
Abstract
The widely used socioecological rainbow model from Dahlgren and Whitehead specifies determinants of health inequity on multiple hierarchical levels and suggests that these determinants may interact both within and between levels. At the time of its inception, digital determinants only played a minor role in tackling inequities in public health and were therefore not specifically considered. This has dramatically changed: From today's perspective, health inequities increasingly depend on digital determinants. In this article, we suggest adapting the Dahlgren-Whitehead model to reflect these developments. We propose a model that allows formulating testable hypotheses, interpreting research findings, and developing policy implications against the background of the global spread of digital technologies. This may facilitate the development of a new line of research and logic models for public health interventions in the digital age. Using the COVID-19 pandemic as a case study, we illustrate how the digitization of all aspects of life affects the different levels of determinants of health inequities in the Dahlgren–Whitehead model. In doing so, we deliberately argue for not introducing a separate digital sphere in its own right, but for understanding digitization as a phenomenon that permeates all levels of determinants of health inequities. As a result, we present a digital rainbow model that integrates Dahlgren and Whitehead's 1991 model with digital environments to identify current health promotion and research issues without changing the rainbow model's initial structure.
This article outlines how our understanding and conceptualization of digital determinants of health inequities can be supported by adapting a widely-used socioecological model of health and health inequities, the ‘rainbow’ model of the determinants of health and health inequities. 1
At the time of writing this article, the COVID-19 pandemic was an ongoing global health threat, with implications reaching into virtually all aspects of everyday life. In this context, digital non-pharmaceutical interventions such as contact tracing apps, proximity recording devices, or QR-code-based admission systems highlighted the increasing importance of digital tools in public health. However, during the course of the pandemic, it has also become evident how such tools can cause health inequities—for example, through limited access to digital infrastructure, 2 lack of high-quality data that would allow developing of targeted measures for minorities, 3 or digital tools that were not tailored to the needs and abilities of their target populations. 4
The ‘rainbow’ model of health inequities is a socioecological model in which determinants of health and potential policy interventions are organized on five hierarchical levels. These are, in descending order (i) general socioeconomic, cultural, and environmental conditions, (ii) living and working conditions, (iii) social and community networks, (iv) individual lifestyle factors, and (v) age, sex and constitutional factors, with the latter being individual-level stable characteristics. On these levels, so-called “positive health factors”, “protective factors”, and “risk factors” are assumed to influence health—for example, on level (ii), hazardous working conditions would constitute a health risk factor. The unequal distribution of these factors is considered a determinant of health inequities—a violation of the ideal that everyone should be able to achieve their full health potential regardless of their social position or other socially determined factors.1,5 In our example, the exposure to hazardous working conditions is unequal, as workplaces that feature hazardous working conditions are disproportionally filled by individuals with lower educational attainment. If such an unequal distribution of health problems is considered avoidable or unjust, the term “health inequities” is applied. According to the WHO, “Equity is the absence of avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically.” 6 In the original (1991) version of the Dahlgren and Whitehead model, the different levels and the potential interactions and interdependent relationships between factors on the different levels are key to mapping and understanding the determinants of health inequities. Accordingly, policy measures to reduce health inequities can and should be distributed and organized on these levels. However, between the original specification of the levels and determinants of health inequities in 1991 and the third decade of the 21st century, technological advances and in particular the development of digital 1 tools and devices that are now widespread have re-shaped and influenced virtually every aspect of society as well as individual everyday lives. 5 These advances in digital technology and digital transformation also imply that the determinants of health and health inequities in Dahlgren and Whitehead's model are subject to a digital transformation, a process by which digital technology complements or replaces existing non-digital systems, and creates novel processes.
A recent article 7 proposed to add an additional level “Virtual world, information and communication technologies” on top of the existing five levels of the rainbow model, arguing that this scalar approach represents “the fundamental effect information and communication technologies (ICT) have on human health and on developing public health policy,” concluding with the notion that ICT, creating a virtual environment, operates outside of the existing levels. This extension of Dahlgren and Whitehead's model with an additional level allows examining how far the unique environment shaped by digital technologies affects health and health inequities. On the one hand, this addition emphasizes the paradigmatic shift encountered by the digital transformation in health, as many aspects of health as well as therapeutic and preventative efforts have experienced a qualitative shift rather than just a platform shift through the transfer into a digital environment. 8 On the other hand, however, this digital transformation has arguably permeated into most aspects of everyday life and therefore into most of the layers and levels in the Dahlgren and Whitehead model.
Therefore, rather than constructing a novel, separate layer of influence, we suggest that the existing levels provide a usable framework to describe, examine, and modify digital determinants of health inequities—by specifying the digital influences within the existing levels. This allows hypothesizing and examining within-and between-layer interactions: for example, differences between countries in popular opinion to which extent digital patient records are deemed acceptable (an example of a “general socioeconomic, cultural and environmental” condition on the outermost layer) can influence the degree to which digital tools are likely to be utilized in shared decision-making processes between patient and healthcare provider (an example of healthcare provision, an aspect of “living and working conditions.” 1 At the same time, it is possible that digital developments in one particular domain within one layer can buffer or exacerbate the effects of other digital determinants in the same layer. For example, telemedicine applications to service remote and rural areas with specialist medical care and knowledge can indeed improve access for otherwise disadvantaged 2 populations—in particular in emergency situations such as the COVID-19 pandemic. 9 In addition, socioeconomic barriers to accessing telemedicine services—either through lack of individual resources such sufficient bandwidth and data volume or through the lack of effective technological and personnel infrastructure are likely to exacerbate existing inequities in access to specialist medical services. 10
In this article, we briefly illustrate the original levels of policy in the Dahlgren and Whitehead Model. Second, we outline how digital developments can be integrated into the model to derive testable hypotheses, interpret research findings, and develop policy implications (Figure 1). This may facilitate the development of new lines of research and logic models for public health interventions.
General socioeconomic, cultural, and environmental conditions
On the highest level of analysis (Policy Level 1), Dahlgren and Whitehead emphasize the relevance of socioeconomic, cultural, and environmental factors as determinants of population health from an equity-in-health perspective. They argue that health inequities have increased as a result of neoliberal economic policies and globalization. These health inequities could be addressed by strengthening international organizations to counter the neoliberal paradigm. On the one hand, the general global economic policy counts as one influential socioeconomic determinant of health inequities. On the other hand, an equity-in-health perspective must also shift to individual countries, infrastructural factors and, in particular, national legislations. 1
With regard to digital technologies, a focus on this level lies on the different generational resource allocations and the political implementation of data protection policies. In the context of the COVID-19 pandemic, more and more digital health technologies such as contact tracing apps have been developed and distributed. The use of these technologies requires access to technology and—in most cases—broadband mobile data services. As a result of the so-called “digital divide,” barriers to digital access differ between different population groups. Interventions on this level could accordingly contain measures to improve access through both infrastructure and distribution measures that consider the needs of diverse populations. 11 For example, to improve access to emergency services during the COVID-19 pandemic, cell phones were handed out through health care providers in Ontario, Canada. 12 At the same time, such structural interventions require the accompaniment of digital literacy measures to address health inequalities. 13 Other aspects concern the legal design of data protection: Although legal issues have been raised here before, they have taken on new significance in the digital age, as trust in good data protection legislation is central to the success of digital interventions. 14
Living and working conditions
Living and working conditions assume a central position in both determining health inequities and as entry points for strategies and policies to reduce health inequities in the initial formulation of the rainbow model. It is within these everyday settings where people are most likely to encounter, recognize, and experience the health consequences of digital developments. Digital technology increasingly affects most living and working conditions, as it serves as a gatekeeper to health services and other social determinants of health. For example, increasing digitization of health services can limit the access to and the availability of such services to those who have stable and reliable internet access. 20 Difficulties in accessing the internet can reduce access to essential social determinants of health: In a qualitative study, Baum and colleagues 21 highlight that limited internet access also limits access to (in particular higher) education, the housing market, employment options and social networks. This in turn can create a vicious cycle of social disadvantage and increasing health inequities. Difficulties in internet access can thus lead to worse health outcomes and increased health inequities through both direct (problems accessing health services) and indirect (problems accessing wider determinants of health) routes. 22 We present three exemplary aspects of living and working conditions in which digital transformation processes could affect health equity—workplace features, housing, and the delivery of healthcare—knowing that digital transformation processes will affect equity aspects of the health impacts in other living and working conditions specified in the rainbow model as well (educational settings, food and agricultural sectors, water and sanitation, unemployment).
Work environment: In the rainbow model, the work environment is conceptualized as a place where social inequities, for example differences in educational attainment, resulting in differential exposure to work-related health risks. Such inequity effects are also conceivable with regard to digital factors in the workplace. For example, workplaces and occupations that are more likely to be occupied by individuals with lower educational attainment such as delivery drivers are increasingly using digital technology with biometric sensors to monitor driver behavior, or tracking time off task through digital assistants at warehouses.15,16 These factors (limited personal control, external targets, digital monitoring) in turn have been related to increases in work-related stress, turnover intent, and lower mental health.17,18
Housing: Housing has been conceptualized as the entry point for health inequities as for example housing-related health risks such as the concentration of indoor air pollutants are more likely to affect disadvantaged populations. 19 However, socioeconomic differences in the quality of housing could also affect how digital determinants affect health—disadvantaged populations are less likely to be able to access the internet with sufficient bandwidth, either through financial (expensive contracts) or physical (slow internet connections in rural and disadvantaged locations, shared internet access within one or multiple households) barriers, which in turn can lead to inequities in the access to quality health information and care.
Health Care: Originally conceptualized to explain health inequities through differences in access to quality health care, universal health insurance, or outreach services for vulnerable populations, this sector has also equity implications through digital technologies. For example, telemedicine applications to service remote and rural areas with specialist medical care and knowledge can indeed improve access for otherwise disadvantaged populations—in particular in emergency situations such as the SARS-CoV-2 pandemic.9,23 As discussed above, socioeconomic barriers to access telemedicine services—either through lack of individual resources such as internet provider contracts with sufficient bandwidth and data volume 24 or through the lack of effective technological and personnel infrastructure 25 are likely to exacerbate existing inequities in access to medical services. Increasingly, health insurances employ digital assistants in customer contact, for example in directing customers to appropriate healthcare providers, and it is not entirely unlikely that the lower costs incurred through such digital assistants could lead to their increasing implementation in lower cost tariffs.
On the basis of the different sectors within this layer, it is further possible to identify research areas both in cross-sectoral and cross-layer interactions. An example for a cross-sectoral interaction are additive effects on health inequities caused through housing aspects such as slow internet connections and inequities in health services such as more digital assistants in cost-saving tariffs. Cross-layer interactions could be inequities caused through inequities through digital health services access (digital assistants) and lower levels of digital health literacy in those with lower educational attainment (layer “individual lifestyle factors”).
Equity aspects of social and community networks
On the level of social and community networks, Dahlgren and Whitehead 1 suggest that weak social support networks are linked to a wide spectrum of conditions, while supportive relationships have protective effects. They also suggest that social networks and support systems might be weaker among disadvantaged groups. 1 Accordingly, in order to promote equity in health, social networks should be strengthened in deprived areas. This could be done by creating meeting places, including those for defined groups (e.g., single mothers, elderly, etc.). Another approach focuses on more targeted community development projects (e.g., improving access to health information, collective action on defined causes of diseases, improving self-confidence and the possibilities to influence health policies). In a more recent version of this chapter (now labeled “Social and community inclusion policies”) Dahlgren and Whitehead introduce vertical social interactions. Vertical is understood as bringing groups from different positions at the social scale together. 1 While vertical approaches operate on a society-wide basis, horizontal approaches are clustered locally.
The term “social networks” has gained, or rather added, a whole new meaning since the first publication of the “rainbow” model. Today, the term social network also refers to “… a website that is designed to help people communicate and share information, photographs, etc. with a group.” 26 In fact, internet-based services such as social networks or internet fora are increasingly used to connect individuals with each other. A comprehensive list of internet-based social networks relevant to public health has been suggested by Griffiths and Dobermann. 27 They distinguish between different functions: dissemination of information, collection and, collation, and correction of information, emotional support, campaigning, and fundraising.
In how far do digital platforms increase or decrease equity in health? Dahlgren and Whitehead stated that (analog) social networks are weaker among socially disadvantaged and assign them “lower participation rates in decisions that affect their lives.” In order to participate in digital platforms, a minimum of technical equipment is required. While access to smartphones and affordable internet flat rates has widened during the past years, the non-material hurdles might be more difficult to surpass. A basic level of digital literacy is required to engage with and post on these platforms, At the same time, the amount of (health) misinformation distributed through social media platforms requires skills and resources. However, these skills and resources are unequally distributed, as will be detailed below.
An advantage for financially limited groups is the lack of additional costs for most health-related information on the internet. At the same time, being able to critically assess the quality of this information and misinformation for health benefits requires resources in terms of literacy, which again are unequally distributed. For example, a recent survey in Germany found lower digital health literacy to be associated with higher age, lower educational attainment, and lower income. 28 Social differences in health literacy might therefore lead to individuals with a low level of health literacy being worse off with than without sometimes contradictory health (mis)information from different sources. An overview of reviews 29 found only limited evidence that interactive social media interventions might improve health outcomes, health behavior, and in particular health equity. Specifically for social media platforms with existing social networks, it was concluded that more research is needed to assess the effects on health outcomes and health equity in populations at risk for disadvantage. Some sources highlighted the potential for social media to reach populations who might be difficult to reach otherwise.
In sum, social networks do have the potential to improve or deteriorate health and to reinforce or mitigate health equity. Digital social networks might need some minimum level of curation to enable an exchange of information that is aligned with the goals of improving health and health equity.
Individual and lifestyle factors
This fourth level refers to individual resources as well as personal behavior and ways of living that can both promote or damage health. Lifestyles are socially patterned with more disadvantaged individuals tending to adopt more unhealthy behaviors such as smoking, sedentary lifestyles or unhealthy eating habits compared to their more advantaged counterparts. 30 This implies that lifestyle-related health inequities may be reduced through targeted health education programs and policies in the form of food labeling and nutrition education to positively influence individual eating habits. At the same time, Dahlgren and Whitehead acknowledge that individual lifestyles are determined by constraints of monetary and time resources. As a result, policies aiming to improve an individual's lifestyle need to take restrictions on choice into account. 31
The availability and use of digital technologies permeate almost every aspect of individuals’ lifestyles and as such have the potential to influence health outcomes. There are multiple pathways where research has found the use of digital technologies to negatively impact health—for example, a systematic review and meta-analysis on smartphone usage and mental health outcomes among children and young people suggests a consistent relationship between excessive screen-time using smartphones and negative mental health outcomes including anxiety, depression and poor sleep. 32 There are consistent associations between problematic smartphone use and lower physical and mental quality of life, 33 which is likely due to increased risks of poor sleep quality and anxiety as well as depression symptoms. 34 At the same time, if designed and implemented well, digital technology can support interventions to promote more active and healthier lifestyles through easy access to health-related information (e.g. websites about nutrition) and promotion of physical activity (e.g. fitness tracker and running apps). For example, digitally mediated behavior change interventions that make use of evidence-based behavior change techniques are indeed effective in reducing sedentary behaviors and increasing physical activity. 35
This means that exposure to digital technology and digitally mediated content can—at least to a degree—constitute a health-protective factor (through better access to quality health information or quality intervention content) or a health risk factor (through for example being exposed to health-related misinformation or questionable social norms as discussed above). This could explain seemingly contradictory evidence: Individuals from more socially disadvantaged backgrounds on the one hand engage more in digitally determined sedentary lifestyles and less in health-promoting activities, 36 which suggests more access to digital tools. At the same time, individuals from disadvantaged backgrounds might have greater difficulties in obtaining and interacting with health-promoting technology, in particular, if this access requires tangible or intangible resources. 37 This in turn may increase health inequities. Similarly, digital access can facilitate access to reliable health information online but at the same time increase exposure to health misinformation, which again depends on unequally distributed individual resources. 38 The degree to which digital access constitutes positive health protective factors or negative exposure and health risk factors is likely to depend on a person's access to tangible and intangible resources—which are likely to overlap with the known sociostructural risk factors for health inequalities (for an overview and classification suggestion, consider the PROGRESS-Plus 39 framework). 40
Further, lower levels of competence in finding and understanding health-related information on the internet may exacerbate health inequities. A large study in 28 European countries found that particularly older males were less likely to use the internet for health purposes, and at the same time access less high-quality health information. 41 These differences in turn can contribute to health inequities. While age differences in access to digital technology for health purposes have been documented for over 20 years, 42 current research highlights that these age differences need to be differentiated further—for example, white older Americans were much more likely to extensively use the internet to search for health information and health services than older black Americans. 43
The examples mentioned above are just a few to illustrate how digital technology may affect health inequities through individual lifestyles and according to individual socio-structural factors. Examining relationships between factors on the individual level and health inequities should therefore be an integral part of policies improving the digital transformation in health.
Discussion
In this essay, we have suggested an extension of the “rainbow” model 1 to theorize, operationalize and test digital determinants of health inequities. We suggest that digital determinants of health are organized on multiple hierarchical levels starting from individual-level determinants such as educational attainment to higher-level determinants such as cultural or policy norms. The implication is that health inequities are the result of differential access to resources and barriers in these layers. Importantly, cross-level interactions of the digital determinants may have increasing or limiting effects on inequities in health. This also implies that there are possible interactions by which the effects of specific determinants might be exacerbated or buffered through other determinants.
Here, we apply this hierarchical multi-level structure to outline in how far the application of digital technology within the contexts of the domains in the “rainbow” model can lead to inequities in health—and, at the same time, how targeted changes and improvements in resources on these multiple levels might contribute to overall improvements in health, and decreasing inequities in health at the same time. In order for digital technologies to help reduce health inequities, it is crucial to provide access to such technologies to the entirety of the population. As such, strategies aiming at improving lifestyles through digital means need to be based on an understanding of the availability and restrictions on the choices of individuals in general and more importantly of individuals from disadvantaged backgrounds. This includes bottom-up approaches such as participatory design for developing digital health technologies in order to meet the specific needs of the target population. Additionally, educational approaches to ensure sufficient digital literacy (i.e. an individual's ability to find, evaluate and communicate information through digital media; https://literacy.ala.org/digital-literacy/) in all groups of the population, not only the most highly educated, may help to facilitate access to digital health technologies. Widespread access to digital services and technologies may help narrow the digital divide and as such promote and improve healthy lifestyles for all individuals, not just those from more advantaged backgrounds. At the same time, access to digital services can constitute a risk factor for worse health—be it through direct effects such as increased sedentary behavior, 36 poorer sleep quality, 34 or exposure to health misinformation. 38 The degree to which, for any person, digital access constitutes a resource for better health or a risk factor for worse health, likely depends on individual resources such as digital health literacy.13,37
Further, through the digital “rainbow” model we can specify levels with specific domains of determinants of health inequities. These domains can be used to both organize systematic observation and research on specific and interactive effects of digital technologies on health inequities at these levels, which in turn allows formulating specific hypotheses about the effects of these determinants.
The example of the German digital COVID-19 Warning App illustrates that digital technologies in public health may have effects on health inequities through various pathways on multiple levels and interactions between levels: For example, on the layer of general socioeconomic factors, shared attitudes requiring high levels of privacy and data protection led to multiple consent requirements in the app, which is likely to have disenfranchised disadvantaged users (an individual-level factor), in particular since it was not clearly communicated in how far this additional burden could lead to individual benefits for the user. Table 1 highlights further potential interactions, which emphasizes the practicability and relevance of including digital aspects into the existing layers of the rainbow model. Singular or multiple additional digital environment factors would not suffice to describe these interactions or allow deriving testable hypotheses.
German COVID-19 warning app.

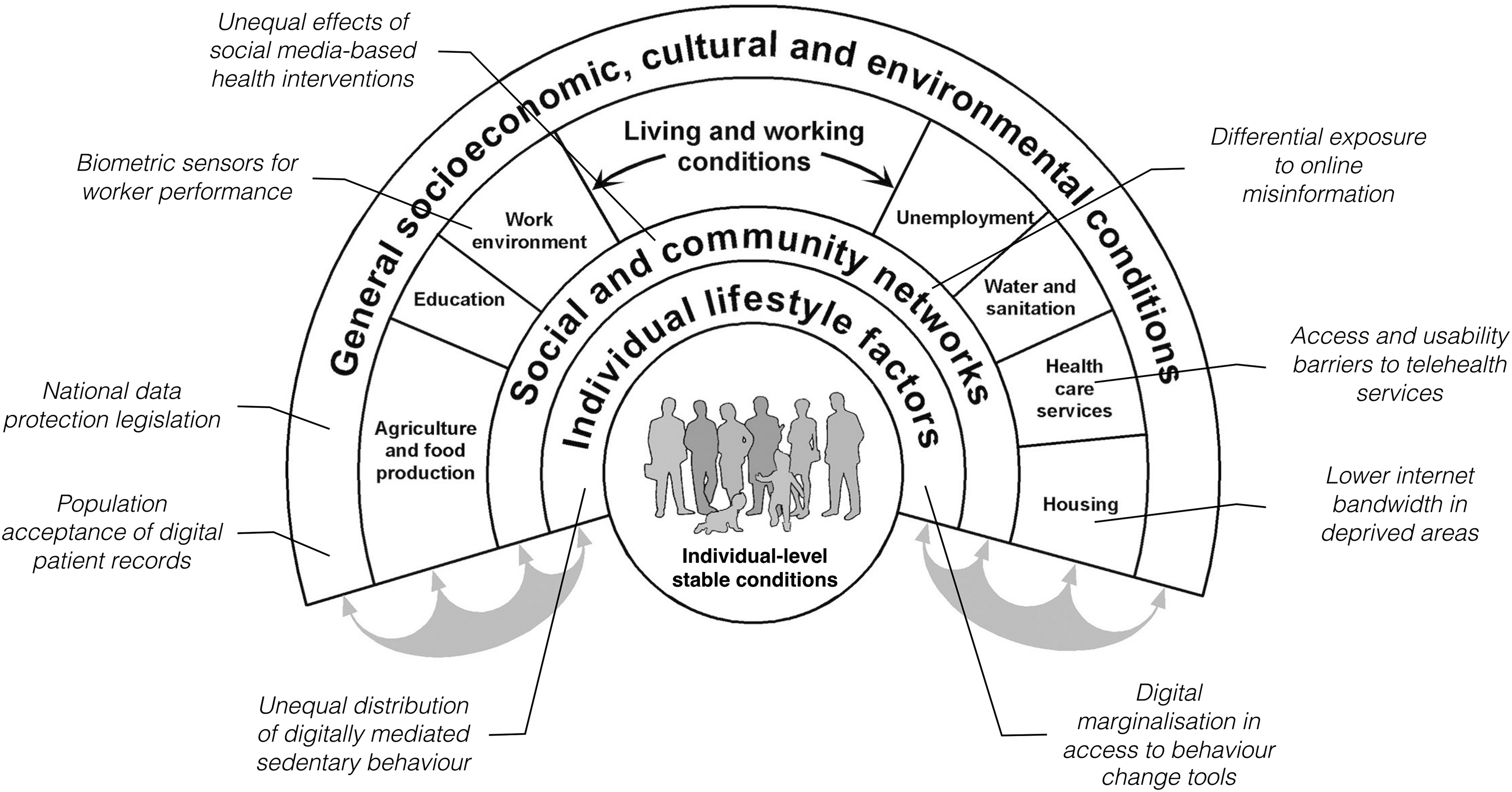
Rainbow model (figure based on Dahlgren and Whitehead 5 ) with examples for digital entry points of health inequality.
The “digital rainbow” also allows applying the current discussion on how commercial interests influence the determinants of health49,50 to digital influences on health. The papers mentioned above discuss how far commercial interests of tobacco, alcohol, food and other commodity producers, 50 or, in addition, commercial enterprises that profit from the commodification of privatized health or education services, 49 contribute to health inequities. In the digital context, for example, the algorithms underlying social media platforms provide users with escalating content including health misinformation in order to keep them engaged with the platforms for longer periods of time, thus maximizing advertisement revenue. The increased exposure to health misinformation is thus not a bug, but a key feature of these algorithms in order to maximize the time people spend on these platforms, 51 which illustrates the intertwining of commercial interests with digital determinants of health. As the degree to which individuals are susceptible to health misinformation again depends on individual resources, this can lead to increased health inequalities if users from disadvantaged backgrounds for example refuse protective behaviors or choose not to get vaccinated against COVID-19. 38
Implications for research and practice
A socioecological model such as the “digital rainbow” provides a template for the development of a framework for equity-based evaluations of digital applications in public health. While not every domain and every level might be of relevance for every digital application, the general notion of multiple levels and interactions is an important addition to research on digital applications in public health.
This notion allows theorizing and developing outcome dimensions for the evaluation of digital technologies in public health on multiple levels, thus bearing potential implications for the assessment of such technologies: If there is a plausible model for how inequity effects might be generated by the contexts and domains of the digital rainbow model, then targeted research (either original or secondary data and reviews) can examine the plausibility of such influences. Ultimately, this may provide an argument for including these outcomes in the criteria for evaluating frameworks. 3 Most importantly, the potential interactions of domains both within and between levels can provide plausible pathways for the examination of hitherto unknown mechanisms by which digital technology could lead to inequities in health. 52
Limitations
This essay is subject to several limitations that might impact the implications drawn. First, the selection of the literature has been purposeful rather than systematic. However, as the main aim of this paper was the development and illustration of digital influences within the layers of Dahlgren and Whitehead's model of the determinants of health inequities rather than a systematic overview of the evidence, this limitation might be less consequential compared to an evidence review. Second, it is acknowledged that both the number of layers and sections within layers of the original model are somewhat arbitrary. However, the main issue here is to illustrate a hierarchical socioecological framework of determinants of health inequities—specific health outcomes might require other levels of layers and different sections. Third, our discussion focuses on analyzing digital determinants of health inequalities. These inequalities can result from interventions employing digital technologies, but leave open the question of effective interventions to mitigate such inequalities. However, the model might be useful in identifying interactions between layers, which in turn can be used to identify entry points for interventions to reduce health inequalities.
Conclusion
Digital technology permeates virtually every aspect of our everyday lives, and as such are deeply embedded within the health-constituting settings in which we “live, work, learn and play.” At the same time, digital technology exerts its effects on health and health inequities within and through these settings. The “digital rainbow” model proposed here outlines where the effects of digital technologies might be located, and thus offers implications for further development of theory and applications to reduce inequities in health.
Footnotes
Acknowledgments:
The authors acknowledge the support of the Leibniz ScienceCampus Digital Public Health in enabling and contributing to the workshop discussion around the initial ideas for this manuscript.
Contributorship
BS and TJ conceived the concept of the manuscript. BS drafted the first version of the manuscript. HHD, AG and TJ contributed to the literature search, writing and editing of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding:
The authors gratefully acknowledge the Leibniz ScienceCampus Bremen Digital Public Health (lsc-diph.de) support, jointly funded by the Leibniz Association (W4/2018), the Federal State of Bremen, and the Leibniz Institute for Prevention Research and Epidemiology—BIPS.
Ethical approval
Not applicable as no human or animal data was used in this study.
Guarantor
BS.