
Abstract
Objective
Chlamydia is one of the most common sexually transmitted infections in teenagers and young adults. This study used a mixed-methods analysis to investigate targeted promotion of chlamydia home-testing on social media.
Methods
Our first study, in which face-to-face interviews with young women were conducted, sought to explore their attitudes and preferences towards social media-based health promotion. Our second study used Facebook and Google analytics to examine visits to a chlamydia testing page (where chlamydia testing kits could be ordered online), both before and after a targeted Facebook-based health promotion campaign was conducted.
Results
The interviews revealed Facebook to be the preferred choice of social media, with participants perceiving it to be a powerful and far-reaching platform for social interaction. Participants also highlighted several aspects of promotional content to be important at increasing engagement with the target population, including appropriate use of colour, level of interactivity, use of humour and anonymity. The website analysis showed a 277% increase in the direct entrance on the chlamydia testing kit page and a 41% increase in chlamydia test kit orders, in comparison with the baseline period prior to the intervention.
Conclusions
The findings support social media as an engaging medium for the online promotion of chlamydia self-testing and implicate Facebook advertising as a useful tool in addition to community-based chlamydia screening services. Future research needs to identify whether targeted social media-based health promotion could lead to higher chlamydia diagnosis rate in comparison to traditional communication channels.
Introduction
Worldwide, 1 in 20 young people annually contract a curable sexually transmitted infection (STI). 1 In the UK, STI rates remain high, with approximately half a million new cases occurring each year. 2 The estimated costs of STI treatments provided by the National Health Service (NHS) equate to £620 million per year. 3 Young women remain at a disproportionately higher risk of acquiring an STI than men, 2 in part due to the asymptomatic nature of many female-acquired STIs and the failure to recognise infections before they spread. The World Health Organization, supported by Public Health England, subsequently identify heterosexual females aged 15–24 years as a high-risk group for STIs.
In England, women under the age of 25 are at an increased risk for chlamydia. It is the most common STI and, if untreated, it can result in pelvic inflammatory disease and infertility. In 2016, over 1.4 million chlamydia tests were carried out and over 128,000 chlamydia diagnoses were made among young people aged 15–24 years. 2 Chlamydia represents almost one-half (49%) of all STI diagnoses in the UK annually and therefore efforts to combat this rate must be maintained. Since 2003, an opportunistic National Chlamydia Screening Programme has been introduced in England for both males and females aged 15–24 years. Within the programme, chlamydia tests are distributed in various community and health settings, such as sexual health and general practice clinics. However, there has been a continuous decline in chlamydia screening since 2013. 2 The number of tests fell by 8% between 2016 and 2017, thus novel ways of promoting chlamydia screening need to be identified.
Targeted sexual health promotion on social media
Description of popular social media sites

*Descriptions presented from Google Search
There is evidence suggesting that interventions developed for social media increase safe sex behaviours, such as condom use,7,8 and reduce STI incidence. 7 Social media services allow for ‘targeted marketing’ where advertisement recipients can be narrowly selected by gender, age, ethnicity, sexual orientation, geo-positioning and specific online behaviours such as location ‘check-in’ and endorsement ‘like’ buttons. 9 That technology allows health intervention designers to select their most relevant populations, which might be ‘hard-to-reach’ through conventional communication channels. A scoping review on the use of social media for sexual health promotion indicated that these interventions are capable of increasing knowledge about STIs, resulting in desired short-term behavioural outcomes such as HIV testing or chlamydia screening. 10 Nevertheless, it is still unclear whether social media interventions can lead to permanent changes in behaviours such as consistent condom use, as only a few studies have attempted to examine their effects over time.
The utilisation of social media as a medium to distribute sexual health interventions is relatively new, so there remains a need to understand which type of intervention content appeals most to the target audience. By identifying the type of content young people respond to best, interventions can be designed and tailored to produce optimal results. Previous research on the use of social media for sexual health communication showed that young people were concerned about bullying, their privacy, embarrassment and stigma attached to sexual health.11,12 While scare tactics were seen as unhelpful, the researchers suggested that humour was capable of overcoming stigma and promoting engagement with clinical services. Therefore, we conducted two studies aimed (a) at assessing the attitudes and preferences of young women towards receiving sexual health information via social media, and (b) at examining the outcome of a targeted Facebook health advertisement promoting chlamydia screening. The overall objective of this research was to determine whether social media advertisement could be utilised to increase the uptake of chlamydia screening in young people.
Study 1: method
Design
We used a qualitative approach incorporating semi-structured interviews and thematic analysis to explore young women’s views on sexual health promotion on social media. Our interviews were supported by a topic schedule, and were conducted between January and March 2017 at the campus of Southampton University. The study was approved by the University of Southampton Ethics Committee (reference: 24235)
Recruitment and participants
We aimed to recruit women who might be at higher risk of chlamydia. We advertised our study using wall posters, aimed at sexually active women, at various venues within the University of Southampton, as previous studies indicated that female students were susceptible to STIs due to living in settings with substantial social mixing. 13 The participation was voluntary and no incentive was offered. Interested women were asked to contact the researchers to arrange an interview.
In total, 19 female undergraduate students took part in this study, with an age range of 18–24 years (median = 20). Sixteen participants identified as White British and two as Black British, and all self-identified as heterosexual.
Procedure and data collection
Data collection and analysis were conducted by three psychology students who received comprehensive training on qualitative research methods. At the beginning of the interview, all participants were shown an information sheet outlining confidentiality and the right to withdraw at any time. Women were then asked to sign a consent form. All interviews were audio-recorded and lasted around 20 minutes. The topic schedule consisted of six questions about attitudes towards sexual health promotion on social media, preferences for the content of promotional campaigns, as well as potential barriers and facilitators to engagement with social media health promotion for women at risk of STIs. Based on individual responses, the interviewer aimed to explore in-depth which components of social media health promotion might be the most attractive and appealing. The interview finished by debriefing participants and offering information about local sexual health services.
Data analysis
The audio-recordings were transcribed verbatim and data were anonymised. Thematic analysis 14 was performed to identify commonalities and patterns of responses as emerging from the raw data. Researchers familiarised themselves with the data before engaging in the initial coding. Each researcher was asked to identify candidate themes and subthemes. This process was conducted independently to increase the validity of the overall data analysis. The results were then compared and discussed among the researchers. In case of disagreement, the lead researcher (TN) was contacted to resolve any ambiguities on the final set of themes and subthemes.
Study 1: results
In general, women in our sample had moderate knowledge about STIs and poor awareness of available screening services, including self-sampling that could be conducted at home or any other off-clinic settings. Five participants were able to recall a social media advert for sexual health (i.e. contraception and condoms), but none could remember any particular chlamydia screening campaign prior to the study. Table 1 outlines four themes and exemplary quotes in relation to our first aim: ‘preference for social media’, ‘advert form’, ‘promotion focus’ and ‘concerns over social media’.
Exemplar quotes from thematic analysis on the use of social media for targeted sexual health promotion.

Preference for social media
Most women reported using mobile phones to access social media as opposed to other digital devices. When asked about their preferences for using social media to view content about sexual health, the participants talked about the mainstream popular sites, i.e. Facebook, Twitter, Instagram, Snapchat and YouTube. Facebook was seen as the most frequently used site, on which participants spent most of their time. It was viewed as the site with the highest number of users and social networks. Facebook was also perceived as the site where digital content can go ‘viral’ by sharing and acknowledging it between users. Several women thought that Twitter was mainly for explicit and more serious content, where users were able to verbalise their political and activist views. Instagram was also seen as an appealing site for aesthetics and visual content, such as pictures and personalised videos. Several participants agreed that sexual health campaigns could be incorporated into Snapchat and YouTube as the users tend to be displayed promotional or marketing material before they can use these services. However, compulsory advertisement viewing was seen as repetitive, potentially leading to habituation, annoyance and an increased tendency for women to tune out from the message of the advertisement.
Advert form
Women perceived various forms of engaging sexual health promotion, such as short and comprehensive online videos, animated characters, cartoons and still pictures. The participants agreed that the choice of colour was important as it would affect the way people may feel or think about sex, but there was no consensus regarding which colours were perceived as more attractive. A few women thought that bright and colourful adverts were ‘eye-catching’ and ‘positive’, while ‘plain and simple’ were viewed as ‘boring’ and unappealing. The majority of participants viewed short animations and videos to be more appealing than still pictures at gaining their attention, allowing the promotional content to be absorbed and remembered. However, the length of the video or animation was seen as important for the engagement, with most women having a preference for shorter videos, notably under 1 minute long. In videos, the use of narration was perceived as more engaging and likeable over reading lines of text. Women felt that sexual health adverts should use positive, personal and empowering messages that can make them feel good about themselves.
Promotion focus
All women believed that sexual health promotion needs to be interactive and engaging in order to immediately attract the attention of views. Some participants felt that the use of ‘real-life’ characters such as celebrities or known people from their community could to allow them to relate to the content of sexual health adverts, making it more realistic and genuine. They discussed personal similarities between the characters in the adverts and themselves in terms of age or ethnicity. Women also thought that sexual health adverts need to be humorous and light, instead of scary and terrifying. However, a minority of the participants were against the use of excessive humour regarding sexual health, as this could diminish its seriousness and significance. Many reported preferences for factual information, such as the percentage or ratio of women experiencing chlamydia, as a good way of outlining the scope of the problem and attracting women’s attention. In this context, ‘shock’, understood as a reaction to unexpected information about personal risk, or disbelief were perceived as having a positive effect on engagement with the advert.
Concerns over social media
Women expressed several concerns about sexual health promotion on social media. These were mainly related to privacy and confidentiality, as the participants preferred not to be seen as those viewing sexual health adverts. The majority of women thought that targeted advertisement on social media was a good idea, but they were against interventions that could show other users that they had been interested in STI screening. The participants were concerned about being stigmatised and perceived as promiscuous. Their anonymity was central to the engagement, and interventions that could leave traces of their online activity were seen as unsuitable. Most women were against being contacted via social media directly by clinical services with questions about their sexual health and screening. Thus, the indirectness of sexual health communication on social media was viewed as essential for the success of this intervention type.
Study 2: method
Design and intervention
A Facebook-based sexual health promotion campaign was developed to promote home-based chlamydia testing to adolescents and young adults. The Facebook advert was a graphic interchange format (.gif) animation that lasted 10 seconds on a loop, with three messages: ‘You are unique. You are important. Your sexual health matters to us. Free and easy chlamydia test online.’ Users that clicked on the animation were automatically taken to the www.letstalkaboutit.nhs.uk chlamydia screening site, where they were able to order a home-based testing kit to be delivered to the place of their choosing by post. The website activity data were analysed to determine whether the Facebook advertisement affected engagement with an online chlamydia testing service. Two time periods, a baseline (4 August to 14 September 2017) and the intervention (15 September to 26 October 2017), were included in the analysis. The survey was approved as a service evaluation by Solent NHS Trust Clinical Governance (reference: SE-255). For ethical reasons, the advert was not restricted to women to reduce inequality in access to chlamydia screening amongst young people.
Data collection and analysis
The Facebook advert cost £1000 and was set to appear on the Facebook news feed of users, who were between the ages of 13 and 24 years, living in the county of Hampshire, UK. The advert, as well as the chlamydia testing kits, were not restricted to women only as part of the local sexual health services but were taken as an indicator of potential engagement through social media. Data about user engagement with the intervention were generated automatically by Facebook and Google analytics. A similar method of data analysis was used in previous research on sexual health promotion on social media. 15 Analysed data referred to the website activity where chlamydia test kits could be requested (www.letstalkaboutit.nhs.uk). Selected data were analysed to compare the periods before and after the Facebook advertisement. Facebook analytics was used to measure the engagement with the chlamydia advert, particularly the ‘click-through rate’. We used Google analytics to measure the number of visits to chlamydia testing webpages and relevant sexual health service pages. We also assessed the total number of chlamydia tests requested during the two periods, available from the distributor of the testing kit. Data were analysed using descriptive statistics.
Study 2: results
In total, the Facebook advertisement reached 40,347 women and 37,292 men, of which 1400 women and 1413 men interacted with the advert (3.6%) over the period of the intervention. Amongst those who interacted, 27% were between 13 and 17 years of age. The advertisement resulted in 2825 visits to the chlamydia testing page out of 348,777 impressions of the advert (see Table 2). We observed a 277% increase in the direct entrance on the chlamydia testing kit page and a 41% increase in chlamydia test kit orders, a 29% increase in the number of samples tested and a 36% increase in positive chlamydia results in comparison to the baseline period prior to advertisement. There was an overall increase in the visits to sexual health webpages between the two periods.
Engagement with the chlamydia testing advert, page, and the number of test kits before and after the targeted Facebook advertisement.
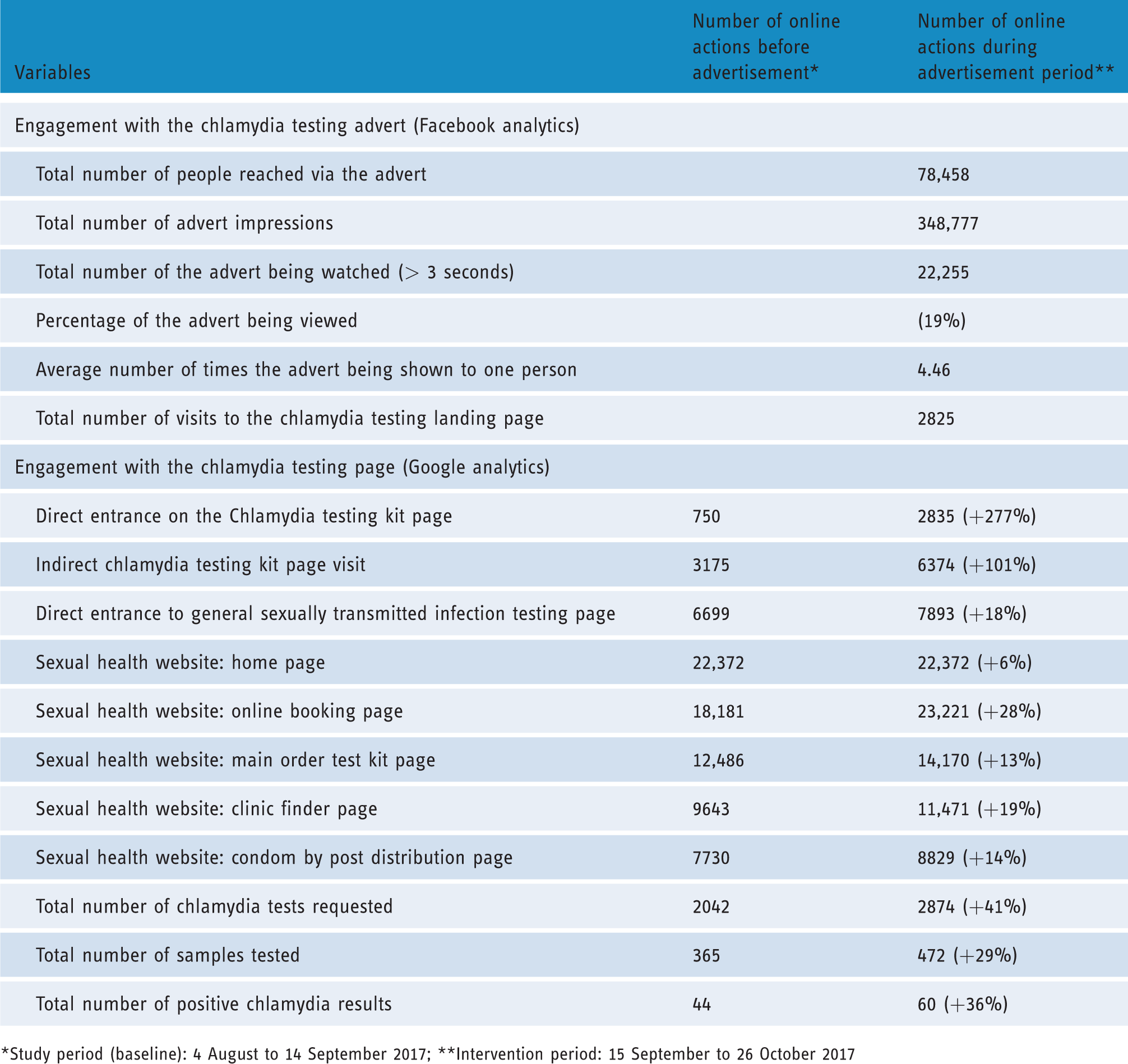
*Study period (baseline): 4 August to 14 September 2017; **Intervention period: 15 September to 26 October 2017
General discussion
Our study shows that the targeted Facebook advertisement increased the uptake of chlamydia self-sampling and the number of positive results in adolescents and young adults. There was a preference for visual platforms, such as Facebook and Instagram, where users can interact with the intervention content. The attractiveness of the advert and its ability to be informative, humorous and encouraging were perceived as important features for young women. The use of animations or videos, and the incorporation of ‘real-life’ actors, were seen as relevant and engaging. Women viewed positive and empowering messages as appealing, and influential in their decision-making. Our intervention, a simple animated text, resulted in a substantial increase in traffic to our chlamydia testing website and test kit requests. Thus, this research demonstrates that the use of social media could supplement the traditional methods of promoting chlamydia screening to young adults.
The findings support previous research showing that social media can be used for sexual health promotion.10,16 Several studies have shown positive effects on outcome; however, only two used advertisement services to disseminate the intervention. In one study, the use of Facebook pages with sexual health content, in particular the signs, symptoms, treatment, screening and prevention of chlamydia infection, showed a 23% increase in condom utilisation and 54% reduction in positive chlamydia cases amongst the intervention viewers compared to non-viewers. 7 Another intervention, ‘Get Yourself Tested’, which used a combination of Facebook and Twitter advertisements with conventional health promotion to encourage chlamydia screening, observed a 743% increase in web traffic and 224 home kit test requests. 17 Although only Facebook advertisement was selected for our intervention, future studies should consider a social media campaign using multiple platforms in parallel for the most optimal effect. In addition, the media provide advertising services allowing health messages to be tailored or targeted to the most ‘at risk’ individuals. As our participants accessed these platforms using mobile phones, the intervention designers need to ensure the optimisation of adverts for geo-positioning technology, 18 to make them able to target individuals in areas or populations most affected by the outbreaks of STIs. Future research should explore the effectiveness of geo-targeting methods using postcodes or areas of higher deprivation in reaching those at risk of infection. As features of the advertisement differ by each platform, additional studies need to identify which of social media platform provides the greatest opportunity for public health interventions in terms of reach and engagement.
The results indicate that sexual health adverts on social media might be more interactive if they incorporate informative messages that are able to increase risk perceptions of STIs, delivered in a humorous and respectful way to overcome the attached stigma. Although the participants acknowledged the aspects of ‘fear arousal’ in digital health promotion, the evidence indicates that perceptions of response effectiveness and self-efficacy are more important than fear appeal; thus, this behaviour change technique should not be considered on its own. 19 Our intervention focussed on personal and empowering messages about individual uniqueness, and the importance of sexual health matters, as per recommendations from previous research. 20 The findings are consistent with the current literature, indicating humour as a preferable strategy for sexual health 11 and general health promotion,21,22 but there is also evidence suggesting that humorous messages regarding sexual health education may influence the likelihood of individuals partaking in unprotected sex. 23 Two previous studies identified the use of humour on social media as a method to reduce concerns and worries about potential bullying from viewing sexual health content.11,24 Future research needs to explore attitudes towards humour in digital health interventions to provide greater clarity on its benefits and potential harms.
In line with previous findings,24,25 our study emphasises the need for anonymity when viewing sexual health adverts. Due to the nature of digital networking, many participants were worried about their privacy and confidentiality. As sexual health is a delicate topic, young people indicated a strong preference to remain anonymous if they were willing to access sexual health content through social media adverts. Intervention designers need to ensure that any traceable information, for example website ‘cookies’, would not be collected in order to prevent the unnecessary promotion of sexual health material from unrelated online advertisers, as that could put users at risk of unintentionally revealing their online interests. Anonymity on social media represents a challenge in promoting sexual health services but remains vital for increasing engagement for targeted advertisement campaigns.
There is a need for multidisciplinary collaboration in the delivery of sexual health interventions online. As more health services now utilise social media, specialist ‘user experience’ experts might be required to identify the forms and contents most effective in engaging with populations of interest. Thus, the knowledge of health psychologists, information technology specialists and marketing advisors is essential to maximise the impact of social media adverts in healthcare. Adverts should be tailored to the needs of specific populations at risk of STIs, such as men who have sex with men, and Black and ethnic minorities, to make them more personal, relevant and persuasive. Intervention developers need to incorporate a patient-centered approach, using qualitative methodologies and ‘A/B testing’ methods, in designing digital sexual health interventions in order to maximise their effectiveness.
Limitations
Several limitations of the present research have been identified. The participant sample used in study 1 consisted of heterosexual women only, as this population is at an increased risk for chlamydia. However, the attitudes towards sexual health communication on social media of men and non-heterosexual individuals may differ. Thus, these variations in views need to be explored in future studies in order to identify the most relevant components for tailored digital health promotion. Furthermore, the qualitative study was conducted by three female psychology students supervised by an experienced qualitative researcher. The thematic analysis was conducted separately to ensure the accuracy, transparency and validity. However, it is unclear whether the saturation levels were reached. The analysis might have been enriched if the project was conducted by experienced researchers able to explore the components of social media interventions in more detail, in particular by seeking views on pre-designed advert templates promoting chlamydia screening.
In study 2, the observed increase in the uptake of chlamydia home-testing kits in the intervention period could also be due to confounding variables, such as seasonal effects or a general increase in the awareness of chlamydia testing amongst Hampshire residents. We identified an overall surge in activity on the sexual health pages during the advertisement period. However, the observed increase in the chlamydia test uptake was atypical, especially as the chlamydia tests have been available online within Hampshire since March 2015. The advert attracted a comparable number of young men and women, and it is unclear whether this was due to individual responses to the advert, based on its attractiveness and persuasiveness, or an algorithm used by Facebook to ensure equal representation of both sexes as set within the advert parameters. Therefore, the designs and effectiveness of future health advertisements should be compared, especially with populations outside of Hampshire and with different demographic characteristics.
It must be acknowledged that Google analytics and other free-to-use analytical tools may not be the most appropriate method of intervention evaluation, 26 as these only provide data on online interactions and engagement. There is a possibility of ‘accidental engagement’ if participants are attracted to the advert for reasons other than chlamydia screening, such as humour. To address such analytical issues, theoretical frameworks for the evaluation of interactive media need to be considered. 27 Future studies need to measure the user's journey from viewing the advert, screening uptake and the testing kit return rate to potential positivity rates and chlamydia treatment, as this would give a more accurate estimate of potential cost-effectiveness. It is also possible that people with higher levels of health literacy and at lower risk of STIs were more likely to engage with social media-based interventions. Thus, research needs to explore if this method could be tailored to the most relevant populations.
Conclusion
Social media platforms provide opportunities to increase uptake of chlamydia screening at relatively low cost. Our findings identify features of sexual health communication on social media and provide evidence that such advertisement is associated with an increase in chlamydia screening uptake. This method could supplement existing methods of promoting STI screening in young adults and may reverse the reported decline in the chlamydia screening uptake. A multidisciplinary and patient-centered approach is required to design adverts that are capable of high engagement. Future studies need to identify how social media and social networking sites could be incorporated into screening programmes, such as the National Chlamydia Screening Programme, while preserving confidentiality and maintaining the trustworthiness of individual sexual health and general practice clinics. Social media platforms offer powerful tools for highly targeted health promotion and they have the potential to significantly increase awareness of STIs, alter negative attitudes towards screening and promote active engagement with sexual health services.
Footnotes
Acknowledgements
We would like to thank Aman Balrow and Lucy Mason for their help with data collection.
Contributorship
TN, OH and KH designed and conducted the study. JB and KH contributed to the analysis. All authors contributed to the interpretation of results and the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the University of Southampton Ethics Committee (ref: 24235) and Solent NHS Trust Clinical Governance (ref: SE-255).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the University of Southampton and Solent NHS Trust.
Guarantor
Dr Tom Nadarzynski.
Peer review
This manuscript was reviewed by two individuals who have chosen to remain anonymous.