
Abstract
Objective
Temporal processing deficits were found among children with attention-deficit/hyperactivity disorder (ADHD). The present study aims to develop an online temporal processing assessment that can be conducted remotely, and the sensitivity of the test was assessed on a group of children with ADHD.
Methods
A total of 188 children were recruited, including 94 typically developing (TD) children, and 94 children with ADHD. The online assessment consists of two temporal-order judgment (TOJ) tasks. One task used tone pairs presented with two interstimulus intervals (ISIs) (305ms and 40ms). Another task used pairs of consonant-vowel (CV) syllables with 20 varying ISI levels. Participants were asked to determine the sequence of the sound pairs.
Results
The results showed that ADHD children were less accurate (ISI 305ms: M = 83.90%; ISI 40ms: M = 66.28%) than TD children (ISI 305ms: M = 89.36%; ISI 40ms: M = 77.16%) in the tone task. Similarly, ADHD children showed a higher ISI passing threshold (M = 283.64ms) than TD children (M = 199.76ms) and higher accuracy in the CV task. Hierarchical binary logistic regression suggested a model to predict ADHD children using accuracy in ISI 40ms in the tone task and ISI passing threshold in the CV task. Receiver operating characteristic (ROC) analysis yielded a sensitivity of 75.58% and a specificity of 51.11%.
Conclusion
ADHD children showed temporal processing deficits of both tones and CVs. The online assessment may be a valid tool for differentiating ADHD children from TD children.
Introduction
Temporal processing is a fundamental perceptual processing skill. It allows us to perceive, discriminate, and organize rapid, successive events. According to Farmer and Klein, 1 temporal processing involves a hierarchy of information processing, starting from the most simple level (i.e. detection and identification of the target visual or auditory stimuli), to a higher level (i.e. the individuation and dissection of rapid and successive stimuli), and lastly, to the most complex level (i.e. perception and production of the temporal order of two or more rapid and serial stimuli). The hierarchy of temporal processing corresponds to a series of laboratory tasks such as simultaneity judgment, gap detection, and temporal-order judgment (TOJ).
Among various paradigms that measure temporal processing, the TOJ task is a well-known paradigm to assess the processing of perceptual latencies among information in different modalities. 2 In a TOJ task, two stimuli are presented using various interstimulus intervals (ISIs), and participants are required to repeat the sequence of stimulus presentations. For example, as early as in the 1970s, Tallal and Piercy 3 utilized the TOJ paradigm to compare children with developmental aphasia and children with typical development (TD). Aphasic children showed impairment in discriminating and sequencing brief tones, suggesting a potential temporal processing deficit. Later studies extended the search of temporal processing deficits to children with other neurodevelopmental disorders, such as attention-deficit/hyperactivity disorder (ADHD),4–6 dyslexia (see a review by Meilleur et al. 7 ), and autism spectrum disorder (ASD) (see a review by Meilleur et al. 7 ). From neurodevelopmental perspectives, the brains of children with temporal processing deficits have not developed the skill of separating and distinguishing brief and successive sound features. 8 They process speech information using a long-time-chunk representational mode rather than a normal, intra-syllabic feature-distinguishing mode.
Temporal processing in ADHD has drawn more attention in the recent decades. Regarding the studies using auditory TOJ paradigms, two studies reported higher TOJ threshold for tones (ADHD: 420ms; healthy control: 92ms in Cardy et al. 4 ; ADHD: 153ms; non-ADHD: 68ms in Fostick 5 ) in ADHD children. Another study examined the accuracy in the TOJ tasks of both tones and consonant-vowels (CVs) to compare children with ADHD, children with a reading disability, children with comorbid ADHD and reading disability, and TD children. Results showed that in both the tone and the CV task, children with ADHD tend to perform less accurately than TD children but did not reach a statistical significance. 9 Besides, in both groups, performance was generally impaired with decreasing ISI, suggesting that ISI can be an important factor affecting the performance in TOJ tasks. Other tasks also suggested a potential auditory temporal processing deficit in ADHD children. One study showed that children with ADHD tend to be less consistent in identifying and labeling tones or CVs from a continuum of auditory stimuli. 10 A later study showed that ADHD children displayed a general impairment across various auditory temporal processing tasks, including gap detection threshold, the threshold for detecting a 32 ms and 512 ms tone in quiet, and the threshold for the simultaneity judgment of tones. 11
Given the limited literature on the TOJ performance in ADHD, one aim of the present study is to fill in the research gap by examining the temporal processing ability in children with ADHD using auditory TOJ paradigm. Regarding the design of experimental tasks, two TOJ tasks using nonverbal (i.e. tones) and verbal (i.e. CVs) stimuli were adopted. In addition, the ISI level in two TOJ tasks were carefully selected by referring to previous studies. For the tone task, Tallal and Piercy 3 reported that TD children scored 100% correct while aphasic children scored 76% correct in the TOJ of tone pairs with ISI at 305ms. With ISI shorter than 305ms, the performance of both TD children and aphasic children decreased with the decreasing ISI, but the aphasics’ performance was more markedly impaired. Besides, some experimental studies have evidenced that the minimum ISI between two successive stimuli for correctly reporting their temporal order is about 20–40ms.12–14 Such order threshold seems to be invariant for stimuli across sense modalities in a normal population.12,14 Kanabus et al. 15 have also revealed that the order threshold at which normal individuals could obtain 75% of correct responses in a TOJ task was at 40ms, independently of the visual and auditory modality. Therefore, the present study has adopted these findings to design two different levels of ISI (i.e. 305ms and 40ms) for the TOJ of tones. For the CV task, we followed the ISI levels (500, 400, 300, 250, 200, 170, 140, 110, 90, 70, 50, 40, 30, 25, 20, 15, 10, 7, 3, and 0 ms) used by Strehlow and colleagues. 16 Two hypotheses were proposed: first of all, we hypothesized that children with ADHD were impaired in the TOJ tasks of both tones and CVs; second, their impairments were more significant at shorter ISI.
Another important aim of the present study is to develop and validate an online temporal processing assessment based on a group of children with TD and ADHD. While all the reported temporal processing studies used face-to-face tests, this is the first study examining the sensitivity of an online assessment of temporal processing. In the present study, participants can receive the assessment at home under the instructions of experimenters through telecommunication. This is especially important during the pandemic of COVID-19, as our online assessment can minimize face-to-face interactions and reach people in less accessible regions in the future. It has been a tendency to develop online tests for cognitive functions,17–19 detecting various cognitive disorders such as mild cognitive impairments, 20 dyslexia,21,22 and central auditory processing disorders. 23 Online tests can be more cost-effective in test administration and data extraction and allow for data collection from a large sample. Yet, it is more difficult for online tests to control environmental factors (e.g. ambient distractions and technical problems) and maintain participants’ attention than offline lab tests, especially when there is no supervision on test administration. Besides, online tests may have higher demand on participants’ computer literacy. The present study tried to minimize the potential weaknesses in online tests, as both experimenters and parents/teachers were involved in guiding and monitoring the children to perform the assessment, and the whole assessment only lasted for 15–30 min. We further hypothesized that our online assessment could be a sensitive tool for discriminating ADHD children from TD children.
Method
Participants
Participants were recruited through posting advertisements at parent groups of various social media (e.g. Facebook and WhatsApp), and mass mail in Hong Kong. Children were recruited if the following inclusion criteria were met: (1) aged between 5 and 17 years, (2) with normal hearing, (3) able to understand Cantonese, and (4) accessible to computers or tablets to perform the online assessment. Participants will be excluded if they meet any one of the following criteria: (1) unable to complete the assessment due to technical problems, (2) failed to understand the instruction and pass the practice sessions, or unwilling to cooperate, and (3) the performance in the assessment was severely biased due to technical problems as documented by experimenters. Among the recruited sample, 94 children have been diagnosed with ADHD based on the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) by a psychiatrist, a pediatrician, or a clinical psychologist at the Child Assessment Centre (a public health service in Hong Kong) or at private clinics. Besides, 94 age- and gender-matched children were identified as typically developing (TD) children, without any reported diagnosis of developmental disorders (e.g. ADHD, ASD, learning disability, and abnormal intelligence), psychiatric disorders (e.g. anxiety and depression), and subjective complaints from parents on children's difficulty in attention or self-control. In the TD group, the proportion of children (5–11 years) and adolescents (11–17 years) were 75.53% and 24.47%, respectively. In the ADHD group, the proportion of children and adolescents were 79.79% and 20.21%, respectively. The TD group contained 28 females and 66 males, and the ADHD group contained 26 females and 68 males. Given that male children were more prone to ADHD than female children, the recruited sample included more males than females. Besides, the ADHD group contained 55 (58.51%) ADHD children without any comorbidities, 29 (30.85%) ADHD children who were comorbid with special learning difficulties (SpLD) (including 22 (23.40%) ADHD children with dyslexia), and 10 (10.64%) ADHD children with other comorbidities including special language impairment (SLI), emotional disorders, gross and fine motor difficulties, oppositional defiant disorder (ODD), limited intelligence, and social and communication disorder.
Procedure
Online consent forms from the parents of our participants were obtained before the study. Participants received the assessment in their own homes using computers or tablets with internet access. Each participant was guided by a trained experimenter to perform the task step-by-step with an online platform (i.e. Zoom) and was encouraged to complete the assessment. Participants were asked to share the screen and share sound in Zoom so that experimenters could vividly explain the instructions, monitor the assessment progress, and help participants with any technical problems. In addition, young children were also accompanied by a parent or a caretaker for technical assistance. Participants were also asked to re-tell the instructions from the experimenters to ensure that the requirements of the experiments were clearly understood. The whole assessment lasted for 15–30 min, taking place from 9:00 am to 6:00 pm on Monday to Saturday. As an incentive, parents received oral reports on their children's performance in the assessment. This study was conducted in accordance with the World Medical Association Declaration of Helsinki. The research protocol was approved by the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (Reference number: 2021.029-T).
Materials
Paradigm
The present paradigm was designed based on the TOJ task. Participants need to go through two practice sessions before the formal test to get familiar with the stimuli and paradigm. In the first practice session, participants were asked to identify individual sounds. In the second practice session and the formal test, they were asked to repeat the sequence of sound pairs. As shown in Figure 1, each type of sound (i.e. high-pitch tone and low-pitch tone in the tone task, and /ba/, /da/, /ga/, /ka/, /pa/, and /ta/ in the CV task) was represented by a unique icon on the screen. Once a sound or a pair of sounds were played, participants made responses by clicking on the corresponding icon using a mouse or a finger, depending on the device (i.e. computers or touch-screen tablets) used for the assessment. Feedbacks were provided in the first practice session and the first four trials in the second practice session; however, no feedback was provided in the formal test The participants went through these procedures twice, with one TOJ task on tones, and another TOJ task on CVs.

Example of the computer screen of a participant during the online temporal processing assessment. (a) The tone task and (b) the consonant-vowel (CV) task.
Stimuli
Tone: The sound stimuli involved two types of square tone at high (3000 Hz) and low (300 Hz) frequency. Each tonal sound had a duration of 15ms. The first practice session contained a minimum of 20 trials and could be passed by making eight correct responses in 24 consecutive trials. The second practice session contained a total of 8 trials and could be passed if making at least one correct response in the latter four trials. The formal test session contained 60 trials of tonal pairs. In the first 30 trials, tonal pairs were separated by an ISI of 305ms. The latter 30 trials were separated by an ISI of 40ms. Accuracy rates in two ISI conditions were assessed separately.
CV syllables: Six CV syllables including /ba/, /da/, /ga/, /pa/, /ta/, and /ka/ were adopted from the standard Bergen dichotic listening paradigm. 21 Each CV sound had a duration ranging from 500ms to 590ms. The first practice session shared the same number of trials and passing criteria as the first practice session of the tone task. The second practice session contained ten trials and could be passed if making at least two correct responses in the latter six trials. In the formal test session, the total number of trials ranged between 60 and 80. Thirty-three different combination of CV pairs was generated by six CVs and was presented randomly. The ISI within CV pairs were presented following the 3-down, 1-up staircase protocol used in Strehlow and colleagues. 16 The 20 levels of ISI were reduced in nonlinear steps (i.e. 500, 400, 300, 250, 200, 170, 140, 110, 90, 70, 50, 40, 30, 25, 20, 15, 10, 7, 3, and 0 ms) if correct responses were made on three consecutive trials within each ISI condition, and increased if one incorrect response was made. Accuracy rates at each ISI level were calculated, and the shortest ISI at which participants obtained three consecutive correct responses was regarded as the ISI passing threshold.
Results
Demographics
Table 1 showed that there was no significant difference between groups in term of age (t(186) = 0.009, p = 0.99) and gender (
Demographic characteristics of children with typical development (TD) and attention-deficit/hyperactivity disorder (ADHD).

Performance in the TOJ of tones
To evaluate the performance in the tone task, mixed ANOVA was performed to examine the ISI condition (305ms and 40ms) × group (TD and ADHD) interaction. Significant interaction (F(1, 186) = 5.12, p = 0.03,

Accuracy (%) of the tone task in interstimulus interval (ISI) 305ms and 40ms conditions in children with typical development (TD) and attention-deficit/hyperactivity disorder (ADHD).
Performance in the TOJ of CV syllables
The data were analyzed in two ways: First, the passing threshold of children with ADHD with TD children was compared. Second, the accuracy rate of various levels of ISI was examined. First, an independent t-test was carried out to compare the difference in ISI passing threshold between TD children and ADHD children, excluding four TD children and eight ADHD children who did not pass at the longest ISI (i.e. 500ms). Results showed that the ISI passing threshold of ADHD children (M = 283.64ms, SD = 176.84ms) was significantly longer than that of TD children (M = 199.76ms, SD = 195.13ms) (t(174) = −2.98, p = 0.003, d = 0.45). This result suggested that ADHD children have a higher passing threshold than TD children, that is, they required longer interval time between stimuli to discriminate them.
Next, mixed ANOVA was also performed to examine the percentage of accuracy across 20 levels of ISI. Mauchly's test of sphericity suggested that the assumption of sphericity was violated (p < 0.001), therefore Greenhouse–Geisser's estimate of epsilon (

Accuracy (%) of the consonant-vowel (CV) syllable task in 20 interstimulus interval (ISI) conditions in children with typical development (TD) and attention-deficit/hyperactivity disorder (ADHD).
Accuracy (%) in 20 interstimulus interval (ISI) conditions of the consonant-vowel (CV) task in children with typical development (TD) and attention-deficit/hyperactivity disorder (ADHD).

Note: Degree of freedom (df) was adjusted when equal variance was not assumed.
Figure 4 showed the accumulative percentage of children in the TD group or the ADHD group who passed the CV task at each ISI level. The largest difference between the TD and the ADHD group occurred in ISI 25ms, at which 33 (36.57%) TD children but only 8 (9.30%) ADHD children passed the CV task. Even for ISI threshold as high as 250ms, which was identified as a sufficient time for processing speech units in normal young adults, 24 the advantage of TD children over ADHD children still persists. While 56 (62.22%) TD children passed the CV task with an ISI threshold equal to or shorter than 250ms, only 41 (47.67%) ADHD children obtained the same level of ISI passing threshold. The discrepancy between the accumulative percentage of TD children and ADHD children who passed the CV task reduced evidently at ISI 400ms. Therefore, ADHD children needs longer interval time than TD children to pass the CV task.

Accumulative percentage of children with typical development (TD) and attention-deficit/hyperactivity disorder (ADHD) who passed at each interstimulus interval (ISI) level in the consonant-vowel (CV) task.
Prediction for group membership using task performances
To evaluate the ability of the tone task and the CV task in predicting the TD and ADHD children, hierarchical binary logistic regression was performed (Table 3). Several models using different sets of predictors were compared to determine which model can better predict the group membership.
Comparison of models using different sets of predictors.
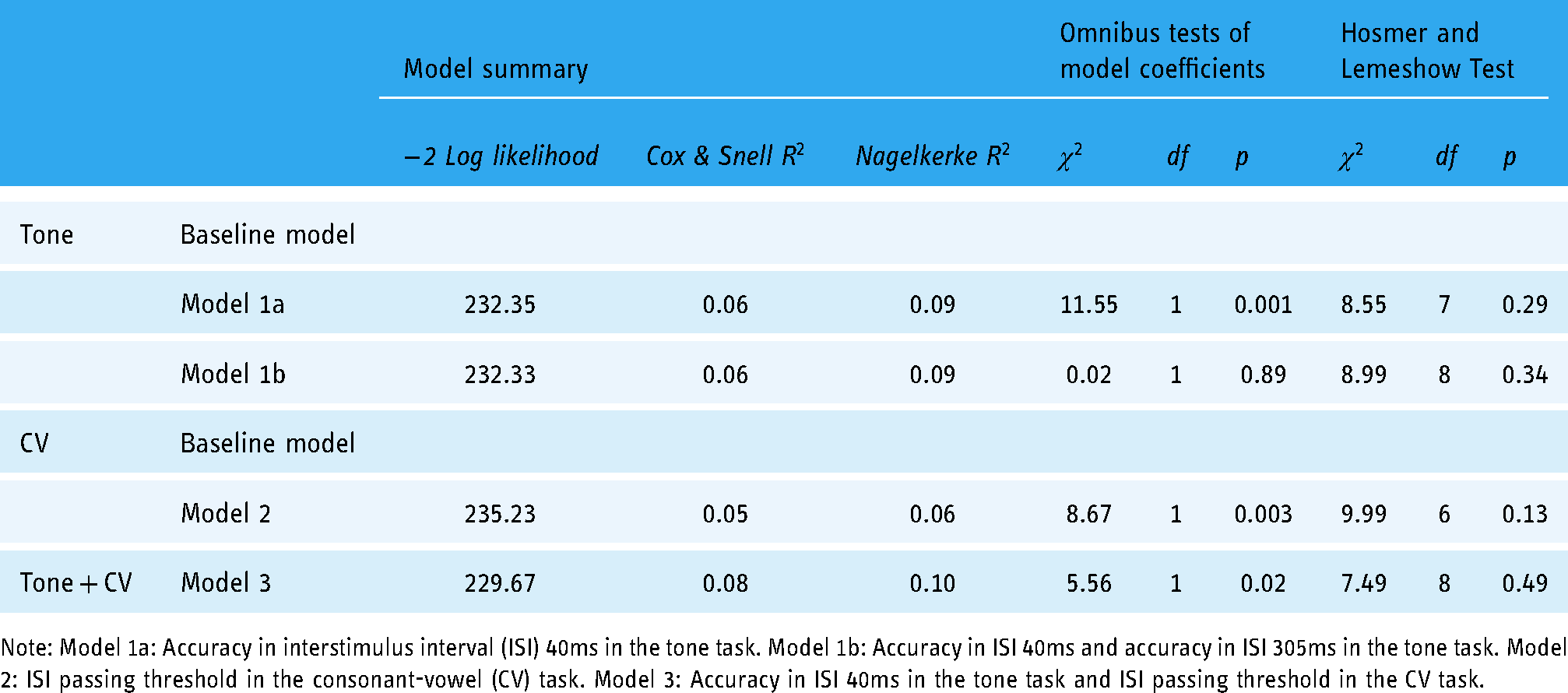
Note: Model 1a: Accuracy in interstimulus interval (ISI) 40ms in the tone task. Model 1b: Accuracy in ISI 40ms and accuracy in ISI 305ms in the tone task. Model 2: ISI passing threshold in the consonant-vowel (CV) task. Model 3: Accuracy in ISI 40ms in the tone task and ISI passing threshold in the CV task.
First of all, the prediction ability of the tone task was evaluated. Accuracy in two ISI conditions of the tone task were entered into the model step by step. Results showed that the accuracy in ISI 40ms was a significant predictor (
Second, Model 2 used the ISI passing threshold in the CV task to predict the group membership and suggested ISI passing threshold as a significant predictor (
To further investigate the performance of both tone and CV tasks in predicting the group membership, Model 3 included the accuracy in ISI 40ms of the tone task and the ISI passing threshold of the CV task. Results showed that Model 3 explained 8% of the variance in the group membership (Cox & Snell 

Receiver operating characteristic (ROC) curve of the composite score using accuracy in interstimulus interval (ISI) 40ms of the tone task and the ISI passing threshold of the consonant-vowel (CV) task for detecting children with attention-deficit/hyperactivity disorder (ADHD).
Discussion
The present study aims at examining the temporal processing in ADHD children based on two TOJ tasks. Our results confirmed the first hypothesis, suggesting that the ADHD children were impaired in the auditory temporal processing of tones and CVs. In the tone task, ADHD children were less accurate than TD children at both short (40ms) and long (305ms) ISI. This result extended the findings of the study by Tallal and Piercy 3 to children with ADHD, in which aphasic children were impaired in the TOJ of tones at ISI 305ms and shorter ISI levels. In the CV task, the accuracy rate of ADHD children was generally lower at different ISI levels ranging from 0ms to 500ms. This result complemented to the scarce literature testing the TOJ of CVs on ADHD children, as only one study by Breier et al. 9 showed that ADHD children tend to perform less accurately than TD children in the TOJ task of /ba/-/da/ sound pairs at ISI 10 and 70ms but did not reach a statistical significance. Also, the mean and the distribution of ISI passing threshold in the CV task suggested that ADHD children required longer interval time than TD children to successfully sequence the CV pairs. The accuracy rate at each ISI level and the ISI passing threshold together showed that the ability to process CVs within a brief and restricted time was generally impaired in ADHD children. Moreover, our work contributed to the investigation of temporal processing in a broader range of speech sounds by including six different CVs, compared to previous studies in which usually only two to three different CVs were used.9,10,25–27
Besides, in both tone and CV tasks, a significant main effect of ISI was found, as the accuracy decreased in both TD and ADHD groups when ISI decreased, which was also consistent with previous studies in which both TD group and aphasia/ADHD group showed lower accuracy in short ISI than in long ISI.3,9 Therefore, our second hypothesis was confirmed. Moreover, children with ADHD showed more salient impairment at shorter ISI in both the tone task and the CV task. In the tone task, the relative between-group difference in accuracy was significantly larger at ISI 40ms (14%) than at ISI 305ms (6%); in the CV task, the discrepancy between the proportion of TD children and the proportion of ADHD children who passed the CV task were larger at shorter ISI levels and reduced evidently at ISI 400ms or longer. Therefore, the ISI level is a significant factor affecting the performance in TOJ tasks and the discriminative power of the assessment. Besides, when future studies try to develop interventions for temporal processing deficits, they may consider starting with temporal processing tasks using long ISI levels, so that participants can benefit from long ISI and hear the successive sounds clearly at first. Then, the ISI level can be reduced step by step, allowing participants to gradually adapt to successive sounds with short ISI.
The last hypothesis was also confirmed by the results from regression analysis and ROC analysis, suggesting that our online TOJ tasks of tones and CVs could be sensitive in detecting ADHD children. For the tone task, accuracy in ISI 40ms condition (but not in ISI 305ms) significantly predicted the group membership. For the CV task, the model using ISI passing threshold alone also significantly predicted the group membership. Nevertheless, the best prediction was made when both the accuracy in ISI 40ms of tone task and the ISI passing threshold of the CV task were included in the model. By using a cut-off at −0.302 for the composite score, the model can provide a sensitivity of 75.58% and a specificity of 51.11%. While the majority of studies investigated the temporal processing in ADHD children using only tones,4,5,11 relatively few studies used both tones and CVs.9,10 The present study utilized both tasks, and the results suggested using both the tones and the CVs yield a more sensitive test in differentiating ADHD children from TD children. Future studies may explore whether the TOJ of nonverbal stimuli (e.g. tones) and the TOJ of verbal stimuli (e.g. CVs) involve some different processing mechanisms, so that they have their unique contributions to the detection of ADHD children, and make the detection more sensitive when the performance in both nonverbal and verbal task were used.
To our knowledge, the present study is a pioneer attempt for assessing temporal processing online remotely. The results suggest that this means of assessing seems to be sensitive in discriminating ADHD children with temporal processing deficits from TD children. Our assessment may serve as a screening test for the potential temporal processing deficits in children. Given that the test can be done online remotely, more children can be tested effectively and efficiently, and this approach may allow the detection of children with ADHD in the early stage of development. Besides, our assessment can benefit a broad range of people regardless of the geographical limitations and minimize face-to-face interactions during the pandemic of COVID-19. Therefore, the present online assessment of temporal processing could be a time-saving, cost-effective, and easily accessible tool for the early detection of potential temporal processing deficits for children or even adults.
Our present study has some limitations. Since only children with ADHD were tested in the present study, future studies may further evaluate the discriminative power of this test in other neurodevelopmental disorders (e.g. dyslexia and ASD) and brain disorders (e.g. dementia and traumatic brain injury). Second, the large range of age range (5–17 years) of our selected may not be able to demonstrate TOJ ability across different age cohorts. Future studies may consider investigating a specific age group of children (e.g. primary school students aged 6–12 years) with larger sample size. Third, since we did not collect information on the subtypes of ADHD from parents or teachers, temporal processing performance was analyzed based on the whole ADHD group. Future studies may examine the temporal processing in different ADHD subtypes. Besides, ADHD children with different comorbidities were grouped together. The potential effect of comorbidities may be considered and controlled in future studies. Lastly, in both the tone task and the CV task, ISI levels were presented in a reducing order (i.e. from long ISI to short ISI). It is worth exploring if there is a potential order effect of ISI type, by counterbalancing the sequence of ISI conditions.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076221120325 - Supplemental material for Temporal processing deficit in children with attention-deficit/hyperactivity disorder: An online assessment
Supplemental material, sj-docx-1-dhj-10.1177_20552076221120325 for Temporal processing deficit in children with attention-deficit/hyperactivity disorder: An online assessment by Agnes S Chan, Zihan Ding, Tsz-lok Lee and Sophia L Sze, Natalie S Yang in Digital Health
Footnotes
Acknowledgments
The authors would like to thank Quin Chan, Christy Cheung, Kenneth Lai, Evan Lau, and Katie Leung for collecting data for this study. Further appreciation is extended to all participants and parents/guardians for their assistance in the experiments.
Contributorship
ASC and SLS contributed to the conception, and design of the study. ZD, TL, SLS, and NSY contributed to the acquisition of the data. ASC, ZD, TL, and NSY contributed to the analysis, and interpretation of the data. All authors contributed to the drafting and revising of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first author (ASC) received a grant from Lee Hysan Foundation. ASC is also the founder and director of Pro-Talent Association Ltd. All other authors have no conflicts of interest to disclose.
Ethical approval
The present study was conducted in accordance with the World Medical Association Declaration of Helsinki. The research protocol was approved by the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (Reference number: 2021.029-T). Online consent forms were obtained from the parents of all the participants.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Lee Hysan Foundation (grant number N/A).
Guarantor
The first author (ASC) takes full responsibility for the article, including for the accuracy and appropriateness of the reference list.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.