
Abstract
Aims
The use of virtual care enabled by digital technologies has increased, prompted by public health restrictions in response to COVID-19. Non-hospitalized persons in the acute phase of COVID-19 illness may have unique health needs while self-isolating in the community. This scoping review aimed to explore the nature of care, the use of digital technologies, and patient outcomes arising from virtual care among community-based self-isolating COVID-19 patients.
Methods
Literature searches for peer-reviewed articles were conducted in four bibliographic databases: CINAHL, Medline, Embase and Cochrane Database of Systematic Reviews between January and February 2022, followed by hand-searching reference lists of included articles. Two levels of screening using defined eligibility criteria among two independent reviewers were completed.
Results
Of the 773 articles retrieved, 19 were included. Results indicate that virtual care can be safe while enabling timely detection of clinical deterioration to improve the illness trajectory. COVID-19 virtual care was delivered by single health professionals or by multidisciplinary teams using a range of low-technology methods such as telephone to higher technology methods like wearable technology that transmitted physiological data to the care teams for real-time or asynchronous monitoring.
Conclusion
The review described the varied nature of virtual care including its design, implementation, and evaluation. Further research is needed for continued exploration on how to leverage digital health assets for the delivery of appropriate and safe virtual COVID-19 community care, which can support patient recovery, control transmission, and prevent intensifying the burden on the health care system, especially during surges.
Introduction
The coronavirus disease (COVID-19) pandemic resulted in the implementation of a wide range of public health measures to control the circulation of the highly infectious virus.1,2 Individuals who tested positive for COVID-19 were ordered to self-isolate to prevent transmission of the virus; clearance from self-isolation was based on rapidly changing clinical management guidance. 3 At the height of the pandemic, case management and contact tracing were routinely conducted as part of infectious disease control practices. 4 However, much of the emphasis was placed on ensuring that the patient understood and complied with the quarantine order, rather than on well-being and recovery. Most recently, some jurisdictions around the world have begun easing public health restrictions such as modifying mask mandates and lifting legal self-isolation requirements.5–7 Despite the revocation of legislated orders to self-isolate, newly confirmed self-isolating COVID-19 patients may have unique health needs that warrant support provision beyond being given instructions to stay home. With virtualized health care advancing expeditiously across health systems, particularly related to preventing viral transmission and acquisition, there is potential for this modality to be integrated into COVID-19 care pathways.
The incorporation of digital technologies into health care, using information and communications technology, falls under the umbrella of digital health, 8 with which virtual care fits in. Recent literature describes a need for remote care to maintain health service provision when in-person visits are limited, 9 as well as, for continuity of care for populations such as diabetes, cancer, mental health, and obstetrics.10–13 A systematic review exploring telehealth's role during the COVID-19 pandemic finds that telehealth plays a key role in reducing viral spread while conserving health system capacity, even while the patient or provider has acquired COVID-19. 14 In response to the emerging need, jurisdictions across Canada have adapted physician billing, 15 similar to other countries such as the United States of America and Australia that have shifted policies to promote telehealth use.16,17
In contrast to hospitalized patients for acute COVID-19 treatment, asymptomatic persons or those who experience mild symptoms may have less care offered; however, the care for these individuals should not be neglected as appropriate medical interventions, and psychosocial and other supports are needed during the course of isolation. 18 For patients in the early phase of COVID-19 illness, telecare has the potential to effectively monitor for clinical deterioration and to provide at-home treatment. 19 COVID-19 and the rapid expansion of virtual care are both relatively novel; there may be gaps in knowledge about the use of virtual care for COVID-19 patients. A greater understanding of the range of virtual health services offered to self-isolating COVID-19 patients may improve their access to health care, contribute to monitoring for clinical deterioration, help to ensure compliance with self-isolation, and examine the overall quality of care during the active illness and isolation period.
Purpose and objectives
The purpose of this scoping review is to explore the nature and outcomes of health care services provided through virtual modality for community-based self-isolating COVID-19 patients and to identify gaps in the literature on the use of virtual care for this population. Objectives of this review include:
To examine the types of virtual health care services and supports that are provided to COVID-19 patients who are self-isolating in the community. To describe the technology that is utilized in delivering virtual care to COVID-19 patients who are self-isolating in the community. To describe who delivers virtual care, and for how long, to COVID-19 patients who are self-isolating in the community. To explore the COVID-19 patient outcomes arising from virtual care during the self-isolation period in the community.
Methods
This scoping review followed the methods outlined by the Joanna Briggs Institute including a comprehensive search of four databases, staged eligibility screening using two independent reviewers, data extraction, and analysis. 20 Details on the scoping review methods can be found in our scoping review protocol. 21
Search strategy
Information Sources. The following bibliographic databases were searched during the time period of January 30, 2022, to February 3, 2022: CINAHL, Medline, Emcare, and the Cochrane Database of Systematic Reviews. Subsequent hand-searching was conducted in Google Scholar and reference lists.
Delimiters, Keywords and Boolean Operators. Each search strategy was designed and implemented in consultation with a health sciences librarian to ensure appropriateness and comprehensiveness. For CINAHL, Medline, and Emcare databases, delimiters included English language and date range of the year 2020 to 2022. The CINAHL search was additionally limited to journal articles. Keywords and subject headings in various combinations including COVID-19, COVID19, Novel Coronavirus, Coronavirus, SARS-COV-2, 2019-ncov, cov-19, virtual care, telemedicine, telehealth, telenursing, telepractice, telecare, telemonitoring, mhealth, ehealth, digital health, remote monitoring, remote consultation, ambulatory monitoring, home monitoring, isolation, quarantine, positive, diagnosed and diagnosis were included. The Boolean operator OR was used for variations of keywords representing each of the concepts. The use of keywords for the search was adapted for each database; however, all searches followed a combination of virtual care AND COVID-19 AND quarantine AND positive. This refined combination was adopted after the initial searches using the two concepts of virtual care and COVID-19 yielded thousands of irrelevant references. Table 1 displays a summary of the sources and yield, and number of references that were screened-in after the completion of level 1 and 2 screening.
Summary of yield and results by eligibility screening.

Eligibility Screening. Two reviewers (LCL, CC) independently screened abstracts and full-texts using predetermined eligibility criteria for the inclusion and exclusion of references. Two levels of screening were used: level 1 applied to all titles and abstracts and level 2 applied to full-text papers that passed level 1. Any conflicts were resolved through discussion. We included articles that focused on the provision of health care interventions delivered virtually among persons with active COVID-19 and who were self-isolating in the community.
Studies were excluded if they (1) were not empirical studies, (2) reported on individual case studies or case presentations with n = 1 or 2, (3) discussed virtual care hypothetically or as recommendations rather than implementing a virtual intervention, and (4) did not focus on the patients but on caregivers or providers. Although virtual platforms have been documented to assist with surveillance, 22 diagnosis, 23 and contact tracing, 24 eligibility screening was applied to the references in an effort to remain within the scope of virtual care from the lens of care for the persons diagnosed with COVID-19. Figure 1 presents the PRISMA flowchart of the identification, screening, and inclusion of references for the review.

Flow diagram of databases, yield, and screening results.
Data Extraction and Synthesis. Data were extracted using a data extraction tool that the reviewers developed. Using this tool, the data were categorized for type and dose of virtual care, technology used, health discipline of provider, and patient outcomes. The data were then summarized and synthesized.
Results
A total of 19 articles met the eligibility criteria and were included in the review.25–43 A summary of the included articles can be found in the Appendix. Of the 19 relevant records, most were conducted in Australia (n = 6),25–30 followed by Canada (n = 4),31–34 the United Kingdom (n = 2)35,36, United States of America (n = 3),37–39 India (n = 1), 40 Germany (n = 1), 41 France (n = 1), 42 and China (n = 1). 43 Two Canadian studies were based on the same virtual program, however, separate data collection and analyses were completed.32,33 Three studies reported samples that included children.25,29,30 Some studies focussed specifically on special populations, including cancer patients, 42 perinatal patients, 38 patients with existing hypertension, 31 patients with immunological, pulmonary, or cardiac conditions, 41 patients with COVID-19 from under-served communities, 37 and patients with no family physician or have lost access during the pandemic. 32 The included articles reported a wide range of study designs. Some articles clearly stated their study designs such as prospective cohort 31 and observational descriptive, 32 while others were more ambiguous in articulating their designs. Sample sizes ranged from 46 to 7074 participants.31,39 No study reported any power calculation to determine sample sizes. Results, based on objectives of the review, were synthesized by types of health services and supports, technology, care provider, and patient outcomes.
Types of Health Services and Supports. All included studies provided some form of remote monitoring or virtual assessment; however, the nature and dose of these varied considerably. Symptom monitoring and assessment were the most common type of service in the virtual care basket, addressing the biomedical needs. Nine studies implemented a system to identify the risk and urgency based on the clinical presentation of participants such as a red-amber-green rating, 35 higher-risk and lower-risk classification25,26,28,32,34,36,39 and symptom severity, 38 which affected the frequency or timeliness of contacts with the health provider, or care model. While the monitoring of vital signs and bio-signals was offered by several studies, Michaud et al. 31 in particular, tested the feasibility of a self-assessment and self-monitoring model whereby participants themselves autonomously seek medical care based on a severity algorithm provided by the study. Six other studies relied on a provider-monitoring or patient-provider collaborative model for the review of vital sign and bio-signal values, and trends to advise when in-person assessment or ambulance were required.27,29,32,33,39,41 One feasibility study had a protocol for notifying the hospital when a patient was being transferred. 34
Furthermore, virtual health services and supports include the provision of health advice and patient education such as when to access emergency care, symptoms that signify clinical deterioration,25,34,37 and prevention of transmission and isolation requirements.32,37,39,42,43 Medication reconciliation or patient education about medication use were offered.28,32,37 Few of the included studies offered services and supports beyond the biomedical approach. Psychosocial supports were available either directly from the program or via a referral.28,29,33,42,43 Other services were also described, such as resource provision or linkages to community resources including grocery delivery or meal assistance,33,37,42 free personal protective equipment, 37 and peer connection with other COVID-19 patients. 43 Eleven studies also offered dedicated helplines, contact information, or similar safety system, whereby the patient can reach a provider directly, or message or page a provider when needed.26,28,29,32,34,36,39,40,42,43 Notably, research conducted in Australia and UK highlighted the use of “virtual wards” as an extended hospital service, using inpatient language such as admissions and bed days.28,30,35 However, these wards did not involve inpatient face-to-face admission; rather the ward provided virtual care remotely to patients in their homes or usual dwelling in the community.
The frequency of contacts with patients ranged from a low of only when initiated by the patient 36 to a high of up to three times daily 29 when there were synchronous interactions. When studies utilized automated vital sign monitoring, digital communication of health data by machine occurred up to fifteen-minute increments. 41 Table 2 outlines the variation in services and supports alongside the frequency of contacts.
Count of studies by types of services and supports, and frequency of contacts to patients.

Note: This table provides an overview of the number of studies offering each type of health service and support against the frequency of interactions. Some studies offered different levels of service for different groups of patients based on their virtual care protocol. The table is not intended for the counts to add up to the total number of studies included in the review.
The duration of the virtual care programming varied across studies with some specifying a minimum number of days such as 7 days 38 or maximum number of days such as 14 days.25,31,33 Other studies did not specify time frame parameters, where discharge relied for example, on symptom resolution, isolation clearance, or clinician judgment about recovery.26,28–30,32,34,35,37,39,41,43 Figure 2 summarizes the duration of virtual care.

Summary of duration of virtual care.
Technology. What and how technologies were used varied across studies. Where virtual care was delivered only by telephone between patient and provider, real-time communication occurred. However, virtual care programs, delivered with the assistance of digital technology such as a mobile application with built-in messenger function, enabled a combination of asynchronous and synchronous interactions. Table 3 presents a summary of the digital health technologies reported.
Summary of digital health technologies by study.

Web-based platforms or applications allowed for two-way online consultation visits. Video conferencing was substituted by telephone calls when patients did not have digital access33,34 or conversely, telephone calls were supplemented by video conferencing when escalation of care was required for visual assessment. 37 Where provider-patient interactions took place over video platforms, several studies’ remote monitoring also comprised the use of equipment for the assessment of vital signs for some or all patients.27,29,32,33 Distribution of pulse oximeters and thermometers to patients isolating at home was also common.27,29,32,33,36 Telemedicine or telehealth provided solely through telephone calls (without any other equipment) was the mode of health care delivery in five studies.,25,26,28,30,38 Usage of digital applications designed for health care, such as the digital platforms with patient and clinician portals were used.33,35 For example, Swift et al. 35 operated a virtual ward through a digital platform where patients could enter information which were then transmitted and displayed on the clinical dashboard for clinician monitoring. Applications leveraging social media networking platforms were also described in two studies.40,43 Both studies, based in Asia, optimized the messenger feature for text communication, as well as the telephone function within the social media networking platform.40,43 One of them also relied on the Cloud for completion of telemedicine form that gathered assessment information on the patient. 43
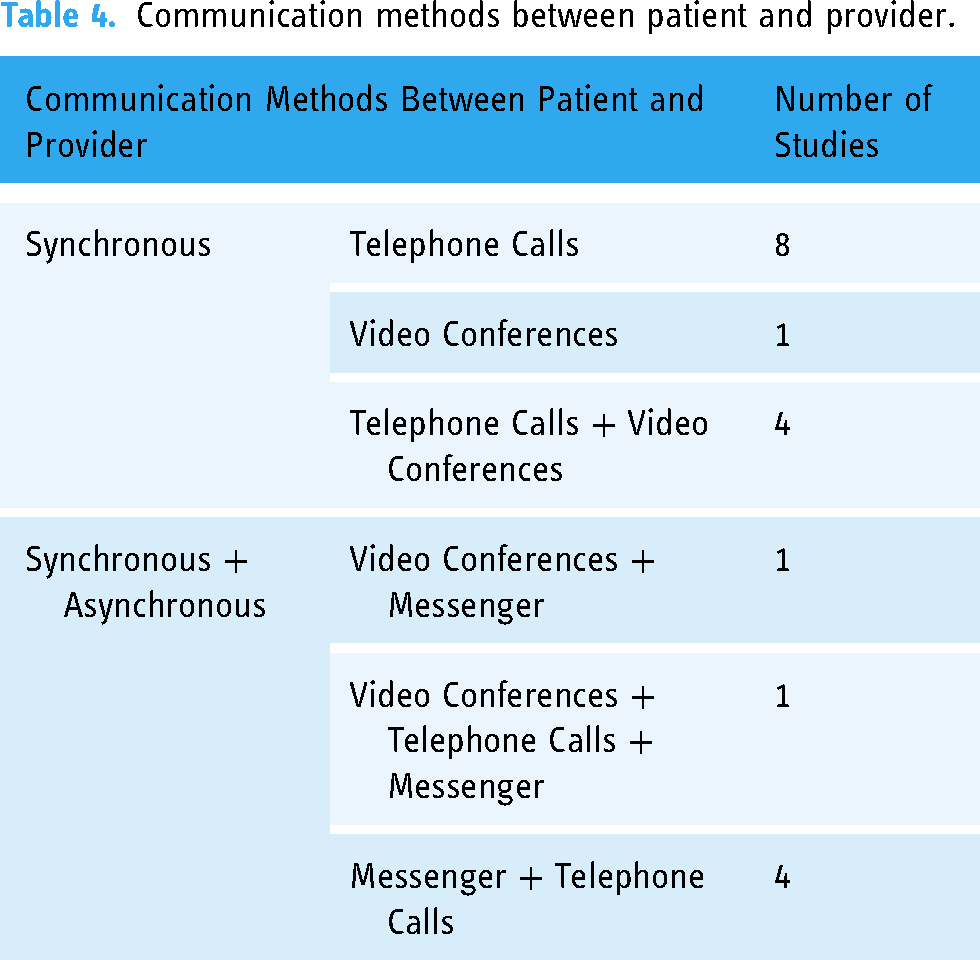
The deployment of wearables and equipment where vital sign data and bio-signals were transmitted electronically were reported by authors. For example, continuous monitoring was enabled by data collected every fifteen minutes from an in-ear device on patient oxygen saturation, respiratory and heart rates, and core temperature and sent via Bluetooth to a secure server. 41 Similarly, a wearable patch was applied to the axilla for continuous temperature monitoring, and a pulse oximeter for heart and oxygen saturation rates was used, with Bluetooth transmission. 29 In another study, patients were tasked with measuring their vital signs two times a day; although the emphasis was on self-monitoring rather than by the care providers, data for the vital signs were collected and transmitted via an application on the patients’ device and were reviewed by the team. 31 In sum, these studies allowed for transmission of the vital sign health data to be automated. Table 4 outlines the communication methods between patient and provider with the number of corresponding studies.
Communication methods between patient and provider.
Health Care Provider. The providers who delivered virtual COVID-19 care in the included studies reflect heterogeneity in the range of professional disciplines. Studies involved delivery of virtual care by nurse only (n = 5),27,29,30,39,42 physician only (n = 3),26,34,36 nurse practitioner only (n = 1), 31 medical students (n = 1), 37 or interprofessional teams (n = 6).28,32–35,38,43 One study in France specifically had nurse navigators engage with cancer patients with COVID-19. 42 Three studies did not indicate the disciplines of team members directly providing care to COVID-19 patients,25,40,41 although one reported that they were allied health professionals. 25
For virtual care teams that encompassed more than one professional discipline, there was no consistent composition of interdisciplinary teams. Nurses and physiotherapists provided care through video consultation in the UK, 35 obstetrical nurses and physicians provided telehealth in the US, 38 while other studies utilized teams with more interdisciplinary team members including physicians and nurses, complimented by psychologists, 43 mental health or social workers, pharmacists, practitioners,28,32,33 nurse practitioners,32,33 and pharmacy residents. 32 Where studies involved direct care by physicians, these physicians practiced in family medicine,32,33 infectious disease34,36 and obstetrics. 38 Many of the included studies had a clinical pathway that incorporated the consultation with or referral and escalation to physicians when signs flag clinical status decline.25,28,30,32,33,37–39,41,42 In the Canadian program with a comprehensive interprofessional team, the team held daily huddles and weekly rounds; physician specialists in this program also included internist, respirologist, and psychiatrists. 33 Likewise, an American study focusing on the obstetrical population also held daily team huddles. 38 Despite the virtual care being directly provided by nurse navigators in the French study, the authors emphasized the importance of interdisciplinary team meetings to assess the intervention on a regular basis. 42
Patient Outcomes. Outcomes that were reported varied across studies. Most commonly, the relevant records reported on hospitalizations, deaths, participant symptomatology, and referrals to in-person or hospital care as outcomes of the study. However, these results presented in the studies reflect vast diversity in the reporting of outcomes.
Hospitalizations and Deaths. There were few patient deaths amongst studies that reported on patient mortality, with most indicating that there were no patient deaths related to COVID-19, with one study reporting a high of 1.4% mortality rate. 37 Hospital admission rates were also low, ranging from zero25,29,30,32–36,42,43 to 9.4% of patients, 39 with the exception of one study that had over 50% of patients requiring hospital admission. 37 This virtual program involved telephone support and assessment, resource provision, and other services for under-served communities in “safety net clinics”. 37 Most studies additionally reported on their program's ability to advise the patient to seek in-person or emergency care when there was heightened concern about the patient's condition. This was a frequent safety outcome for several studies. Where this safety outcome was reported as a percentage of patients in the sample, there was a range of 2% 33 to 13%. 41
Availability of Care. Many studies included a total count of the number of virtual visits or contacts with their patients, ranging from 109 35 to 2089. 40 These represent how available care was for patients during their isolation. Of those studies reporting number of virtual visits or contacts per patient, some reported a range (one to six and one to eight calls, 36 five to eight calls, 40 ); others reported median number of contacts per patient (median of four visits per patient 33 ), while some reported on the mean number of contacts per patient such as 10.9 calls per patient, 42 one call per day, 38 or a combination of these measures of central tendency (average 2.79 calls ranging from one to 11, 37 one to 20 calls with a median of six calls, 26 and one to 30 contacts per patient with a median of 16 contacts per patient 29 ). Coffey et al. 39 reported that 80% of low intensity patients and 78.4% of high intensity patients completed the monitoring as per care plan for at least 1 day. Virtual interactions were reported to last for a mean duration of 8.5 min by phone, 15 min by video, 29 15 min by phone, 26 and a high of 27.5 min by video. 35 It is noteworthy to highlight that one study observed that patients opting for contact through the application interacted less (6.2 calls) than those who solely participated via telephone (13.9 calls). 42 In addition, one study reported a 16% rate on uptake for post-discharge follow-up calls. 25
Discussion
This scoping review aimed to explore the nature and patient outcomes of virtual health services provided during the active phase of the illness to persons with COVID-19 who were isolating in the community. The included studies converge on addressing a gap in the health care for newly diagnosed COVID-19 patients in the community. Table 5 summarizes key findings.
Discussion summary.

Symptom and Health Status Monitoring. Monitoring for symptoms and actively detecting for physical health status decline in isolating patients via asynchronous and synchronous communication, or a combination of both have been described. Findings from the relevant records suggest that disease severity and clinical progression could be assessed safely based on symptoms reported over telephone using little technology, more technology via video conferencing, or more sophisticated technologies involving software applications and algorithms. Yet, a low technology model (with no medical equipment) may present clinical challenges for assessing key clinical indicators such as dyspnea.30,34 Use of video conferencing and portable medical equipment at home allow the health care provider to perform visual assessments of the patient and review of vital signs virtually, 29 which better mimics the in-person assessment than the traditional low technology telehealth. This review found that telephone-based care took place synchronously, while virtual care anchoring on digital applications provided additional access to health care providers through messenger, which offered alternatives to real-time-only encounters, especially if patients have a preference.
Technology and Platforms. Wearables and other artificial intelligence-assisted digital tools have been emerging as a trend in healthcare including use in physical activity 44 or glucose tracking. 45 In the context of COVID-19, wearables have been explored to innovate care for COVID-19 patients at home. Wearable technology was tested among some of the included studies to monitor vital signs for detecting worsening COVID-19 disease. Research by Wurzer et al. 41 demonstrated that patients could be monitored for over 13 h on a daily basis through the retrieval of clinical information for assessment. They also acknowledged that issues with the technology could affect the quality of the data such as the physical size and fit of the in-ear device for each patient. The collection of bio-physical data from any device requires active participation from the patient. In Michaud et al.'s 31 study of vital sign monitoring completed by patients themselves, findings revealed that there is potential to promote patient's self-management with technological tools. Yet, in this study, 61% of the patients completed 14 days of vital sign monitoring, suggesting that there is an opportunity to explore facilitators for adhering to interventions and fidelity to the treatment. Multiple factors may influence an individual's intention to use the wearable device, including attitudes and health interests. 46 Further, selection of devices based on reliability and effectiveness in evaluating health outcomes should be carefully made in health research and in practice. 44
Leveraging social media as a platform for health promotion has been previously documented to engage in areas such as sexual health, 47 nutrition, physical activity, and smoking, 48 and most recently for COVID-19 vaccination campaigns. 49 Included in this scoping review, were two studies that made use of common social networking mobile applications; the research pointed to the convenience of using common and widely-used apps so that patients did not need to download a separate app,40,43 while also having the ability to facilitate peer support for patients to support other patients with providing tips in the group chat. 43 Social media use by health care organizations has become widespread for education, health information dissemination, mobilization for purposes such as influencing policy, and more. 50 The selection of applications may be dependent on contextual factors, including understanding specific communities and settings, while weighing the benefits of providing some form of care against the risks of an absence of care. The utilization of social media and networking platforms may have benefits; however, privacy and confidentiality implications cannot be overlooked. Alongside the convenience of digital solutions, distinctive cybersecurity challenges arise related to protecting personal health information, ensuring secure networks, finding a private location to conduct patient conferencing, and more. 51 From selection of platform to obtaining patient consent, implementation of virtual care using any platform or digital solution must involve performing privacy impact analysis, conducting privacy and security trainings, crafting and clearly outlining an information management framework and virtual care policy. 51
While deployment of more advanced digital technologies may be a facilitator for enhanced assessment and communication between patient and provider, the requisite of patients and their caregivers being able to use the technology, requires that digital solutions be user-friendly. 29 The reliability of these digital solutions and networks, as well as the comfort of wearable devices where they are used, can also affect the success of the virtual care intervention.35,41 Additionally, digital equity must be at the forefront of virtual care design for COVID-19 patients. Scaling up and spreading of virtual health care for COVID-19 patients cannot exclude population groups and communities who do not have access to the internet, devices, or other resources essential for receiving care remotely. Even while relying on a low technology model of using telephone modality in a virtual care program, researchers reported a substantially higher hospitalization rate among the sample compared to other studies included in this review. 37 In this particular study, the patient population was reported to commonly face barriers in accessing care and experience health disparities, suggesting that social determinants of health shaped their COVID-19 acquisition likelihood and severe illness trajectory. Especially prudent, is taking action to address digital and health equity among communities that have been disparately affected by COVID-19 infections. While virtual services aim to detect deterioration early on in the disease trajectory and to escalate care in a timely manner, navigating through the complex digital system requires thoughtful design. Clinicians, researchers, and policy-makers must ensure that under-served communities, which are significantly more affected by COVID-19, do not get left further behind as healthcare leverages digital tools to enable improved care.
Care Pathways and Care Teams. To enable seamless continuity of care when hospital transfers are indicated and to promote preventative infection control practices, community virtual care programs for COVID-19 patients should consider building in a mechanism for alerting the receiving hospital. This would involve pre-planned actions outlined for the emergency department and infection control department to follow, as executed by a large metropolitan Canadian hospital. 34 Similarly, an Australian study's hospital transfer process also included notifying the public health unit, hospital executive, and the ambulance, with the ambulance, further notifying the emergency department. 29 Better coordination of services across communities and health care settings presents benefits for controlling the spread of the virus. Interlocked to hospital transfers, is the pathway for care, which encompasses integration of assessment of objective measures such as vital sign values, subjective measures such as symptoms reporting, and clinician judgment. The findings from this review depict the potential for customization of care or service level for patients, depending on their risk for severe illness progression and psychosocial needs. Nine studies’ virtual programming entailed classification of patients into risk categories, with some adjusting the frequency of contacts based on the risk level. However, there are differences in how patients were categorized. Standardizing the categorization of risk may help better compare across studies. One way of standardizing the clinical risk level is to optimize the use of the WHO's disease severity guidance that defines mild, moderate, severe, and critical COVID-19 disease. 52
Furthermore, this review demonstrates that care given by interdisciplinary teams can offer a more comprehensive continuum of services to community-based COVID-19 patients. Where care was provided by an interdisciplinary team, patient needs beyond the bio-medical nature may be met through provision of psychosocial supports and resource linkages.32,33,43 In parallel, tangible supports like grocery delivery and personal protective equipment 37 or supports addressing food insecurity 33 are also key to meeting patient needs more holistically when considering the realistic effects of the social determinants of health. This suggests that there is value in having a comprehensive basket of services, based on individual patients’ and families’ lived situations and scenarios, which could improve their recovery and well-being. The initial search for literature yielded some records on telerehabilitation53–55 and remote diagnostic imaging.56,57 These had a more core focus on diagnostics or longer-term COVID-19; although, they did not meet the review's inclusion criteria, they signal increasing advancement in the breadth of digital health services available for non-hospitalized COVID-19 patients.
Variations. There is much variation in the implementation of virtual care programs for COVID-19 patients, as well as variation in the study designs and reported outcomes. This is unsurprising, given the emergency nature of the pandemic and the just-in-time pivoting that has been required to keep health systems afloat amidst responding to emerging needs and restrictions. There were marked differences in the selected patient outcomes and how they were reported, even when outcomes were similar. First, as part of the safety metric, patients were advised to seek urgent medical care at the hospital or another center for in-person assessment. However, these were not consistently reported. It is challenging to compare how frequently community COVID-19 virtual care is able to refer to community-based in-person assessment and treatment across studies, as some reported on the number of visits to the emergency department without reporting the number of unique individual patients. Some study samples also included a mix of confirmed or diagnosed COVID-19 cases with probable or suspect cases36,38 and other studies not specifying whether emergency department visits were referred or patient-initiated. Therefore, the depiction of the state of hospital referrals among the patient group of interest is unclear. Second, although the total number of patient-provider interactions occurring virtually can illustrate the volume or uptake, these counts may be meaningful only within the context of the particular study. Other factors such as the dose of the virtual care, timelines of the study, and sample size, will influence the number of patient-provider virtual encounters. Thus, standardizing how to quantify “how much” virtual care is provided can contribute to a better illustration of dose and impact, if patient outcomes are to be compared against the efficacy of virtual interventions. Third, only one study reported on the percentage of hospitalized participants who expressed that they would not have initiated visiting the hospital had they not been participating in the study. 41 This may be clinically significant, and worthwhile in investigating across research, although there would be limitations in measuring this outcome. Fourth, one study revealed that one participant had not adhered to the quarantine. 29 Despite the recent loosening up on legal requirement to isolate in some jurisdictions, compliance to isolation will continue to be essential in preventing the community spread, thus, of high importance to evaluate. To better support patients to remain in isolation while infectious, it may be essential from a patient-centered perspective, to assess their needs holistically and incorporate additional services such as tangible supports like grocery assistance, which was offered in one study. 37
Future Research. This scoping review highlights an emerging body of evidence for efficient and safe provision of virtual health care for community-based self-isolating persons with COVID-19 in the acute phase of disease. In spite of the substantial variation in methodologies, interventions, and outcomes across existing research, the included research studies addressed a gap in service for patients isolating at home due to a COVID-19 diagnosis. This considerable variation, however, poses an opportunity for future research to more consistently build on existing research to evaluate the effectiveness of virtual care, whether through directly impacting or by mediating factors affecting the health outcomes of COVID-19 patients.
Clear theoretical and operational definitions of the problem (such as lack of availability of care during the self-isolation period) are needed, especially with the continuously evolving nature of the pandemic The design of interventions relies on having clarity of the problem, a vision for the desired improvement, and outline of the active ingredients of the health intervention including components, mode, and dose. 58 In conceptualizing virtual care, researchers can wrestle with what constitutes the intervention. For instance, virtual care itself may be considered an intervention. An alternative approach may be to consider virtual care as the mode of delivery of an intervention, rather than the intervention. Studies included in this review offered virtual care for different lengths of time. Virtual care programming generally lasted for a duration of around 14 days, however there is no consistency in the dose of the intervention. Even when there is seemingly common duration such as services offered for 14 days, it is not always clear whether service was completed for a total of 14 days from enrolment or from the patient's symptom onset date, specimen collection date, case reported date, or another date. There may be opportunities for engagement in intervention research comparing the outcomes of groups with virtual care versus routine care, or outcomes of groups using different platforms and technologies. The recent appearance and authorization of oral antiviral medications signals another shift in treatment for patients, and may additionally prompt adjustments to and re-examination of virtual care program planning for COVID-19 patients.
Virtual programs covered by this scoping review frequently classified patients by risk category, which affected the frequency of contacts from the provider to the patient. However, these categorizations and classifications differed. Researchers can consider standardizing risk assessments. Similarly, common outcome measures for research could be applied for better comparisons in COVID-19 research. This is strongly advocated by the WHO Working Group of the Clinical Characterisation and Management of COVID-19 Infection (2020), urging the development of minimum data elements in research. 59 Patient experience, beyond patient satisfaction, emerged as a significant gap in the virtual COVID-19 care research.
Limitations
This scoping review was undertaken to explore the state of the literature on virtual care for the COVID-19 patient isolating in the community. A limitation of this review may be missing relevant records that were not identified from databases beyond those used in this search, and literature not published in English.
Conclusion
Despite a trend in easing of public health restrictive measures in some areas around the world, the threat of variants persists. 60 Early detection of clinical deterioration and disease progression can facilitate appropriate decision-making, which consequently ensures that there is no delay in assessment and treatment, while promoting the prioritization of patients who are in need of hospitalization. 61 The provision of virtual care for patients at home can meet patient needs while curbing spread of the virus to others. Amidst the shifting and ever evolving nature of the COVID-19 response, the safety and high-quality care for community-based isolating patients diagnosed with COVID-19 remain a gap in need of attention and narrowing. Findings from this scoping review mapped out the current evidence on virtual care provision for persons with COVID-19, who are self-isolating in the community, and point to a breadth of research, practice, and policy opportunities. Serving this particular population benefits the patients themselves, and the hospitals, while reducing the overall burden on an already stretched health care system. It is important to commit and invest in appropriate and safe virtual care pathways for infectious diseases to better prepare for future outbreaks and pandemic threats.
Footnotes
Acknowledgments
We would like to thank Don Kinder for consultation on the search strategy.
Contributorship
LCL and CC conceptualized the study, developed the protocol, conducted eligibility screening. Extraction of data and formal analysis were conducted by LCL and verified and refined by CC. Original draft was prepared by LCL, and substantive edits and revisions to manuscript content made by CC and LCL. All authors reviewed, edited, and approved the final version of the manuscript.
Ethical approval
The authors consulted with the institution's Research Ethics Board about the need for ethical review. Ethical review and approval were waived for this scoping review as it did not involve the use of either humans or animals as participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
LCL
Appendix: Summary of Included Articles.
Summary of Characteristics and Findings of Included Studies

| Author, Year and Country | Purpose Statement | Design | Sample Size and Patient Characteristics | Type and Dose of Health Service and Supports | Technology Used (what and how?) | Health Providers (who?) | Patient Outcomes |
|---|---|---|---|---|---|---|---|
| Swift et al.
35
(2021) UK |
“to share a description of the service and early outcomes, as healthcare systems around the world face ongoing challenges.” (p.8) | Observational service evaluation | Size: n = 65 Age: 21.5-87.4 Characteristics: COVID-19 clinical diagnosis, < 10 days from symptom onset, respiratory symptoms, lone household, clinically vulnerable, access to a device |
Virtual ward that includes remote support and follow-up post hospital discharge; helpline with daily symptom monitoring Patients monitored as red, amber or green ratings, with red indicating urgent response needed Duration: Until discharge from program |
Digital application with patient and clinical portals, messenger, video, and clinical dashboard Patients enter data into patient portal, calculating score for clinician and classified as red, amber, green ratings Vital sign equipment: Thermometer, Pulse oximeter Communication: Asynchronous and synchronous encounters |
Nurses, physiotherapists | Mortality: zero COVID-19 related deaths Hospitalization: 6.2% of patients had re-admission to in-person hospital Emergency/Urgent/In-person care: not reported Virtual encounters: 109 virtual conferences for red rating, 114 video conferences for amber. Video consultations for red alerts had mean time lasting 27.5 min. Mean length of stay in virtual ward = 13.2 days. 91% of patients stayed for 9 or more days. Other: 56.3% (p = 0.049) reduction of number of red days from admission to virtual ward to final day; 68.2% (p = 0.002) reduction of number of red days from first 3 days to final 3 days |
| Clarke et al.
25
(2021) Australia |
“to describe the rapid implementation of a telephone based COVID-19 community monitoring service and the demographic and clinical characteristics of those enrolled.” (p.1125) |
Retrospective mixed methods evaluation | Size: n = 850 Age: 0–90+ Characteristics: COVID-19 diagnosis (36% with “high-risk” factors) |
Provision of health advice and support, clinical social and welfare assessments, education on isolation, symptoms signifying deterioration, post-discharge call High-risk = daily calls Low-risk = calls every other day Duration: up to 14 days |
Telephone Communication: Synchronous encounters |
Allied health providers, and medical officer, general practitioner for consultation when escalation required |
Mortality: zero deaths Hospitalization: 3.7% Emergency/Urgent In-person care: 3.5% of patients identified as having clinical deterioration who needed to seek urgent care Virtual encounters: Uptake for post-discharge follow-up call of 16% |
| Bell et al.
36
(2021) UK |
Not stated | Retrospective service evaluation | Size: n = 192 (pilot) and n = 47 (validation) Age: 32–55 (pilot period) and 29–60 (validation) Characteristics: Visited emergency |
Follow-up assessment and provision of test result Low-risk patients = self-serve call in High-risk patients = follow-up calls by clinician judgement Duration: > 14 days |
Telephone, electronic health record system Vital sign equipment: Pulse oximeter for some patients Communication: Synchronous encounters |
Infectious disease specialist | Mortality: zero deaths Hospitalization: 4.8% planned reattendance and 2.4 unplanned reattendances that led to admission in pilot. 1.3% planned and 6.2% unplanned reattendances that led to admissions in validation period. Emergency/Urgent In-person care: 21.7% had “planned reattendance” to in-person assessment (directed by clinician from telephone assessment) and 7.2% “unplanned” Virtual encounters: In pilot period of all patients with suspect COVID-19, range of 2–17 telephone appointments daily. In pilot period, for confirmed or probable COVID-19 diagnosis, range of 1–6 telephone calls. In validation period, for COVID-19 positive patients, range of 1–8 telephone calls, 6.2% “planned reattendance” and 8.3% “unplanned” Other: 42.2% discharged to general practitioner |
| Wong et al.
37
(2022) USA |
“to describe a telehealth-based program to monitor patients in the outpatient setting, assess the feasibility of establishing and maintaining such a program, and to briefly describe and compare the outcomes of our clinic patients with those in our greater local community” (p.1) |
Retrospective feasibility cohort | Size: n = 296 Age: 19–91 Characteristics: COVID-19 diagnosis, patient of primary care medicine clinic serving “vulnerable” populations |
Assessment and monitoring of symptoms, education on prevention of transmission, resource-provision during isolation (including grocery delivery support from local community resources, free personal protective equipment and medication reconciliation) with daily weekday calls Duration: until recovery |
Telephone and video consultations (when escalation required/clinically indicated) Vital sign equipment: Pulse oximeters for some patients (later months at organization) Communication: Synchronous encounters |
Medical students and physician (when escalation required) | Mortality: 1.4% Hospitalization: 53.7% Virtual encounters: Average number of calls = 2.79, range 1–11. Total > 800 calls |
| Malwade et al.
40
(2021) India |
“to provide an example from a hospital in India using the social networking app, WhatsApp, as a teleconsultation (TC) alternative during the COVID-19 pandemic” (p.2) | Retrospective (Not specified – appears to be descriptive) |
Size: n = 318 Age: 18–65 Characteristics: smart phone use |
Provision of diagnostic reports and clinical advice such as blood tests for co-morbidities or assessment at hospital Duration: 17 days |
Mobile app, telephone Communication: Asynchronous and synchronous encounters |
Not specified (“Health care providers”) | Emergency/Urgent In-person care: 30 patients advised to seek hospital care Virtual encounters: total of 2089 telephone calls ranging from 5–8 calls; 47 instances for communication of diagnostic results Other: Reduction of visiting the hospital unnecessarily |
| Micallef et al.
26
(2021) Australia |
To “[a]scertain characteristics of patients with COVID-19 managed by telehealth…Ascertain amount of time taken by staff to perform this care, and whether this care might reduce burden on other services of healthcare organisation” (p.2) | Retrospective observational cohort study, single centre | Size: n = 158 Age: 18–94 Characteristics: positive SARS-CoV-2 result |
Review of symptoms, counselling and support; ‘safety net’ advice, prescription or medical notes High-risk = daily calls Low-risk = call every other day Duration: until symptoms resolved |
Telephone Communication: Synchronous encounters |
Clinic physicians and, infectious diseases specialist | Mortality: 0.6% Hospitalization: 3.8% admitted to hospital Emergency/Urgent In-person care: 6.3% required in-person assessment; 2.5% required ambulance to home Virtual encounters: Total of 1151 telephone calls. Median 6 calls per patient; range 1–20 telephone calls, average duration of call 15 min. Median stay in program = 10 days (range of 3–32) Other: 88.6% managed at home with no complications |
| Raffan et al.
27
(2021) Australia |
“to contribute to the growing body of literature on the virtual care experience by providing insight into the patient experience of a prescribed COVID-19 model of virtual care in an Australian context” (p.1) |
Survey (Appears to be mixed methods with grounded approach for free text responses) |
Size: n = 265 Age: >18 Characteristics: positive COVID-19; home quarantine or health hotel |
Remote vital signs monitoring twice daily, temperature monitoring, 24/7 access to RN Duration: Not specified but appears to be 14 days based on quarantine orders |
Video conferencing Vital sign equipment: Pulse oximeter, temperature patch (High-risk have wearable devices) Communication: Synchronous encounters |
Registered Nurse | Other: Overall positive patient experiences |
| Michaud et al.
31
(2021) Canada |
“to assess the feasibility of self-assessment of vital signs and symptoms with electronic transmission of results, by self-isolating individuals with positive SARS-CoV-2 polymerase chain reaction (PCR) test” (p.2) |
Prospective cohort | Size: n = 46 Age: mean 54.1 Characteristics: positive PCR, hypertension diagnosis, access to internet, phone and computer |
Vital sign (blood pressure, heart rate, respiratory rate, oxygen saturation, temperature) self-assessment twice a day, assessment of symptoms via questionnaire for self-monitoring, telephone call at day 3 and day 10 for discussion of concerns Duration: 14 days |
Mobile application for phone or tablet (to record vital signs) with transmission of data to database and algorithm (for patient's decision-making based on vital signs and symptom severity), telephone Communication: Asynchronous and synchronous encounters |
Nurse Practitioner | Virtual encounters: Patients completed: Mean of 12.3 days of vital signs; 10.8 days of reporting of symptom. 61% completed vital sign measuring for all 14 days and 89% for minimum 7 days. Other: Upwards of 16.9% severe fatigue, upwards of 20.1% with abnormal oximetry value; abnormal vital signs and severe symptoms had higher rates in the first week than second week |
| Wurzer et al.
41
(2021) Germany |
“to reliably and continuously monitor biosignals relevant to the course of an infectious disease” (p.3) |
Feasibility |
Size: n = 153 Age: median 59 Characteristics: positive PCR test result, one pre-existing immunological, pulmonary or cardiovascular condition |
Biosignal observation and monitoring by team 24/7 of biosignals taken for 3 min every 15 min, daily telephone support and assessment of symptoms and cognition Duration: until end of isolation or if hospitalized |
Telephone Wearable: in-ear device with data transmission to a server Communication: Asynchronous and synchronous encounters |
Not specified (“trained members”) Physicians for consultation when escalation required |
Mortality: 1 death Hospitalization: 7 patients in intensive care Emergency/Urgent In-person care: 13% sent to hospital by the team Virtual encounters: Participants were monitored for median of 9 (IQR 6–13) days with median 13.3 (IQR 9.4–17.0) hours of monitoring per day Other: Of those participants who remained isolating at home, zero had unforeseen complications Approximately 90% of patients who were hospitalized noted that they would not have sought hospital care as timely if they were not participating in the study including those who were admitted to intensive care |
| Pimlott et al.
32
(2021) Canada |
“describes the natural history, clinical management and outcomes of patients who received care during the first 5 weeks of the CovidCare@Home virtual clinic” (p.550) |
Retrospective chart review, observational, descriptive study | Size: n = 73 Age: 19–68 Characteristics: lab-confirmed positive result, mildly to moderately symptomatic, no family physician or no access to family physician during pandemic, majority of sample employed in high-risk settings |
Assessment and monitoring daily or every two days (depending on patient's condition), management included messages about self-isolation, hydration, and medication use Higher-risk = contact up to two times a day with pulse oximetry and temperature assessment Duration: Not specified |
Video conferencing and telephone Vital sign equipment: Thermometer and pulse oximeter (for some patients) Communication: Synchronous encounters |
Family medicine-led interdisciplinary team: Family medicine residents, staff family physicians, nurses (initial visit by family medicine resident and physician with follow-up by resident and physician or nurse) Support provided by pharmacist, pharmacist resident, social workers, nurse practitioners, secretary, administrator and specialists |
Mortality: zero deaths Hospitalization: zero Emergency/Urgent In-person care: 6.8% sent to hospital emergency and 1.4% to ambulatory care unit; 12.3% required care beyond virtual program Virtual encounters: First virtual visit occurred on average 3.2 days post testing. Most patients mean of 8.1 days (SD 6 days) with close to 5 virtual visits Other: 88% with mild disease. 32.9% of patients were mailed pulse oximeter and 6.8% mailed a thermometer for further monitoring |
| Schultz et al.
28
(2021) Australia |
“to describe and evaluate the implementation of a virtual ward as a COVID-19 hospital avoidance response strategy and identify opportunities for improvement and future applicability.” (p.434). |
Mixed methods observational | Size: n = 238 Age: 18.8–84.3 Characteristics: confirmed diagnosis |
Virtual ward that includes risk assessment, daily calls of once or twice with psychosocial support, medication review, support for food access and financial management Duration: until end of isolation |
Telephone Communication: Synchronous encounters |
Nurses, pharmacists, social workers, medical officers, administrative officers, and medical officers (when escalation required) | Hospitalization: 20 admissions for inpatient hospitalization Emergency/Urgent In-person care: 29 counts of episodes of presenting at emergency (25 counts of emergency department visits for COVID-19 reason) Virtual encounters: Total 2451 virtual bed days. Average duration in program 9.3 days (s.d. 7.1 days) Other: Majority of patients were able to isolate at home, with some readmission to virtual ward 15 patients had more than 1 episode in the virtual ward |
| Ferrua et al.
42
(2021) France |
“to provide a comprehensive description of the CAPRI-COVID intervention” and “to provide feedback on the usefulness of this platform for cancer patients” (p.4486) | (Not specified – Appears to be mixed methods, descriptive and cross-sectional ) |
Size: n = 129 Age: mean 59 Characteristics: Cancer patients diagnosed with COVID-19 |
Assessment and education of minimizing COVID-19 exposure with patients and relatives, home care and meal assistance, symptom monitoring (telenursing or by patient via app) Nurse calls plus messaging or call initiated by patients as needed during operating hours Longer-term support additionally offered Duration: at least 14 days until 2 days after symptoms resolved |
Mobile application with telephone platform, messaging, and dedicated telephone line Communication: Asynchronous and synchronous encounters |
Nurses (“Nurse Navigators”) and assistant nurses | Mortality: Zero COVID-19 related deaths Hospitalization: 7.8% admitted to hospital with no COVID-19 related intensive care Emergency/Urgent care: 17.1% accessed emergency department. 28 patients were referred by the nurse navigator to seek emergency care Virtual encounters: Average 10.9 calls for each patient. Patients who used the app had 6.2 calls per patient versus 13.9 calls for patients using telephone. Other: 19.4% asymptomatic 8 participants had home care initiated; 22 patients were referred for psychosocial needs |
| Agarwal et al.
33
(2021) Canada |
“to describe the model of care in COVIDCare@ Home and discuss its initial adoption, feasibility and safety in the first 5 weeks” (p.E325). |
Descriptive | Size: n = 97 Age: 31–58 Characteristics: COVID-19 diagnosis |
Initial and follow-up assessments every other day, or every 3 days dependent on risk level, brief counselling and linking to community resources, communication with patient's primary care provider as applicable Duration: 14 days from the onset of symptoms |
Telephone and video conferencing, patient portal with messenger, dashboard Vital sign equipment: Thermometers and pulse oximeters (for some patients) Communication: Asynchronous and synchronous encounters |
Family physician, family medicine resident, Registered Nurse, mental health worker or social worker, nurse practitioner, pharmacist Consultation with internist, respirologist, and psychiatrist |
Mortality: zero deaths Hospitalization: zero Emergency/Urgent In-person care: 2 patients were referred to emergency department by program Virtual encounters: Median 4 visits per patient (IQR 2–5 visits). Median of 8 days (IQR 5–10 days) follow-up duration. Total 415 visits. 62% of virtual visits were by video conferencing Other: 16 patients had virtual conference with social worker (6 patients received support for food and finance insecurity; 4 patients for support with mental health needs), 6 for pharmacist consultation |
| Hutchings et al.
29
(2021) Australia |
“to describe the implementation of and early experience with virtual health care for community management of patients with COVID-19” (p.1) | Observational cohort | Size: n = 162 Age: 11–79 (3 pediatric, 2 perinatal) Characteristics: positive COVID-19 test result |
Provision of “welcome package” delivered to home, vital sign monitoring (no BP), symptom monitoring for clinical assessment, provision of psychosocial support with scheduled contacts from team 3 times a day (at least one video conference daily Duration: until end of isolation |
Telephone and video conferencing, Mobile application Wearable: Temperature patch and pulse oximeter with Bluetooth for readings on device (Mobile app); temperature readings sent to dashboard Communication: Asynchronous and synchronous encounters |
Nurses and medical officers (when escalation required) | Mortality: zero deaths Hospitalization: 2.5% patients sent to hospital emergency with 1.9% admitted inpatient Emergency/Urgent In-person care: 3% ambulance call rate, and 2.5% patients sent to hospital emergency Virtual encounters: Median of 16 and range of 1–30 contacts per patient; 66.3% of the contacts were video-based. Median 15 min (IQR 13–15 min) for video conferences Median 8.5 min (IQR 5–15 min) for phone. Median of 8 days duration in virtual service (range 1–17 days) Other: 81.5% of patients had equipment delivered. 1 patient did not comply to self-isolation order |
| Ferry et al.
30
(2021) Australia |
“(1) to describe the clinical characteristics of an Australian cohort of patients with COVID-19, (2) to evaluate the clinical care provided to this cohort through a virtual ward model, and (3) to identify any possible predictors of deterioration” (p.2) |
Retrospective clinical assessment, single-centre (Appears to be descriptive) |
Size: n = 223 Age: 14–78 (2 pediatric) Characteristics: confirmed COVID-19 |
Virtual ward that includes symptom monitoring, assessment of well-being and social factors Duration: until end of isolation |
Telephone Communication: Synchronous encounters |
Nurses and medical officers (when escalation required) | Mortality: zero deaths Hospitalization: 8% patients had referral to hospital, with 5.4% hospital admission and 16.7% requiring intensive care Emergency/Urgent In-person care: 8% Virtual encounters: Median duration in virtual program 8 days (range 1–44 days). Other: 92% of patients clinically recovered and discharged. Majority of patients had mild COVID-19 |
| Lam et al.
34
(2020) Canada |
“to develop and test the feasibility of a virtual care program for physician assessment and follow-up of outpatients with COVID-19 in self-isolation” (p.E407) |
Feasibility (Not specified – appears to be descriptive cohort) |
Size: n = 50 Age: 30.5–59.5 Characteristics: positive COVID-19 test result |
Standardized assessments for initial and follow-up contacts), follow-up contacts explore symptom changes, education on the disease and symptoms which would signal need for medical attention Activation of hospital pager to contact infectious disease physician if symptoms are of concern Stable patients have minimum weekly contact, Other patients up to two times a day based on physician judgement Coordination with hospital in the circumstance when patient needs to be transferred to hospital Duration: until cleared by infectious disease physician |
Video conferencing (for patients who have access to video-based platform) and telephone Communication: Synchronous encounters |
Infectious disease physician | Mortality: zero deaths Hospitalization: 4 patients admitted Emergency/Urgent In-person care: 12% of patients required transfer to hospital Virtual encounters: 64% of the patients were assessed by virtual video platform (others were by phone). Median duration for patients who were discharged from program = 12.5 days (IQR 8.75–16) days. |
| Reforma et al.
38
(2020) USA |
“to describe the feasibility and clinical and process outcomes associated with a multidisciplinary telemedicine surveillance model to triage and manage obstetrical patients with known exposures and symptoms of COVID-19” (p.1) | Descriptive (quality improvement) | Size: n = 135 Age: 29–35 Characteristics: prenatal and postpartum (no more than 6 weeks post birth), confirmed COVID-19 (or exposed to COVID-19 or experienced symptoms of COVID-19) |
Assessment and education on isolation, symptoms, hygiene, with follow-up calls daily or every other day, and encouragement to contact primary OB care provider for OB-related needs Duration minimum 7 days |
Telephone Communication: Synchronous encounters |
Obstetrical nurses and physicians | Hospitalization: 9 patients Emergency/Urgent In-person care: 19 patients Virtual encounters: 85.9% of patients accepted 2 or more calls. Average 1 telephone call per day. Median 7 days (IQR 4–8 days) duration in telemedicine care Other: 50.4% had positive test result; 86% of patients were managed remotely without inpatient care; 19 patients were sent for in-person assessment with 9 admitted (7 of whom positive with COVID-19) Note: Results not stratified by COVID-19 positive status |
| Xu et al.
43
(2020) China |
“to evaluate a telemedicine model that was developed to address the challenges of treating patients with progressive COVID-19 who are home-quarantined and shortages in the medical workforce” (p.1) | Retrospective single-centre | Size: n = 48 Age: median 37.5 Characteristics: COVID-19 positive test result |
Telemedicine form on Cloud for initial and subsequent assessment, guidance on isolation requirements, group chat with other participants and team; worsening symptoms or decline in mental state would be escalated for hospital care; mood support from psychologist Duration: until clinically recovered |
Social Media Mobile app with telephone calling, e-counselling, messenger Communication: Asynchronous and synchronous encounters |
Physicians, nurses, and psychologist | Mortality: zero deaths Hospitalization: 6 patients admitted to hospital with 2 critical Virtual encounters: 63% of participants continued with program, 35% self-discontinued program as they were recovered |
| Coffey et al.
39
(2021) USA |
“to determine the feasibility and safety of the COVID-19 [remote patient monitoring] as measured by patient engagement with the technology, rate of alerts and escalations managed by virtual care teams, acute care resource utilization rates, and patient clinical outcomes” (p.3) | Retrospective cohort | Size: n = 7074 (2314 low-intensity, 4760 high-intensity) Age: 17–101 Characteristics: confirmed COVID-19 lab result, high-intensity care patients had one or more risk factors for severe illness |
Symptom assessment two times a day, vital sign data collection, education on care plan, and when to go to emergency with 24/7 monitoring Duration: until graduation (clearance) or drop-out |
Digital app with messages, telephone Vital sign-equipment: Thermometer, pulse oximeter, optional BP monitor (if patient owns one) for low-intensity and Bluetooth BP monitor, body scale, thermometer, pulse oximeter (passive collection of physiological data) for high-intensity Communication: Asynchronous and synchronous encounters |
Nurses and physicians (when escalation required) | Mortality: 0.4% Hospitalization: 9.4% hospital admission 78 ICU admission High-intensity participants accounted for most acute care utilization Emergency/Urgent In-person care: 11.4% of participants had emergency visit Low-intensity: Median duration 9 days. 3.2% of all tasks alerted nurses of symptom or vital sign that signalled a need for clinical assessment – each one received assessment while 9.4% of these resulted in escalation High-intensity: Median duration 12 days 72.1% participants remained in program until graduation Care plan compliance 72.5% 19.6% of all tasks alerted nurses of symptom or vital sign that signalled a need for clinical assessment – each one received assessment while 18.8% of these resulted in escalation. 78.9% Patient engagement (monitoring at least one day) Other: Care plan compliance 61.6% |