
Abstract
Background
The Saudi government and the MOH launched six mobile application help in tracking positive cases, get medical consultation from home, and vaccination for coronavirus disease 2019 (COVID-19). Our study was conducted to evaluate the role of mobile health applications in the prevention and detection of pandemic disease from population perspectives.
Methods
A cross-sectional descriptive exploratory research design was utilized in this study. Based on the sample size calculation (described below), we recruited a convenience sample of 462 participants from the Northern Border Region according to the set of inclusion and exclusion criteria: Anyone over 12 years of age, including both genders and both Saudi citizens and non-Saudi citizens, were eligible to participate during the period from March 2022 to the end of July.
Results
In total 462 were participated, and 79.2% of them were females. There was a statistically significant difference between educational level and the overall score of public satisfaction with the ease of use of mobile health applications as well as overall satisfaction with the services provided by mobile health apps during the COVID-19 pandemic. Additionally, there was a statistically significant difference between gender and the role of mobile applications in the prevention of COVID-19 (p = 0.028).
Conclusion
The study found that most participants agree that the mobile health applications launched by the Saudi government and Ministry of Health have been successful in aiding the anticipation and early detection of COVID-19 cases, as well as facilitating access to healthcare services. Over half of the participants strongly agree that these mobile applications have been very effective and beneficial for their health and have helped save time.
Introduction
Coronavirus disease 2019 (COVID-19) is a pandemic disease that has disseminated around the world. It causes a variety of diseases mainly transmitted by droplets; the severity of the disease varies from a simple cold to severe pneumonia. 1 All countries are suffering significantly from the COVID-19 pandemic and all countries are suffering from this crisis in all respects: social, economic, spiritual and environmental. 2 The first verified patient of the COVID-19 pandemic in Saudi Arabia was detected on March 2, 2020. Thereafter, the number of confirmed cases and their contacts has increased in the following countries. There are 307,479 confirmed cases of COVID-19 and 3649 deaths from COVID-19.3,4 The government must take immediate and resolute preventive measures to minimize and control the spread of the disease. 5 In addition, the country has increased diagnostic testing, precautions and preparedness procedures to prevent the spread of the disease for all residents in the country, either Saudi or non-Saudi, resulting in 280,143 recoveries during that period. 3
One of the first countries that expected the threat of COVID-19 is Saudi Arabia and started protective and preventive measures. Together with the continuous effort to maintain public health, an assuring letter from the Custodian of the Two Holy Mosques, King Salman bin Abdulaziz Al Saud, Ruler of the Kingdom of Saudi Arabia, was directed to the community. Their exact words were, “We are living through a difficult period in world history, but we are fully aware that it is a period that has ended despite its cruelty, bitterness and difficulty, Saudi Arabia, remains to take precautions to deal with this pandemic and limit its effects.” 3
The Saudi government employed extreme measures to control the spread of COVID-19 among its citizens. This includes imposing nationwide restrictions, closing all schools and universities, and prohibiting domestic and international travel; installing thermal cameras in public places to facilitate in the detection of suspicious cases; and providing free vaccines not only to citizens but also to residents.6,7
Even with the remarkable measures taken to limit the epidemic, the accomplishment or failure of these efforts is greatly dependent on how the population behaves. Limiting the transmission of COVID-19 and protecting communities requires the involvement of every member of every community to act and prevent transmission. People's behaviors, and their willingness and ability to follow public health and social measures, continue to be the most powerful means to stop the spread of the virus. 8 The Saudi Ministry of Health immediately increased people's awareness and encouraged the following of precautionary measures, most importantly enhancing the importance of the population to maintain social distancing and launched several continuous educational programs and campaigns, health tools. Furthermore, with the widespread availability of technology, it has become necessary to collaborate with health organizations to promote first-level prevention. Creating an application that helps track cases, help decrease contact with infected individuals and be the connecting link for spreading awareness and safety measures between the individuals and the health minister using social media and various platforms. 9
In the 21st century, technology has become a crucial part of our daily lives. In the face of the pandemic, technology and science were able to collaborate and develop applications that help circulate and exchange data in the network. The government, residents, health workers, and other officials incorporated to monitor the pandemic and improve decision-making in various aspects of life. 10 The Saudi government and the Ministry of Health launched six applications, namely: Tabaud, Sehhaty, Tawakkalna, Tetamman, Sehha, and Mawid. These mobile application helps track positive cases, get medical consultation from home, and enables an easier and faster way to book appointments for PCR tests and vaccines for COVID-19.11,12
The Tawakkalna Application is an application launched and developed by the Saudi Data and Artificial Intelligence Authority (SDAIA) to support government efforts directed at managing COVID-19. 13 Initially, the goal of this application was to monitor individual movement using GPS, electronically demand movement license during curfew period, investigate own violations, and report other individuals such as large meetings that could increase the risk of disease spread. The app enabled displaying the user's medical appointment and reviewing the latest health news and updates about the spread of the disease and raising awareness for ways to prevent it. In the case of the infected individual, the ministry of health keeps up with their condition by frequently answering health-related questions.
Nowadays, as we cautiously return to normal life, Tawakkalna becomes a broader application to use and includes more aspects of life, for instance, Hajj and Omrah license. Furthermore, the dashboard enables users to view their personal and driving license and vehicle information, book COVID-19 vaccine appointments and health passports that confirm that the person has completed his COVID-19 vaccination; also, the visitor manual check-in, which is used in all public and private settings, QR-coded to check visitors’ health status. 13 The most important application that was also launched by the Saudi SDAIA with the cooperation of the Ministry of Health is the Tabaud application. The app notifies those who are in contact with a registered infected person during the 14 days prior, confirming the infection using Bluetooth. The application sends notifications while maintaining the full privacy of users. 13 Sehhaty is an application that allows users to have access to their health information and provides various health services for all individuals in Saudi Arabia. These services include testing for COVID-19, appointment booking, instant consultation service, medicine search and medicine list, sick leave, e-prescription, infection prevention and control, dependent service, and school screening. 14 The Tetamman application (Tetamman means rest assured) is one of the MOH applications to prevent COVID-19 and control its transmission by reinforcing the commitment of all persons directed to self-isolation or quarantine and follow-up their cases. Maintaining protection and health care by providing medical assistance such as direct contact with 937-Service Center to ask for help, COVID-19 test results, daily symptom check-up, and count down indicator for health isolation. 3
Seha is an online health application that provides simple and sustainable solutions to enable individuals to receive health care and prevention at home, provide medical services through consultation audio-video healthcare made by experts of the Ministry of Health and through artificial intelligence technology, allowing users to obtain safe medical information. 14 Also, the Mawid apps developed by the Ministry of Health allow patients to book, modify, or cancel their appointments in primary healthcare centers.14,15
The specific nature of the COVID-19 pandemic requires strong coordination of connected data, people, systems, and the public health agencies, epidemiologists, and government use different systems, data formats, or standards, which made the ability to identify trends and develop interventions against the pandemic harder. 16 In this challenging time, the use of technologies to combat the pandemic has raised challenges in many aspects. 17 Mobile health (mHealth) applications can offer information about the population and their movements that helps to understand COVID-19 tendencies and respond accordingly. The collected data through this application is helpful in contact tracing, cluster identification, and observation of quarantine. During the COVID-19 epidemic, various useful technologies were created to aid in the prompt identification and screening of infected people. Mobile phones, which are incredibly common devices and an information gateway, allow people to update their knowledge and make better decisions in the interim. Smartphones can be used to track people and examine the keywords they use to self-diagnose, as well as to install helpful apps that help detect infected persons. Numerous technical and review studies have examined smartphone applications for COVID-19 management. Many studies have examined various mobile applications that are used to assess the opportunities, challenges, issues, and lessons associated with using these devices to manage diseases.18–20
Despite the importance and effectiveness of these applications, the spread and use of these applications depends greatly upon population awareness and behavior, which are affected by data privacy concerns. Assessment of public perception about the mHealth applications’ role during the COVID-19 pandemic is very important in providing direction for future health care crises and pandemics and helps in improving the services of these applications. By the time of the study, no research has been conducted to evaluate public awareness about mHealth apps in Northern Border Region, Saudi Arabia. The current study was conducted to explore the role of mHealth applications in the prevention and detection of pandemic disease from a population perspective. The following research objective was assessed: first: in the Northern Border Region, the public's perception of the role of mHealth apps in the prevention and detection of the pandemic has been assessed. The second objective is to identify the level of public satisfaction with the role of mHealth applications and their services produced by the Ministry of health. The third one is to explore the challenges and problems hindering the users of mHealth apps. The researcher was examining the following research questions as follows: First what is the level of public perception and satisfaction with the role of mobile apps in the anticipation and recognition of the pandemic disease in the Northern Border Region? The second research question is What are the challenges facing individuals in the northern border region regarding the use of mobile apps.
Methods
Design and sample size
A cross-sectional descriptive exploratory research design was utilized in this study. The study was conducted in the Northern Border Region and related cities in Saudi Arabia during the period from March 2022 to the end of July. Based on the sample size calculation (described below), we recruited a convenience sample of 462 participants from the Northern Border Region according to the set of inclusion and exclusion criteria: Anyone over 12 years of age, including both genders and both Saudi citizens and non-Saudi citizens, were eligible to participate. The sample size was calculated based on the formula z2 pq/d2. In this formula, p is the expected prevalence, q is 1 - p, and d is the margin of error at 5%. The factors which were considered while calculating the sample size were the prevalence (p) = 50% as there was no previously relevant published study that was done in the northern border region and to give the maximum sample size, the power of the study as 80%, and the z score of 1.96 is equated to a 95% confidence level in a two-sided test. Considering the above factors with the anticipated 20% non-response rate, the total sample size was calculated as 462 (385 + 20% × 385). Respondents were invited to voluntarily fill out the online questionnaires through social media (such as WhatsApp, Twitter, etc.). After that, the snowball sampling technique was used, where the participants were asked to forward the survey link to their friends and colleagues using a note in the message attached with the survey link.
Instruments and questionnaire
One tool was used for data collection namely: society's perception and satisfaction with the role of mobile applications in the prevention and early detection of COVID-19 cases structured questionnaire. The researchers developed a self-administered web-designed questionnaire after reviewing related literature.21,22 The tool included four parts. Part I: socio-demographic characteristics of the participants, including age, gender, education level, nationality, marital status, region, and occupation. Part II: contains questions related to society's perception about mobile applications produced by MOH during the COVID-19 pandemic. They addressed general questions about the Ministry of Health's various types of mHealth apps, the role of mobile apps in COVID-19 prevention and detection, and their thoughts on the persistence of these apps after the crisis. The respondent was asked to respond to every question in the form of “Yes or No.” Part III: This section covers questions related to benefits, satisfaction, and the ease of use of mHealth applications produced by MOH during the COVID-19 pandemic. The questionnaire covered questions related to how easy it is to use this application, whether you need help to use the application, whether the information of the app is well organized, and whether the app helps in the detection and prevention of the spread of COVID-19. The respondent was asked to respond to every question in the form of a 5-point Likert scale (5 = strongly agree, 1 = strongly disagree). Part IV included open-ended questions about the challenges and barriers for mobile application use and utilization.
Reliability and validity
The researchers took important steps to establish the validity and reliability of the survey instrument used in the study. The validity of the developed survey was verified, and the researchers reviewed the translation to ensure accuracy. The researchers established, translated, and adapted a data collection tool and tested its validity with five nursing experts in the field of pediatric and community health nursing to assess the content validity of the instrument. The questionnaire is sent to the expert via E-mail. The experts provided feedback on the relevance, comprehensiveness, and clarity of the survey items, ensuring the tool accurately measured the intended constructs. A test of reliability was performed using Cronbach's alpha, which yielded an alpha coefficient of 0.83, indicating good internal consistency reliability.
Pilot study
Prior to the primary data collection, the researchers conducted a pilot study with 46 participants, which equated to 10% of the total study sample. The purpose of this pilot phase was to assess the feasibility, applicability, and clarity of the survey tool within the specific research context. Since the pilot study did not involve any interventions and was solely focused on validating the questionnaire's suitability, the researchers include these 46 participants as part of the overall study sample. This approach was taken because the pilot participants did not report any concerns or issues regarding the questionnaire, ensuring that their responses remained unaffected by prior familiarity with the instrument. The researchers believe that the inclusion of the pilot study participants does not introduce bias or compromise the integrity of the data collected. This conclusion is based on the relatively small size of the pilot sample in comparison to the primary study sample, which minimizes the potential impact on the overall results.
Ethical considerations
Ethical consent form was issued from Northern Border University with the following number (HAP-09-A-043) with decision number (4-91443 H) April 5, 2022. Prior to enrollment study and, after explaining the purpose of the study, the participants provided written informed consent at the beginning of the questionnaire. Given that the study included a subset of minor adolescents aged 15 to less than 20 years, who represented (15.58%; n = 72) of the total sample, additional measures were taken to ensure ethical compliance. Specifically, written informed consent was also obtained from the parents or legal guardians of these minors prior to their participation. This process involved providing detailed information about the study, including its objectives, potential risks, and benefits, to ensure that guardians could make an informed decision on behalf of their children. The consent forms were designed to be easily understood, and participants were encouraged to ask questions to clarify any uncertainties. This dual consent process underscores the commitment to ethical standards in research involving vulnerable populations, ensuring that both the minors and their guardians are adequately informed and consenting to the study's procedures. After completing the informed consent form, the participants had access to the questionnaire questions and could complete the research questionnaire. Participants are informed that all information is encrypted, and confidentiality has been considered.
Data collection
Data collection was done electronically through an online questionnaire. The researcher shared links with people using various social media platforms and community networks after explaining and clarifying the purpose of the study and drafting the purpose and consensus and intention to participate in a Google survey. The researchers announced the study's goals and provided a link to the questionnaire in an announcement shared on Facebook, Twitter, and WhatsApp groups among the students, colleagues’ administrators and all groups in the Northern Border region to participants. At first, the researchers used convenience sampling by sending out direct invitations to students, colleagues, administrators via these organizations. Then the researchers used snowball sampling tactics to increase the reach of our outreach by asking the participants to share the study link with their groups & families and so enable a wider circulation of the questionnaire.
Statistical analysis
The computerized statistical package STATA/SE version 11.2 for Windows (STATA Corporation, College Station, TX), and MS Excel were used for data entry, presentation, and analysis. Descriptive statistics, mean ± standard deviation (SD), and frequency and percentage, were used to summarize data as appropriate. The distribution of numerical data was examined using the Shapiro–Wilk W test. The Chi-squared test and the Fisher exact test (FET) were used to detect differences in categorical data and the Kruskal–Wallis test and the Mann–Whitney test were used to detect differences in continuous variables. Multiple linear regression analysis of participants’ ease of use, benefits, and satisfaction of MOH applications was carried out to identify significant predictors. Statistical significance was accepted at p < 0.05.
Results
Table 1 shows the demographic characteristics of the participants. The total number of participants in the study was 462. 79.2% of them were females (n = 366). More than one third (n = 167, 36.15%) of participants in this study were under 30 years old, with a mean ± SD of 31.50 ± 12.30. Most participants were Saudi (76.2%, n = 352). Regarding educational level, approximately two thirds of participants had bachelor's degrees (n = 295, 63.8%).
Demographic characteristics of the studied participants.

Figure 1 shows the opinion of the population about the most common health applications that had an active role during the pandemic. The highest percentage was assigned to Tawakalna application from both male and female followed by Sehhaty application.

The most common applications that had active role during the pandemic according to gender.
Table 2 shows the public perception of mHealth apps and their role in the detection and prevention of COVID-19. According to Table 2 most participants agree with the applications launched by MOH to help in the inhibition and early discovery of COVID-19 cases with more females (96.45%) agreeing compared to males (90.63%) and the difference was statistically significant (p = 0.028). The most used mobile applications during the pandemic were Tawaklna (88.5% for females, 95.8% for males) and Sehhaty (50.6% for females, 55.2% for males). Most respondents (95.63% for females, 95.83% for males) preferred to have a comprehensive application that provides all the services, rather than multiple separate applications. When asked about the most suitable application to provide all the necessary services, Tawaklna was the most preferred choice across all age and gender groups. The statistical analysis (Chi-squared and Fisher's exact tests) shows that the only significant difference was in the usage of the Tatammen application, which was more prevalent among the 30–40 age group (p = 0.02).
Relationship between age, gender and society's perception and satisfaction with the role of mobile applications in the prevention and early detection of pandemics.
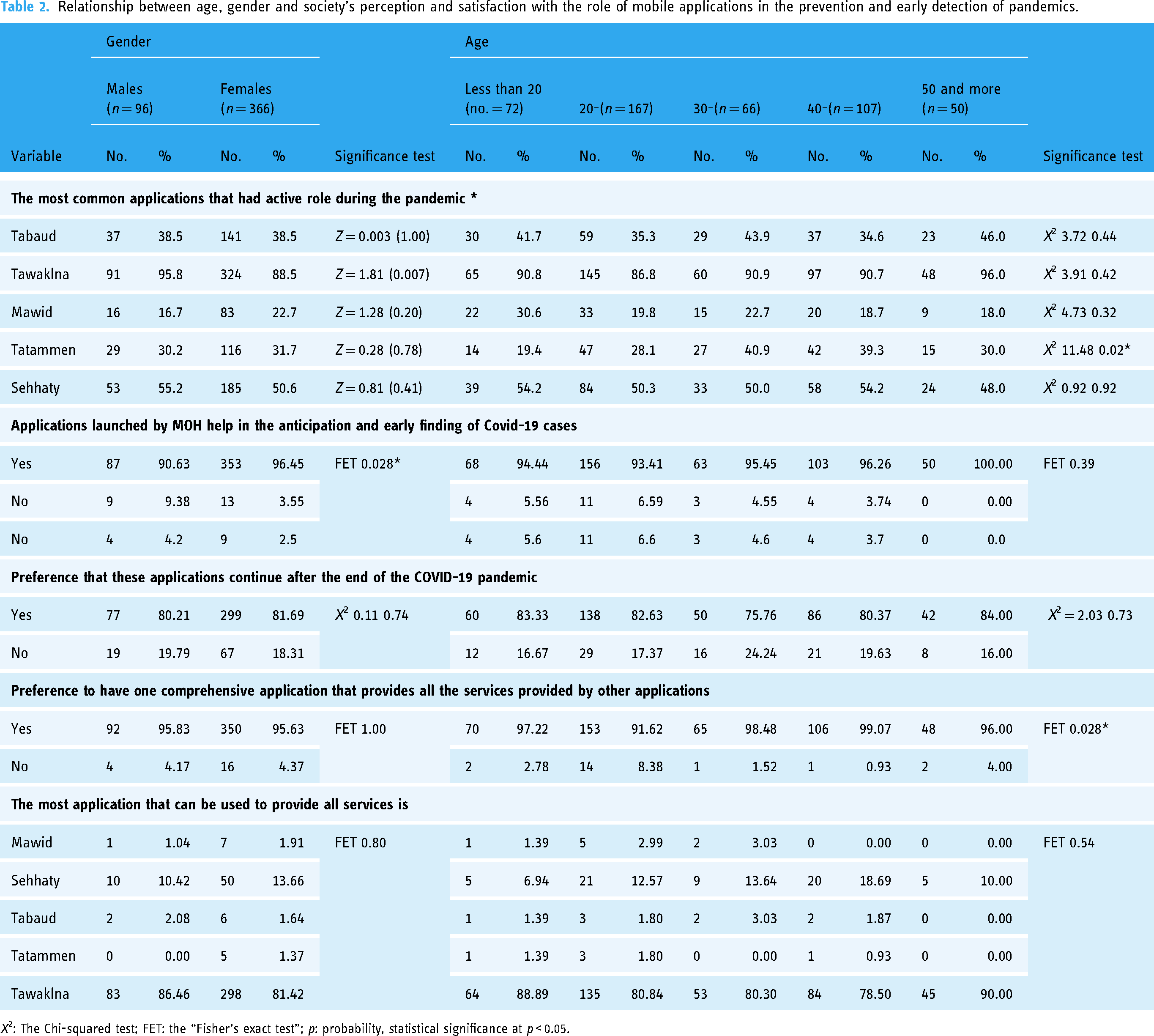
X2: The Chi-squared test; FET: the “Fisher's exact test”; p: probability, statistical significance at p < 0.05.
Figure 2 shows opinions of the population about the role of mHealth apps in facilitating access to health care. Most female and male participants from different age groups agreed that mHealth apps facilitated access to healthcare during the pandemic, with over 90% indicating the apps were helpful in this regard.

Opinion of the population about the role of mobile health apps in facilitating access to health care.
Table 3 shows public satisfaction with the ease of use and benefits of mHealth apps and their role in detecting and preventing COVID-19. It is obvious that approximately half of participants strongly agree that mobile applications launched by the MOH are easy to use, easy for all users to learn how to use them quickly, and the data in the app is well prepared, so they were able to use them easily (55.63%, n = 257 and 47.62%, respectively). However, a significant number of respondents (34.2%, n = 158) were neutral about whether they needed help using the applications. Regarding the benefits of mHealth applications, more than half of participants strongly agree that mobile applications launched by the MOH are very effective and beneficial for their health; more effective in saving time and fulfilled the purpose for which they were created (58.01%, 51.73%, and 52.60%, respectively). The overall scores for “ease of use” and “benefits” of the mobile applications were 24.37 ± 3.30 and 17.54 ± 2.57, respectively, indicating a generally positive perception among the public.
Public satisfaction with the ease of use and benefits of mobile health apps and their role in detecting and preventing the pandemic disease.

Figure 3 shows public satisfaction with the services provided by mHealth applications and their role in detecting and preventing COVID-19. There was generally positive opinion about the mHealth apps, with most respondents agreeing that the apps were created and responded quickly, had well-integrated functions, and that they plan to continue using them after the pandemic. However, some respondents 22.08% (n = 102) felt there were too many apps, making it difficult to quickly access information. In general, they were very satisfied with these apps, with the mean score of 23.89 ± 3.34.
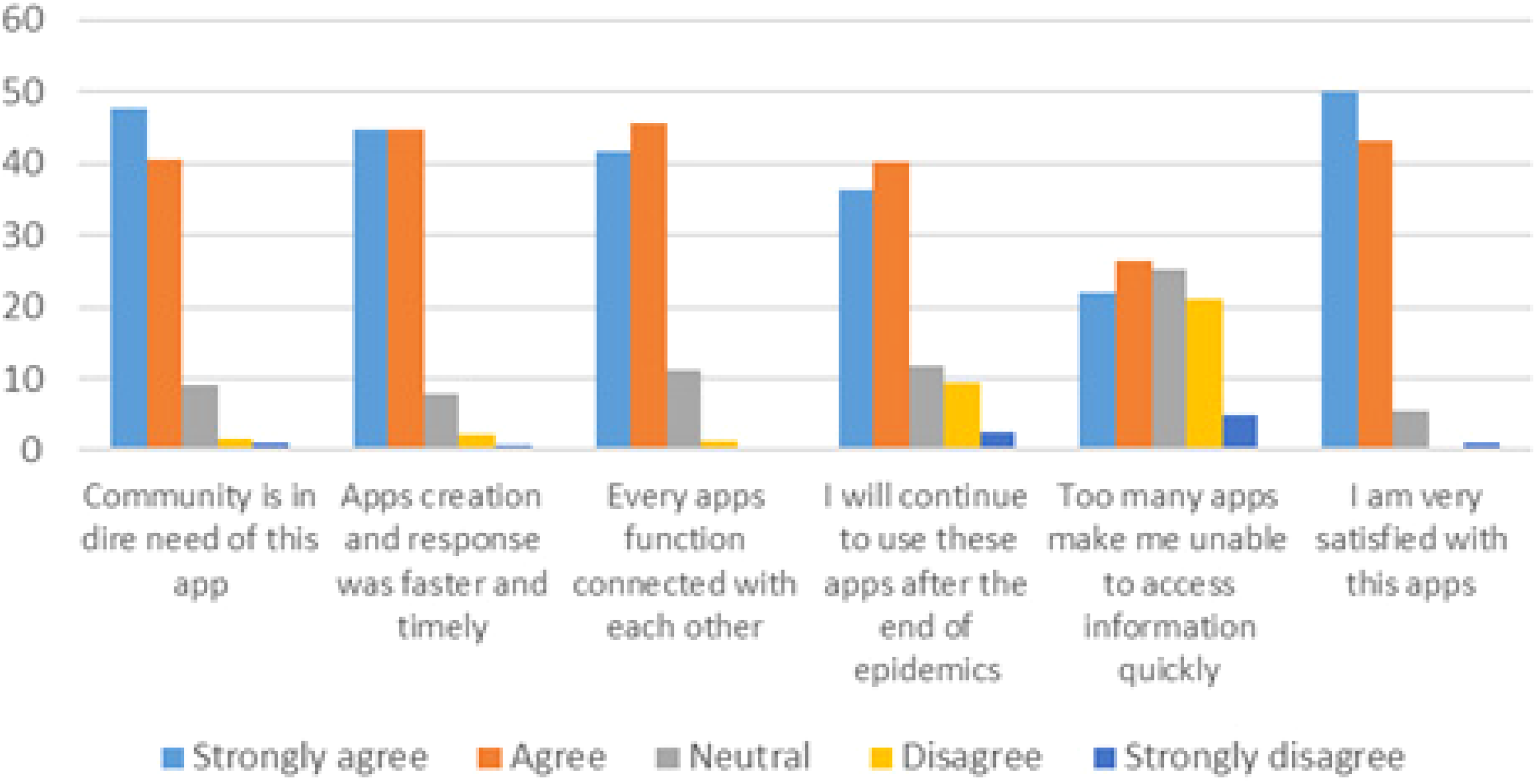
Public satisfaction with the services provided by mobile health applications and their role in detecting and preventing the pandemic disease.
Table 4 shows the relationship between demographic characteristics and public satisfaction with the mHealth application score. There was a statistically significant difference between educational level and the overall score of public satisfaction with the ease of use of mHealth applications as well as overall satisfaction with the services provided by mHealth applications during the COVID-19 pandemic (p = 0.001 and 0.005). There were no statistically significant differences in the “ease of use,” “benefits,” and “public satisfaction” scores across different age groups. Females had a slightly higher “ease of use” score compared to males (24.73 ± 3.18 vs. 23.95 ± 3.71), but the difference was not statistically significant.
Relationships between demographic characteristics and public satisfaction with mobile health application score.

Comparisons were carried out using the Mann–Whitney test or the Kruskal–Wallis test as appropriate.
* p < 0.05.
** p < 0.01.
Table 5 illustrates multivariate regression analyses between public satisfaction with mHealth application and their demographic characteristics. The table provides the regression coefficients (B), 95% CIs, and p-values for each independent variable. In the univariate analysis, age showed negative significant relation with ease of use indicating that younger individuals find these applications easier to use compared to older individuals. Compared to those under 20 years old, participants aged 20–30 (B = -2.55, 95% CI: −3.83 to −1.26, p < 0.001), 30–40 (B = -2.04, 95% CI: −3.18 to −0.89, p = 0.001), and 50 and above (B = -2.40, 95% CI: −4.02 to −0.79, p = 0.01) reported significantly lower ease of use scores. However, age was not significantly associated with perceived benefits or overall public satisfaction. The multivariate regression analysis revealed that nationality (Saudi vs. non-Saudi) and educational level (bachelor and postgraduate degrees) are significant predictors of public satisfaction with mHealth applications. This suggests that educational attainment and cultural factors play a significant role in the satisfaction levels. Gender was also a significant predictor, with females reporting higher ease of use compared to males.
Multivariate regression analyses between public satisfaction with mobile health application and their demographic characteristics

Discussion
Technology is the future and useful tool for early recognition of pandemic disease. This will be accomplished by creating apps that function as a reliable network between patients and healthcare professionals, allowing for condition monitoring. It can significantly impede treatment and proper health education while maintaining COVID-19 health precautions. The use of health applications has greatly expanded beyond the medical field to include all other life aspects. The current paper conducted a rapid review to assess the role of mobile applications in the prevention and early detection of pandemic disease from population perspective in Northern Border Region, Saudi Arabia. The results indicate the positive role that technology played in the prevention and detection of the COVID-19 pandemic in the community, as all participants agreed that the mHealth applications launched by MOH played an effective role in the prevention of COVID-19. Similarly, a study conducted by Montazeri et al. 23 reported that most healthcare professionals believed that mHealth technology could contribute to the prevention and self-care of COVID-19. They further believed that the use of mHealth technology could be helpful in the prevention, treatment, and diagnosis of COVID-19. Various studies have shown that hat digital technologies provide a unique opportunity to enhance the diagnosis and management of infectious diseases and can be used in the management of various stages of COVID-19 disease, including monitoring and screening patients with early signs of COVID-19 before referral to hospitals and prevent COVID-19.24–26
Accordingly, the Tawakkalna application was the most common application utilized by participants during the period of pandemic, and most participants replied that they preferred the Tawakkalna application to be a more comprehensive application that could offer services provided by other applications. The use of mHealth apps, especially Tawakkalna, has increased for a variety of reasons, including the fact that during the COVID-19 pandemic, the Saudi government has imposed a regulation a major decree prohibits anyone from entering a medical facility, school, workplace, shopping or any other place in the kingdom without first showing their status in Tawakkalna. Other reasons could be the continued growth of these apps led by the Saudi Ministry of Health and Data and Artificial Intelligence, as well as good internet access and connectivity in Saudi Arabia. This result was consistent with Aldhahir et al., 27 who reported in his study that for respondents who stated not using the Seha app, the Tawakkalna app was the most employed health app provided by the MOH.
mHealth technologies have been recognized as a more affordable and accessible approach to delivering high-quality healthcare services to patients in low- and middle-income countries (LMICs) with fragile health systems, high prevalence of tropical diseases, high rates of infectious diseases, and high mortality rates. 28 While mHealth activities are predominantly found in high-income countries (HICs) for transforming healthcare, there has been a rising trend in the integration of mobile health into the existing eHealth services in LMICs The exponential growth in mobile phone penetration and acceptability in LMICs suggests that utilizing mobile phones for healthcare services could be a promising strategy to address the healthcare challenges in these resource-constrained settings. 29
In relation to public satisfaction with ease of use and benefits of mobile applications, this study illustrated higher satisfaction as most participants agreed that mobile health applications launched by MOH are easy to use, effective in saving time and help them in the management of their health and health problems effectively. Similarly, Alanzi et al. and de Veer et al.,22,30 in their study found that >60% of participants replied that they would use e-health apps. Furthermore, variances were identified between young and old male and female perceptions in terms of ease of use and satisfaction with mobile health apps, indicating that diverse genders and age groups have different levels of skills and capabilities in using the app and therefore have differences in their attitudes.
Our results show that gender and education level have a significant relationship with usage patterns and satisfaction with mobile health apps. Female users access mobile health apps more often than male users. This highlights the psychological differences between the sexes regarding telemedicine implementation and motivations for its use, which have been discussed in the previous literature. Similar results were represented by Alam et al. and Zhang et al.,31,32 this suggests that people with less education are less likely to use telemedicine. Therefore, the Ministry of Health needs to be more sensitive to people, especially those with low education. A study conducted by Gallagher et al., 33 reported that age and education were important influences on technology use. Younger and more educated patients were more likely to use mobile technology and to do so for health reasons, as well as to use apps, especially, if they were employed.
Additionally, Aldhahir et al., 27 reported in their study an increase in user satisfaction with the services provided in the app. This is reflected in the frequency of use and has promising implications for other medical applications. In his research, he also suggested that we should measure consumer satisfaction with other mobile health apps we did in our research. This can be attributed to the growing awareness among individuals and social networks about mobile health apps and their role in the prevention of the COVID-19 pandemic.
The study results suggest that a relatively small percentage of participants reported facing problems while using the mHealth application. These problems included difficulties in accessing the required information due to the variety of available applications, network issues, and challenges in using the mHealth applications. This finding is anticipated, particularly among older individuals and those with lower educational attainment. Similar results have been discussed in the literature, which indicates that despite the growing interest in mHealth in recent times, access to mHealth applications remains a challenge that requires urgent attention. The research also reveals several potential challenges and barriers that hinder the implementation of mHealth for disease screening and treatment support in LMICs. These include geographical access and internet connectivity barriers, policy and regulatory barriers, limited awareness of mHealth applications, inadequate information and communication technology (ICT) infrastructure, limited healthcare worker competence in mHealth, funding challenges, poor architectural design, and a lack of standardization in LMICs. These findings highlight the need for concerted efforts to address these barriers and ensure the widespread and effective adoption of mHealth technologies in resource-constrained settings.34–37
Limitations and future work
Even though this study examines the role of mobile apps in controlling the COVID-19 pandemic in the Northern border region and provides insight into the phenomenon, it still has some limitations. Addressing these limitations will create opportunities for further research. Firstly, the scope of this study is limited to the Northern Border area and convenience sampling technique was used; Future research could uncover insights into mobile app usage during the pandemic for comparison across different countries with random sampling to represent all population in the same proportion. Second, due to the lockdown and social distancing, this study conducted an online survey. Other studies may conduct face-to-face interviews to better understand this phenomenon. Third, people's knowledge, experiences and perceptions can change over time; Future research may address this issue through longitudinal studies. Public perception of the availability and usefulness of mobile applications is an important factor. Anyone can use the mobile app if they are familiar with the service. To this end, the government must implement awareness and motivational programs so that the public realizes the usefulness of the applications and is attracted to their use.
Conclusion and recommendations
The study concluded that technology indeed played a positive and important role in the prevention of the spread of COVID-19 among the community and eased the adjustment of the new life modifications that it has caused. These applications also help in avoiding non-essential face-to-face contact between the healthcare provider and the patients while continuum to provide care and consult with the application, thus maintaining social distancing and avoiding virus transmission. The study found that most participants agree that the mobile health applications launched by the Saudi government and Ministry of Health have been helpful in helping to anticipate and identify COVID-19 cases early and facilitating access to medical care. Over half of the participants strongly agree that these mobile applications have been very effective and beneficial for their health and have helped save time.
The results also showed a statistically significant difference between educational level and the overall satisfaction with the ease of use and benefits of the mobile health apps, as well as the overall satisfaction with the services provided. This suggests that individuals with higher levels of education may have a more positive perception of mobile apps and their utility. Additionally, there was a statistically significant difference between gender and the perceived role of the mobile apps in COVID-19 prevention, with females generally having a more favorable view. The researchers recommend Longitudinal studies and comparative analyses across different regions & demographic groups to provide valuable information for enhancing the effectiveness of these technologies. Implement targeted educational and awareness campaigns to inform the public, especially those with lower levels of education, about the capabilities and benefits of mobile health apps. This can help improve overall utilization and satisfaction. Longitudinal studies could be explored in future research to monitor shifts in public opinion and usage trends of mobile health apps over time. Deeper understanding of the population's changing requirements and preferences allows for more adaptive and responsive health technology solutions.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076241292106 - Supplemental material for Role of mobile health applications in prevention and detection of pandemic disease: A population perspective
Supplemental material, sj-doc-1-dhj-10.1177_20552076241292106 for Role of mobile health applications in prevention and detection of pandemic disease: A population perspective by Amal Ahmed Elbilgahy, Mada Huwaydi Alenezi, Aseel Hamed Alruwaili and Sarah Muteb Alhathal in DIGITAL HEALTH
Supplemental Material
sj-doc-2-dhj-10.1177_20552076241292106 - Supplemental material for Role of mobile health applications in prevention and detection of pandemic disease: A population perspective
Supplemental material, sj-doc-2-dhj-10.1177_20552076241292106 for Role of mobile health applications in prevention and detection of pandemic disease: A population perspective by Amal Ahmed Elbilgahy, Mada Huwaydi Alenezi, Aseel Hamed Alruwaili and Sarah Muteb Alhathal in DIGITAL HEALTH
Footnotes
Acknowledgment
The authors gratefully acknowledge the approval and the support of this research study by the Grant No. (NURA 2022-11-1532) from the Deanship of Scientific Research at Northern Border University, Arar, Saudi Arabia.
Author contributions
AAE & SME conceptualized the research idea, prepared research tool, collected, organized and interpreted data. MHA and AHA writing the introduction, collecting data, prepare research tool, writing the discussion. All authors wrote initial and final draft of article and provided logistic support. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All generated data were included in this article.Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical consent form was issued from Northern Border University with the following number (HAP-09-A-043) with decision number (4-91443 H) April 5, 2022. Prior to enrollment study and, after explaining the purpose of the study, the participants provided written informed consent. Participants are informed that all information is encrypted, and confidentiality has been taken into account.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Northern Border University (grant number NURA 2022-11-1532).
Guarantor
Dr Amal Ahmed Elbilgahy (AAE).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.