
Abstract
Introduction
Developmental language disorder (DLD) is a neurodevelopmental condition characterised by persistent and pervasive challenges in daily communication. This paper describes the process of designing a digital word-learning intervention for this population that aligns with routine clinical practice, is evidence-based, and has strong theoretical rationale.
Method
The intervention design process involved research collaboration between academics, clinicians and software professionals.
The Medical Research Council's framework for developing complex interventions provided preliminary guidance; greater design depth was introduced by adding recommended elements from a synthesis of intervention design literature. The resulting intervention design was refined with focus group feedback from speech and language therapists, which underwent reflexive thematic analysis.
Results
Intervention design features were generated by aligning word-learning traits characteristic of the disorder with evidence-based vocabulary intervention strategies and clinician requirements for embedding digital practice in routine service-delivery.
Mock ups for a mobile intervention app were developed from the design features and shared for refinement with practicing speech and language therapists who had day-to-day experience of supporting children with DLD.
Conclusion
This paper outlines the process of defining the therapeutic components of a digital intervention, guided by empirical literature and clinician insights. These initial findings will serve as a foundation for co-designing with children with DLD to shape the final design, particularly in terms of motivation and engagement features.
Investing at the design stage in the determinants of successful translation of research into practice, increases the likelihood that the resulting intervention will demonstrate both research effectiveness and clinical uptake.
Keywords
Introduction
Developmental language disorder (DLD) is a neurodevelopmental condition that results in significant, ongoing challenges in everyday communication. 1 It is estimated to affect 7% of children, 2 and is a heterogeneous disorder with nature and severity varying not only between children but also within a child influenced by internal physiological and psychological mechanisms and external social and environmental factors.3–5 DLD can occur in isolation or alongside other neurodevelopmental disorders with broad aetiology such as Attention–Deficit/Hyperactivity Disorder and Dyslexia. 1 Difficulty with word learning is characteristic of almost half of all children with DLD, 6 and is predictive of limitations in wider areas of language, literacy, academic attainment, social skills, and general well-being.7–9
Empirical literature suggests that children with DLD struggle to associate the social, perceptual, cognitive and/or linguistic signals that help match sounds to meaning during word learning. 10 For example, a child with DLD who is shown a bottle of antibiotics and a stethoscope for the first time may struggle to differentiate the words when told one is worn by a doctor. This is because they must determine the answer by combining their knowledge of object properties with what they are able to see (i.e., only one can be ‘worn’). Difficulties processing signals for language acquisition may present as immature, as divergent or both.
The role of technology
The World Health Organisation reports significantly increased interest and adoption of digitally delivered health and care in many countries since widespread remote working measures were introduced during the COVID-19 pandemic. 11 In particular, this has led to greater exploration of interventions being introduced through mobile devices given their ubiquitous nature, convenience and affordability.12,13 With regards to word learning, user-friendly mobile devices present the opportunity for children with DLD to create and access multimedia content relating to a target word, i.e., through text, images, audio and video. It is hypothesised that this would support the cross-situational, multisensory cue integration required for optimum vocabulary acquisition.
There are some indications of the potential of digital vocabulary interventions in existing research involving school-aged children with DLD when technology-enhanced vocabulary interventions have been compared with traditional paper-based approaches. For example, one study 14 targeted word learning by introducing relevant video content on mobile devices as well as through books, and reported significantly greater gains in the understanding, naming and defining of target words with the use of multimedia compared to reading alone. A limitation was that the children played a passive role due to the target words and video content being pre-selected by the researchers. Another study 15 introduced a custom-made digital aid which enabled children to independently access the sound of initial letters of target words as needed during word learning, alongside strategies introduced by a speech and language therapist (SLT). The study reported significantly greater gains in the accurate naming of words when compared to SLT input alone. Whilst this finding is promising, the technology was limited to providing audio cues only.
It must be noted that the response to digital stimulus during word learning may be dependent on the child's presenting profile. One study which explored the use of images and videos to support word learning, reported a significant correlation between severity of language difficulties in children with DLD and the extent to which background music interfered with word learning. 16 This indicates that any digital vocabulary intervention would need to be adaptable to individual language and learning needs.
In addition to the digital content of an effective vocabulary intervention, research should focus on current digital clinical practice to identify core design requirements. Here the needs of the intervention provider are fundamental for translating empirical efficacy into practice.17,18 The provider is responsible for interpreting research findings, planning how the results can enhance practice, and evaluating meaningful impact. Despite this pivotal role, a systematic review of digital interventions for children with communication difficulties identified that the requirements for the intervention provider, most commonly the SLT, to effectively deliver the intervention tended to be overlooked. 19 To overcome this gap in the literature, much can be learned from the numerous profession-wide surveys of paediatric SLTs which have explored digital service delivery during and since the remote-working measures of the COVID-19 pandemic, including work by the primary author of this paper.20–24 A consistent theme from the surveys is that a key influencer of technology uptake is its consideration as routine practice across the profession. As a result, identifying positive drivers to the adoption of technology in care which are used consistently across paediatric SLT services and incorporating these within the intervention design is of great importance.
These service-level requirements can then be refined by sharing early-stage intervention prototype designs during in-depth focus groups with SLTs who specifically support word learning in children with DLD. This aligns with empirical recommendations that considering provider requirements which are both profession-wide and client-specific will lead to a more sustained and effective approach to the design, development and adoption of digital solutions.19,25
Developing a complex intervention
Interventions for children with DLD are complex, not only because they must cater to the heterogeneity of the population, but also due to the range of possible delivery models with variability of place, person, resources, and activities. 26
Intervention programmes are predominantly led by SLTs who deliver evidence-based therapy in partnership with parents, educators and psychologists. Given the pervading nature of communication, therapy may be provided in a range of settings such as the home, school or clinic. Words targeted by such interventions should be relevant to the child, such as their interests, school curriculum and family routine. 27
The UK Medical Research Council (MRC) provides guidance on the development and evaluation of complex interventions used in health and care services.28,29 The guidance is presented over four phases: development, feasibility/piloting, evaluation and implementation. For the development phase, the MRC framework advocates the use of evidence and theory to model the processes and outcomes that constitute a complex intervention.
Bleijenberg et al. 30 extended the MRC framework by adding intervention design guidance with the aim to improve clinical uptake. Recommended additional steps include clearly defining the presenting condition and its implications, determining the needs to be addressed by the proposed intervention, and understanding current practice (Figure 1). The resulting coordinated list of intervention requirements can guide features for the novel intervention. As highlighted by SLTs with experience of designing digital interventions for children with disabilities, this stage requires input from specialist software designers and developers to generate appropriate technical requirements. 31 The final output of the design process is generally a proposed prototype of the intervention. 30

The research described in the current paper combined the MRC complex intervention development guidance28,29 with recommended elements from the intervention design literature as defined by Bleijenberg et al. 30 to generate required content for a digital word-learning intervention for children with DLD. Through collaboration with specialist software designers and developers, design mockups were then created which were used to produce an intervention app prototype. This was shared with paediatric SLTs actively supporting children who have DLD with word learning and the therapist feedback used to refine the intervention design.
In line with best practice guidance when developing digital therapy tools for children with additional needs,32–34 the intervention design will also incorporate specifications obtained from children with DLD. An integrative approach is planned whereby clinical- and evidence-based practice will define the therapeutic framework for the intervention as reported in this paper. These intervention mechanics will serve as a skeleton to which contributions from children with DLD around making the therapy motivating and engaging will be added. As such, work subsequent to this paper will involve co-design sessions with children who have DLD to understand their views and preferences around word learning. This will provide necessary content to form a complete intervention design.
This paper therefore aims to report on two areas:
Phase 1 – The design of a digital word-learning intervention informed by existing theory and research. Phase 2 – Clinician feedback on the novel intervention design and how this led to further refinement.
Method
The Guidance for Reporting for Intervention Development Studies in Health Research (GUIDED) 35 was followed to comprehensively describe the intervention design process and to ensure completeness of reporting (Appendix A).
Phase 1 – Intervention design
The MRC intervention development guidance28,29 and synthesised intervention design guidance 30 helped generate design ideas for a digital word-learning intervention for children with DLD. This phase was undertaken by the authors who in addition to being researchers were qualified paediatric SLTs (RA and RH) and a health psychologist (MC). The work was completed over a period of 18 months and involved desktop research and remote team calls to work through the steps below.
Profiling the disorder
Word learning traits common in children with DLD were identified and related to corresponding models of language learning theory. The profile of presentation was drawn from a multinational and multidisciplinary consensus study of criteria and terminology for children with language difficulties 1 and related literature.4,5,10,36–40 Contributors to the consensus included SLTs, educational psychologists, psychiatrists, paediatricians and specialist teachers.
Identifying the evidence
A systematic review of articles published between 1990 and 2023 reporting on vocabulary intervention outcomes for primary-school-aged children (5–11 years) with DLD was completed. 41 The review identified intervention strategies with indications of effectiveness and considered implementation factors that may influence efficacy (e.g. nature of targeted words, dosage, provider and location).
Examining existing practice
A review of existing profession-wide surveys of paediatric SLT digital practice was conducted. The review considered national surveys conducted during the COVID-19 pandemic (2020–2021) to allow learning from the wide-scale adoption of technology during the pandemic.
Findings from the surveys were synthesised and analysed using the Capability, Opportunity, Motivation and Behaviour (COM-B) model. 42 This provided a theoretical framework to identify behaviour change drivers to support the digital intervention being adopted as part of standard practice.
Modelling the process and expected outcomes
Strategies to target specific areas of need and anticipated change processes were identified. These presumed causal pathways for the intervention were synthesised in a logic model to demonstrate the relationship between intervention activities for word learning and expected vocabulary outcomes. Contextual factors which could influence intervention response were also described.
Defining intervention features
This stage involved collaboration between the research team (authors of the paper: RA, RH, MC) and a private software company, to consider the digital intervention features required to achieve word-learning efficacy and intervention uptake as informed by existing empirical literature.
Specifications included the prompts, interactions and interfaces needed for the digital intervention to achieve optimum effectiveness. The design scope extended beyond technological requirements to identify intervention design principles such as accessibility and usability standards.
Phase 2 – Clinician feedback and refinement
In this phase, feedback on a word-learning intervention prototype created from design ideas generated in Phase 1 was obtained from the professionals who would implement the intervention in practice, paediatric SLTs. Reference was made to the Reflexive Thematic Analysis Reporting Guidelines 43 (RTARG) to provide conceptual and methodological coherence in the analysis and reporting of findings (Supplement 1).
As the work was necessarily exploratory, a focus group was conducted with results of interest being views that supported or opposed existing intervention features. In line with RTARG recommendation, rather than seeking consensus, an inductive interpretivist paradigm was adopted, which assumed multiple subjective and separately constructed responses to the intervention prototype that would require interpretation.44,45 The positionality of the researchers within the fields of SLT and health psychology was balanced by having the lead software designer facilitate the running of the focus group and support data analysis in order to provide a technical lens. The goal was for the SLT feedback to be interpreted by the researchers and software designer using their professional knowledge and findings from existing literature to guide intervention refinement.
Target population and sample size
The participant eligibility criteria comprised qualified paediatric SLTs with a minimum of 6 months of experience, currently supporting word learning in school-aged children with DLD.
Based on established guidance for focus group research,46,47 this study aimed to recruit between 6 and 8 participants for the group in order to have enough people to generate varying opinions and perspectives and small enough to allow each individual to participate fully and be heard.
Consent and ethical considerations
Approval for this study was obtained from the School of Health and Psychological Sciences Research Ethics Committee, City St George's, University of London, UK (ETH2122-0815).
All participants received detailed information about the purpose of the study beforehand and gave written and verbal consent. Participants were informed that their participation in the study was voluntary and that all responses would be anonymised for confidentiality. They were advised of their right to withdraw from the study at any time up to analysis without any negative implications.
Recruitment
Purposeful sampling was used by approaching a school-based SLT service within one London borough. With the permission of the service manager, an email with a cover letter and information sheet was sent to relevant team members. Written consent was obtained from six paediatric SLTs actively supporting word learning in school-aged children with DLD who expressed an interest to participate in the study.
Procedure
A focus group discussion guide was used based on a template for novel intervention approaches developed and validated by Krueger and Casey46,47 who are considered experts in the field of focus group research (Supplement 2).
The focus group began with an introduction by the primary author (RA) who highlighted the purpose and aims of the research. This was followed by a demonstration of the digital word-learning intervention prototype by the lead software designer. After this, SLT feedback was gained using questions from the discussion guide read by the primary author.
The focus group session lasted approximately 90 min and was concluded when it was agreed by all six participants that relevant areas had been fully explored.
Setting
The focus group took place in a meeting room at the community base for the participating clinicians in Wandsworth, London. The rationale was guidance from Kruegar and Casey 46 that familiar settings are likely to elicit more open discussions.
Data collection and analysis
Clinician views were audio recorded during the focus group and then later transcribed with identifying information removed. The transcription underwent reflexive thematic analysis using explicit semantic coding based on expert guidance by Braun and Clarke. 44 In keeping with the purpose of the research, i.e., to refine intervention design requirement, this involved seeking and coding text interpreted as relating to the strengths of the intervention design or areas requiring refinement. The codes were then collated into prominent themes to provide greater understanding of participant feedback.
Transcripts were coded by the primary author in consultation with the lead software designer. Themes were then developed and refined by the research team (authors of the paper: RA, RH, MC) and the lead software designer using direct quotations to capture the reflections and recommendations of the participants. The analysis process concluded when it was agreed by the research team that saturation had been reached, i.e., all relevant codes and themes had been generated from the data.
The findings guided targeted refinement of the intervention design as reported in the results section of this paper.
Results
Phase 1 – Intervention design
Profiling the disorder
A comprehensive description of the disorder helped define the multifaceted profile of vocabulary difficulties in children with DLD.
Details of presentation (Table 1, Column 1: DLD Profile) extended beyond types of word errors, 1 to include underlying processing mechanisms and environmental factors that may be influencing observed difficulties as this would impact the intervention approach. This included the effect of attention, 1 memory,1,36 literacy, 37 social responsiveness38,39, and self-management,1,40 on word learning as well as the influence of the saliency, frequency and consistency of sound and meaning cues.1,10,39
Defining the clinical population, evidence-based support strategies, and the intervention features to elicit desired changes.
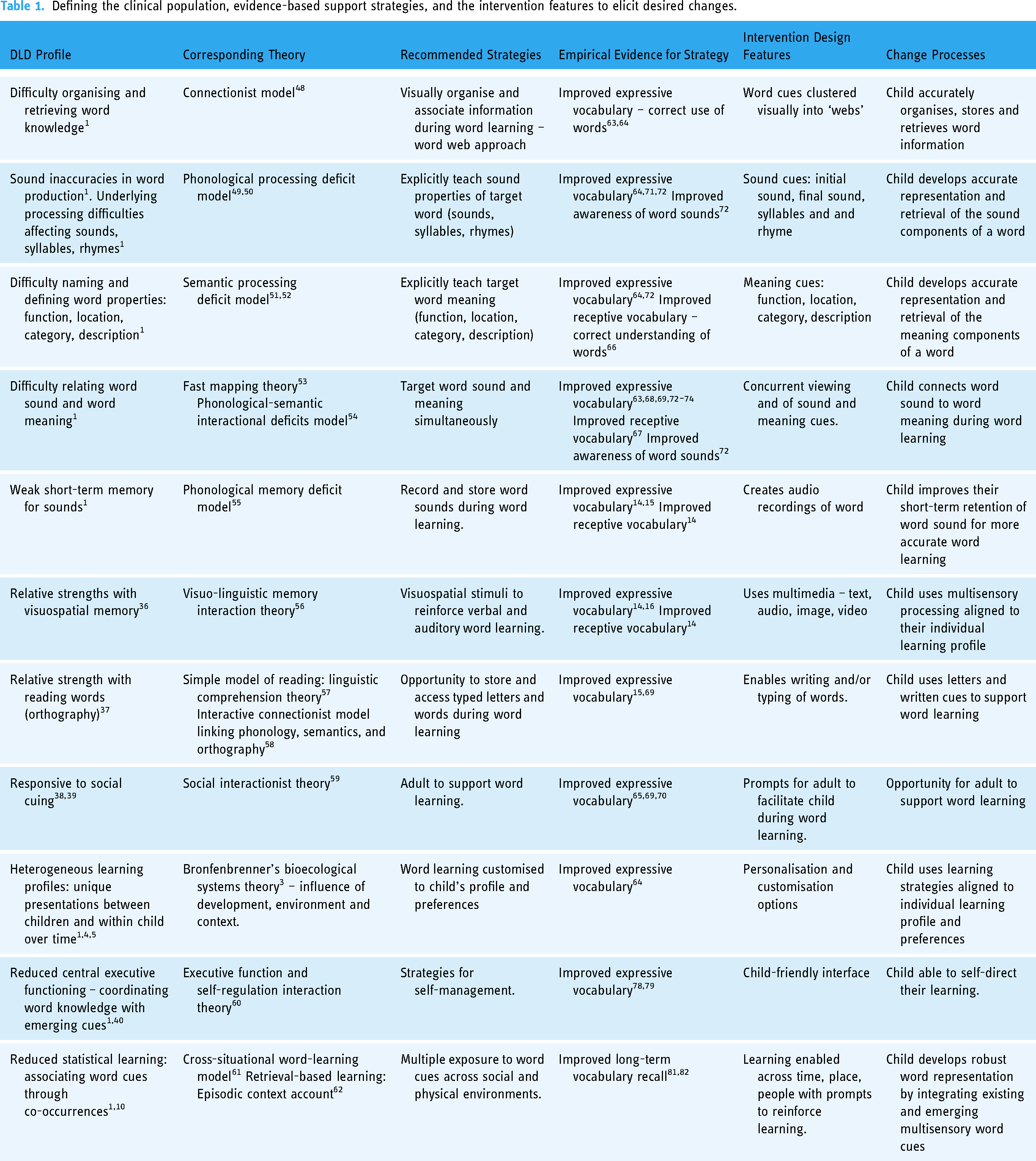
To guide intervention targets, theoretical models were identified which corresponded to the presenting profile and provided possible explanation for the characteristics described (Table 1, Column 2: Corresponding Theory3,48–62).
Identifying the evidence
Existing vocabulary intervention studies involving children with DLD, as synthesised in a systematic review, 41 helped collate recommended strategies for the proposed intervention.
The review 41 identified twelve interventions delivered in English (UK,15, 63–68 US,14, 69–71, New Zealand 72 ), two in Dutch (set in the Netherlands 16 ), one in French (set in Switzerland 73 ) and one in German (set in Germany 74 ); providing collective data for 288 participants (167 males, 78 females, 43 unknown).
Most studies were of medium design quality, and this, coupled with the small number of studies identified, means that practitioners should be guided by response to treatment as well as the research findings when applying the intervention in practice.
Word-learning strategies with the greatest indication of effectiveness were extracted from the review and are reported along with the study source and the targeted area of difficulty (Table 1, Column 3: Empirical Strategies and Column 4: Empirical Evidence for Strategy).
One approach, known as word-web therapy, stood out in the systematic review due to being described as popular in clinical practice as well as demonstrating significant word-learning gains during clinical trials appraised as having good quality.63,64 Word-webs resemble an approach commonly known as mind maps 75 and involve using diagrams which arrange sound and meaning properties around a target word to visually represent networks of association.
A key feature of word webs which was also found to effectively improve word-learning in several other studies, was the simultaneous and explicit targeting of the sound and meaning properties of words.63,67–69,72–74 Additional word-learning gains were reported when contextual cues were provided in the form of written text, narratives and during social interactions.65,69,70 Effectiveness also improved when strategies aligned to the child's presenting profile of word-learning difficulties (sound errors, meaning errors, both) and corresponding needs. 64
Three of the reviewed papers used multimedia (audio, images and videos)14–16 to effectively support word learning. Two of the three multimedia intervention papers14,16 referred to Mayer's Cognitive Theory of Multimedia Learning 76 and corresponding instructional design principles to guide intervention development. 77 The design principles optimise cognitive processing during multimedia learning by (i) minimising extraneous processing demands such as background noise that may be distracting, (ii) facilitating intrinsic processing through tasks that are accessible and manageable, and (iii) optimising novel processing using cues to align acquired and existing knowledge.
An important finding from the systematic review was specificity in intervention response, gains generally did not transfer to non-targeted words15,63–65,73 and showed depreciation once therapy ended.15,64,65,68,70,73 This finding guided requirements for developing the novel intervention, for example, ‘self-management’ was included as a recommended word-learning strategy to avoid ongoing dependency on therapists.78,79 The metalinguistic awareness required for this self-cuing is unexpected to develop before age seven, 80 implying that the novel intervention will be most appropriate for children of upper primary school (age 7–11 years). A further strategy was the opportunity for retrieval practice across social and physical environments to reduce depreciation of learning and improve long-term vocabulary recall.81,82
The review summarised the factors which may affect intervention response, including relevancy of target words, dosage, provider and location. These have been recorded as influencing factors in the novel intervention design (see Moderating Factors in Figure 2).
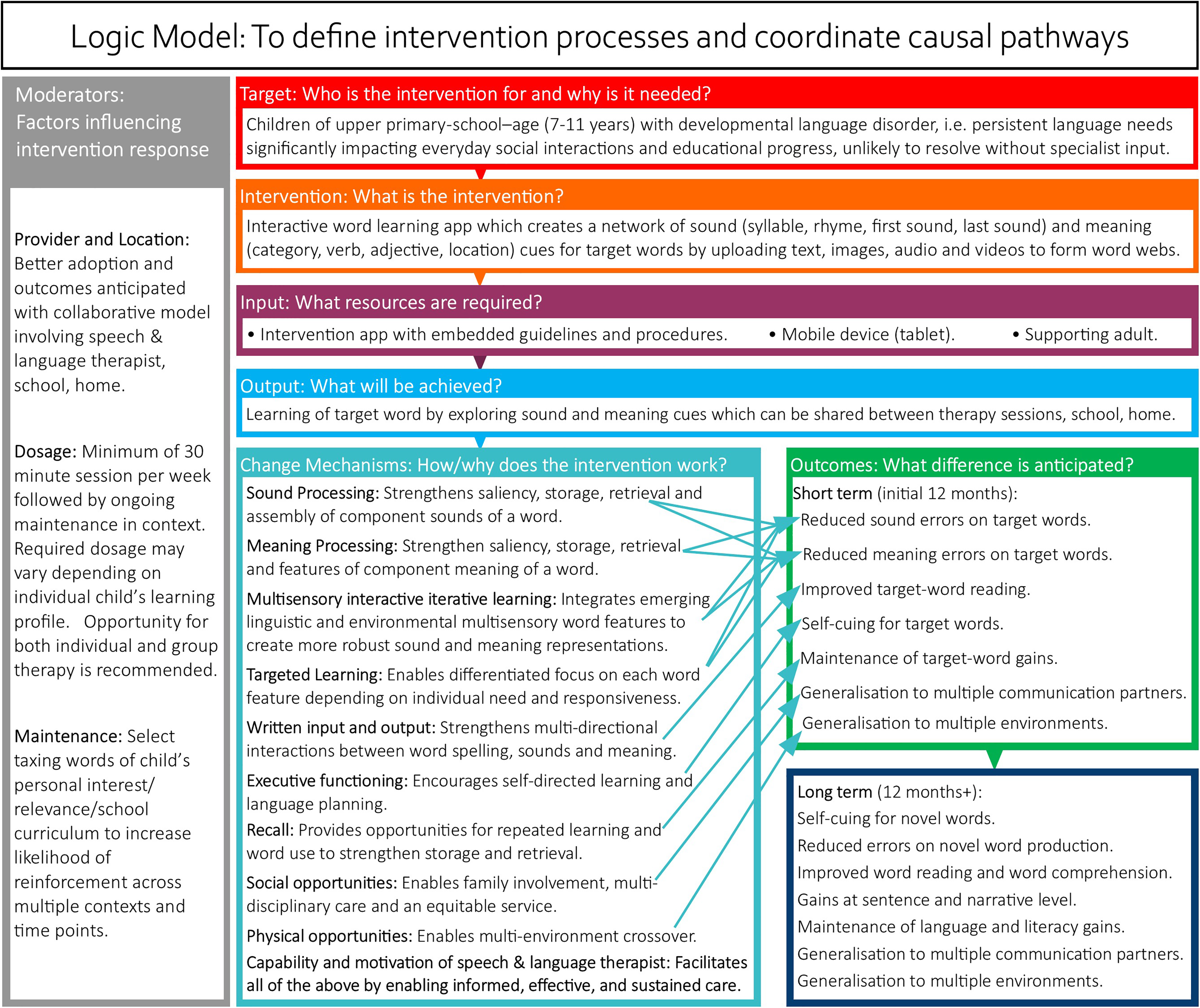
Logic model for a digital word-learning intervention to support children with DLD.
Examining existing practice
A review of existing surveys identified five studies that collectively reported over fifteen hundred survey responses from paediatric SLTs regarding their views and experiences of digital practice during and since the extensive remote working measures introduced in response to the COVID-19 pandemic. The surveys spanned the UK- (n = 424; n = 438),20,21 US (n = 269; n = 259),22,23 and Hong Kong (n = 135). 24
Where measured, the surveys consistently indicated an increase in clinician's perception of their frequency, convenience and confidence with digital practice following COVID-19 compared to before the pandemic.20–23 However, the surveys also indicated a range of challenges to digital uptake, as well as measures that would facilitate overcoming the obstacles to embedding the use of technology in routine care.
A series of requirements were identified to embed the mobile word-learning intervention into regular service delivery by paediatric SLTs (Table 2, Column 1: Requirements for Routine Digital Practice). These requirements were based on areas of consensus for factors facilitating routine digital practice as reported in the reviewed surveys. Examples included ensuring that the digital word-learning intervention enables involvement of families and partner professionals so that there is alignment with standard paediatric SLT practice.
Clinician requirements to support adoption of the mobile word-learning intervention in routine digital clinical practice.
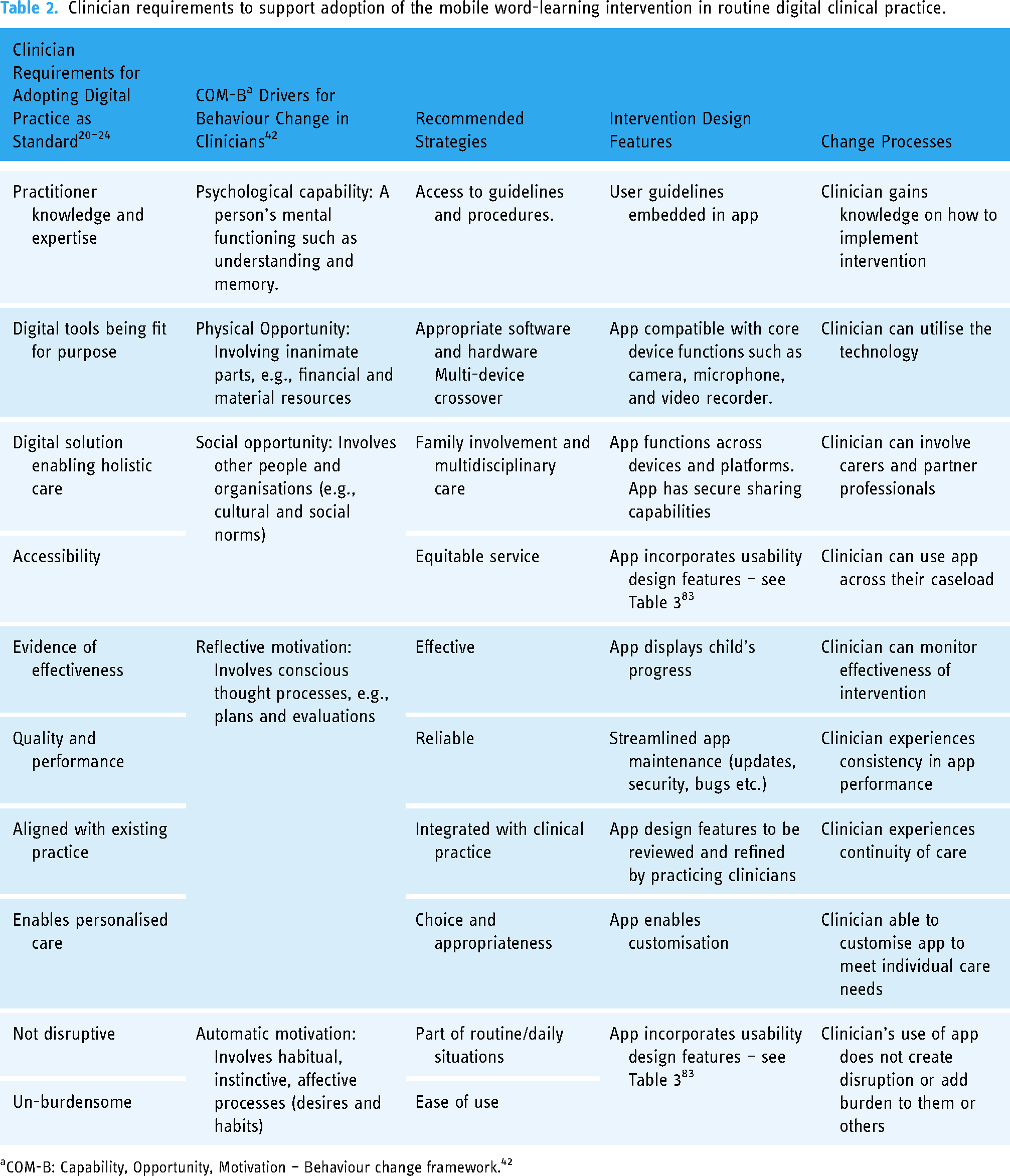
COM-B: Capability, Opportunity, Motivation – Behaviour change framework. 42
The COM-B 42 framework of behaviour change drivers was applied to organise the requirements by type: Capability – clinician skills and knowledge; Opportunity – convenience, suitability, accessibility; and Motivation – effectiveness, quality, continuity (Table 2, Column 2: COM-B Drivers for Behaviour Change in Clinicians). Corresponding strategies were then identified to facilitate the behaviour change required for the adoption of the digital word-learning intervention as part of regular service delivery (Table 2, Column 3: Recommended Strategies). For example, multi-device crossover functionality to ensure that the intervention can be accessed by carers and partner professionals in a range of settings.
Modelling the process and expected outcomes
Expected change processes were modelled to link each area of need with recommended strategies (Table 1, Column 5: Change Processes; Table 2, Column 4: Change Processes).
This informed a logic model to illustrate the relationship between the components of the intervention (Figure 2). The model defines the target group, intervention approach, intervention resources, expected outputs and desired outcomes. Change mechanisms within the model propose how and why the components of the intervention may work. Factors influencing change processes are listed to highlight contextual moderators.
Defining intervention features
This stage considered the digital design features required for intervention efficacy and clinician acceptability. Table 1 (Column 6: Intervention Design Features) charts how technology could create an interactive word-web tool which, through transition from adult-guiding to self-cuing, would support a child with mapping word sounds and meaning using multimedia text, audio, image, and videos created and viewed across place, and time.
Table 2 (Column 5: Intervention Design Features) focuses on features for implementation of the intervention in routine practice, such as embedded guidance, interoperability, app performance, and alignment with care pathways. Best practice compliance requirements were generated from Shaban and Pearson's Learning Design Framework 84 which aligns Mayer's Cognitive Theory of Multimedia Learning, 76 as utilised by existing vocabulary intervention studies,14,16 with user-centred principles specifically for children with learning disabilities (Table 3). 83 The framework and its application to intervention design have been validated and evaluated empirically.84,85
Usability principles and guidelines when designing applications for children with learning disabilities from Shaban and Pearson's Learning Design Framework, 83 (pp4–6) (with permission).

Phase 2 – Clinician feedback and refinement
Intervention prototype
Figure 3 presents mock-ups of the key intervention components created using a collaborative app prototype design tool known as Figma Design. 86 These were shared for feedback during a focus group with paediatric SLTs who routinely employ word-learning strategies to support children with DLD.

(a–e) Intervention Mockup. From clockwise top left: (a) Home screen. (b) Word cues screen. (c) Content upload. (d) Range of uploaded content. (e) Summary of learning.
The mobile app is designed for SLTs to introduce to children with DLD when supporting word learning during therapy. Therapy sessions at school are routinely attended by support staff such as teaching assistants who can then reinforce app use during the school day as and when word-learning support is needed. Similarly, therapists can model the app to parents who can support the child at home. The aim is for the child to move from adult facilitation to independent app use so that they can self-cue during word learning.
In terms of technical features, the intervention is developed as a web-based app that is accessible across multiple platforms, browsers, and devices, but optimised for tablets, as children are more likely to access these both at school and at home. Since the app is delivered through a browser, it does not need to be downloaded or installed, saving storage space. Additionally, app maintenance - including updates, security management, troubleshooting, and bug fixes - can be managed in real time.
The prototype mock-ups were not intended to cover all design requirements generated in Phase 1, but rather to provide a scaffold from which therapist feedback, based on their experience supporting word learning in children with DLD, could guide further design iterations. Below is a summary of the features presented to the therapists:
A word-learning intervention app prototype in the form of interactive word-webs, which create networks of sound and meaning cues for target words by uploading text, images, audio and videos in a structured and synchronised manner. On the home screen, children start by typing a personally chosen word and creating or uploading an image they associate with that word (Figure 3(a)). This leads to a screen of word cues: sound (first sound, last sound, syllables, rhymes) and meaning (category, adjectives, verbs, location). The child selects the cue they wish to explore (Figure 3(b)). The next screen allows the child to create, upload and replay multimedia content (text, image, audio, and video) related to the selected sound and meaning feature of the personally relevant word (Figure 3(c)). Content can be built up over time (Figure 3(d)). A summary screen shows the learning for each cue (Figure 3(e)). The app is designed to enable children with DLD to build up a bank of meaningful words. It is organised logically so that it can be accessed, added to, and shared across different time points and environments.
Participant characteristics
Table 4 summarises key participant demographics and demonstrates that the paediatric SLTs provided a varied sample in terms of specialism and experience.
Participant information (paediatric speech and language therapists).

Summary of thematic analysis
The focus group data was categorised into three overarching sections in line with the purpose of the study, i.e., to inform the intervention: design strengths, design weaknesses, design suggestions. Within each category prominent themes were defined, and these have been reported below with direct quotations to allow greater understanding of the clinician feedback.
Category 1: Design strengths
The therapist's first impressions were positive. There was praise for the visual structure of the app (Theme 1), the use of features to enable customisation (Theme 2), and the opportunity to create and save resources more conveniently than with paper-based interventions (Theme 3).
The therapists found that the logical, minimalist design helped make the app intuitive to use.
‘I like the graphics. I think it's quite nicely laid out and quite easy to use’ (Participant 5).
‘What you need to click on and what you can fill is really clear’ (Participant 2).
The use of muted background colours was also seen as a positive as it was ‘not overwhelming or distracting’ (Participant 3).
The therapists welcomed that the app enabled children to add personalised content relating to a target word using their preferred modalities (audio, images, video).
‘They (the children) can easily capture what's around them at school and just use’ (Participant 2).
‘I think children would be more motivated because they love working with tablets. “Oh, look that's our voices” and that's probably more memorable for them. It's not the Teaching Assistant writing things down on a piece of paper. They're creating it and experiencing the learning’ (Participant 6).
‘When you look at the style of learning of the young people we work with, it is so much more visual, multi-sensory based, and what this does is allow you to access that multi-sensory experience really quickly and easily’ (Participant 1).
The ways in which a mobile app enables more efficient and convenient implementation of word-learning activities compared to traditional paper approaches were discussed.
‘The resources can be produced without going to too much effort with preparing. So, if you want action pictures, you have to go in and get pictures from the school … whereas on a tablet you can just quickly take them and then talk about it’ (Participant 2).
‘It's good … practically as well because you don't have to worry about printing resources in advance … you've got it all on the iPad’ (Participant 4).
‘The Teachers can have it out whenever the child's doing their writing or they can go back to it if they've forgotten about the word so it's like a prompt … always there if needed which makes things a lot easier’ (Participant 3).
Category 2: Design weaknesses
Areas requiring improvement included greater clarity for the user (child and supporting adult) on the purpose of the app (Theme 1), better alignment to existing language learning approaches (Theme 2), and more comprehensive monitoring and reviewing of progress (Theme 3).
For example, therapists felt that certain wording used to describe activities was open to interpretation.
‘It is better if things are explicit, rather than expecting the adult or children to infer what they should do. So instead of “Write something here” if you want the child to type a word on the first page, put “Tap to type a word” as the prompt’ (Participant 4).
In addition, an illustration to represent word cues was considered too abstract for the children to understand or relate to which could lead to disengagement.
‘Pictures as cue icons I think are really good, but the image that's been chosen for hand clapping to represent syllables, it's quite abstract compared to photos of actual hands’ (Participant 6).
The app design presented to the therapists organised word sounds and meaning cues separately. Whilst the therapists felt that this provided visual balance and symmetry, they commented that it did not accurately represent therapeutic practice where cues circle the central target word.
‘I think I anticipated looking like what our word learning usually look like. Obviously, it's a different format, but I wonder if our kids are maybe not going to be using the app all the time, if they're using paper word webs in class, then it’ll be confusing’ (Participant 3).
Therapists also felt that if the app intervention only focused on individual words rather than also considering the use of those words in sentences then this would restrict the strength of gain and benefits.
‘I think using well in a sentence is often the biggest teller of whether they've understood the word’ (Participant 5).
Therapists highlighted the influential role that progress markers play in therapy as they ‘motivate the children by allowing them to track their achievements’ (Participant 5).
Therapists also stated that being able to monitor progress is important for planning purposes and for providing updates to parents/carers and other professionals.
‘I'll usually get vocabulary lists from teachers, and rate them with the children to determine what they've already looked at, what they already feel confident with, then decide which we're going to be looking at together. I then have a bank of words to which I add ratings and progress to share with the children and with teachers’ (Participant 3).
In addition, a mechanism for reviewing and reinforcing gains was called for.
‘I think being able to revise the words is key. I really liked the ways you can explore words, but I worry that once you walk away from it, you weren’t prompted to return’ (Participant 1).
A need for a range of summaries of learning was also commented on. Whilst a summary screen showing the complete word web for a particular word was available, the ask extended to all words targeted by an individual child and across all children on a certain therapist's caseload or attending a certain school.
Category 3: Design suggestions
A range of features were proposed to enhance the app. The suggestions aimed to better explain to users what the app is for (Theme 1), to motivate the child (Theme 2), and to assist professionals with caseload management (Theme 3):
The use of prompts to highlight key features that were both written and verbal using a text-to-speech feature was advised. This is integrated into many familiar technologies and enables text to be converted into speech sounds imitative of the human voice.
There were calls for embedded tutorials to clarify app purpose and use.
‘An explanation for everybody who uses the app would be really helpful … reduce confusion and inconsistency’ (Participant 3).
The use of games, trophies and more child-centred features were suggested.
‘They’re so used to video games; they might want to see some of what they enjoy already to make them want to use this’ (Participant 2).
However, the importance of a balance between engaging and distracting was discussed.
‘Just thinking about all the stuff kids like to play with online. How can we add some of the motivators but without it being confusing or too much’ (Participant 6).
Therapists suggested embedding a vocabulary measure within the app which could be completed at baseline and repeated as required with the date stamped.
Summary screens and dashboards were requested to demonstrate progress made at the level of caseloads, schools and individual children. These should be easy to share with parents/carers and other professionals both electronically and through print outs.
‘Because we're in multiple schools we need more just one page with all the users. Instead, perhaps having per school, so opening a school folder and then having all the users that would be easier to navigate or filtering all users by school’ (Participant 4).
Design refinements following clinician feedback
Findings from the clinician feedback have led to the following updates which are summarised visually in Figures 4–6:
(a and b) Updated intervention mock-up: onboarding tutorials for parents and professionals. From top down: (a) Background information. (b) Step-by-step guide.
App prompts
- Onboarding tutorials for parents and professionals have been added (Figure 4(a): Background information, Figure 4(b): Step-by-step guide)
- Text-to-speech features have been added enabling the children to click and hear written words.
- In-app prompts (images and text) have been updated to be more explicit and understandable (for example Figure 5(a)).
(a–d) Updated intervention mockup. From clockwise top left: (a) Home screen. (b) Word test. (c) Arrangement of word cues. (d) Achievement pop-up.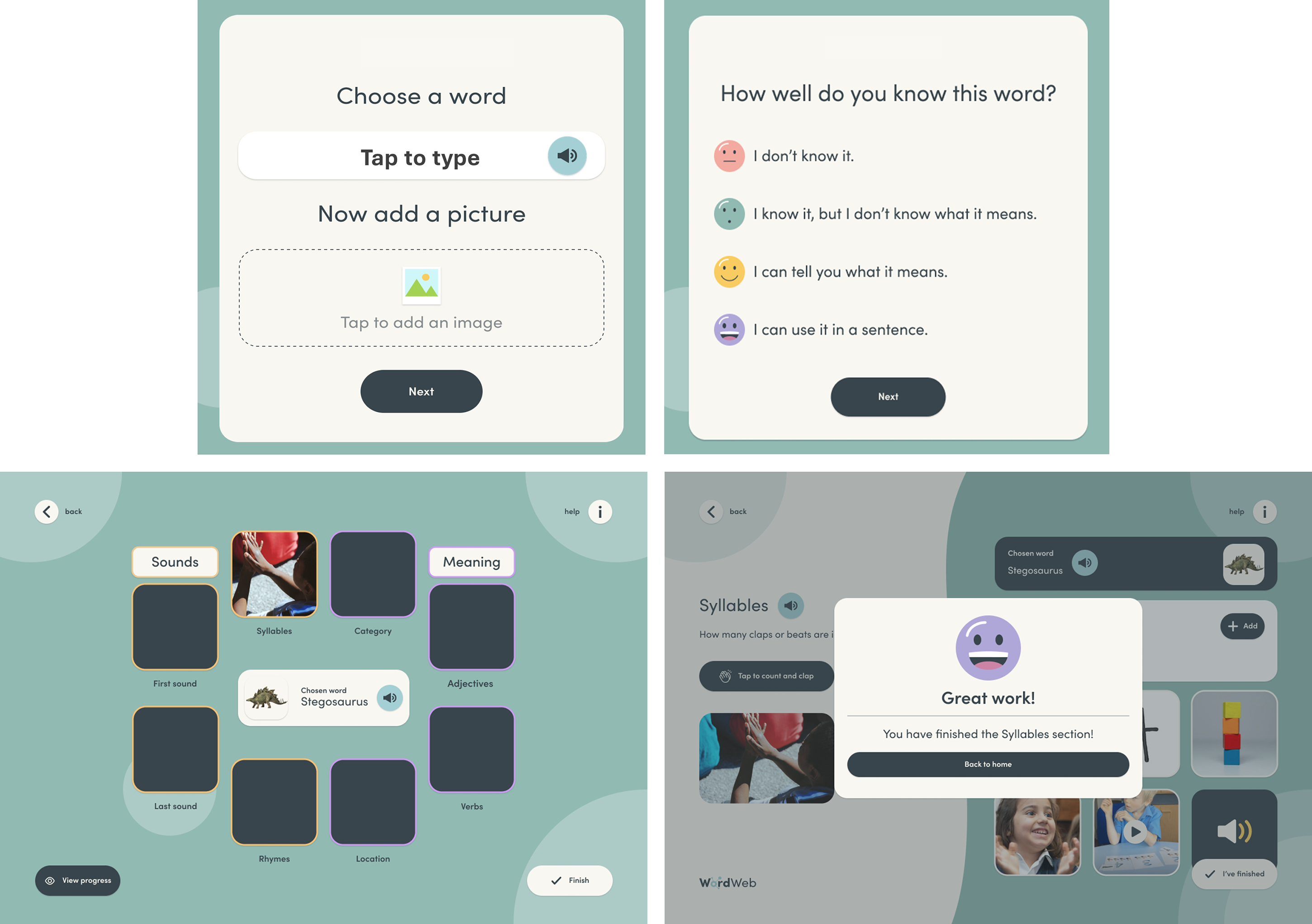
Monitoring progress
- An empirically advocated baseline vocabulary assessment which can be repeated at any time has been included (Figure 5(b)).87–89
- A therapist dashboard has been added which includes summary information per child (Figures 6(a)–(b)).
(a–b) Updated intervention mockup. From top down: (a) Therapist dashboard. (b) Summary per child.
Therapy approach
- The word-learning cues have been arranged in a circle around the target word to align with the paper-based word web format commonly used in current practice (Figure 5(c)). 64
- Prompts to practice the target word in sentences have been added.
Child engagement
- Achievement pop-ups have been added which appear following completion of activities (Figure 5(d)). Design ideas for further engagement features will be sought through separate co-design sessions with children who have DLD as described in the Introduction section of this paper.
Discussion
This paper describes how the design of a digital word-learning intervention for children with DLD has been informed by empirical evidence and practitioner experience.
Interventions for this population are complex due to diversity in presentation and variability of intervention contexts. 26 This creates a tension in intervention design research between fidelity of replication and the need to tailor interventions to be sensitive to different delivery models.
To address this challenge, the MRC complex intervention development framework28,29 and complimentary design guidelines 30 were adopted to create a digital word-learning intervention based on theory, research, and existing surveys of professional practice. The empirically informed intervention design was then refined using feedback from therapists actively supports word learning in children with DLD. This approach has led to an intervention design that combines robust research literature with the day-to-day implementation experience of therapists as discussed further below.
A customised intervention
DLD represents a heterogeneous condition with presentation influenced by multiple biopsychosocial factors.4,5 To account for this, the intervention has been designed to align strategies according to types of word-learning difficulties (sound errors, meaning errors, both) and preferred learning styles. Practitioners will therefore be able to personalise the therapy according to the individual needs of the children being supported. This feature makes it unique from digital word-learning interventions in existing studies14–16 and ensures agreement with best practice guidance for DLD vocabulary interventions48,64 and mobile health and care applications.12,13
Evidence-based design
Word-learning strategies for the intervention were derived from a systematic review of intervention efficacy studies and related work involving children with DLD. 41 This ensured that the design was grounded in research evidence.
However, as reported by Utianski et al., 90 practicing SLTs consistently cite lack of contextual considerations as a barrier to translating findings from field studies to clinical care. To address this, factors influencing the implementation of evidence-based word-learning strategies such as location, provider, intensity, and opportunities for reinforcement, were considered as part of the intervention design. This replicates the inclusion of contextual moderators when defining evidence-based strategies for novel interventions that have been reported, albeit sparingly, in the existing literature. For example, McKean et al. 91 worked with paediatric SLTs and health visitors to develop a hybrid face-to-face and digital intervention to promote children's language development within the home environment. Evidence-based techniques were selected for the intervention by carefully considering which strategies from systematic and scoping reviews could be applied routinely by caregivers. This was done to increase the likelihood of intervention uptake.
Routine service delivery
To ensure relevancy to the clinical landscape in which the intervention would be delivered, the surveyed experiences of paediatric SLTs following the rapid, widespread adoption of technology in response to COVID-19 remote working measures were considered.
A unique research perspective emerged from these existing surveys, as therapists were able to reflect on their experience of digital practice at scale as opposed to following specific clinical trials which would have generally been the norm for digital intervention research previously. For example, therapists extended their evaluation of digital solutions beyond individual episodes of care to broader implications such as barriers to extending digital care models to families and partner professionals.
These wider requirements helped identify design features for the digital word-learning intervention to not only support initial uptake amongst clinicians but also effective and sustained adoption within complex care pathways. This is important as estimates indicate that less than half of clinical innovations ever make it into standard service delivery despite demonstrating research effectiveness. 92
Mapping change processes
In keeping with the complexity of the population and their needs, several theoretical models and frameworks informed the change mechanisms underpinning the intervention design.
For example, rather than referring to a single language learning model, a range of language processing theories were selected which correspond to the range of word finding needs and presentation observed in children with DLD. This is in keeping with current empirical thinking around multiple, interacting etiological pathways influencing vocabulary development in children with DLD.64,93,94
In addition, a behaviour change framework was applied to the surveys of professional digital practice to understand the capability, opportunity and motivation that paediatric SLTs require to embed technology within routine service delivery. This approach replicates work by Stringer et al. 95 who used a behaviour change framework to understand the needs of paediatric SLTs in order to transform their regular service delivery model. In that case, the goal was the introduction of collaborative interventions with teachers rather than adoption of technology in care. With both studies, a list of intervention requirements were identified which were anticipated to facilitate change in routine practitioner practice.
The theoretical assumption of how and why the intervention would be effective were synthesised to inform a logic model of intervention processes which coordinated the therapeutic content, the recipients, the context, the outputs and expected outcomes. Existing digital therapeutic research has demonstrated that this structured approach to modelling intervention components makes it easier to identify potential gaps, inconsistencies, and areas of improvement during later evaluation and implementation stages.96,97
Bridging the gap between clinicians and software professionals
This study uniquely combined clinical and technical thinking to generate app design features which met word-learning efficacy requirements. As explored by informatics researchers Du and Tekinbas, 31 growth in technology adoption by SLTs has generally not been matched by increased collaboration with software experts. This has resulted in therapists often attempting and failing to adapt mainstream applications for use during specialist interventions. 98 A gap in shared epistemology between clinical and computer sciences has been proposed as a barrier to jointly designing digital interventions. 31 The research in this paper was able to overcome this issue by synthesising frameworks and guidance from both fields as well as ensuring that clinical academics and software professionals worked together to interpret data relating to intervention design features.
Clinician feedback
Gaining the views of therapists who regularly implement word-learning interventions whilst still at the ideation stage proved to be a valuable and informative step. Areas not yet considered were added to the design, increasing the likelihood of adoption in practice. These design amendments were made easily without substantial time or resource implications, which is significant as lengthy and expensive delays in the journey from research to practice has been attributed partly to inefficient research methodologies.90,99 Furthermore, in research that has included SLTs among other health care workers, clinician contribution to digital intervention design has been identified as an influencing factor for care providers when selecting a preferred solution. 100
Limitations
As the intervention design is heavily informed by the evidence on current interventions and practice, the process inevitably suffers from the same limitations as these sources of information. With regards to vocabulary intervention effects, the greatest weaknesses identified in the systematic review were limitations with the quantity and quality of studies. 41 As such, the evidence of efficacy should be treated with caution and intervention outcomes monitored closely during delivery. Similarly, the findings from the surveys of clinical digital practice which have guided the intervention design, provide a snapshot of service delivery by a sample of the profession at particular points in time.
Another important consideration is that the work in this paper provides partial design features for the final intervention. The therapeutic elements will be further shaped and enhanced by the design views of children with DLD. End-user contributions will predominantly guide motivational and engagement aspects such as the design of child-friendly app prompts, symbols for word-learning cues, and progress markers. As discussed by researchers who have undertaken similar work designing interventions for neurodiverse children, the merging of empirical, clinical and end-user perspectives is complex as it requires careful orchestration between different disciplines, generations and contributions. 33 Equality of influence may not always be achieved, and in previous studies, it is often the views of the children that are marginalised.32,33 As an alternative to therapy-driven approaches when creating digital products to facilitate neurodiverse children, some researchers have called for experience-driven design where the child's preferences drive technical specifications. 101 Given the dearth of research in the intervention design space, there is learning to be gained from having a range of methodologies and as the field becomes more established future work could focus on comparing approaches.
Conclusion and next steps
This paper describes how design ideas for a digital word-learning intervention were generated from theory, research and practice through collaboration between academics, clinicians and software professionals.
A subsequent study will identify design requirements generated by children with DLD to ensure that the resulting intervention is motivational and engaging. This will be followed by usability testing as a precursor to clinical evaluation trials.
These research stages will create new knowledge to iteratively influence the design, development, evaluation and adoption in routine practice of the digital word-learning intervention.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251324442 - Supplemental material for Designing a digital intervention for children with developmental language disorder: Aligning theory, research and clinical practice
Supplemental material, sj-docx-1-dhj-10.1177_20552076251324442 for Designing a digital intervention for children with developmental language disorder: Aligning theory, research and clinical practice by Rafiah Ansari, Ros Herman and Martin Cartwright in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251324442 - Supplemental material for Designing a digital intervention for children with developmental language disorder: Aligning theory, research and clinical practice
Supplemental material, sj-docx-2-dhj-10.1177_20552076251324442 for Designing a digital intervention for children with developmental language disorder: Aligning theory, research and clinical practice by Rafiah Ansari, Ros Herman and Martin Cartwright in DIGITAL HEALTH
Footnotes
Contributorship
RA researched literature and conceived the study. RA, RH and MC were involved in gaining ethical approval, and data analysis. RA wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
A private software company, Big Lemon®, provided technical expertise.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Approval for this study was obtained from the School of Health and Psychological Sciences Research Ethics Committee, City St George's, University of London, UK (ETH2122-0815).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The primary author, RA (Clinical Doctoral Research Fellow, ICA-CDRF-2018-04-ST2-029), was funded by the Health Education England/National Institute for Health Research (NIHR) for this research project. The views expressed in this publication are those of the authors and not necessarily those of the NIHR, NHS or the UK Department of Health and Social Care.
Guarantor
RH.
Supplemental material
Supplemental material for this article is available online.
APPENDIX A. GUIDED – A guideline for intervention development studies 35

| Item description | Where item is located in manuscript |
| 1. Report the context for which the intervention was developed. | Figure 2: Logic Model which includes contextual factors influencing the intervention (moderators) |
| 2. Report the purpose of the intervention development process. | Table 1, Column 6 and Table 2, Column 5: Intervention change processes |
| 3. Report the target population for the intervention development process. | Table 1, Column |
| 4. Report how any published intervention development approach contributed to the development process | Additional design steps from synthesis of design literature 30 |
| 5. Report how evidence from different sources informed the intervention development process | Table 1: Recommended strategy > Empirical evidence Intervention design feature > Change process |
| 6. Report how/if published theory informed the intervention development process. | RESULTS SECTION: Table 1, Column 2: Theories underlying DLD profile. Table 2, Column 2: COM-B model of clinician’s behaviour-change drivers 42 |
| 7. Report any use of components from an existing intervention in the current intervention development process. | Table 1: Recommended strategy > Empirical evidence > Intervention design feature > Change process |
| 8. Report any guiding principles, people or factors that were prioritised when making decisions during the intervention development process. | Table 1, Column 3 and Table 2, Column 3: Recommended strategies Clinician feedback and refinement. |
| 9. Report how stakeholders contributed to the intervention development process. | |
| 10. Report how the intervention changed in content and format from the start of the intervention development process. | |
| 11. Report any changes to interventions required or likely to be required for subgroups. | Figure 2: Logic Model which includes contextual factors influencing the intervention (moderators) |
| 12. Report important uncertainties at the end of the intervention development process. |
|
| 13. Follow TIDieR guidance when describing the developed intervention. |
|
| 14. Report the intervention development process in an open access format. |
|
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.