
Abstract
Objective
This study employed a participatory design approach to develop a mobile health (mHealth) application tailored for older adults, aiming to promote healthy living and active lifestyles. It addresses key adoption challenges and barriers to sustained engagement in the ageing population.
Methods
Four co-design workshops were conducted in Singapore between February and May 2024 with community and healthcare stakeholders. Participants included 10 middle-aged and older adults (‘current and future older adults’), five healthcare providers, and five community centre staff. These sessions gathered insights and feedback on an initial prototype of the SingaporeWALK (Wearables & Apps in Community Living & Knowledge) app, designed to track physical activity, mental well-being, and dietary habits. Data from usability assessments and stakeholder feedback informed iterative design improvements.
Results
The study identified key user preferences, usability barriers, and engagement strategies essential for designing effective mHealth apps for older adults. Participants emphasised the need for intuitive interfaces, multilingual support, and integrating community-based activities to enhance user experience and engagement. Additionally, participants suggested innovative features such as AI-driven tools to improve accessibility and usability.
Conclusion
The study underscores the importance of user-centric design and stakeholder collaboration in developing effective mHealth solutions for older adults. SingaporeWALK demonstrates the potential of participatory design to address the unique needs of ageing populations, fostering sustained engagement and improving quality of life.
Keywords
Introduction
Mobile health (mHealth), which encompasses health services delivered through mobile devices like smartphones and wearables, has created unprecedented opportunities to provide accessible and convenient healthcare. 1 In 2021, the World Health Organization (WHO) released the Global Strategy on Digital Health 2020–2025, designed to enhance the digital health ecosystem by incorporating tools like mHealth to improve health outcomes worldwide. 2 One of the most pressing areas where mHealth can play a transformative role is in addressing the healthcare needs of the rapidly ageing global population. The proportion of individuals aged 65 and above is projected to nearly double from 9.3% in 2020 to 16% by 2050, representing approximately 1.5 billion people. 3 As older adults face increasing health challenges, mHealth applications offer a strategic solution for promoting healthy ageing and improving healthcare access.
However, despite its potential, mHealth adoption among older adults remains limited due to significant barriers in design, usability, and long-term engagement. Studies have identified several key challenges, including a lack of inclusive design practices, inadequate tailoring of content to older users, and concerns over accessibility and usability. 4 A critical gap exists in the direct involvement of older adults in the design process itself. Addressing these barriers requires innovative approaches that actively involve older adults in the design and development process to ensure mHealth solutions align with their needs and preferences.
This study aims to bridge this gap by employing a participatory design approach to co-develop mHealth applications that promote healthy lifestyles and active ageing. Singapore serves as an ideal case study, given its rapidly ageing society ‒ where 19.1% of the residents are aged 65 and above, 5 and its increasing smartphone adoption among older adults, which rose from 74% in 2017 to 89% in 2022. 6 While this study focuses on Singapore, the findings hold broader implications for ageing societies worldwide, emphasising the potential of participatory design in making mHealth applications more inclusive and effective. By integrating agile development principles, such as continuous feedback loops and iterative design processes, this approach ensures that the final application is not only functional but also relevant and user-friendly, key factors for driving adoption and sustained engagement among older adults.
To investigate these issues, this study co-develops SingaporeWALK (Wearables & Apps in Community Living & Knowledge), a prototype mHealth application designed to promote physical activity and active ageing among older adults in Singapore. 7 The app incorporates user-centred features tailored to older adults, including step tracking, personalised health tips, and interactive community engagement functions. Through a series of co-design workshops with end-users and stakeholders, this study aims to: (a) ensure the mHealth application is aligned with the unique needs of older adults, (b) enhance user engagement and accessibility through user-centric design features, and (c) provide insights into the socio-cultural factors influencing health technology adoption among older adults.
Literature review
The literature review for this research paper explores two key areas relevant to the study: (a) inclusive designing for the ageing population and (b) user engagement and long-term retention strategies for mHealth applications. These areas help structure and guide the development of the mHealth app prototype to ensure usability and sustained adoption among older adults.
Inclusive design for ageing population
The global demographic shift towards an ageing population necessitates the development of digital health tools that are not only accessible but also genuinely usable for older adults. A significant barrier to achieving this is that many mHealth applications fail to account for the multifaceted nature of age-related changes. To systematically address these challenges, Wildenbos et al. proposed the Mobile Health Usability for Older Adults (MOLD-US) framework, which categorises ageing barriers into four key domains: cognition, motivation, physical ability, and perception. 8 This framework provides a valuable lens for understanding the complex interplay of factors that influence older adults’ ability to interact with mHealth technologies.
Within the cognitive domain, age-related changes such as slower information processing speed and reduced working memory capacity can impede the learning of new technologies. 9 Consequently, prevailing design principles advocate for simple, intuitive interfaces with larger fonts, consistent layouts, and step-by-step instructions. 9 This is further supported by checklists for creating health-literate mHealth apps, which offer practical guidance for developers. 10
Age-related decline in psychomotor performance is difficult to quantify due to multiple contributing factors, such as loss of muscle power or common-age illness like Arthritis. This often leads to a decrease in range of motion in joints and increase in variability of finer motor movements. 11 mHealth application design must therefore accommodate decreased range of motion and variability in finer motor movements. 12 Ageing also leads to a decline in physical ability and can be a crucial aspect when considering the implementation of physical elements, such as exergames. Some considerations will include avoiding the use of rapid moving interface elements, and the possibility of playing the game while sitting. 13 In general, instances of exergames with older adults are mostly held using Wii and Kinex platforms, given the ease of use and compatibility with various sensors. 14
A decline in perception functions, particularly vision and hearing, occurs as one ages. Visual abilities that are often impacted includes, the ability to discriminate between colours (violets, blues, and greens), the ability to resolve details, the ability to focus on close objects, and the ability to detect contrast. A usability evaluation done on two health apps for older adults reported significant usability issues due to perception barriers. 15 Researchers recommend that information should be compartmentalised through the usage of bold colours, icons and headings, fonts should be sufficiently large, the usage of distinguishable, non-glaring colours, and the adherence to Web Content Accessibility Guidelines 2.0. 16 Additionally, participants in a recent study expressed appreciation for audible system feedback alongside visual readouts. 17
Apart from sensory perception, it is also crucial to address the mental perception of older adults. A systematic review on 57 telehealth studies on older adults noted that the two most common themes for utilisation barriers of telehealth were technical literacy and lack of desire. 18 These two themes have similarly been highlighted in other literatures as ‘frame-of-mind’ barriers, 19 ‘motivational’ barriers 12 and ‘Psychosocial’ factors. 11 Most of these concerns relate to attitudes toward and perceptions of technology, where older adults are generally less technical literate and coupled with the rapid advancement of technology, the inertia to learn something technical increases. Researchers hence recommend for mHealth apps to provide easy access to help, provide a ‘failure-free’ environment through positive system feedback, and provide sufficient customisation for ease of use. While ease of use significantly influences older adults’ technology acceptance, compatibility with personal goals and lifestyle also plays a major role. 11
User engagement and retention strategies
A key challenge in mHealth applications is maintaining user engagement and retention. It was noted that mHealth apps for older adults often experience low adoption, inconsistent usage, and engagement drop-offs due to ineffective design strategies, complex navigation, and insufficient consideration of age-related limitations. 4
Various studies have proposed strategies for mHealth apps, including reward mechanisms, social interaction features, and gamification.20,21 Motivation remains a significant barrier for older adults in adopting and consistently using technology. Beyond accessibility and ease of use, additional features are required to retain and engage users beyond the initial phase. For instance, a summary report on mHealth applications targeting older adults suggested that rewards are effective in enhancing usage. 20 These incentives can take various forms, such as financial rewards (e.g., grocery vouchers) or performance-based rewards (e.g., congratulatory messages after completing a task). Singapore's Healthy365 initiative exemplifies this approach, demonstrating how incentives can successfully drive participation in health-related digital programs.
In addition to rewards, fostering social interaction has been identified as a key factor in sustaining long-term engagement. Research indicates that older adults are more likely to continue using an app if they perceive a sense of community or shared experience. 22 Features such as virtual support groups, activity challenges, and progress-sharing tools can encourage sustained participation by leveraging social motivation. Furthermore, gamification elements ‒ such as leaderboards, point-based rewards, and progress indicators ‒ can enhance the interactive experience, making health-related activities more engaging and enjoyable. 21
The literature review has provided a greater understanding on the current landscape of mHealth applications, in particular the inclusive designing for ageing population, user engagement and long-term retention strategies, and various design processes for health technologies. It is important to note that many of the available studies on mHealth applications are focused on a specific health condition (e.g., Dementia, Diabetes, etc.) and there are limited studies on a mHealth application that is targeting a larger set of audience, such as older adults in general. Given the increasing intersection of technology and an ageing demographic, it becomes imperative to bridge this literature gap on mHealth applications that aims to promote healthy living and active lifestyle among older adults. Therefore, the following research questions were formulated:
RQ1: How can participatory design approaches be effectively utilised to develop mHealth apps that promote healthy living and active lifestyles among older adults? RQ2: What are the key design features and processes that enhance user engagement and adoption of mHealth applications among older adults?
Following the formulation of the research questions, we acknowledge that the initial development of the app prototype was grounded in the designers’ and researchers’ assumptions, emphasising the necessity for further refinement and enhancement. To ensure the app's design aligns with the actual needs and preferences of the target audience, we conducted co-design workshops involving older adults, healthcare providers, and community centre staff. Through the implementation of the co-design approach, the study aims to review the benefits and effectiveness of this collaborative process in developing mHealth app for older adults, addressing RQ1. Moreover, reviewing the resulting key design features and processes from this collaboration will provide insights into how user engagement and adoption can be enhanced, hence addressing RQ2.
Methods
Study design
In this study, we employed a qualitative participatory design approach to co-develop the SingaporeWALK mHealth application. The study was conducted in Singapore between February and May 2024 across multiple community and healthcare settings, including St Luke's ElderCare Golden Years Centre, REACH Community Services @ Bukit Batok, and Tan Tock Seng Hospital. We held four co-design workshops (three in English, one in Chinese) with 20 participants: 10 older adults aged 50–76, five healthcare providers (one nurse and four health coaches), and five community centre staff. This age range included middle-aged adults approaching seniorhood and older adults, ensuring the app's relevance for healthy ageing across transitional life stages. Each workshop incorporated: (a) focus group discussions to gather user insights, (b) feature ideation to propose app improvements, (c) prototype testing for hands-on evaluation, and (d) usability testing to assess functionality and ease of use. This participatory approach facilitated iterative feedback, enhancing the app's usability and relevance. Through this process, we addressed: (RQ1) the effectiveness of co-design in developing mHealth applications for older adults, and (RQ2) key design features that promote engagement and adoption.
Participants engaged with the SingaporeWALK prototype, designed to promote healthy living among older adults through physical activity, nutrition tracking, and mental well-being features. We used open-ended questions in discussions to explore usability, content, and features, complemented by closed-ended questions in a structured online survey for usability assessment (Figure 1). This approach aligns with the say-do-make model, 23 which extends traditional design methods by incorporating user-created solutions. Unlike conventional approaches that focus solely on what users say and do, we integrated a user innovation board where participants recorded pain points and proposed mHealth improvements on a 31-inch mahjong paper roll. This provided a tangible reference for iterative design refinements.

Co-design workshop structure.
Data analysis
We conducted an inductive thematic analysis of the co-design workshop transcripts, following Braun and Clarke's six-phase framework. 24 All audio recordings were transcribed verbatim and carefully checked for accuracy against the audio files. The analytic process proceeded through several iterative stages. First, two coders immersed themselves in the data by reading the transcripts multiple times to achieve familiarity. They then performed line-by-line open coding, identifying meaningful text segments and assigning descriptive labels. These codes were systematically organised into a colour-coded coding matrix in Microsoft Excel, which allowed for comparisons across participants and workshops. Following this, codes were grouped into provisional categories that captured patterns within the data. Through repeated refinement, categories were then consolidated into broader, higher-order themes that reflected participants’ shared perspectives and unique experiences. Discrepancies in coding were reviewed in regular consensus meetings, during which coders discussed divergent interpretations until agreement was reached. All revisions and decisions were documented in an audit trail to ensure transparency of the analytic process. A third researcher, independent from the coding process, subsequently reviewed the final set of themes and illustrative quotations to ensure they were coherent, internally consistent, and accurately represented the data.
SingaporeWALK app
SingaporeWALK is a mHealth application to promote physical activity, nutrition tracking, and mental well-being for older adults. Currently in its prototype phase, the app includes three main components: (a) exercise module – Interactive exergames and guided exercises designed to target various muscle groups for enjoyable physical activity; (b) nutrition module – tracks meals, water, and milk intake, providing insights and recommendations for healthier dietary habits; (c) well-being assessment module – a questionnaire-based feature that evaluates psychological, social, and emotional well-being, offering tools for self-reflection and mental health resources. Developers built the app using Flutter, a cross-platform framework that supports rapid iteration and testing within a Dart-based codebase.
Usability assessment
Numerous usability tests and evaluations exist for mobile applications. With the rise of mHealth, the Mobile App Rating Scale (MARS) was introduced as a targeted evaluation tool specifically for health mobile apps. 25 However, MARS requires evaluators to have in-depth familiarity with the app's functionalities, typically achieved through structured training exercises. 26 This makes it less suitable for older adults participating in co-design workshops. To address this challenge, we adapted a usability evaluation framework proposed by Arnhold et al., 27 originally designed for expert evaluations of mobile apps for older adults. This framework is based on ISO and DIN usability standards and includes criteria relevant for older users, such as interaction processes, interface design, and content comprehensibility. It was systematically developed and tested with expert evaluators to ensure standardisation and relevance for older populations. For this study, we created a simplified, participant-facing version of the questionnaire. We developed questions corresponding to the main subcriteria, grouped into three sections: Ease of Use, Presentation, and Comprehensibility. Each question utilised a 5-point Likert scale. 28 This adaptation aimed to maintain the framework's structure while ensuring usability for older adult participants in co-design workshops (Table 1).
mHealth application usability rating criterion adapted from Arnhold et al. (2014).

Results
Findings from the co-design workshops with older adults, healthcare providers, and community staff are presented in four thematic areas: (a) stakeholder perspectives on participatory design, (b) user preferences and needs, (c) key design elements, and (d) prototype evaluation and usability testing. Together, these results demonstrate how participatory design shaped the SingaporeWALK prototype and identified critical success factors for engagement and adoption.
Stakeholder perspectives on participatory design
The participatory design process enabled participants to share experiences with existing mHealth apps and propose improvements. Engaging multiple stakeholders was essential to capturing the broad spectrum of needs and challenges related to mHealth usage among older adults. Healthcare providers emphasised the clinical value of integrating app-generated health data into patient care, while community staff underscored the importance of social engagement features to support sustained use. Older adults contributed detailed feedback on accessibility barriers, particularly concerning interface navigation and content complexity.
The workshops also generated innovative ideas not yet widely available in existing apps. These included: (a) AI-powered nutrition tracking using computer vision to streamline food logging; (b) enhanced accessibility tools, such as video guides; and (c) simplified navigation systems tailored for low digital literacy. These suggestions reflected both unmet needs and opportunities to expand app usability and functionality.
Balancing diverse stakeholder needs was a key challenge. Healthcare workers favoured detailed graphical displays of mental health data to support continuous monitoring, whereas older adults preferred simpler, more intuitive interfaces, reporting that multiple graphs and numeric values felt overwhelming. The iterative design process allowed the team to reconcile these perspectives, ensuring that both clinical requirements and user-friendly design principles were addressed. This balance demonstrated the utility of participatory design in producing solutions responsive to both professional and end-user needs.
User preferences and needs
The initial component of co-design workshops involved insights gathering through focus group discussions. These explored participants’ prior experiences with mHealth apps, motivational drivers, and usability barriers.
Most participants were aware of mHealth apps, with Healthy365 and HealthHub being most frequently mentioned. Older adults who utilised HealthHub for scheduling medical appointments found the process straightforward, particularly those proficient in English. The Healthy365 app was commonly used for exercise-related activities such as step tracking and health challenges. Despite its popularity, some older adults found navigating the interface difficult, especially those less familiar with technology. Healthcare workers and community staff substantiated these findings, providing additional insights into older adults’ experiences with mHealth applications. Healthcare workers highlighted that older adults prefer in-person visits due to familiarity and personalised assistance. This preference stems from a sense of security and trust in face-to-face interactions, which are perceived as more reliable for healthcare needs. Many older adults also expressed apprehension towards adopting telehealth technologies, citing concerns about their ability to effectively use digital platforms independently, and the threat of online scams.
A strong motivational driver for using mHealth apps among older adults was the availability of incentives, such as vouchers and rewards. These incentives were highly effective in encouraging engagement with health-promoting activities and applications; however, when asked if they would continue participating without incentives, most older adults expressed diminished interest. One participant noted that despite available rewards for sleep tracking in Healthy365, she opted not to engage with the feature due to discomfort. This finding underscores the limitations of extrinsic motivation, where usability concerns and personal comfort can outweigh financial incentives, highlighting the need for intrinsically motivating features prioritising user comfort and ease of use. Importantly, grocery vouchers and similar rewards were mentioned only as examples of existing national programmes (e.g., Healthy365) cited by participants; the SingaporeWALK prototype itself does not include any incentive model.
Healthcare workers and community staff identified additional motivational drivers for effective mHealth adoption among older adults. One approach involved bridging the digital divide by incorporating digital features into real-life activities. For instance, community staff shared a successful initiative hosting Zoom calls for health coaching sessions with older adults at Active Aging Centres. This approach received enthusiastic responses because it allowed technology engagement in a supportive environment, without the complexities of independent setup. These sessions not only facilitated learning about health and wellness through digital platforms but also provided a sense of community and social connection among participants.
As revealed through the discussions, older adults who were not proficient in English faced significant challenges when using these apps, highlighting a critical barrier to accessibility and usability. One older adult remarked: I understand English, but some of my peers do not, and this means that they can't use the apps that are in English.
This language barrier often resulted in frustration and reduced the likelihood of these older adults engaging with the technology. Concerns were raised about the font size and readability of app content, as well as the length and complexity of questionnaires and instructions, which can deter users from fully engaging with app features.
Participants identified the need for better integration and synchronisation of mHealth applications with existing healthcare systems, including both public health clusters and private GP clinics. Many users expressed confusion between multiple apps offered by different health clusters and for different purposes. One participant articulated: One simple app, you don't need to have so many apps. This one app, you can book your activities, medical appointments, your health metrics, teleconsultation, everything you want in the app.
They preferred to have multiple functions, such as making medical appointments, booking for exercise and wellness classes, steps tracking and more, all within an app. The lower technology literacy prevalent among older adults, do indeed pose challenges in navigating complex app interfaces and understanding technological processes. However, healthcare workers and community staff noted progress in the technological literacy of older adults. Community staff have observed a growing segment of ‘future older adults’, who are increasingly receptive to technological solutions, and can utilise mHealth apps to a larger extent. This demographic shift underscores the increasing importance of mHealth applications in supporting the health and well-being of older adults, especially in the near future.
Key design elements
To address RQ2 regarding design features and processes that enhance user engagement and adoption, the second phase of co-design workshops focused on feature ideation. Participants collaboratively brainstormed and proposed new features for mHealth applications, documenting ideas on large roll paper (31" mahjong paper). This phase systematically identified key design elements that could improve user engagement and adoption rates among older adults. The analysis revealed four critical design categories that significantly influence user engagement:
Accessibility and usability tools
Participants suggested that apps should have the inclusion of voice text, read-out-loud texts, and the ability to enlarge the content. Furthermore, within the different pages in the app should have video guides that give step-by-step tutorial on that specific page.
AI nutrition tracker
Current mHealth applications that have the function for nutrition tracking often requires user to input the food manually for meal logs. However, these apps may not have a comprehensive database of food items, necessitating users to log their meals based on multiple components. This manual input process can be tedious and inconvenient for users. Participants hence suggested to incorporate Artificial Intelligence elements into recognising the food based on a picture, which would then streamline the process of manual meal logs.
Comprehensive all-in-one app
Participants noted that current health apps typically serve single purposes, such as booking of medical appointments or tracking health metrics. It was proposed that these functions can be consolidated into an app, allowing for seamless synchronisation of health-related data. Healthcare workers also opine that the synchronisation of health-related data could prove to be very useful for doctors and healthcare staff to understand the patient's health status and history.
In-app social chat groups
Some of the participants using the Healthy365 app encounter issues with relying on external WhatsApp groups for updates regarding exercise and wellness classes. These groups are used to disseminate information, such as changes to the venue, timing, or activities. Participants who are unaware of these chat groups may miss out on important updates despite having signed up for the classes. It was hence suggested for chat groups to be integrated within the app. This functionality could also further extend to include community chat groups where users can stay connected and engaged beyond just class updates.
Prototype evaluation and usability testing
Physical activity and movement data
In this section, participants were introduced to exergames ‒ interactive games that requires the user to produce physical body movements to play. The app features three different games, each targeting specific body movements. It was explained to participants that these games would require the wearing of sensors to monitor the movements, and the game would primarily be played through the phone screen (Figure 2).

SingaporeWALK interface – activity and movement page.
Most participants were unfamiliar with exergames but are receptive to trying it out if given a chance. The idea of exercising through video games received positive interest, with participants expressing a preference for competitive elements. One participant noted: The games sound fun, but I would prefer a bigger screen or a way to play together.
Another participant emphasised the importance of social interaction during gameplay: The social aspect is quite important in these types of games because let's say if I am alone at home, the motivation to actually play will be lower.
Alternatives suggested includes casting the game onto a larger screen, such as a smart television at home, or conducting the game at community centres, where older adults can play the games on a bigger screen and without the hassle of setting up the equipment. Some participants also expressed their preference for playing the games in a social setting as it allows for more social interaction and competitive elements.
Mental well-being
In the next section, a mental well-being questionnaire was introduced. This questionnaire consists of 14 questions, based on the Mental Health Continuum-Short Form (MHC-SF), a validated instrument with confirmed internal consistency and construct validity across emotional, social, and psychological well-being domains. 29 Participants were invited to take the questionnaire and share their opinions afterwards (Figure 3).

SingaporeWALK interface – mental well-being page.
For most participants, this was their first time completing a self-report questionnaire for mental well-being. They recognised that such an addition would be beneficial for monitoring and self-evaluating their mental health. However, several concerns emerged regarding questionnaire frequency, repetitiveness of questions, and difficulty understanding response options. Addressing these concerns, participants suggested shorter questionnaires with simpler vocabulary to improve accessibility for older users. They also recommended incorporating visual aids, such as numeric scales or slider scales with expressive icons, to enhance clarity and ease of use. Healthcare workers emphasised the need for actionable follow-up steps after questionnaire completion, suggesting that recommendations and resources based on results should be provided to ensure practical benefits for users.
Dietary and nutrition
In the last section for nutrition tracking, participants are introduced to the app interface, which includes simple buttons to add water, milk, and meal intakes into the nutrition log (Figure 4).
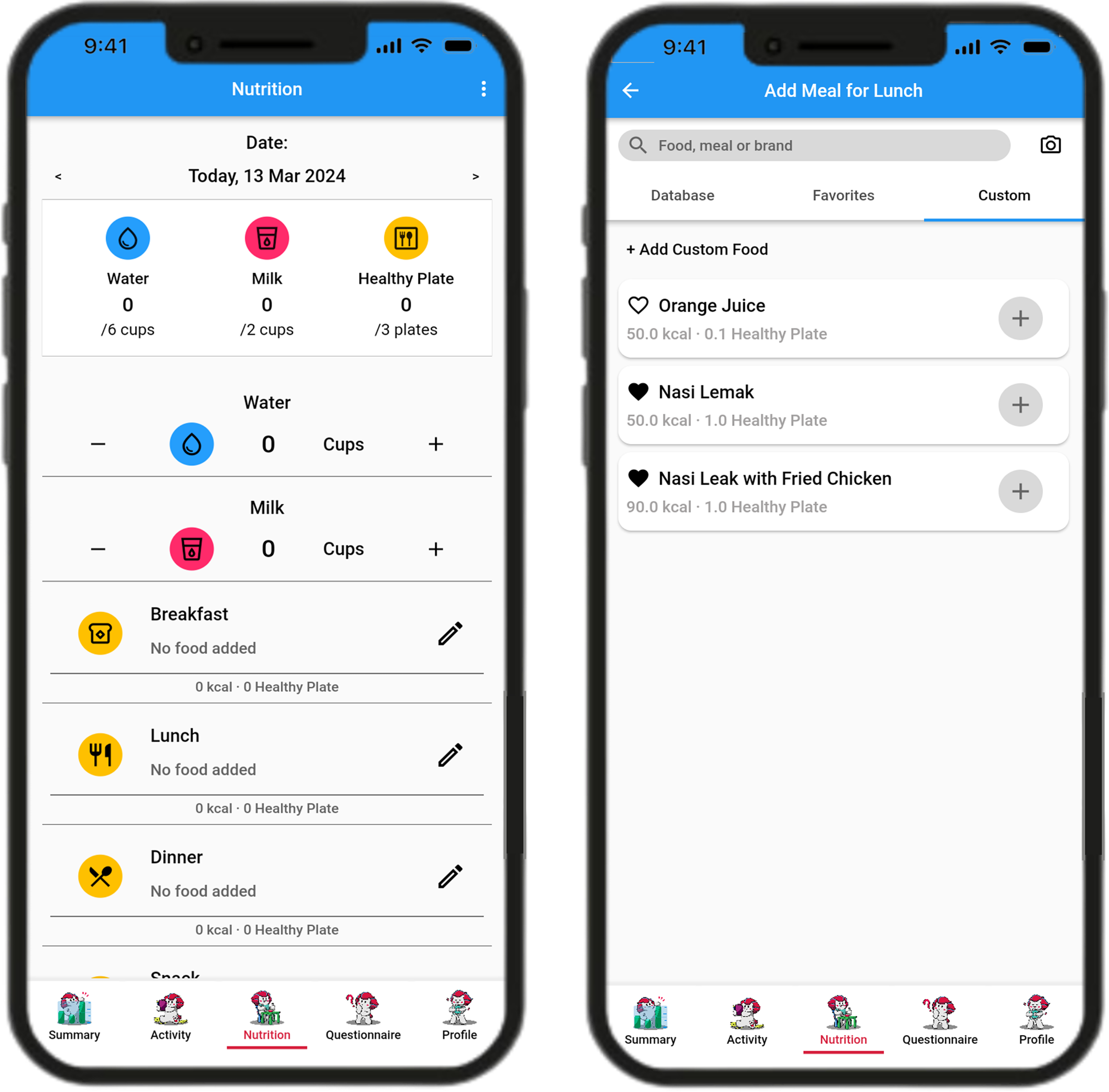
SingaporeWALK interface – nutrition page.
Although participants were familiar with meal-logging features in apps like Healthy365, none reported logging meals daily. Participants cited a lack of incentives and motivation as a primary barrier. Without clear benefits or rewards, they felt less inclined to make the effort to log their meals regularly. Furthermore, one participant expressed: I tried to use the meal log function, but I often find that the food item I consumed is not in the database, and they require manual logging in which is tedious, and I do not know the nutrition content either.
The limited database of food and drinks available in the app, often required them to manually input meal components. This process was considered tedious and time-consuming, further discouraging regular use.
At the end of the app testing, participants completed a modified usability scale that assessed ease of use, presentation, and comprehensibility on a 5-point Likert scale. Overall, the app was perceived as reasonably intuitive. Ease of use received the highest average score (3.78/5), with participants highlighting the clarity of signposting and section headers, which helped them navigate different functions with minimal confusion. Figure 5 illustrates the average scores across the three usability dimensions.
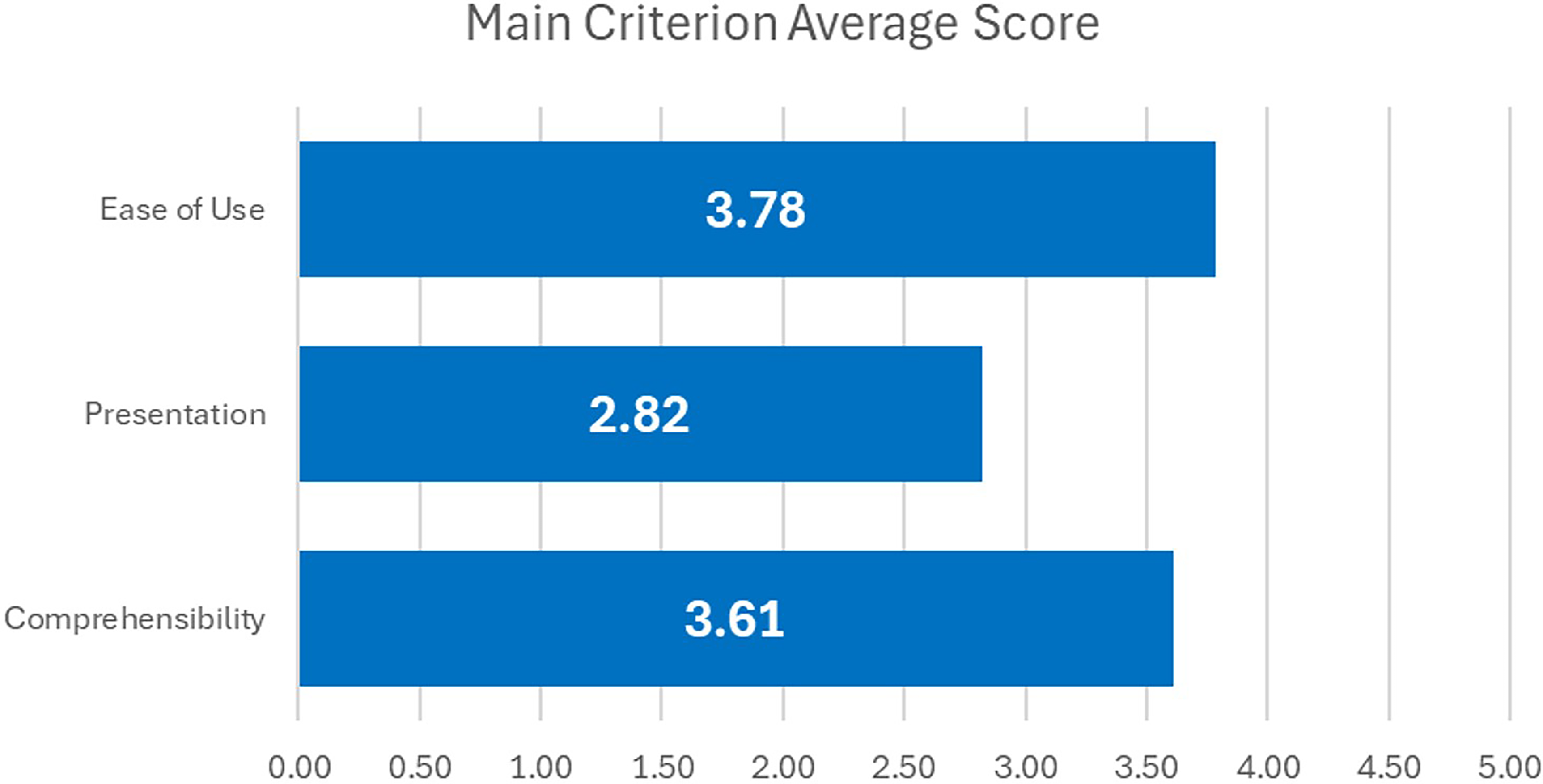
Average scores for usability assessment (5-point Likert scale).
In contrast, presentation was rated lowest (2.82/5). Participants expressed dissatisfaction with the small icon and text sizes as well as the colour scheme, noting that the current palette of bright orange, yellow, and green against a white background was difficult to read. They recommended larger buttons to reduce accidental clicks and improved colour contrast to enhance visibility. These concerns are exemplified in Figure 6, which shows the current presentation of icons, text, and colour contrasts within the app interface.

SingaporeWALK interface – welcome page.
Comprehensibility achieved a mean score of 3.61/5, suggesting that participants generally understood the app's features, terminology, and navigation labels. However, some noted that the phrasing of questionnaire items in the Chinese version was overly long, which risked reducing engagement and comprehension among older users.
Discussion
This study demonstrates the value of participatory design in developing mHealth applications for older adults, while also extending existing knowledge in several important ways. First, it shows how a multi-stakeholder co-design process ‒ bringing together older adults, healthcare providers, and community staff ‒ can reconcile diverse and sometimes competing needs. Through this process, design features emerged that balance clinical utility (e.g., detailed health data for professionals) with user-friendliness (e.g., simplified interfaces for older adults), offering a replicable model for inclusive digital health innovation. Second, the study provides new insights into older adults’ motivational dynamics in mHealth adoption. While incentives remain a strong driver of initial engagement, sustained use was found to depend more on intrinsic motivators such as social connection, usability comfort, and integration into community-based activities. These findings clarify how participatory design can surface and address motivational tensions that are often overlooked in conventional user-centered design (UCD). Finally, while grounded in Singapore, the findings highlight the opportunities and challenges of developing mHealth solutions in a rapidly ageing yet digitally advanced society, where strong national health initiatives and growing digital literacy among older adults create fertile conditions for scalable innovation.
Participatory design effectiveness and user insights
Our findings from the focus group discussions demonstrate that tangible incentives, such as grocery vouchers and redeemable points, act as powerful motivators for initial app engagement among older adults. This aligns with Li et al.'s emphasis on reward mechanisms in mHealth adoption. 20 Singapore's National Steps Challenge illustrates how incentives, when paired with wearables, can successfully promote physical activity. However, echoing Harrington et al., 4 our results highlight that sustainable engagement requires more than incentives alone, and must be supported by fundamental improvements in usability and accessibility. Beyond rewards, participants emphasised the importance of gamification and social interaction for long-term retention. Features such as competitive elements, group challenges, and peer support were consistently described as appealing. These preferences resonate with Uchino et al.'s work, 30 which underscores the health-promoting role of social interactions. Our findings extend this literature by showing that for older adults, social connection is not simply a secondary driver but a foundational determinant of both app retention and health outcomes.
Participants also identified language barriers and interface complexity as major usability challenges, particularly for non-English speakers. These findings validate the MOLD-US framework, which highlights cognition, motivation, physical ability, and perception as critical barriers to mHealth adoption. 8 Empirical evidence from our study reinforces this framework: participants stressed the need for simplified language, larger fonts, and intuitive navigation. Crucially, our findings position usability not merely as a technical consideration but as a core determinant of sustained engagement, underscoring the importance of accessibility-driven design.
The integration of AI-enhanced features, particularly the proposed AI nutrition tracker, received strong positive feedback. This aligns with recent reviews of AI-enabled mHealth models, 31 suggesting that automation of complex tasks such as meal logging can address age-related declines in motor skills. 12 Participants’ preference for an all-in-one app that consolidates multiple health functions further reinforces prior findings on older adults’ desire for integrated, easily navigable platforms. 32 Consolidation not only enhances user experience but also reduces cognitive load, increasing the likelihood of sustained adoption.
Finally, the co-design workshops directly shaped the SingaporeWALK prototype. Participants’ calls for simplified navigation, clearer visual elements, and AI-driven functionalities were integrated into iterative refinements. This iterative process exemplifies how participatory design moves beyond conventional user feedback, embedding end-user perspectives throughout development. Consistent with prior studies, 33 our findings affirm that a human-centered, participatory approach improves usability and accessibility when older adults’ lived experiences are systematically incorporated into design decisions.
Theoretical implementations
This study contributes to the theoretical advancement of inclusive digital health design by showing how participatory co-design can operationalise established frameworks in real-world mHealth development for older adults. Specifically, our findings demonstrate how the MOLD-US framework, 8 UCD methodology, 34 and usability evaluation tools24,26 can be extended through iterative, user-informed design practices.
Cognitive barriers were evident in participants’ reports of information overload, complex navigation, and memory-dependent tasks. Their preference for simplified interfaces and step-by-step guides directly addresses these challenges. Motivational factors also revealed a nuanced dynamic: while extrinsic motivators such as vouchers and rewards triggered initial use, intrinsic motivators ‒ including social connection and usability comfort ‒ proved more influential in sustaining long-term engagement. This echoes broader motivational theory, which suggests that external rewards may initiate behaviour but intrinsic factors determine persistence.
Physical ability constraints, particularly among participants with motor limitations, shaped preferences for large buttons, voice input, and minimal fine-motor requirements. These preferences corroborate MOLD-US recommendations for accessible interaction design. Perceptual barriers, such as reduced vision and contrast sensitivity, were also prominent, reinforcing the importance of high-contrast displays, adjustable font sizes, and auditory feedback.
Our findings extend MOLD-US by demonstrating how participatory design can actively mitigate cognitive and perceptual barriers through iterative co-creation. Unlike prior studies that applied MOLD-US primarily as a diagnostic tool, this study positions it as a practical design guide, integrated into real-time development. Furthermore, our participatory approach draws on UCD principles 35 but extends them by actively positioning older adults as co-creators rather than passive recipients. This directly challenges dominant technology design narratives that marginalise ageing populations. By involving older adults in co-design workshops and usability testing, our study illustrates that granting agency to older users produces technologies that better reflect their lived realities.
Finally, the adoption of a usability assessment framework ‒ combining the MARS scale 24 with adaptations tailored to older adults 26 ‒ illustrates how social science theories of accessibility and inclusion can be operationalised in digital health. By pairing quantitative metrics with qualitative feedback, we achieved a richer understanding of how older adults interact with mHealth applications. The focus on reducing cognitive load and enhancing visual clarity aligns with accessibility theories aimed at supporting users facing social and technological disadvantage. In doing so, this work addresses broader societal concerns around the digital health divide and the exclusion of older adults from innovation spaces. 36
Practical implementations
The findings have several implications for developers, healthcare providers, and policymakers. Developers should prioritise intuitive interfaces, simplified navigation, larger fonts, and minimal steps for task completion to address common barriers. Integrating automated features such as AI-driven nutrition tracking can reduce cognitive load and support users with motor or cognitive limitations. Embedding social interaction functions including group challenges and peer support can foster community and enhance sustained engagement.
Healthcare providers can support adoption by recommending mHealth apps as part of routine care, integrating them into treatment plans, and offering training to older adults who face digital barriers. Policymakers, meanwhile, can strengthen adoption ecosystems by funding app development tailored for older adults, providing subsidies for devices, and supporting digital literacy programmes.
Taken together, these contributions extend prior work on UCD by demonstrating how culturally grounded, multi-stakeholder approaches can enhance inclusivity, usability, and long-term engagement. While developed in Singapore, the model is transferable to other rapidly ageing societies, offering a replicable framework for participatory co-design that balances cultural specificity with globally relevant lessons for digital health innovation.
Limitations
This study's primary limitation lies in its relatively small sample size of 10 older adults, 5 healthcare providers, and 5 community centre staff. While providing valuable insights, this modest sample limits the generalisability of findings to broader populations. A second limitation concerns participant characteristics. Most participants were smartphone users with existing technological literacy and were recruited from community programmes and health check-ups. They therefore represented a relatively health-engaged and digitally literate group, which may have made them more receptive to the app's design features and contributed to more favourable usability feedback. As a result, barriers experienced by less health-engaged, less technologically confident, or harder-to-reach older adults may have been underrepresented. Nonetheless, this profile reflects an increasingly important demographic of digitally savvy older adults, whose perspectives are valuable for anticipating future patterns of mHealth adoption. To address this limitation, future research should recruit larger and more diverse participant groups, including those with lower digital literacy or health engagement, to enhance inclusivity and generalisability.
Finally, time constraints limited the iterative design process to a single round of testing and refinement of the SingaporeWALK prototype. A more comprehensive iterative process ‒ entailing multiple cycles of user feedback, testing, and refinement ‒ would likely yield more substantial usability improvements. These findings should therefore be considered preliminary, underscoring the need for further iterations to fully realise the potential of the co-design approach.
Future directions
Building on the current findings, we plan to conduct additional co-design cycles to further refine SingaporeWALK by integrating stakeholder feedback. These cycles will involve a broader and more diverse participant pool, including individuals with varying levels of digital literacy and health engagement, to strengthen inclusivity and generalisability. Following refinement, expanded usability testing will be conducted in both Singapore and Hong Kong. This cross-cultural evaluation will provide insights into the app's effectiveness across different ageing populations and healthcare contexts, offering stronger evidence for the scalability of participatory design approaches in mHealth.
In the longer term, longitudinal studies are needed to evaluate the durability of engagement strategies such as rewards, gamification, and social interaction features, and to examine their effects on physical activity, mental well-being, and broader health outcomes. Such studies will be essential for establishing the effectiveness of SingaporeWALK as a scalable intervention for healthy ageing. Finally, future research should explore the integration of emerging technologies such as Artificial Intelligence and Virtual Reality. AI-driven features, including personalised health recommendations, predictive analytics, and adaptive interfaces, may substantially improve accessibility and usability for older users, while Virtual Reality holds promise for fostering social engagement and immersive health promotion.
Conclusion
This study offers critical insights and practical strategies for designing mHealth applications tailored to the needs of older adults. Through participatory design workshops involving older adults, healthcare providers, and community centre staff, we identified key user preferences, usability barriers, and engagement drivers specific to this demographic. The findings underscore the importance of intuitive interfaces, multilingual support, and community-based features in enhancing usability and fostering sustained engagement.
The study's significance lies in demonstrating the value of a participatory, multi-stakeholder approach within the Singapore context, where digitally savvy older adults and strong national health initiatives create favourable conditions for scalable digital health solutions. By addressing challenges such as technological literacy and interface complexity, our work advances knowledge on inclusive mHealth development for ageing populations.
Looking ahead, these findings will guide further co-design cycles and expanded usability testing in Singapore and Hong Kong, laying the foundation for cross-cultural applications. Ultimately, this study highlights the potential of inclusive, user-centred design to produce accessible, engaging, and effective mHealth solutions that support active ageing both locally and globally.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251390573 - Supplemental material for Co-developing SingaporeWALK mobile health app: Enhancing physical health and mental well-being among current and future older adults through inclusive technology
Supplemental material, sj-docx-1-dhj-10.1177_20552076251390573 for Co-developing SingaporeWALK mobile health app: Enhancing physical health and mental well-being among current and future older adults through inclusive technology by Kit Ho Chan, Ling En Oh, Huanyu Bao and Edmund Wei Jian Lee in DIGITAL HEALTH
Footnotes
Acknowledgments
We extend our sincere gratitude to FullHealth for their support in facilitating participant recruitment, St Luke's ElderCare Golden Years Centre, REACH Community Services @ Bukit Batok, and Tan Tock Seng Hospital for providing facilities for the workshops. We are especially thankful to the community members, including older adults, healthcare providers, and community services staff, who actively participated and contributed to the workshops. Additionally, we would also like to acknowledge Dr Yichi Zhang for her invaluable guidance in laying the foundational framework for the workshops through her previous research project.
Ethical approval
This study was approved by the Nanyang Technological University, Singapore, Institutional Review Board (IRB) under protocol number IRB-2022-945, with the latest approval granted on 27 February 2024.
Consent to participate
All participants obtained explicit written informed consent through a digitally signed consent form prior to participation in the study. The procedure was reviewed and approved by the Nanyang Technological University Review Board.
Consent for publication
Not applicable, as no identifying personal data, images, or videos of participants are included in this manuscript. All tools, frameworks, and questionnaires used in this study are derived from previously published and validated sources in the literature. Since these materials are widely available for academic use (e.g., standardised psychological scales or items) and do not require explicit permission from copyright holders for research purposes, no additional permissions were sought. Proper citations for all sources have been provided in the manuscript.
Author contributions
Chan Kit Ho served as the lead author, overseeing project conceptualisation, guiding the data collection and drafting the manuscript. Oh Ling En contributed to data collection and analysis. Huanyu Bao provided expertise in formulating search strings with library resources, offered intellectual input, and contributed to the editing of the manuscript, as well as coordinating various aspects of the project. Edmund Lee, as the Principal Investigator, provided overall guidance on project conceptualisation, data collection and manuscript writing.
Funding
This work was supported by the Ministry of Education (MOE) in Singapore under the Social Science and Humanities Fellowship (SSRC2022-SSHR-006), and the National Research Foundation, Prime Minister's Office, Singapore, through its Campus for Research Excellence and Technological Enterprise (CREATE) programme, via the Intra-CREATE Seed Collaboration Grant (NRF2021-ITS009-0012). We would also like to acknowledge that the publication of this research is supported by the Strategic Seed Fund from the City University of Hong Kong (Project number: 7020115).
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Please contact the corresponding author Dr Edmund W. J. Lee regarding data availability.
Research transparency statement
In the interest of academic transparency and research integrity, we wish to inform you that we have a separate paper on the SingaporeWALK app currently under review at another journal. The present manuscript specifically focuses on the co-design methodology and participatory development process, utilising data from 20 participants to examine UCD principles related to the SingaporeWALK app. In contrast, the separate paper under review involves a different study population (n = 48) and addresses the technical implementation and evaluation outcomes of the app. These two studies have distinct research questions, methodological approaches, and datasets, exploring different aspects of the design and implementation of the SingaporeWALK app. We aim to maintain full transparency in our research process, and we want to explicitly notify the journal editors about these two separate papers concerning SingaporeWALK.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.