospitals for areas lacking medical resources. It can be seen that the Internet hospital provides a viable solution to inequities in medical resources and improves the accessibility and equity of medical services, so the government can strengthen its support and input due to the extension effect that Internet hospitals may bring. However, as Internet hospitals expand their footprint, measures to ensure quality of care and data protection become critical, hence the need for a more complete regulatory framework, which is noteworthy.
Internet healthcare promoted patient satisfaction
Though the hospital studied in this study does not set up evaluation feedback for patients after each service, patients are allowed to voluntarily submit their comments after receiving online diagnosis and treatment. By conducting content analysis of these collected messages, it becomes that the adoption of online diagnosis and treatment significantly enhances patient satisfaction. The observed increase in patient satisfaction can be primarily attributed to two key factors: the reduction of medical expenses due to the online medical services, and the convenience brought by Internet hospital which allows patients to receive medical care without the need to visit healthcare facilities in person.
Through the use of telemedicine platforms, an emerging technology, doctors can diagnose and treat patients remotely, reducing the time and cost of patient visits and improving patient satisfaction. So we can see that our findings also align with the results of existing literature, reinforcing the notion that a user-friendly medical service experience is positively associated with heightened patient satisfaction.29,30 This underscores the importance of integrating online diagnosis and treatment platforms into traditional healthcare delivery methods, as it has the potential to address some of the prevailing challenges and improve patient outcomes.
The departmental treatment mode showing the applicability of Internet-based treatment in each department
Based on the results of the case studies and cluster analysis, the core constructs that characterized the speed and magnitude of changes in departments in terms of departmental diagnosis and treatment for Internet hospitals were extracted, namely, the convenience of physician–patient interaction and standardization of diagnosis and treatment. The high speed of change in a department, that is, the fast speed of convenient physician–patient interaction, indicated that a department had quickly adapted to online treatment. The large magnitude of departmental change indicated that treatment had become highly standardized, such that greater adjustments were required for departments to adapt to differences between offline and online treatment. To achieve the goals of convenient interaction and standardized consultation, the hospital reconstructed its organizational operation system and established a new operation mode. Thus, convenience of interaction and mode standardization have become core constructs for characterizing organizational agility in the organizational restructuring phase during a crisis. The analysis in this study identified differing types of reconfiguration modes and indices concerning eight departments, which were categorized as three different organizational reconfiguration modes to demonstrate the different characteristics of different departments in Internet-based diagnosis and treatment as well as different applicability of the departments in Internet-based diagnosis and treatment.
Mode 1: fast and convenient interaction with low standardization levels of treatment mode
The departments that demonstrated the characteristics of the first mode included the neurology, respiratory medicine, and ophthalmology departments. Both the number of consultations and the change in speed in these three departments were higher than the mean, that is, the interaction was faster and the magnitude of change was lower than the average, indicating that the level of mode standardization was low. Neurology and respiratory medicine departments were selected for specific analysis as follows.
Neurology department (internal medicine department—neurology)
In SAHSYSU's Internet hospital platform, neurology is the department with the largest number of consultations among all departments, which is closely related to the COVID-19 epidemic (In China, there are specialized psychiatric hospitals, and some general hospitals also have psychiatric departments, but SAHSYSU does not have a psychiatric or psychological department.). The COVID-19 pandemic brought uncertainty, isolation, disruption to daily life, and concerns about health and well-being. For neurology patients, stress and the lack of adequate care would likely result in a deterioration in their conditions. 31 Moreover, on a macro level, for most of the healthy population, the rapid development of the COVID-19 pandemic with the social restrictions imposed resulted in panic, depression, anxiety, and psychological stress to the public, thus contributing to the onset and worsening of common symptoms in department of neurology(internal medicine) such as headache, migraine, and insomnia, keeping the volume of neurology consultations at an all-time high level. Therefore, the motivation for online consultation was relatively high, exhibiting a rapid change. Neurology involves a wide range of topics with a variety of diseases.13,32–34 Multiple types of diseases may be associated with the same symptoms, and the complex nature of the discipline itself requires an in-depth understanding and analysis of patients’ symptoms. Moreover, a patient's feelings about the symptoms may affect a physician's assessment of the disease and such feelings may not be derived from pathological causes but from the somatization of psychological or emotional issues, the level of tolerance also affects how patients perceive the severity of their symptoms. It may be difficult to draw conclusions based on patients’ symptom statements and relevant examination results in both online and offline diagnosis and treatment in the neurology department. A deeper understanding of a patient's physical and psychological state and daily life is required, that is, more personalized and active inquiries need to be conducted based on a patient's condition. Therefore, less adjustment is required for the online diagnosis and treatment in the neurology department compared with offline, thus exhibiting a lower magnitude of change.
During the pandemic, negative emotions were reported to result in the onset and exacerbation of neurological disorders, 35 while Internet hospitals may have helped reduce psychological burden and raise disease awareness through providing official and responsible information, thus alleviating somatization symptoms of psychological stress.14,36 Therefore, in future development of the neurology department in Internet hospitals, comprehensive information concerning patients’ symptoms may be collected via pre-consultation questionnaires to conduct relevant analysis, so as to improve the efficiency and accuracy of online diagnosis and treatment. In the post-COVID-19 era, neurology departments in Internet hospitals should also rely on and aim to improve health consultations as well as universal access to public health.
Respiratory medicine
The total consultation volume in the respiratory medicine department was high, but with obvious temporal distribution characteristics compared with other departments. The consultations occurred mostly from January to March. The geographical distribution was balanced, with little difference between data from inside and outside Guangdong province. COVID-19, an acute respiratory infection, began to spread rapidly in China, and then worldwide, from Wuhan, Hubei in late January 2020. The initial unknown nature and the transmission pathway of COVID-19 caused widespread panic throughout China. People lacked knowledge in terms of self-protection, epidemiological history, and disease characterization, resulting in large-scale demand and action in consultations within respiratory medicine; thus, this department demonstrated a high rate of change. 13 With gradual control of the COVID-19 pandemic and the popularization of related knowledge, the public's understanding of the virus gradually became more objective and their fears declined, which was accompanied with a decreased demand for respiratory medicine consultations. The COVID-19 outbreak significantly boosted the volume of Internet consultation services in respiratory medicine. Respiratory diseases are common and frequent diseases, with a variety of types and multiple possible lesion locations within the respiratory tract. Common symptoms include cough, sputum, dyspnea, and chest pain. However, differing combinations of symptoms as well as subtle differences in similar symptoms (e.g. the different nature of sputum) may be manifestations of different diseases. The characteristics of respiratory diseases combined with the impact of the COVID-19 pandemic made it necessary for physicians to proactively obtain more detailed and individualized information for disease screening. Therefore, respiratory medicine exhibited a lower magnitude of change and still required detailed and personalized consultations similar to offline consultations to make a correct diagnosis.
The high demand of Internet-based diagnosis and treatment in the respiratory medicine department in 2020 was clearly affected by the large-scale COVID-19 outbreak, while the demand for the online diagnosis and treatment in terms of respiratory medicine after COVID-19 mostly involved the treatment of common minor and chronic diseases. The current Internet-based medical practice of the respiratory medicine department has produced favorable results in the management of chronic respiratory diseases and in the diagnosis of low-risk patients with acute respiratory symptoms.37,38 Therefore, during departmental development, while continuing to promote efficient personalized consultation, the quality of medical services may also be improved in terms of the management of chronic diseases through the organization and analysis of diagnosis and treatment data of patients with chronic diseases. Moreover, introducing common symptoms and treatment plans to the general public may help patients to self-evaluate their conditions to improve the overall efficiency of medical services.
The departments exhibiting high change speed and low magnitudes of change had a higher consultation volume with rapid responses to patient interaction. However, the disease characteristics of the relevant departments made it challenging for physicians to reach diagnostic conclusions based only on the patients’ self-reports and the assistance of relevant examinations and test reports in both online and offline consultations. The relatively low reliance on on-site examination for preliminary diagnosis required a smaller magnitude of change for the departments, that is, with a less standardized mode. Therefore, the efficient and accurate collection of relevant information on patients’ individualized symptoms is essential to improve the accuracy and efficiency of relevant Internet-based healthcare.
Mode 2: slow interaction and the highly standardized treatment mode
The departments that demonstrated the characteristics of the second mode were the TCM, endocrinology, nephrology, and rheumatology departments. The rate of change in these departments was lower than the mean, that is, the interaction was slower, while the magnitude of change was higher than the mean, indicating that this mode was highly standardized. The TCM department was selected for detailed analysis below.
Diagnosis in TCM emphasizes the integrated use of the four diagnostic techniques of making observations, listening to breathing, asking about symptoms, and taking the pulse, which involves tongue signs, facial features, sound patterns, and body odors. The pulse findings and patients’ self-reported symptoms were used as diagnostic information. Without face-to-face interaction, physicians were unable to obtain pulse and odor information using the Internet alone. The accurate acquisition of data concerning tongue and facial features as well as voice may also be limited by technology (e.g. screen and volume and tone clarity) and communication methods (text communication instead of video communication), making diagnosis difficult. Moreover, it was also difficult to perform non-pharmacological treatments (important in TCM) using Internet-based diagnosis and treatment. Information obtained using Internet-based diagnosis and treatment in the TCM department was been largely restricted these objective considerations, exerting relatively limited effects. An accurate diagnosis still cannot be separated from an offline face-to-face consultation. Therefore, there was a large gap between Internet-based TCM diagnosis and treatment and offline face-to-face consultation, resulting in relatively low levels of personalization in consultations during online diagnosis and treatment, which manifested as a highly standardized consultation mode. Patients were also aware of the impact of Internet-based diagnosis on the effectiveness of TCM consultations, and their expectations would have been relatively low. Therefore, in future developments of TCM departments in Internet hospitals, a comprehensive collection and analysis of the four diagnostic indicators along with the development and improvement of related auxiliary diagnosis and treatment products (such as electronic nose/electronic olfactometry, pulse diagnostic instrument, and other related products), and the application of information technology (IT) are necessary to advance Internet-based diagnosis and treatment. 39
Endocrinology and nephrology departments required biochemical examinations to determine endocrine and renal function. Moreover, similar to challenges faced in the TCM department, the diagnosis and provision of treatment plans using Internet-based consultations was challenging, resulting in a highly standardized consultation mode. The diagnostic and treatment characteristics of the relevant diseases would affect patients’ expectations and behavior in medical visits, resulting in a lower overall number of visits to the departments in the second mode than in the first mode. Moreover, the visits were more dispersed temporally, that is, the change speed was relatively low.
The number of diagnoses and treatments in departments with low change speed and a large magnitude of change was relatively small, and the data showed relatively scattered visit times, resulting in relatively slow interaction. Owing to these departments’ discipline and disease characteristics, it was difficult for both departments to perform online consultations and to use their main diagnostic tools online; therefore, physicians appeared to make more adjustments during the online consultations compared with their offline consultations, exhibiting a higher level of standardization of consultation modes. Physicians often recommended patients to consult with them offline after the COVID-19 pandemic had subsided. Therefore, intelligent peripheral products that can overcome temporal and spatial limitations are a possible way to optimize Internet-based treatment in related departments.
Mode 3: convenient and fast interaction, and high standardization level of diagnosis and treatment mode
The gastroenterology and thoracic surgery departments demonstrated mode 3 characteristics, in which the rate of change was higher than the mean, that is, the speed of convenient interaction was faster. Moreover, the magnitude of change was lower than the mean, that is, the pattern was more standardized. The gastroenterology department was selected for detailed analysis below.
During the COVID-19 outbreak, in addition to lung-related symptoms, gastrointestinal and liver-related symptoms were also important manifestations in infected patients, which may even precede the respiratory symptoms. Symptoms of taste disturbance were also observed in a large number of infected patients. Digestive diseases, especially gastrointestinal diseases, are common diseases with high demand for treatment. The possible gastrointestinal symptoms of COVID-19 and the subsequent panic owing to the pandemic have been reported to have increased the volume of Internet-based diagnosis and treatment in gastroenterology.40–42 Moreover, Internet-based diagnosis and treatment were feasible in the medical practice of the gastroenterology department. Internet-based diagnosis and treatment can be undertaken through remote management and continuous care of common and chronic diseases in gastroenterology, such as inflammatory bowel disease, functional gastrointestinal disease, and chronic liver disease, and may even improve the quality of related medical services.40,43–46 For diagnostic effectiveness in gastroenterology in terms of the distribution of diagnostic symptoms, the main clinical diagnostic symptoms in new patients seen through the Internet medical platform and face-to-face consultations were abdominal pain and constipation/diarrhea, which presented little variability. 47 In terms of the diagnostic process, Internet-based medicine was able to substantially reduce the need for face-to-face consultations in relation to gastrointestinal diseases, and a large number of Internet-based medical consultations for gastrointestinal diseases were completed within 20 min. The above findings confirmed the practicability of Internet-based medical consultation in gastroenterology and the effectiveness of diagnoses.40,48 When making a diagnosis in the gastroenterology department, simple abdominal palpation may be performed via text or image guidance in Internet-based diagnosis, which may provide certain references to facilitate a physician's diagnosis and may differ somewhat from the high technical requirements of relevant tests in departments such as endocrinology. Gastroenterology was more suitable for online diagnosis and treatment based on the characteristics of the discipline itself, and the mode was highly standardized.
The number of consultations in the thoracic surgery and gastroenterology departments was high and consultation times were concentrated. Moreover, the physicians’ online response and consultation reaction times were faster, showing a highly convenient interaction. These departments were relatively suitable for online diagnosis and treatment in terms of the disease characteristics and the treatment process. Moreover, the mode was highly standardized, which enabled rapid resource allocation and switch of treatment methods to adapt to the online treatment environment and respond more efficiently.
The demand for Internet-based medical care was influenced by the disease characteristics and was driven by the COVID-19 pandemic. Given the background of normalized prevention and control of COVID-19 and IT development in the post-pandemic era, the development of Internet hospitals has become an inevitable trend. Some disease types are more suitable for Internet-based diagnosis and treatment, and can be diagnosed accurately online. However, it was difficult for some departments to fully rely on online communication for diagnosis or greater adjustments were required compared with face-to-face consultations. Therefore, for specific departments, decisions on whether to strengthen the development of Internet hospitals and provide more professional and personalized online diagnosis and treatment, or whether to focus on coordinating online and offline visits more effectively, should be based on the feasibility and effectiveness of the online diagnosis and treatment in the respective departments. According to our research, in the process of carrying out Internet diagnosis and treatment, hospitals should give priority to developing departments suitable for Internet diagnosis and treatment such as ophthalmology and neurology, continuing to explore the rules of Internet-based medical services and accumulate experience in Internet-based medical services, and then gradually open to other departments.
Challenges and future directions of the development process of Internet hospital
Limitations and challenges of the Internet hospital
Utilization of Internet hospitals is developing but is not without potential challenges and limitations. Internet healthcare faces the some challenges. Disparities in regional development, including varying economic conditions, levels of technical expertise, and uneven distribution of medical resources may impede certain regions from providing effective online medical services, as they lack essential resources and technical support. Secondly, data security concerns, as Internet healthcare involves sensitive information such as patient personal data and medical records, requiring measures to ensure data integrity, security, and privacy. Also, certain departments rely on physical examinations, posing a risk of inaccurate diagnoses. Doctors also have offline responsibilities for diagnosis and treatment, sometimes difficult to ensure real-time online consultations, and the delayed response times may adversely impact the patient experience and satisfaction.
In light of these challenges and limitations, more systematic and comprehensive strategies are needed to enhance the deployment and usability of Internet hospitals.
Development directions of the Internet hospital operation
The use of emerging technologies offers promising prospects for Internet hospitals which may effectively improve performances of Internet hospitals. Besides facilitating resource allocation and reducing costs, telemedicine platforms can facilitate interaction and consultation of doctors across regional health sectors and benefit from artificial intelligence to aid clinicians in diagnoses and personalized treatment plans. Remote monitoring devices, such as wearables, enable real-time health tracking for conditions like sleep disorders. Advanced image analysis technology enhances diagnostic capabilities for online consultations, such as using tongue image analysis for remote TCM diagnosis. 49 The integration of image recognition algorithms and artificial intelligence opens up more possibilities for remote diagnostic methods, and with the continued development and application of visual analysis technique or monitoring equipment may, more departments suitable for online medical services, while also improving diagnostic accuracy.
Limitations and future research directions
This study had some limitations.
First, we collected and analyzed patient data of online text consultations from the SAHSYSU Internet hospital from January to December 2020. The research would be enriched if there were multiple types of doctor–patient consultation data, but since SAHSYSU Internet hospital only opened text consultation, we could not get relevant data such as video or telephone consultation. In the future, it would have been helpful to obtain sufficiently large patient data from the Internet hospital prior to the COVID-19 outbreak (pre-January 2020) and during the later COVID-19 era (post-December 2020) to better discuss the characteristics and effectiveness of Internet hospital-based diagnosis and treatment in China, thus providing better solutions for improving service quality.
Second, only diagnosis and treatment data obtained from the Internet hospital were analyzed. In future studies, the actual online and offline conversion rate of Internet hospitals may be investigated through a comprehensive analysis of Internet hospital data and offline medical services after 2020 to provide more solutions for the improvement of Internet hospitals in the post-COVID-19 era.
Third, the SAHSYSU is a comprehensive modern scientific medical hospital. The diagnosis and treatment mode as well as service type of modern scientific medical hospitals differ from those of TCM hospitals. The conclusions obtained in this study may not be fully applicable to clinical practice in TCM hospitals. Relevant research on the characteristics and patterns of Internet-based diagnosis and treatment in TCM hospitals may be conducted in future.
In addition, exploring the potential of incorporating advanced technologies such as artificial intelligence image analysis into Internet hospitals to improve the level of remote diagnosis and treatment is also a feasible research direction.
Conclusions
The COVID-19 pandemic provided the impetus and the need to develop Internet hospitals, which are still required in the post-COVID-19 era to improve the quality of healthcare services. This study presented the practical experience of an Internet hospital based on a tertiary general hospital in China, and discussed the characteristics and advantages of Internet hospital services in time and space. Moreover, this study explored the characteristic modes of Internet-based diagnosis and treatment in different departments, and demonstrated the effectiveness of Internet hospitals in providing continuous and multidisciplinary medical services. With ongoing IT development, the further improvement of Internet hospitals has become an inevitable trend in the post-pandemic era. This study may provide references and lessons for general hospitals in the construction of Internet hospitals and improving medical services in response to the current medical demands or possible future pandemics.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241228418 - Supplemental material for Internet hospital response to the COVID-19 pandemic in a tertiary hospital in China: Perspectives based on a mixed-methods
Supplemental material, sj-docx-1-dhj-10.1177_20552076241228418 for Internet hospital response to the COVID-19 pandemic in a tertiary hospital in China: Perspectives based on a mixed-methods by Xiaolong Wu, Yulin Kuang, Yonglin Guo, Ji Wu and Li Xiao in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank the doctors of the Seventh Affiliated Hospital of Sun Yat-sen University for their help and guidance in this study.
Contributorship
XLW and YLK wrote the first draft of the manuscript. All authors were involved in drafting the manuscript and agreed to its publication. All authors read and approved their sections of the final manuscript. YLG, WJ, and XL read and approved all sections of the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Institutional Review Board/Ethics Committee of the hospital.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China, Science Fund for Distinguished Young Scholars of Guangdong Province, Natural Science Foundation of Guangdong Province, Guangdong Office of Philosophy and Social Science (grant numbers 72202244, 72322020, 72071218, 2023B1515020073, 2023A1515010667, Grant GD23YGL42).
Guarantor
XLW.
Informed consent
Informed consent was obtained from all interviewees before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.