
Abstract
Objectives
Gay, bisexual and other men who have sex with men (GBM) are disproportionately affected by sexually transmitted and blood-borne infections (STBBI) due to stigma and other factors such as structural barriers, which delay STBBI testing in this population. Understanding acceptability of online testing is useful in expanding access in this population, thus we examined barriers to clinic-based testing, acceptability of a potential online testing model, and factors associated with acceptability among GBM living in Ontario.
Methods
Sex Now 2019 was a community-based, online, bilingual survey of GBM aged ≥15. Prevalence ratios (PR) and 95% confidence intervals (95%CI) were calculated using modified Poisson regression with robust variances. Multivariable modelling was conducted using the Hosmer-Lemeshow-Sturdivant approach.
Results
Among 1369 participants, many delayed STBBI testing due to being too busy (31%) or inconvenient clinic hours (29%). Acceptability for online testing was high (80%), with saving time (67%) as the most common benefit, and privacy concerns the most common drawback (38%). Statistically significant predictors of acceptability for online testing were younger age (PR = 0.993; 95%CI: 0.991–0.996); a greater number of different sexual behaviours associated with STBBI transmission (PR = 1.031; 95%CI: 1.018–1.044); identifying as an Indigenous immigrant (PR = 1.427; 95%CI: 1.276–1.596) or immigrant of colour (PR = 1.158; 95%CI: 1.086–1.235) compared with white non-immigrants; and currently using HIV pre-exposure prophylaxis (PrEP) compared to not currently using PrEP (PR = 0.894; 95%CI: 0.828–0.965).
Conclusions
Acceptability of online testing was high among GBM in Ontario. Implementing online STBBI testing may expand access for certain subpopulations of GBM facing barriers to current in-person testing.
Keywords
Introduction
Gay, bisexual and other men who have sex with men (GBM) are disproportionately affected by sexually transmitted and other blood borne infections (STBBI) in comparison to the general population due to experiences of stigma and structural barriers. 1 In Ontario, Canada, GBM comprised the greatest proportion of new HIV diagnoses (64%) in 2019, and 85% of syphilis cases, 40% of gonorrhoea cases and 80% of lymphogranuloma venereum (a subtype of chlamydia) cases in men in 2016.2,3 One way to address this burden is through increased testing, 4 which reduces morbidity by identifying and treating positive cases, thereby reducing population transmission. 5 Stigmatizing certain behaviours, such as condomless anal intercourse and substance use during sexual activities, may discourage GBM from accessing STBBI testing services.6,7 Similarly, structural barriers such as long wait times and few nearby testing clinics are other reasons for delayed STBBI testing in this population.4,6–8
Online STBBI testing might address some of these barriers experienced by GBM and three main types exist worldwide. 9 In the first, users either download or print out a requisition form, which they take to a laboratory for on-site testing. 9 In the second, users receive a self-collection kit in the mail and collect their specimens at home, before mailing it out to a laboratory for testing. 9 In the third, users receive a self-testing kit in the mail and receive rapid results in their home. 9 Linkage to care in the case of a positive test result varies across jurisdictions that have implemented these three online STBBI testing models. However, in the first two scenarios, a health care provider typically follows up with the individual in the case of a positive test result, while users in the third scenario are often recommended to go in person for confirmatory testing. 9
Online STBBI testing services already exist in many high income countries and previous research has found online testing models to be acceptable, accessible, feasible and convenient across different populations and settings. 9 Diagnosis rates have also been comparable to in-person testing, and in cases where they were not, this was due to users being encouraged to test in-person when experiencing symptoms commonly associated with STBBI. 9
In British Columbia (BC), Canada, the first type of online STBBI testing service model, GetCheckedOnline (GCO), has existed since 2014, where users provide biospecimens for testing at specific laboratory locations. 10 There are no out-of-pocket costs for clients of GCO and in the case of a positive test result, clients will be contacted by a nurse for follow-up treatment. 4 As GCO expands service availability across jurisdictions, we were interested in assessing the adoption of this testing model in Ontario, where the economic and political landscape differs due to current centre-right political leadership and a previous history of comprehensive online STBBI testing being only provided by private companies.11,12 We previously identified that the perceived benefits of GCO among GBM include increased anonymity/privacy, convenience and flexibility in testing appointment times.4,8,10 Service providers in Ontario argue that expedited STBBI testing and notifications about when to return for testing would increase testing in this population. 13 When we began this study, no online STBBI testing services existed in the province. Presently, the online STBBI testing services that do exist in Ontario require payment to use the service, only test for HIV, require the user to contact a health care professional themselves if they test positive, and/or limit the number of tests an individual can order online. 9 This highlights the need for a lower-barrier online testing service in the province such as GCO.
We examined Ontario GBM's reasons for delaying in-person STBBI testing, acceptability of online STBBI testing, perceived benefits and drawbacks of using such a service, and factors associated with acceptability of this service. We hypothesized that acceptability would be high and that stigmatized identities and behaviours, and experiences of structural barriers, would be associated with increased acceptability of online STBBI testing.
Methods
Recruitment
Sex Now 2019 was a community-based, online, cross-sectional survey conducted in English and French from November 2019 until February 2020. Eligibility included: being ≥15 years old; identifying as a man (cis or trans), non-binary, and/or Two-Spirit; living in Canada; and having had sex with a man in the past five years and/or self-identifying as any sexual orientation other than exclusively heterosexual. Two-Spirit has been defined as a ‘community organizing tool for the Indigenous peoples of Turtle Island [the Americas] who embody diverse sexualities, gender identities, roles and/or expressions’. 14 The ethics protocol for this study was reviewed and approved by the research ethics boards at the University of Victoria (BC17-487), University of British Columbia (BC17-487) and the University of Toronto (37576). We recruited participants using social media platforms (e.g. Facebook), social/sexual networking websites and mobile applications used by GBM (e.g. Scruff), community organization newsletters and word of mouth. The consent form was provided at the start of the Sex Now 2019 survey. All individuals included in this study were those who consented to participating by selecting ‘Yes’ to this question at the end of the online consent form: ‘Do you acknowledge and agree to these conditions?’
We applied the socioecological model, which posits that understanding and developing appropriate interventions for health behaviours must consider individual, interpersonal, institutional, community and policy factors. 15 We examined factors representing the first four levels that may influence the acceptability of online STBBI testing among GBM in this study.
Measures
Barriers to clinic-based testing were ascertained using the following question: ‘Have any of the following caused you to delay or skip STI [sexually transmitted infection] testing in the PAST YEAR? (check all that apply)’ with a series of 12 different response options as well as an open-text write-in for other reasons. Acceptability of online STBBI testing was posed to all survey participants living in Ontario in the following manner: ‘Suppose you could get tested by printing a lab form from a website or downloading an electric version to your phone, that you then take to a lab in person, and get your results online or by phone. How likely would it be that you would use this service?’. Participants were asked to select their response from a five-point Likert scale (very likely – never). Benefits and drawbacks of this potential service were assessed separately in two questions: ‘For you, what is the greatest BENEFIT/DRAWBACK of this possible testing service? (check all that apply)’ with a series of 14 (benefits) and 8 (drawbacks) response options as well as an open-text write-in for other reasons.
Predictor variables potentially influencing the acceptability of online STBBI testing were selected based on previous findings in the literature and informed by the socioecological model. 15 In preparation for analysis, predictor variables were categorized in four different ways. First, some variables were left as they were (e.g. Age, ‘How old are you in years?’). Second, some variables' response options were collapsed. For instance, in the ethnoracial identity variable, those who selected white only were categorized as ‘white’; those who selected Indigenous alone or in combination with other identities were categorized as ‘Indigenous’; those who selected ‘African’, ‘Caribbean’, or ‘Black’ alone or in combination with other identities except Indigenous were categorized as ‘African, Caribbean, Black (ACB)’; and all other racial/ethnic identity selections and combinations were categorized as ‘Other racial/ethnic groups’. Third, some variables were combined with other variables to create one variable (e.g. ‘Gender identity’ and ‘Trans identity’ were combined into the variable ‘Gender’). Fourth, some variables were combined to create count variables. For example, the count variable ‘Number of sexual behaviours in the past 6 months associated with increased risk for STBBIs’ was created using the following three variables: substance use in the past 6 months, number of sexual partners in the past 6 months, and types of sexual activities in the past 6 months. Substance use during sex in the past 6 months was combined into: ‘Yes’, ‘No’ and ‘No substance use at all in the past 6 months’. Then, number of sex partners in the past 6 months was dichotomized with the categories being: ‘<3’ and ‘3 + ’. Finally, each variable was combined so that each time a person answered ‘Yes’ (or ‘3 + ’ partners in the past 6 months) their score would increase with the range of possible scores being 0–8. See the Supplemental material file for full list of questions, response options and categorization schemes used for this analysis.
Analysis
We restricted the analysis to participants living in Ontario (N = 3581) and excluded those who were missing data on all variables of interest from the analysis (n = 2214, 62%) for a final analytical sample of 1369 GBM. We compared the sociodemographic information between the missing participants to those included in this study and found no statistical difference at p < 0.05 in mean age, proportion of Indigenous and Two-Spirit participants, and proportion of individuals who have not completed high school. However, we did find that our sample had more participants who: were born in Canada (79% vs 73%), were disabled (17% vs 14%), were single (47% vs 38%), lived in large urban centres (77% vs 44%), only had completed high school (15% vs 11%) and were living with HIV (11% vs 4%).
After we performed initial descriptive analyses of the final dataset, we recoded the ‘acceptability of online STBBI testing’ variable as dichotomous with the response options ‘very likely’/‘likely’ as 'likely' versus the response options ‘unlikely’/‘very unlikely’/‘never’ as ‘unlikely’. We dichotomized the variable based on the distribution of responses and to facilitate comparisons with our previous work.8,16 The outcome event we were interested in is the number and proportion of participants who reported being likely to use an online STBBI testing service.
Perceived benefits of online STBBI testing, perceived drawbacks of online STBBI testing and in-person STBBI testing barriers were only examined descriptively and in univariate analyses, to avoid overfitting the multivariable models.
We performed unadjusted analyses examining the acceptability of online STBBI testing using modified Poisson regression with robust variances to generate prevalence ratios (PRs) and 95% confidence intervals (95% CIs). We chose modified Poisson regression over logistic regression as the outcome was common. 17 The multivariable regression model was developed using the Hosmer-Lemeshow-Sturdivant model building approach, which includes seven steps. 18 Step 1: univariate analyses are conducted to identify candidates for the multivariable model; those with a p-value < 0.25 are excluded unless they are of clinical or theoretical importance. Step 2: a model is fit containing all candidates in step 1 and are assessed for statistical significance at p < 0.05. Step 3: All variables that were not statistically significant at p < 0.05 are removed and betas of remaining variables are examined to determine if they have changed by > 20%. Step 4: If a change of more than 20% has occurred, previously eliminated variables are added back one at a time (including those excluded in step 1) based on decreasing effect size, and the model is reassessed after each variable has been included. Step 5: Double check appropriate functional forms. Step 6: assess interactions identified a priori, which in this study included the following intersecting marginalized identities shown to experience health inequities: sexual identity*ethnoracial identity, sexual identity*gender identity, sexual identity*immigration history, ethnoracial identity*immigration history, ethnoracial identity*gender identity and gender identity*immigration history. 19 We assessed for interaction by first including an interaction term in the model and observed if the term was statistically significant at p < 0.05. If it was, we then combined the two interacting variables into one variable, and entered this new variable into the model and assessed for statistical significance again. The final model presents findings using the new combined interacting variable. Step 7: the model is verified using goodness-of-fit statistics and other diagnostics. All analyses were conducted using R Studio.
Results
Descriptive findings
Among 1369 participants, the mean age was 40 and the majority identified as cisgender men (91%), white (77%) and gay (72%, Table 1). Indigenous participants comprised 4% of the sample, with 1% of the sample identifying as Two-Spirit. Half of the participants were single (47%). The majority of participants were born in Canada (79%), lived in large urban centres (100,000 + people, 77%), and had completed post-secondary education (81%). GBM living with HIV comprised 11% of the sample.
Descriptive findings of acceptability of online STBBI testing by variables of interest included in the multivariable model building process (n = 1369).

Number of sexual behaviours engaged in over the past 6 months that are associated with increased STBBI transmission.
Comprised of questions asking when participants were last tested for STBBIs, usual place of testing, and comfort with health clinics.
Number of forms of discrimination experienced in the past year based on ethnoracial identity, trans identity, sexual orientation, etc.
Not mutually exclusive with working full time.
Acceptability of online STBBI testing was high overall (80% were likely to use), and across all subgroups. Many GBM reported no delays in testing for STBBIs in-person (41%; Table 2); however, the three most common reasons for delaying testing included: being too busy (31%), inconvenient clinic hours (29%) and being too stressed/anxious/depressed to get tested (17%). The most commonly reported benefits of online STBBI testing were: it saves time (67%), more convenient than going to a clinic/doctor's office (65%) and the ability to get results online or by phone (58%). One quarter (28%) of participants indicated no drawbacks to using online STBBI testing; however, one-third (38%) worried about the privacy of personal information and one-third (31%) preferred to see a healthcare provider in-person.
Descriptive and unadjusted findings of reasons for delaying STBBI testing, benefits of online STBBI testing and drawbacks of online STBBI testing (n = 1369).
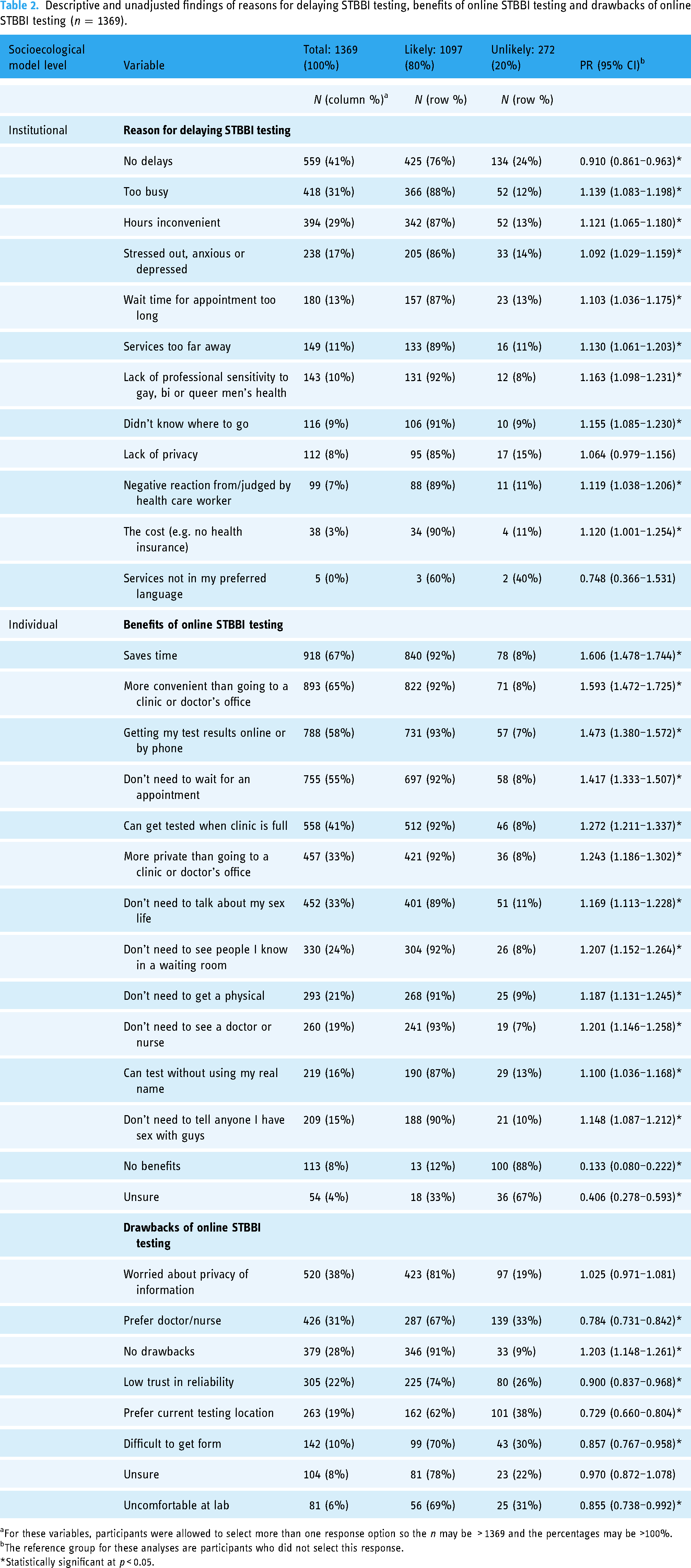
For these variables, participants were allowed to select more than one response option so the n may be > 1369 and the percentages may be >100%.
The reference group for these analyses are participants who did not select this response.
*Statistically significant at p < 0.05.
Unadjusted findings
Results of the bivariable analyses are shown in Tables 2 and 3. All assessed reasons for delaying STBBI testing were significantly associated with being likely to use online STBBI testing except for lack of privacy and services not being offered in participants’ preferred language, which were not associated. The prevalence of acceptability of online STBBI testing was highest among those who indicated that a lack of professional sensitivity about GBM health among providers was responsible for delayed testing for STBBIs (PR = 1.16, 95%CI: 1.098–1.231).
Unadjusted and adjusted findings of acceptability of online STBBI testing by variables of interest included in the multivariable model building process (n = 1369).

Number of different sexual behaviours engaged in over the past 6 months that are associated with increased STBBI transmission.
Comprised of questions asking when participants were last tested for STBBIs, usual place of testing and comfort with health clinics.
Number of forms of discrimination experienced in the past year based on ethnoracial identity, trans identity, sexual orientation, etc.
No estimate was obtained for the ‘Did not identify as Indigenous’ category in the Two-Spirit variable since it is the reciprocal of ‘Indigenous’ category in the ethnoracial identity variable when ethnoracial identity is entered into the model first. We have chosen to report the estimate for ‘Indigenous’ over ‘Did not identify as Indigenous’ as the former is a more important category in this analysis.
Not mutually exclusive with working full time.
*Statistically significant at p < 0.05.
All possible benefits of online STBBI testing were positively associated with acceptability, with the highest prevalence among those who selected that it saves time (PR = 1.61, 95%CI: 1.478–1.744). All possible drawbacks of using online STBBI testing were negatively associated with an increased acceptability, except for those who were worried about the privacy of their information which was not associated with the outcome (PR = 1.03, 95%CI: 0.971–1.081).
Other variables that were positively associated with increased acceptability in using online STBBI testing were: increased number of different sexual behaviours in the past six months associated with increased STBBI transmission (includes substance use during sex, number of sexual partners, condomless anal and vaginal intercourse, engaging in threesomes and group sex and being paid for sexual services); increased number of forms of discrimination experienced; identifying as a non-Indigenous, non-African/Caribbean/Black (ACB) person of colour; and not having been born in Canada. Variables that were significantly negatively associated with acceptability of an online STBBI testing service were: age; identifying as Two-Spirit; living in a small city, town, or rural area; not being open about one's sexual identity; and not currently working. All other variables were unassociated with being likely to use online STBBI testing.
Findings from adjusted models
During the model building process, 18 we excluded the variables of financial stability, disability, mental health, and relationship type as the unadjusted associations had p > 0.25. When entered back into the adjusted model one-at-a-time, they failed to contribute meaningfully to the model and remained excluded. Further, only one interaction examined was statistically significant (i.e. ethnoracial identity*immigration history) which we included in the final model.
Of the statistically significant unadjusted associations, only the following remained positively associated with acceptability of online STBBI testing in the final adjusted model (Table 3): younger age; greater number of different sexual behaviours in the past six months associated with greater STBBI transmission; identifying as an Indigenous immigrant versus white non-immigrant; and identifying as a non-Indigenous, non-ACB immigrant of colour versus white non-immigrant. The association between current HIV PrEP use and acceptability of online STBBI testing became statistically significant in the final adjusted model (PR = 0.894, 95%CI: 0.828–0.965) when compared to those who were not currently using HIV PrEP.
Discussion
The acceptability of online STBBI testing was high (80%) among GBM living in Ontario, Canada, higher than previously identified in a national sample of GBM in Canada (72%). 8 Based on our classification of all these variables using socioecological framing, we found evidence that individual, interpersonal and institutional factors are associated with an increased likelihood of using an online STBBI testing service. Saving time, convenience and getting results online or by phone were the three most commonly endorsed benefits, consistent with previous studies.8,16 Concerns over privacy of one's information and preference to see healthcare providers in-person were the two most common drawbacks selected in this study, also consistent with past work.8,16 Concern over the privacy of one's information may have been particularly salient for participants in our study due to a data breach that occurred at a national diagnostic testing service provider and was reported in the media while Sex Now 2019 was recruiting. 20 Additionally, while most participants delayed testing for STBBIs in-person, many of these same individuals indicated that they would be likely to use an online STBBI testing service if it were available.
Certain subgroups of GBM in Ontario were more likely to anticipate use of online STBBI testing. Younger GBM had increased acceptability of online STBBI testing, which has also been identified nationally. 8 However, in studies we conducted with GBM living in BC two years post-implementation of GCO, we found no statistically significant association between age and intention to use GCO, 16 and that actual service users were older than STBBI clinic users. 7 Future research examining the intention-to-practice gap for online STBBI testing among younger GBM is needed.
Current HIV PrEP users were less likely to use online STBBI testing than those who were not. As routine STBBI testing is required to obtain an HIV PrEP prescription in our setting, many HIV PrEP-using participants may be comfortable with their current testing regimen. This explanation is supported by qualitative interviews with users of GCO in BC. 10
For ethnoracial identity and immigration history, those who were not born in Canada and who identified as Asian or Latin American/Hispanic were more likely to use an online STBBI testing service compared to those who were white-identified and born in Canada. One systematic review examining barriers and facilitators to HIV testing in Canada found that among immigrant populations, barriers to HIV testing included: shame associated with requesting an HIV test and disclosing sexual information; concerns about confidentiality due to either being seen by or receiving services from a member of one's community; lack of health insurance; and linguistic or cultural barriers. 21 Other studies among immigrant men from specific racial/ethnic communities also suggest these as possible reasons for delaying or avoiding testing,22,23 which may explain why they would be more likely to use online STBBI testing in comparison to white non-immigrants in our study. We also found acceptability to be higher among Indigenous immigrants in comparison with white non-immigrants. However, this finding should be interpreted with caution as only four participants reported this overlap, and all four reported being likely to use online STBBI testing. Of note, Indigenous and ACB GBM still reported high acceptability of online STBBI testing at similar levels to white GBM. In addition, at the bivariable level, Indigenous Two-Spirit individuals were less likely to use online STBBI testing when compared with Indigenous individuals who were not Two-Spirit. However, this association was no longer statistically significant in the multivariable model as the presence of the HIV PrEP use variable and differential distribution of living with HIV between these groups nullified this association.
Moreover, a greater number of different sexual behaviours in the past six months associated with increased STBBI transmission were positively associated with acceptability of online STBBI testing. This finding is reassuring as many of the different behaviours that comprise this variable, such as condomless intercourse, multiple and concurrent sexual partners, illicit substance use during sex and the receipt of money or goods in exchange for sex, are all behaviours that GBM report as stigmatized.6,24–26 Participants who have engaged in these activities may either feel more comfortable disclosing these behaviours or not disclosing these behaviours at all when using an online STBBI testing service, rather than disclosing these activities to a service provider in order to avoid feeling judged or stigmatized. 6
Using socioecological framing, we found that individual factors associated with acceptability were: age, ethnoracial identity, immigration history, employment, outness and HIV PrEP use; all of which remained in the adjusted model except employment and outness. Interpersonal factors such as experiences of discrimination and sexual behaviours associated with increased risk of STBBI infection were also associated with increased acceptability of online STBBI testing with only the latter remaining significant in the adjusted model. Most of the institutional factors (reasons for delaying STBBI testing) were associated with increased acceptability of online STBBI testing except for services not available in participants’ preferred languages. Notably, while the associations for community-level factors such as geography and accessing healthcare services were not statistically significant in the adjusted model, the association for geography was in the unadjusted model. These findings illustrate the importance of considering the individual, interpersonal, institutional and community factors that influence GBM's use of online STBBI testing.
Strengths and limitations
Based on this study's cross-sectional design, we cannot infer causality between increased acceptability of online STBBI testing and variables of interest. However, this study design also allowed us to obtain a large sample of the GBM community, including many participants from subgroups often under-represented in other studies, such that we were amply powered to examine associations between variables of interest.
We acknowledge that intention to use online STBBI testing is not the same as actual use if the service were available. However, we have previously found that 42–45% of GCO users were GBM,7,27 and 3% of GBM surveyed 2 years post-implementation in BC had tested through the service. 16 This suggests that many GBM who report intending to use an online STBBI service do test through this platform, if available.
GBM who participated in Sex Now 2019 may differ from those who did not. For instance, as this was an online survey that could reach more geographic regions than in-person or paper-based recruitment, those without access to an electronic device or internet/data would not have participated. Additionally, those recruited from online spaces and who were willing to complete an online survey, may be more willing to use an online testing model than non-participants. We also attribute missing data in some cases to due to incomplete questionnaires, as participants were not required to respond to every question if they did not want to.
There were some differences in the sociodemographic information between those who answered all questions of interest and those who did not. This may bias the results towards higher acceptability of online testing, as those living in Canadian urban centres made up a larger proportion of those who answered every question (77%) than those who did not (44%) and were more likely to use online STBBI testing. However, our sample still included participants outside urban settings and online surveys of GBM tend to be better at reaching those living in non-urban settings. 28 Lastly, GBM who felt uncomfortable completing a survey in English or French may not have participated.
To our knowledge, ours is the first study to quantitatively examine acceptability of online STBBI testing among GBM in Ontario. Other strengths of this study include the use of a community-based research approach where members from the community were involved in all aspects of the study, including design, survey development, participant recruitment and data analysis. In addition, the use of multiple recruitment strategies is responsible for the large and diverse sample obtained. Furthermore, our decision to use modified Poisson regression models with robust variances allowed us to better ascertain and describe the prevalence of the findings reported in our study. Lastly, we elicited feedback from community advisors, particularly those from the Indigenous and Two-Spirit communities, to ensure that the study findings were communicated in a way that would be beneficial for said communities.
Future studies should consider recruiting more participants to assess variables of interest without overfitting of the multivariable model or collapsing categories of interest. This could provide more nuanced findings, such as how more specific experiences of marginalization affect being likely to use online STBBI testing. If possible, using sampling methods such as respondent driven or time-location sampling to obtain a more representative sample would also improve the generalizability of these findings. 29 Qualitative studies examining the acceptability of subgroups based on age, ethnoracial identity and immigration history could further explain online STBBI testing service acceptability.
Should implementation occur in Ontario, diverse promotional strategies will be needed to reach the various groups interested in using this service. Users of GCO in BC have mostly been individuals who have sought clinic-based testing but were instead redirected to GCO when the clinic was full. 27 Digital advertisements on community websites and social/sexual networking websites and mobile applications used by GBM have had varied success in increasing use of GCO, but advertisements in physical spaces frequented by this population remain to be a cost-effective way of increased engagement with GCO. 30 These strategies may be similarly effective in encouraging adoption among those not on PrEP and who engage in more behaviours associated with increased STBBI transmission. For reaching younger GBM and GBM from racialized and/or immigrant communities, a recent study in the US has found that pictured based digital advertisements on social/sexual networking mobile applications used by GBM to be effective in reaching young GBM and GBM of colour. 31 Increased community engagement and leadership in the design, delivery and scale-up of STBBI services may also increase uptake in these communities as well.32,33 We have also found GCO to be a cost-effective alternative for HIV testing among GBM living in Vancouver, BC when compared to clinic-based HIV testing services, 34 which may encourage policy makers to consider implementing a similar service in Ontario.
Conclusion
Acceptability of online STBBI testing was high among GBM living in Ontario, suggesting that it has the potential to address some of the barriers to in-person testing. Should implementation occur, promotion efforts to GBM should highlight benefits such as convenience, saving time and getting results online or by phone while addressing privacy concerns. Many important GBM subgroups are interested in and amenable to online STBBI testing, including those who are younger, not currently using HIV PrEP, who are people of colour not born in Canada, and who engaged in more sexual behaviours associated with increased STBBI transmission. Ensuring these subgroups have access to alternative testing options, such as online testing, may reduce the burden and inequities of STBBIs for this population.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231173557 - Supplemental material for Acceptability of an existing online sexually transmitted and blood-borne infection testing model among gay, bisexual and other men who have sex with men in Ontario, Canada
Supplemental material, sj-docx-1-dhj-10.1177_20552076231173557 for Acceptability of an existing online sexually transmitted and blood-borne infection testing model among gay, bisexual and other men who have sex with men in Ontario, Canada by Joshun JS Dulai, Mark Gilbert, Nathan J Lachowsky, Kiffer G Card, Ben Klassen, Jessy Dame, Ann N Burchell, Catherine Worthington, Aidan Ablona, Praney Anand, Ezra Blaque, Heeho Ryu, MacKenzie Stewart, David J Brennan and Daniel Grace in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to acknowledge Ryan Lisk from the AIDS Committee of Toronto (ACT), and the project's Ontario community advisory board (CAB) for providing feedback and support throughout all stages of this study. In particular, we would like to thank CAB member Aaron Bowerman for providing guidance on how to best interpret and present our findings that pertain to Indigenous and Two-Spirit communities. Most importantly, thank you to all the men, non-binary people and Two-Spirit individuals who participated in the Community Based Research Centre's Sex Now study, for without you, none of this work would be possible.
Authors’ Note
Preliminary findings from this study were presented as a poster at the 31st Annual Canadian Conference on HIV/AIDS Research (CAHR 2022), held virtually from 27–29 April 2022.
Contributorship
This project and its questions pertaining to acceptability, benefits and drawbacks of online STBBI testing were conceived by MG, DG, AA and CW. NJL, MG, KGC, DG, AA and BK were all involved in the design of the Sex Now 2019 study, survey and participant recruitment. This specific analysis was conceived by JJSD with feedback from all co-authors. JJSD led the analysis and writing of the initial manuscript draft under the supervision of DG. All other co-authors provided significant feedback on the analysis plan, data analysis and writing and editing of manuscript drafts. All authors have reviewed and approved this manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The research ethics boards at the University of Victoria (BC17–487), University of British Columbia (BC17–487), and the University of Toronto (37576) approved this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research [FRN: #CTW-1553878]. Sex Now 2019 received funding support from Canadian Blood Services MSM Research Fund, funded by the federal government (Health Canada) and the provincial and territorial ministries of health. The views herein do not necessarily reflect the views of the Canadian Institutes of Health Research, Canadian Blood Services, or the federal, provincial, or territorial governments of Canada. JJSD is supported by a Canada Graduate Scholarship – Doctoral Research Award from the Canadian Institutes of Health Research. MG is supported by an Applied Public Health Research Chair in Sexually Transmitted and Blood-Borne Infections. NJL was supported by a Michael Smith Foundation for Health Research Scholar Award [#16863]. ANB is supported by a Non-Clinician Scientist award from the Department of Family and Community Medicine, Faculty of Medicine, University of Toronto, and is a Canada Research Chair in Sexually Transmitted Infection Prevention. DJB is funded by the OHTN as an HIV Endgame Leadership Chair in Gay and Bisexual Men's Health. DG is supported by a Canada Research Chair in Sexual and Gender Minority Health.
Guarantor
DG.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.