
Abstract
Objective
Temporal processing is the brain's ability to process rapid successive stimuli, and children with neurodevelopmental disorders showed temporal processing deficits. Empirical evidence suggests that in-person intervention on temporal processing improves various cognitive functions of these children, and the present study aimed to study the effects of temporal processing tele-intervention (TPT) on the cognitive functions of children with neurodevelopmental disorders.
Methods
Ninety-five children with neurodevelopmental disorders were recruited and randomly assigned to remotely receive either TPT or conventional language remediation (CLR) in 20 parallel group-based intervention sessions once per week. Their cognitive functions were assessed before and after the intervention.
Results
The TPT group demonstrated a specific and significant improvement in working memory (p < .001). While there was an overall significant improvement in sustained attention in terms of processing speed after both types of intervention (p = .006), the positive effects of TPT might be more prominent than that of CLR given the significant pre–post difference after receiving TPT (p = .012) but not CLR (p = .21). Regarding rapid naming accuracy which had marginally significant improvement after the intervention (p = .03), the trend of improvement in TPT (p = .05) also seemed more apparent than that of CLR (p = .18). Finally, the TPT group had significant improvement in word knowledge (p < .001), rapid naming speed (p < .001), sustained attention in terms of accuracy (p < .001), and verbal learning and memory (p < .01) to an extent similar to that of the CLR group.
Conclusions
These findings suggest that TPT can be a potential intervention for improving cognitive functions in children with neurodevelopmental disorders.
Clinical trial registration number: NCT05428657 at ClinicalTrials.gov (https://clinicaltrials.gov/).
Keywords
Introduction
Temporal processing refers to an individual's time resolution when processing stimuli presented in rapid succession on a timescale as short as milliseconds. It is an essential perceptual processing skill fundamental to many cognitive functions, such as perception, attention, memory, language, and motor abilities.1–4 Temporal processing deficits are common in children with neurodevelopmental disorders. As early as the 1970s, Tallal and Piercy 5 reported that aphasic children demonstrated a deficiency in distinguishing and judging the temporal order of tone pairs. Since then, an increasing number of studies have further demonstrated temporal processing deficits in other neurodevelopmental disorders, including autism spectrum disorder (ASD)6–9 and attention-deficit/hyperactivity disorder (ADHD).10–13 Though inconsistent findings of relatively intact temporal processing for nonspeech stimuli in ASD14,15 and ADHD16,17 have been reported, many studies have put forward that temporal processing deficits found in ASD and ADHD may be a possible factor mediating their cognitive impairment in attention, episodic memory, and language.18–22 For instance, Maister and Plaisted-Grant 19 found that when children with ASD were required to reproduce stimuli with varying durations (a common paradigm testing temporal processing), they committed significantly more errors than typically developed children, and their temporal processing deficit might be the underlying cause of impaired episodic memory. Foss-Feig et al. 20 also reported an association between impairment in rapid auditory temporal processing and difficulties in language processing among children with ASD in a gap detection task. In addition, for individuals with ADHD, Hart et al. 21 revealed that temporal processing tasks were sensitive in classifying children with ADHD from their normal counterparts, and the temporal processing measure was significantly correlated with the core inattention and hyperactive symptoms of ADHD. Temporal processing was also intercorrelated with impaired executive functions in ADHD, such as working memory and attention. However, timing deficits in ADHD remained to exist even when executive functions were controlled, suggesting independent deficits in the temporal domain. 22
To evaluate temporal processing, one of the well-known experimental paradigms is the temporal order judgment (TOJ) paradigm, 23 in which children with neurodevelopmental disorders usually require longer interstimulus intervals (ISIs) to separately perceive two acoustic stimuli that are presented shortly one after the other5,6,8,11,12 and demonstrate lower accuracy in sequencing the two stimuli.5,6,10,12 In specific, children with ASD required 48% longer ISIs for reliable repetition of the sound sequences than typically developed children. 8 Children with ADHD showed a higher TOJ threshold for tones 11 and lower accuracy in sequencing tonal and consonant–vowel (CV) syllabic pairs. 10 Two recent studies applying an online temporal processing assessment revealed similar temporal processing deficits in children with ADHD 12 and ASD, 6 suggesting that children with ADHD or ASD showed significantly lower accuracy rates than their typically developed counterparts in TOJ tasks using tonal and CV syllabic pairs and a higher ISI passing threshold for CV pairs.
Given the deficits in temporal processing commonly found in children with neurodevelopmental disorders, many studies have explored the effectiveness of temporal processing intervention (TPI) in improving their cognitive functions. Empirical evidence suggests that TPI has a positive effect on language abilities. By implementing auditory TPI for 6 weeks, 24 Tallal et al. demonstrated positive outcomes of TPI on speech discrimination and comprehension in children with language-learning impairment. Improvement has also been shown in phonological processing,25,26 rapid naming, 27 spelling, 28 and reading ability 28 in children with dyslexia after TPI. Specifically, Wang et al. 27 reported that Chinese children with dyslexia took a shorter time to complete a rapid digit naming task after receiving 12 sessions of TPI for 3 to 4 weeks. Strehlow et al. 28 also found a 4-week TPI to have positive effects on improving reading and spelling in children with dyslexia.
Apart from language, improvements in other cognitive domains, including attention and memory, were shown after TPI. For instance, Stevens et al. 29 found an improvement in selective auditory attention after 6 weeks of TPI in children with language impairment. In adults, Szelag and Skolimowska 30 reported that TPI improved the sustained and divided attention, visual attention, and memory functions of healthy older adults. In addition, an information processing training program with TOJ-based training of rapidly successive sweeps as one of the six training exercises enhanced global auditory memory scores.31,32
While the majority of studies on TPI are targeted at children with language impairment or dyslexia and older adults,24–32 the effect of TPI on children with ASD and ADHD remains largely unknown. ASD and ADHD are commonly found to have multiple cognitive impairments, and temporal processing is a fundamental skill mediating many cognitive functions. Based on the above empirical evidence for the presence of temporal processing deficits in ASD6–9 and ADHD10–13 and the possible association between their temporal processing deficits and various cognitive impairments,18–22 it is therefore postulated that training on temporal processing may also enhance the language, attention, and memory functions of children with ASD and ADHD.
Besides, previous studies on TPI were primarily conducted through in-person intervention; therefore, the effectiveness of temporal processing tele-intervention (TPT) is still being determined. With the vigorous development of tele-intervention in recent years, some studies have shown that even children with neurodevelopmental disorders could benefit from remote online intervention.33–35 Tele-intervention that can be delivered remotely makes intervention more easily accessible for children with neurodevelopmental disorders in lower-income classes or remote areas. As a result, more children with neurodevelopmental disorders can benefit from tele-intervention. Thus, the present study aims to examine the potential effects of TPT on children with ASD and ADHD. With the positive outcomes of TPI on children and adults, it is anticipated that TPT would show similar benefits as TPI.
The TPT program adopted in the present study was developed by the first author. It is a web-based computerized intervention program that can be administered remotely on a computer or tablet device. The intervention program was designed based on the TOJ task of identifying and ordering pairs of rapidly successive tone and CV stimuli. Since 2019, our team has applied the TPT program to train over 100 children with neurodevelopmental disorders in Hong Kong, and positive outcomes were observed in terms of more accurate temporal processing during the intervention, better verbal expression and comprehension, reading and spelling skills, and academic performance in real life.
Given our encouraging clinical observations and the empirical support for the potential effects of TPI, the present study aims to examine whether web-based TPT can enhance the language, attention, and memory functions of children with neurodevelopmental disorders. Based on previous empirical evidence for an association between temporal processing and cognitive functions1–4 and its deficit associated with cognitive impairments in ASD and ADHD,18–22 it is hypothesized that training the fundamental temporal processing skills could enhance various cognitive functions of children with neurodevelopmental disorders. Besides, the effects of TPT on cognitive functions will be compared with those of conventional language remediation (CLR). CLR was chosen as the comparison group because it is one of the remedial supports commonly provided for children with neurodevelopmental disorders in their formal schools in Hong Kong. By comparing the training effects of CLR, the present study may shed some light on the possibility of applying TPT as an alternative intervention for children with neurodevelopmental disorders.
Methods
Participants
In total, 95 children with neurodevelopmental disorders aged 6 to 11 years in grades 2 to 6 were recruited and referred by their school teachers from 4 local mainstream primary schools. The sample size was predetermined based on the mean effect size of 0.82 for applying TPI to enhance the cognitive functions of children with language impairment, as outlined in Tallal's study. 36 Power analysis was conducted to compute the total sample size per intervention group to be at least 31, with the power at 0.95 and alpha value at .05. Accounting for an approximate 35% attrition rate, a sample size of 48 children per group was required. According to the Education Bureau records, these children were formally diagnosed with ASD, ADHD, specific learning difficulties (SpLD), and/or a borderline level of intellectual functioning. The diagnosis was formulated by a psychiatrist, a pediatrician, a clinical psychologist at a general hospital or child assessment center, or an educational psychologist at school. None of them reported a history of head injury or epilepsy. All children participated voluntarily, with written informed consent obtained from their parents before the study. This study was conducted in compliance with the requirements stated in the Declaration of Helsinki of the World Medical Association. The research protocol was approved by the Joint Chinese University of Hong Kong–New Territories East Cluster Clinical Research Ethics Committee (CREC reference number: 2020.501-T).
Procedure
At baseline, children were assessed individually on their cognitive functions, including language, working memory, sustained attention, and verbal learning and memory, using standardized neuropsychological tests and an experimental paradigm by trained research assistants at their primary schools.
After baseline assessment, they were randomly assigned to receive either TPT (n = 47) or CLR (n = 48) for 20 intervention sessions, 75 minutes each, once per week, over 8 months, which was the usual dosage and duration of remedial support for children with neurodevelopmental disorders in Hong Kong. Randomization was performed by a research assistant using a random number generator. The two intervention groups were matched based on age (t(93) = −0.68, p = .50), gender (χ2(1) = 0.04, p = .85), years of education (t(93) = −0.38, p = .70), and diagnosis (χ2(3) = 4.29, p = .23). Each intervention program was delivered to a group of 10 to 15 children remotely through a video conferencing platform. Each group of intervention was run by a team of one trained instructor with two to three assistants at the same time in a parallel session in separate virtual meeting rooms. The children attended the online intervention sessions at their home or school. In each meeting room, children of the same group met each other virtually. During the training, the instructor was responsible for providing tele-intervention and working with the assistants to help children who had encountered technical problems or difficulties in accomplishing the training tasks.
After the intervention, the children were reassessed with the same tests given at baseline to evaluate the effects of TPT and CLR on their cognitive functions. The assessments were conducted by trained research assistants who were blinded to group assignments. A total of 20 students were excluded due to dropout (n = 6), missing or invalid data (n = 4), or an attendance rate below 25% (n = 10). In addition, the majority of children in the TPT (95%) and CLR (87%) groups were diagnosed with ASD or ADHD. Yet, only a limited number of children with SpLD (n = 5 in the CLR group and n = 1 in the TPT group) and borderline IQ (n = 1 in the TPT group) eventually completed the intervention. They were not equally distributed in the two intervention groups. To reduce heterogeneity between the two intervention groups, seven children with SpLD and borderline IQ were excluded. Finally, 35 children remained in the TPT group and 33 children in the CLR group for data analysis.
Outcome measures
Language
Rapid Automatic Naming (RAN) is an experimental paradigm adopted from Ebaid and Crewther's study that measures rapid letter naming. 37 Participants were asked to read aloud a 6 × 5 array of letters as fast and accurately as possible in 60 s. The total correct score and total errors were computed as separate measures of rapid naming speed and accuracy, respectively. Furthermore, the Chinese Vocabulary Test (CVT) was used to measure Chinese word knowledge. 38 Participants were required to verbally explain the meaning of 18 Chinese words. Each item was scored as “0”, “1”, or “2” and then added together to form a total score.
Working memory
The Number Span Test (NST) with forward (NST-F) and backward (NST-B) conditions was adopted to assess working memory. 39 Participants were read sequences of digits with an increasing span (from 2 to 12) and had to repeat in the same order as presented in the forward condition or reverse order in the backward condition. NST-B requires mental effort to manipulate information, whereas NST-F simply requires holding information temporarily without manipulation. Each condition had maximally 22 trials, and every trial with a correct answer earned one mark. The total score for each condition was computed separately by summing up the number of correct trials.
Sustained attention
The Digit Cancellation Test (DCT) was adopted to measure sustained attention requiring rapid visual tracking and accurate selection of target stimuli. 39 Participants were asked to cancel out as many “3” digits as possible in a two-page array of randomized digits (0–9) in 10 minutes. The total time (in seconds) taken to complete the task and the total score (i.e. correct cancelation minus commission errors) were computed as separate measures of processing speed and accuracy, respectively.
Learning and memory
The Hong Kong List Learning Test (HKLLT) was adopted to measure verbal episodic memory. 40 Participants were required to learn a verbally presented list of 16 two-character Chinese words across 3 learning trials, and then recall the words from memory after 30 minutes. The total correct recall across learning trials and the correct delayed recall were computed as separate measures of verbal learning and memory, respectively.
Interventions
Temporal processing tele-intervention
The online TPT program, developed by our research team, is operated by the Pro-talent Association Ltd in Hong Kong. It is a tele-intervention program that can be run remotely using a computer or tablet device. The tele-intervention program comprises two modules of TOJ-based intervention using tone or CV syllabic pairs separated by varying ISIs (ranging from 500 to 0 ms). In the tone training, each trial presents one of the four possible tone pairs (U-U, U-D, D-D, and D-U) composed of an upward-gliding (U) and/or a downward-gliding (D) tone. In the CV training, there are 36 possible CV syllabic pairs formed from 6 stop-consonant syllables (/ba/, /da/, /ga/, /ka/, /pa/, and /ta/) that involve a rapid formant transition (i.e. rapid frequency changes in the initial tens of milliseconds of the syllable). These syllables were adopted from the standard Bergen dichotic listening paradigm. 41
Each tele-intervention module begins with a practice session to familiarize the trainee with the sound stimuli and the intervention requirements. After passing the practice session, the program automatically proceeds to the training session. The training progresses in difficulty in a three-down-one-up adaptive procedure as the trainee's performance improves. That is, after every three consecutive correct responses, the trainee earns a star and is upgraded to a higher training sublevel with a reducing ISI from 500 to 0 ms; on the other hand, every single error would increase the ISI by one step. The tone and CV stimuli variants are synthesized using Audacity (version 2.2.2) 42 and Praat (version 6.1.11) 43 software. Completing every 20 steps of ISI variants leads to a shortened tone duration in the tone training and a reduced extension and amplification of formant transitions in the CV training. The ultimate goal is to accurately discriminate and sequence the tone at the shortest ISI and tone duration in the tone training and the initial CV syllables without modification in the CV training.
Throughout the training, the participants could replay the stimuli presentation anytime and received guidance from the instructor and assistants. They could choose to continue or quit the training program at any time. Responses were scored automatically, and feedback was provided for each trial. In the present study, the progress of intervention was measured in terms of the percentage of completion (maximally 100%) achieved by the participants. A higher percentage of completion reflects a better ability in temporal processing of auditory stimuli presented in rapid succession.
Conventional language remediation
CLR is composed of interactive teaching and computerized exercises focused on training Chinese reading and writing skills. The training materials were adopted from three standard teaching/training resources published by the Hong Kong Specific Learning Difficulties Research Team, 44 the Department of Special Education and Counselling at the Hong Kong Institute of Education, 45 and the Education Bureau. 46 They involved game-like computerized training programs to teach word recognition, 44 an online animated training program to teach narrative skills and reading comprehension, 46 and some mini-games and paper-and-pencil exercises to build Chinese vocabulary and writing skills. 45
Data analysis
The baseline characteristics and cognitive functions were compared between intervention and diagnostic groups using independent sample t-tests or chi-squared tests. When a confounding variable was identified, analysis of covariance (ANCOVA) was performed to control its effect on the dependent variable. The effects of TPT and CLR on each cognitive domain were compared across time by separate two-way mixed analysis of variance (ANOVA) with time (pre vs. post) as a within-subject factor and Group (TPT vs. CLR) as a between-subject factor. Further post hoc pairwise comparisons using paired t-tests were conducted to examine the specific changes in each group. Bonferroni-adjusted p-value at .025 for family-wise errors was applied to measures from the same cognitive test in mixed ANOVA and paired t-test.
Moreover, their pre–post difference scores (i.e. postmeasurement minus premeasurement) were compared between groups using independent t-tests. Partial eta squared (ηp2) and Cohen's d were presented to indicate the effect sizes. All statistical analyses were performed using SPSS 28.0 software.
Results
Baseline characteristics and cognitive performance
Table 1 presents the baseline demographic and clinical characteristics and level of cognitive functions of the two intervention groups. Both groups were matched based on age (t(66) = 0.12, p = .90), education level (t(66) = 0.33, p = .74), gender (χ2(1) = 0.19, p = .66), and diagnosis (χ2(1) = 0.30, p = .58). They also had comparable baseline cognitive functions (p > .05) (Table 1).
Participants’ characteristics and cognitive performance at baseline.

Children diagnosed with ASD or ADHD include those with a single diagnosis and those with other comorbidities.
n = 32.
n = 34.
ASD: autism spectrum disorder; ADHD: attention-deficit/hyperactivity disorder; CLR: conventional language remediation; CVT: Chinese Vocabulary Test; DCT: Digit Cancellation Test; HKLLT: Hong Kong List Learning Test; NST-B: Number Span Test-Backward; NST-F: Number Span Test-Forward; RAN: Rapid Automatic Naming; SD: standard deviation; TPT: temporal processing tele-intervention.
Further analyses were performed to examine whether children with ASD and ADHD had different baseline characteristics and cognitive functions. Table 2 shows that two diagnostic groups had comparable age (t(66) = −0.85, p = .40) and gender (χ2(1) = 3.84, p = .05), but the ADHD group had a significantly higher level of education than the ASD group (t(66) = −2.73, p = .008). With education level as a covariate in ANCOVA, the two diagnostic groups showed similar performance levels on many cognitive measures (p > .05) as shown in Table 2, except that children with ASD performed better than those with ADHD in the CVT total score (p = .002), the RAN total correct score (p = .007) and the HKLLT total learning (p = .001).
Baseline characteristics and cognitive performance of the two diagnostic groups.
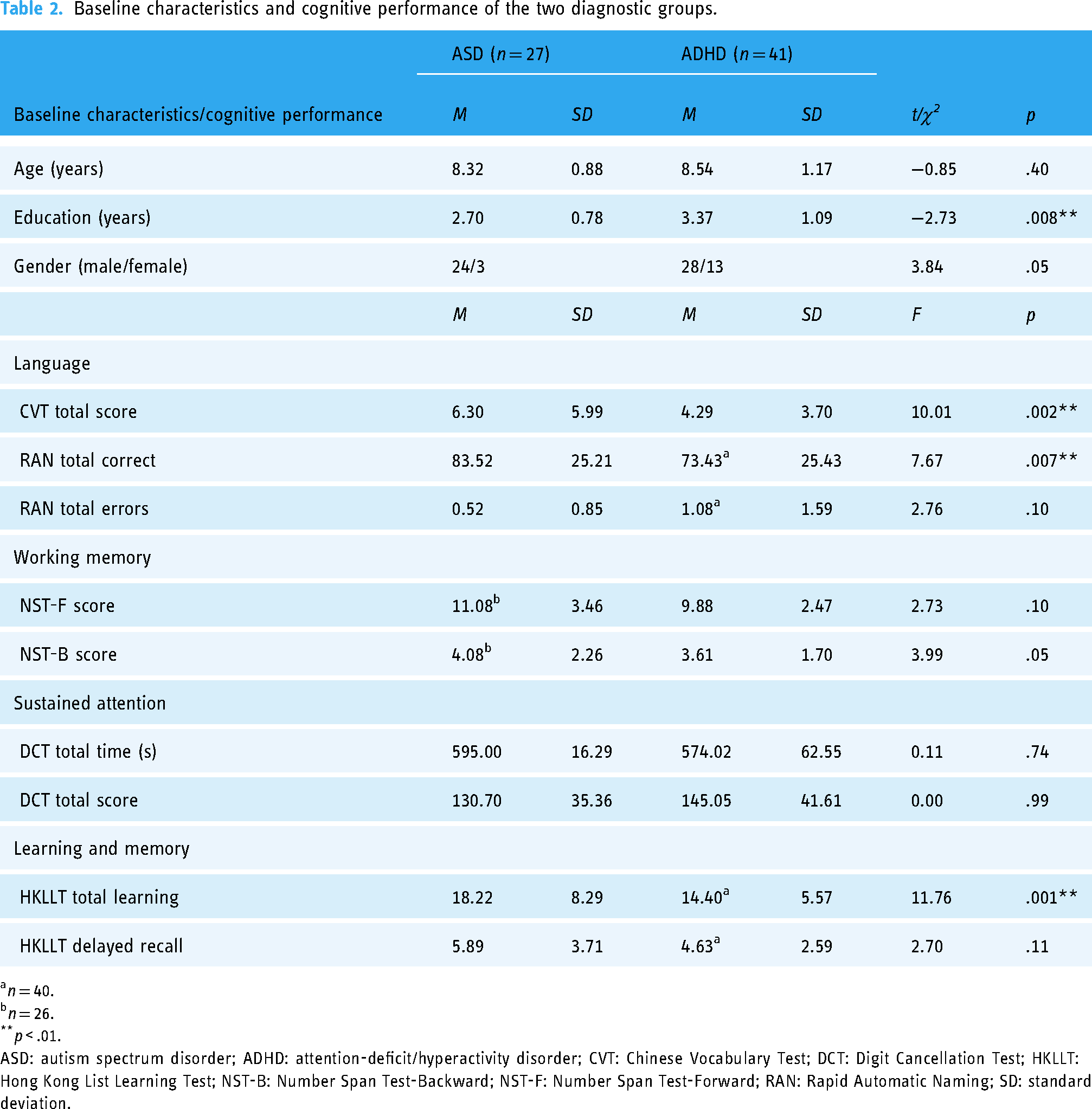
n = 40.
n = 26.
p < .01.
ASD: autism spectrum disorder; ADHD: attention-deficit/hyperactivity disorder; CVT: Chinese Vocabulary Test; DCT: Digit Cancellation Test; HKLLT: Hong Kong List Learning Test; NST-B: Number Span Test-Backward; NST-F: Number Span Test-Forward; RAN: Rapid Automatic Naming; SD: standard deviation.
Intervention attendance and progress
The TPT group (M = 77.4%, SD = 20.1%) and the CLR group (M = 81.7%, SD = 21.2%) had a similar attendance rate (t(66) = −0.85, p = .40). No adverse side effects were reported in both groups. On average, children in the TPT group completed 85.6% (SD = 27.5) of the tone training and 33.7% (SD = 39.0) of the CV training. The overall completion mean of the two training modules was 59.6% (SD = 27.9). While 71% of children completed 100% of the tone training, only 17% completed 100% of the CV training. Relatively fewer children have completed the CV module because many demonstrated difficulty discriminating the CV stimuli with a shortened formant transition, especially for stimuli that sounded closer (e.g. /ka/ vs. /ta/, /da/ vs. /ga/). Given the three-down-one-up adaptive procedure, few children could achieve a 100% completion rate of the CV training.
Improvement in language after TPT
Children who received TPT demonstrated a trend of improvement in rapid naming accuracy, as measured by the RAN total errors (Table 3). Results of two-way time×group mixed ANOVA showed a marginally significant main effect of time (F(1,65) = 4.84, p = .03) with Bonferroni-adjusted alpha value, and the effect size was medium (ηp2 = 0.07). Yet, there was a nonsignificant time by group interaction effect (F(1,65) = 0.04, p = .84). The marginally significant main effect of time suggests that children demonstrated a trend of fewer errors committed after both types of intervention. Though the multivariate results did not suggest a significant interaction effect, post hoc paired t-test showed that children who received TPT committed fewer rapid naming errors, which was marginally significant at Bonferroni-adjusted alpha value at .025 (t(33) = 2.04, p < .05). For the CLR group, the extent of error reduction was not statistically significant (t(32) = 1.37, p = .18). The present results suggest that children after receiving TPT seem to have a more apparent trend of committing fewer rapid naming errors than CLR.
Cognitive performance before and after CLR and TPT.

n = 32.
n = 34.
p < .025 (Bonferroni-adjusted alpha level for measures from the same cognitive test); ** p < .01; *** p < .001; d represents the effect size in terms of Cohen's d.
CLR: conventional language remediation; CVT: Chinese Vocabulary Test; DCT: Digit Cancellation Test; HKLLT: Hong Kong List Learning Test; NST-B: Number Span Test-Backward; NST-F: Number Span Test-Forward; RAN: Rapid Automatic Naming; SD: standard deviation; TPT: temporal processing tele-intervention.
Rapid naming speed, as measured by the RAN total correct score, also did not show a significant time×group interaction effect (F(1,65) = 2.00, p = .16), but demonstrated a significant main effect of time (F(1,65) = 31.07, Bonferroni-adjusted p < .001) with a large effect size (ηp2 = 0.32). Both groups named significantly more letters within the time limits (i.e. at a faster naming speed; TPT: t(33) = −4.38, p < .001; CLR: t(32) = −3.93, p < .001; Table 3), and their extent of improvement was also comparable (t(65) = −1.41, p = .16).
Word knowledge, as measured by the CVT total score, did not show a significant time×group interaction effect (F(1,66) = 0.01, p = .92), but demonstrated a significant main effect of time (F(1,66) = 52.68, p < .001) with a large effect size (ηp2 = 0.44). Both the TPT and CLR groups demonstrated significant improvement in word knowledge after intervention (TPT: t(34) = −5.60, p < .001; CLR: t(32) = −4.72, p < .001; Table 3). Compared to the CLR group, the TPT group showed a similar level of improvement in word knowledge (t(66) = 0.10, p = .92).
In summary, TPT and CLR significantly improve word knowledge and rapid naming speed of children with neurodevelopmental disorders. In addition, TPT has a more apparent positive effect on rapid naming accuracy.
Improvement in working memory after TPT
Two-way time×group mixed ANOVA showed a significant interaction effect on the NST-B score (F(1,65) = 4.87, Bonferroni-adjusted p = .03) with a medium effect size (ηp2 = 0.07). The main effect of time (F(1,65) = 22.45, Bonferroni-adjusted p < .001) was also significant. The results suggest that after the intervention, the TPT group, but not the CLR group, demonstrated significantly higher NST-B scores (t(34) = −4.85, p < .001) with a large effect size (Table 3). The increase in the NST-B score in the TPT group (+ 1.54) was 2.8 times that in the CLR group (+ 0.56), and the between-group difference in the score increase was statistically significant (t(65) = 2.21, p = .03, d = 0.54; Figure 1).
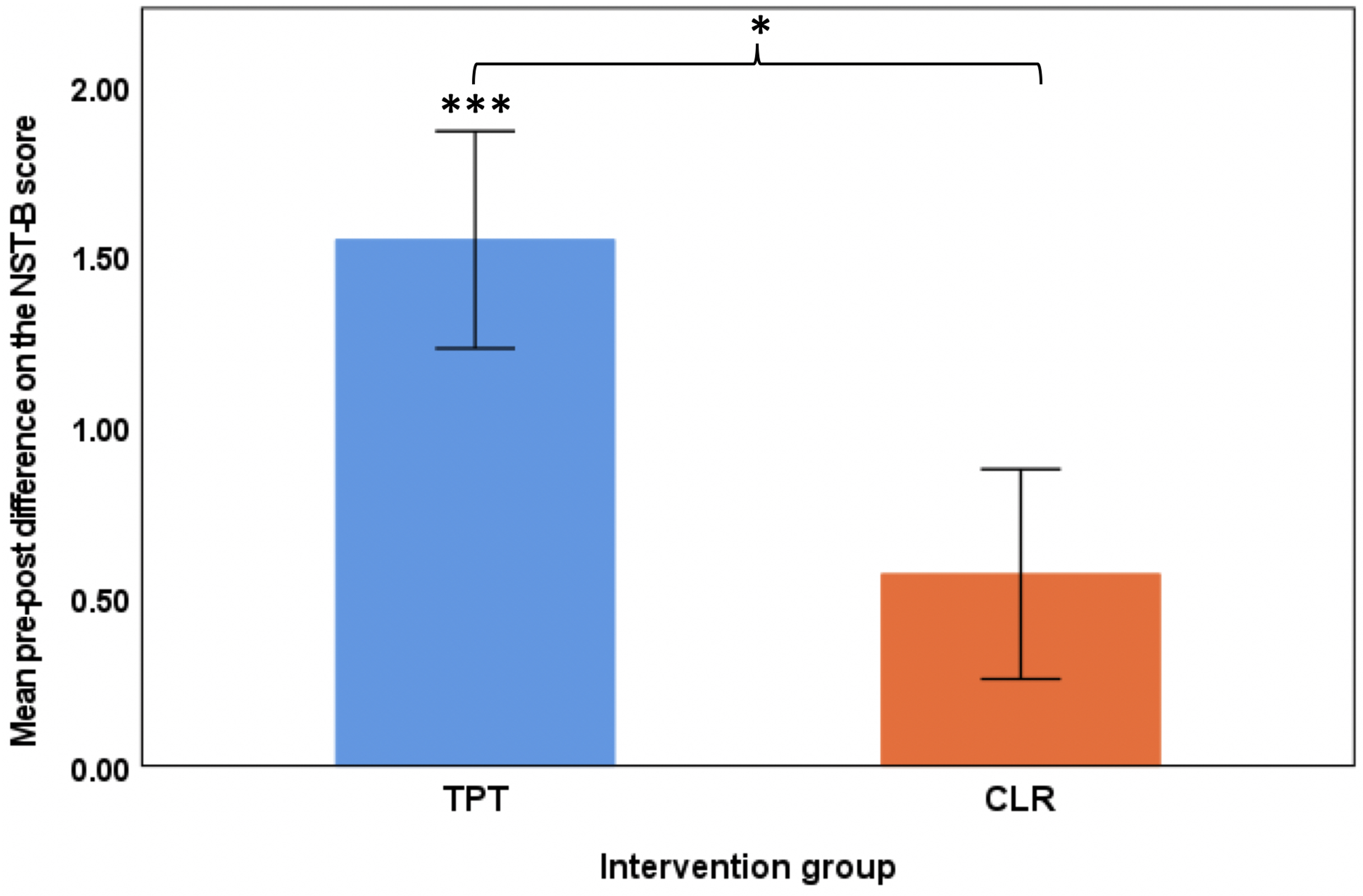
Performance changes on the Number Span Test-Backward score before and after the intervention. The pre–post difference score is computed as postmeasurement minus premeasurement, where a positive value indicates improved performance after the intervention The error bar represents the +/− 1 standard error of the mean. *** p < .001 indicates significant improvements in the NST-B score after TPT based on paired samples t-test with Bonferroni adjustment. * p < .05 indicates a significantly greater increase in the NST-B score after TPT compared to after CLR based on independent samples t-test.. CLR: conventional language remediation; NST-B: Number Span Test-Backward; TPT: temporal processing tele-intervention.
By contrast, there was no significant change in the NST-F score in any intervention group. The result of a mixed ANOVA did not show significant main and interaction effects for the NST-F score (F(1,65) = 0.02 and 0.08, p = .88 and .78, respectively). That means the positive effect of TPT is specific to the working memory that requires mental effort in manipulating auditory stimuli (i.e. NST-B) but not for simply holding these stimuli temporarily without mental manipulation (i.e. NST-F).
Improvement in sustained attention after TPT
The result of two-way time×group mixed ANOVA on the total completion time of the DCT did not show a significant time×group interaction effect (F(1,66) = 1.69, p = .20). Still, it demonstrated a significant main effect of time (F(1,66) = 8.14, Bonferroni-adjusted p = .006) with a medium effect size (ηp2 = 0.11). The significant main effect of time suggests that children could complete the task in a shorter time after both types of intervention. Although the interaction effect was not significant, the results of paired t-tests showed that the TPT group showed significantly faster speeds in canceling the target digits after intervention (t(34) = 2.66, Bonferroni-adjusted p = .012) with an effect size approaching medium level (d = 0.45), whereas the CLR group did not (t(32) = 1.27, p = .21, d = .22; Table 3). After TPT, children became 26 seconds faster in completing the DCT, which was 2.7 times the reduction in completion time in children receiving CLR (10 seconds less). Therefore, the TPT group tends to have a more significant positive effect on processing speed than the CLR group (Figure 2).
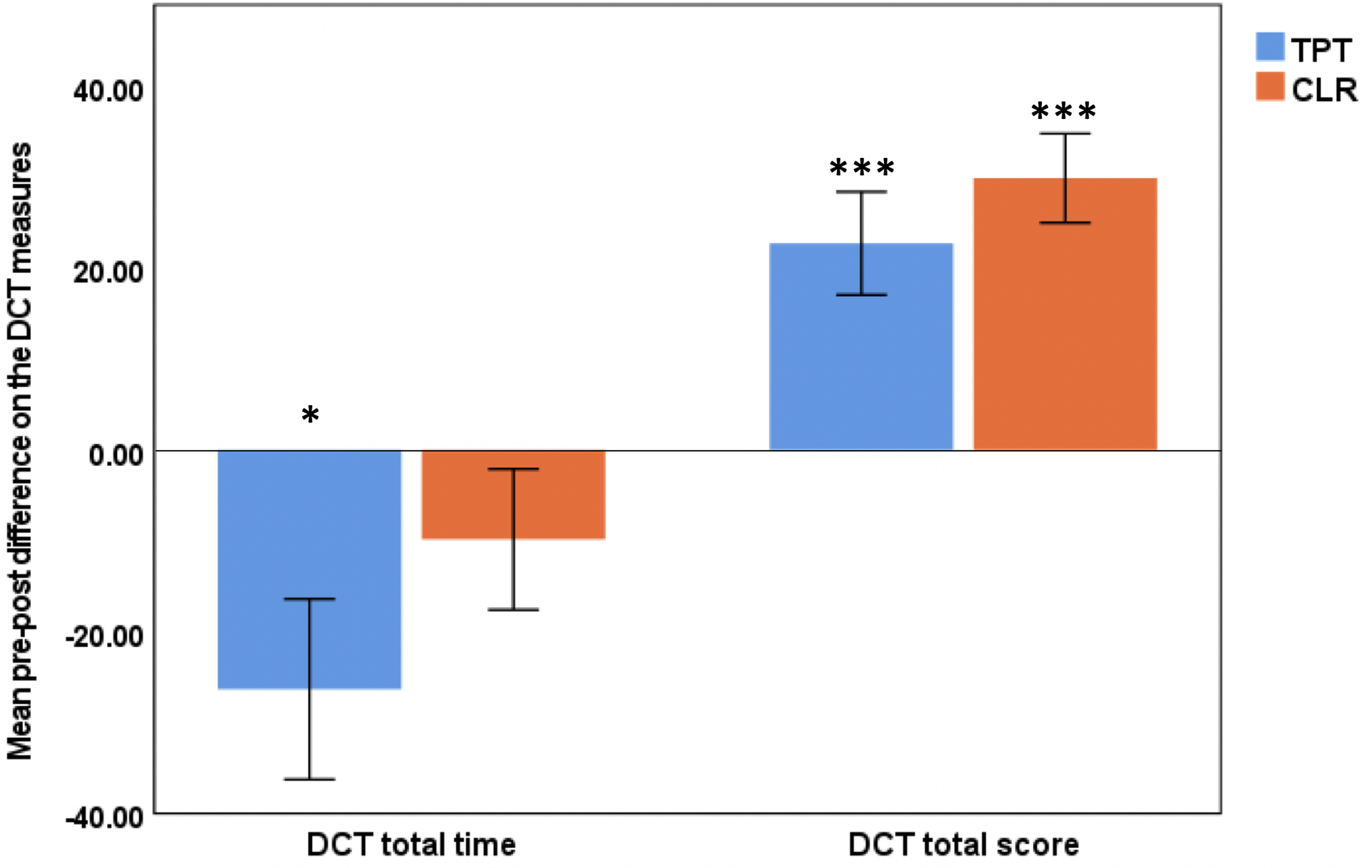
Performance changes in the measures of the Digit Cancellation Test before and after the intervention. The pre–post difference score is computed as postmeasurement minus premeasurement, where a negative value for the DCT total time and a positive value for the DCT total score indicates an improvement after intervention. The error bar represents the +/− 1 standard error of the mean. * p < .05 indicates a significant reduction in the DCT total time after TPT based on paired samples t-test with Bonferroni adjustment. *** p < .001 indicates a significant increase in the DCT total score after both types of interventions based on paired samples t-test. CLR: conventional language remediation; DCT: Digit Cancellation Test; TPT: temporal processing tele-intervention.
Moreover, children not only work faster but also better. The result of two-way time×group mixed ANOVA on the DCT total score showed a significant main effect of time (F(1,66) = 48.60, Bonferroni-adjusted p < .001) with a large effect size (ηp2 = 0.42), though the time×group interaction effect was not significant (F(1,66) = 0.90, p = .35). The TPT group showed a significantly higher DCT total score after intervention (t(34) = −4.00, p < .001), and a similar improvement was also observed in the CLR group (t(32) = −6.09, p < .001; Table 3).
In summary, in a sustained attention task, the TPT and the CLR programs show similar significant improvement in accuracy. Although both groups of children complete the task in a shorter time, TPT, as compared to CLR, may have a higher impact on processing speed in children with neurodevelopmental disorders, given its significant pre–post difference after Bonferroni adjustment.
Improvement in learning and memory after TPT
Both the TPT and CLR groups showed improvements in verbal learning and memory after intervention (Table 3). For total learning and delayed recall measured with the HKLLT, the results of two-way time×group mixed ANOVA did not show a significant time×group interaction effect (total learning: F(1,65) = 1.23, p = .27; delayed recall: F(1,65) = 1.56, p = .22), but demonstrated a significant main effect of time (total learning: F(1,65) = 27.96, p < .001; delayed recall: F(1,65) = 30.37, p < .001) with Bonferroni adjustment. Children with neurodevelopmental disorders demonstrated significant improvement in verbal learning and memory after TPT (total learning: t(33) = −3.06, p = .004; delayed recall: t(33) = −3.11, p = .004) and CLR (total learning: t(32) = −4.37, p < .001; delayed recall: t(32) = −4.63, p < .001). The extents of their improvement in verbal learning (t(65) = −1.11, p = .27) and memory (t(65) = −1.25, p = .22) were comparable. Given that children were exposed to a learning environment on Chinese literacy in CLR, this may facilitate their ability to learn and memorize new Chinese words. However, children who received TPT were not provided with any direct intervention on learning and memory but still demonstrated significant enhancement in verbal learning and delayed recall to an extent similar to CLR.
Discussion
This study showed that children with ASD and ADHD demonstrated improvement in language, working memory, sustained attention, and verbal learning and memory through remote online training on their temporal processing skills. The improvement in working memory requiring mental manipulation of auditory stimuli was specific to TPT but not CLR. There was an overall improvement in sustained attention in terms of processing speed and rapid naming accuracy after the intervention; however, the statistically significant pre–post difference after receiving TPT but not CLR might suggest that TPT seemed to have a more apparent trend of improvement. Improvements due to TPT also extended to word knowledge, rapid naming speed, sustained attention in terms of accuracy, verbal learning, and memory to a degree comparable to those after CLR. These findings suggest that TPT has positive effects on various cognitive functions of children with ASD and ADHD and that the enhancement in working memory is specific to TPT. Therefore, remote online training on auditory temporal processing can be a potential intervention for enhancing the cognitive functions of children with ASD and ADHD.
While previous studies primarily provided in-person TPI,24–29 the present study has added knowledge regarding the possibility and effectiveness of a web-based TPT that can be delivered remotely for children with neurodevelopmental disorders. Other studies have also reported the benefits of remote online intervention for children with neurodevelopmental disorders.33–35 For instance, Aloizou et al. 33 found that 7 to 15-year-old children with autism who attended an online game-like educational program combined with a video conferencing platform for 1 to 2 months demonstrated more significant achievement in reaching their learning goals. Therefore, the web-based mode of intervention may provide a more flexible and extensive approach for reaching children with neurodevelopmental disorders, making intervention more accessible for children in lower-income classes or living in remote areas. The remote modality of TPT may be more cost-effective than in-person training, as the children can do the training independently or with limited assistance from adults at home. Therefore, it may reduce the intervention cost as the required staff will be reduced. Since TPT is less dependent on language and culture; therefore, it can be applied to children in different countries. In addition, the remote TPT allows children in less advantaged backgrounds (i.e. developing countries) to receive training that may benefit them.
The positive effects of auditory TPT on rapid naming and word knowledge found in the present study were in line with some previous studies.24,27,28 For instance, Wang et al. 27 found that TPI exhibited significant correlations with rapid naming and corresponding reading-related abilities among Chinese children with dyslexia. A meta-analysis has reported a moderate-to-strong relationship between rapid automatized naming and reading performance. 47 Besides, the RAN test has been reported to be significantly loaded in both phonological processing and processing speed component in principal component analyses among Chinese dyslexic children. 48 Therefore, it is postulated that temporal processing training that targets improving perceptual processing in the time domain as short as in milliseconds may probably facilitate faster and more accurate letter naming in the RAN test. Tallal et al. 24 also reported improved speech discrimination and comprehension after TPI for children with a language-learning impairment, suggesting that children can process and understand others’ speech more accurately. It is postulated that more efficient tone and speech processing may facilitate children's better learning and understanding of new vocabulary. While the previous interventions were face-to-face, the present study further suggests that TPI can be conducted remotely and yields similar effects.
Apart from the language domain, the present findings are also consistent with previous studies that have reported enhancements in sustained attention, 30 working memory,31,32,49 and verbal learning and memory.31,32,49 However, the present study differs from those studies in terms of participants’ characteristics, intervention intensity, and the complexity of intervention modules. Many of these studies trained healthy older adults for 32 to 40 sessions,30–32,49 4 to 5 days per week for 8 to 10 weeks, yet the present study offered less intensive intervention (20 weekly sessions for 8 months) to children with neurodevelopmental disorders. In addition, previous studies provided intervention programs comprising at least six to nine intervention modules,30–32,49 spanning from simple acoustic tasks (e.g. TOJ of rapidly successive frequency-modulated sweeps) to complex manipulations of continuous speech (e.g. narrative memory). Hence, the positive outcomes are mixed results from different forms of TPI, and the unique contribution of TOJ-based intervention remains unknown.
The results of the positive effects of TPT on children's working memory and sustained attention are particularly encouraging. Children with ASD 50 and ADHD 51 are commonly found to have impairment in working memory and sustained attention. In addition, the capacity of working memory has been reported to be a strong predictor of cognitive development in childhood,52,53 learning outcomes in literacy and numeracy,54–56 and overall academic performance. 57 Therefore, an appropriate and practical intervention that can enhance working memory may facilitate the learning of children with neurodevelopmental disorders and, in the long run, reduce the gaps in cognitive functions and academic performance between children with neurodevelopmental disorders and their peers.
Despite the encouraging findings, there are a few limitations to this study. First, this study only examined the immediate effects of TPT. Whether such positive outcomes can be maintained after intervention warrants future follow-up studies. Second, it is unknown whether cognitive enhancements after TPT and CLR are also related to natural neurodevelopment or learning through education for 8 months. Therefore, it is worthwhile to include a waitlist control group in future studies to explore this issue. Third, without applying neurophysiological measures in this study, the neural mechanisms underlying the positive effects of TPT remain unknown. Thus, further studies applying technologies such as electroencephalogram or functional near-infrared spectroscopy can be conducted to shed some light on intervention-related neural responses. Last but not least, the present study did not include an additional outcome measure of temporal processing ability per se; thus, how the improvement in temporal processing might contribute to the enhancement of cognitive functions remains inconclusive. Therefore, future studies may include different temporal processing measures and examine their association with training-related cognitive performance changes.
Conclusions
Temporal processing deficits found in ASD and ADHD have been proposed to be a possible factor mediating their cognitive impairment in attention, memory, and language. While in-person TPI was reported to improve various cognitive functions in children, the present study has found similar positive effects of remotely delivered web-based TPT on children with ASD and ADHD. Children after receiving TPT, but not CLR, demonstrated a specific enhancement in working memory. The TPT group shows a greater impact on rapid naming accuracy and sustained attention in processing speed than the CLR group. In addition, the TPT group showed significantly improved word knowledge, rapid naming speed, sustained attention in terms of accuracy, and verbal learning and memory, to an extent similar to that of the CLR group. The present findings suggest that web-based TPT may be a potential intervention for improving cognitive functions in children with neurodevelopmental disorders.
Footnotes
Acknowledgements
The authors would like to thank Quin Chan, Christy Cheung, Kenneth Lai, Katie Leung, Evan Lau, Tsz-Lok Lee, Camelia Ding, and Natalie Auyeung for collecting data and/or preparing and assisting with the group intervention for this study. Further appreciation is extended to the school principals and teachers for their recruitment of participants and all forms of support throughout the experiment, as well as to all children and parents for their participation.
Contributorship
ASC contributed to the conception and design of the study. SLS contributed to data acquisition and management. ASC and SLS contributed to the formal analysis of data and drafting of the manuscript. All authors contributed to the interpretation of the data and the review and editing of the manuscript. All authors approved the final version of the manuscript.
Data availability
The dataset generated and analyzed during the current study is available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first author (ASC) is the founder of Pro-Talent Association Ltd. The other authors have no conflicts of interest to disclose.
Ethical approval
The Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee approved this study (CREC reference number: 2020.501-T).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Lee Hysan Foundation Ltd.
Guarantor
ASC