
Abstract
Background
The utilization of mobile health (mHealth) devices such as nutrition and fitness tools seems to be promising in facilitating healthy lifestyle behaviors in middle-aged and older adults. As user acceptance plays a decisive role in the successful implementation of mHealth tools, it is vital to examine the target groups’ acceptance, particularly their usage behavior and attitudes toward these tools. This qualitative study aimed to explore how far middle-aged as well as older adults accept mobile nutrition and fitness tools and to identify facilitators and barriers shaping their acceptance.
Methods
Twenty-one qualitative semi-structured interviews were conducted with German adults aged 50 years and older. Data material was analyzed using Qualitative Content Analysis (Kuckartz).
Results
A comprehensive acceptance typology with three acceptance types could be reconstructed: The Rejection Type, The Selective Acceptance Type, and The Comprehensive Acceptance Type. The target group's acceptance of mobile nutrition and fitness tools appeared to differ considerably across the three acceptance types and between the two different types of mHealth tools – with mobile nutrition tools having been less accepted. Among others, high levels of usability were identified as a key facilitator, while a desire for autonomy and privacy concerns showed to be prominent barriers.
Conclusion
The resulting typology indicates a pronounced heterogeneity among middle-aged and older adults regarding their acceptance of mobile nutrition and fitness tools. The findings highlight a need for more individualized mHealth tools along with respective promotion strategies that are specifically tailored to the needs and expectations of middle-aged and older adults.
Keywords
Introduction
Older age constitutes a major risk factor for the development of chronic noncommunicable diseases which are associated with an increase in morbidity and mortality rates.1,2 Previous research has provided strong evidence for links between diverse unhealthy lifestyle behaviors and the development of chronic diseases: For instance, unfavorable dietary patterns (e.g., including high amounts of red meat, insufficient fruit, and vegetable intake), as well as physical inactivity, foster the development of cancer, and cardiovascular diseases.3–6
Positive lifestyle changes involving a reduction of those risk factors have been demonstrated to decrease the risk of developing chronic illnesses as well as improving individuals’ overall health status and quality of life. 7 Such positive lifestyle changes can also benefit health outcomes if initiated in middle and old(er) age. 8 In this context, previous research has highlighted the transition from the occupational phase to retirement as an opportunity for (the initiation of) change toward such healthier lifestyle behaviors.9,10 Thus, the so-called peri-retirement phase, respectively the age span from 50 years and older, is of specific research interest for investigations with the aim of supporting public health promotion.
So far, various approaches for the promotion of healthy lifestyles among adults of middle and older age have been examined. Mobile health (mHealth) tools have shown potential to effectively promote healthy lifestyle behaviors such as maintaining a favorable diet 11,12 and high physical activity levels.13,14 The potential of mHealth tools essentially depends on the target groups’ usage behavior, with user acceptance playing a decisive role. Definitions of technology (e.g., mHealth) acceptance differ widely across disciplines as well as with respect to the cultural context. 15 Internationally, the most prominent definitions are the Unified Theory of Acceptance and Use of Technology (UTAUT 1 & 2)16,17 as well as the Technology Acceptance Model (TAM). 18 Despite the existing conceptual variance, there appears to be broad consensus on various dimensions conjointly shaping users’ technology acceptance: among those are actual usage (e.g., usage frequency, length of use), user experiences (e.g., perceived usefulness, perceived ease of use) as well as attitudes (e.g., privacy concerns) toward technological respectively digital tools.15,19
There is a relatively large body of research on the acceptance of mobile health applications focusing on populations at large.20–22 With respect to the population of middle-aged and older adults, previous research has identified facilitators and barriers regarding the usage of general mHealth technology: on the one hand, motivation and support (e.g., from other mHealth users), as well as a high level of usability (e.g., ease of use) depict central facilitating factors. 23 On the other hand, a lack of motivation, high time expenditure, and difficulties in handling technical devices are among the most prominent barriers toward mHealth technology use. 23
Despite this evidence, research on middle-aged as well as older people's acceptance that specifically addresses mobile nutrition and fitness tools indicates a (significantly) lower acceptance of middle-aged and older adults in comparison to younger populations. 24 This was reflected, among others, in lower usage frequencies, more negative attitudes toward technological devices as well as diverse barriers (e.g., related to the ease of use). However, the existing body of knowledge regarding nutrition and fitness app acceptance was shown to be rather scarce and thus remains tenuous. 24 More specifically, studies particularly exploring the target group's usage behavior, attitudes toward and expectations of these tools as well as facilitators and barriers shaping their acceptance are yet missing.
In order to draw sound conclusions for the future development of effective mobile nutrition and fitness tools tailored to the specific needs and resources of middle-aged and older adults, a more comprehensive in-depth understanding of the target group's acceptance is required. Against this background, this qualitative study aimed to explore how far middle-aged and older adults accept mobile nutrition and/or fitness tools. In addition to inductively exploring various acceptance characteristics, we thereby sought to understand the actual usage behavior of and attitudes toward such tools as well as to identify associated facilitating and hindering factors.
Methods
Under the umbrella of the German Competence Cluster Nutriact – Nutritional Intervention: Food Patterns, Behavior, and Products, a qualitative, cross-sectional study was carried out from 2018 to 2020. Ethical approval was granted by the Ethical committee of the Charité – Universitätsmedizin Berlin (EA4/151/16). This work was conducted under consideration of the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist. 25
Recruitment procedure
Since we strived to explore our research questions with respect to middle-aged and older adults, eligible participants were community-dwelling adults aged 50 years and older. Recruitment was carried out by a combination of snowball sampling and theoretical sampling. 26 Aiming for theoretical saturation, participant recruitment took place gradually during the analysis process of interviews already conducted. Thereby, a heterogeneous sample particularly in terms of mHealth tool usage and general attitudes toward mobile devices was sought for. To be able to recruit a relatively heterogeneous range of study participants, for instance with regard to age, sex, and occupational status, both online and offline recruitment channels were utilized. Study participants were primarily recruited through social networks (online and offline) as well as via postings and flyers in public places such as supermarkets and pharmacies. In doing so, efforts were made to select the sites in such a way as to ensure the recruitment of participants from various social milieus. Enrollment continued until theoretical saturation was reached, i.e., until the inclusion of new study participants would not yield any new insights regarding the research question. Potential participants were asked to contact the responsible researcher by phone or e-mail. Once initial contact was established, a telephone conversation was held in which eligibility for study participation was clarified and information on the course and content of the study was provided. Study participation was compensated with an expense allowance of 20€ per interview.
Data collection
Qualitative semi-structured interviews were conducted using an interview guideline that primarily involved open-ended questions stimulating narratives. In order to obtain a largely complete, unbiased picture of the participants’ daily (diet-related) routines at the level of practice, the first guiding question (i.e., narrative stimulus) aimed at triggering thick descriptions of typical daily diet-related routines by asking: “Please tell me about your day yesterday. How did the day go exactly? I would like you to tell me everything in detail and in sequence; feel free to start in the morning after you got up.” To allow for comparative analysis, this first question was phrased exactly the same way across all interviews. Thereafter, questions were posed according to the semi-flexible interview guideline as well as immanently generated depending on the course of the interview. The interview guideline was pretested in three interviews. At the end of each pretest interview, feedback on the interview process and guiding questions was obtained from the participants. Subsequently, the interview guideline was discussed and modified within the research group. The major interview themes and sample guiding questions are summarized in Table 1.
Major interview themes and sample guiding questions (exmanent & immanent).

Note. Guiding questions were posed in German language in the interviews.
Depending on the participants’ preferences, the interviews took place either at the researchers’ institute, at the participant's home or in a public space. Before the interviews started, participants gave written informed consent regarding their study participation and verbally agreed to the interviews being tape recorded. All interviews were tape recorded and saved in encrypted form. The recordings were transcribed verbatim and subsequently anonymized, i.e., all personal information potentially revealing the study participants’ identities was pseudonymized. The data material was handled in accordance with the European legal standards of data protection (DSGVO).
Data analysis
Data were analyzed using Qualitative Content Analysis by Kuckartz. 27 First, each interview transcript was skimmed and broadly summarized for the purpose of data organization. Thereafter, the researchers developed a category system in an iterative process involving two major steps: (1) the identification of descriptive, “natural codes” and (2) the generation of “analytical codes.” 27 Once the system had been established, the (sub)categories were checked and, if necessary, adjusted in order to be sufficiently exhaustive (i.e., (sub)categories cover all identified themes), on the one hand, and discriminable (i.e., no two (sub)categories cover the same themes), on the other hand. Based on the final category system, the content-analytical development of a typology according to Kuckartz 27 was carried out. To do so, the categories were linked with one another by means of conceptual mapping. Subsequently, the researchers used the resulting concept map to cluster patterns of acceptance across study participants. Thereupon, a comprehensive typology of acceptance of mobile nutrition and fitness tools was derived. The first author coded the data material and was responsible for further steps of analysis (e.g., the clustering and interpretation). The evolving coding system, concept map, and final typology were intersubjectively validated within the research team as well as by means of interpretation workshops held within a qualitative research group of the Charité – Universitätsmedizin Berlin. In case of ambiguity, consent was reached by discussion among the three researchers involved in this study.
Results
Participant characteristics
A total number of 21 interviews were conducted. The mean age of the study participants was 68 years with an age range from 56 to 81 years. Two-thirds of the interviewees were female (n = 14) and one third was male (n = 7). All but one participant (n = 20) lived in an urban environment, while one interviewee lived in a rural area (n = 1). Approximately two-thirds of the study participants were retired (n = 15), the other third (n = 6) was employed. Further characteristics are displayed in Table 2.
Participant characteristics.

Note. #=interview pseudonym; yrs.=years; smartphone = self-reported smartphone ownership; acceptance type = inductively generated typology classification (see result section: Typology of Middle-aged and Older Adults’ Acceptance of Mobile Nutrition and Fitness Tools).
Emergent acceptance characteristics
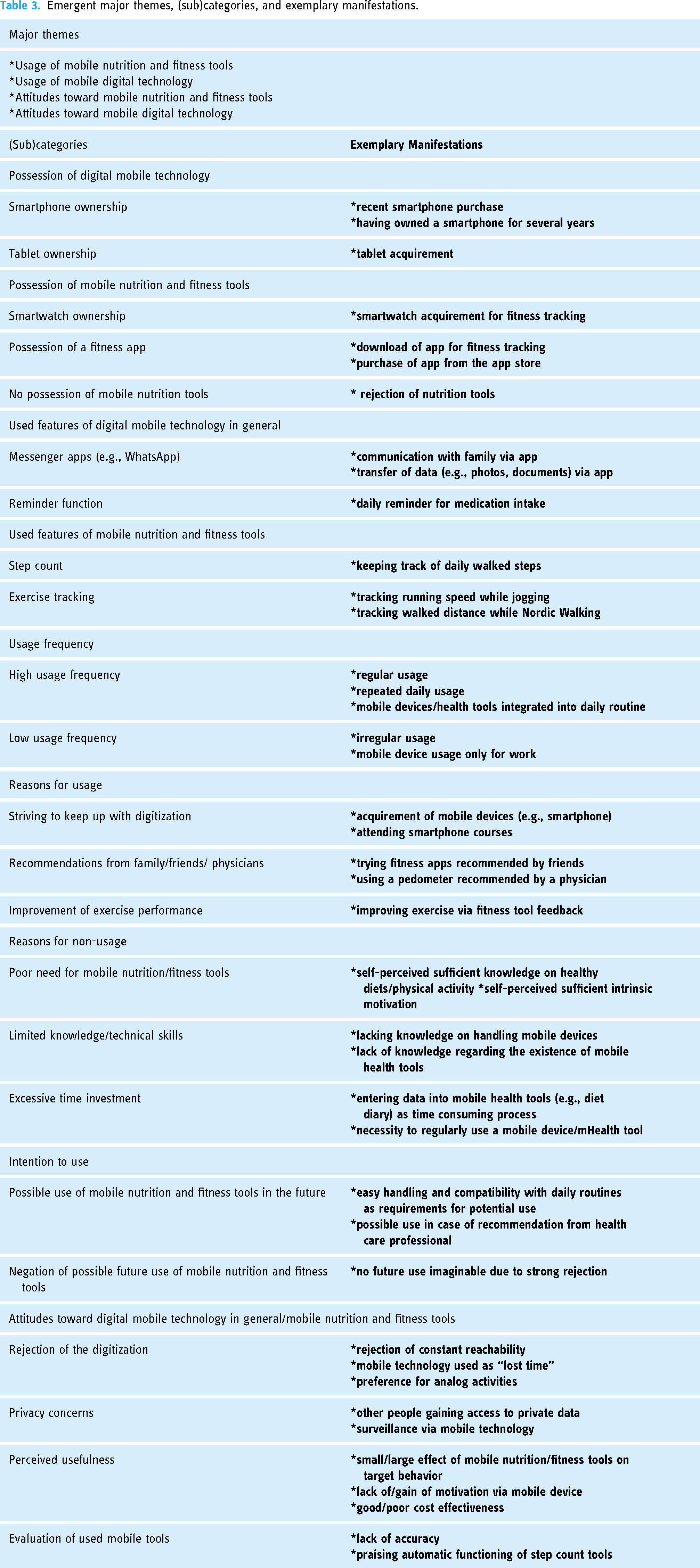
Four major themes emerged from the content analysis: (1) Usage of mobile nutrition and fitness tools, (2) attitudes toward mobile nutrition and fitness tools, (3) usage of digital mobile technology, and (4) attitudes toward digital mobile technology. Simultaneously, various main categories and subcategories reflecting the different characteristics of the major themes were extracted. An overview of the categories as well as the most prominent subcategories and their exemplary manifestations across the interviews are presented in Table 3.
Emergent major themes, (sub)categories, and exemplary manifestations.
Typology of middle-aged and older adults’ acceptance of mobile nutrition and fitness tools
We derived three different manifestations of acceptance from the category system, which constitute the basis of our typology: the Rejection Type, the Selective Acceptance Type, and the Comprehensive Acceptance Type. Figure 1 illustrates the interrelations of the main themes and categories characterizing the target group's acceptance, which underlie the typology.

Illustrative model of the emergent themes, main categories, and their interrelations constituting the three acceptance types.
The three acceptance types differed in the extent to which they used mobile nutrition and fitness tools, digital mobile technology in general as well as in their attitudes toward those tools. Particularly the possession and acquirement of mobile nutrition and fitness tools and digital mobile technology as well as the usage frequency thereof varied greatly between the three types. The data material revealed various reasons for (non-)usage of the mobile tools that showed to be characteristic for each acceptance type. The participants’ attitudes toward mobile nutrition and fitness tools as well as toward digital technology in general showed to be located on a spectrum between endorsement and rejection. Overall, the acceptance toward the respective tools and the different specifications showed to be influenced by various facilitating factors as well as barriers. In the following, each acceptance type is described in greater depth with respect to the aforementioned central characteristics.
The rejection type
The Rejection Type is characterized by non-existing acceptance of mobile nutrition and fitness tools manifesting in non-use and an overall negative attitude toward those tools. None of the study participants of this type used any type of mobile nutrition or fitness tools. Likewise, they had never used one in the past and negated potential use in the future. A central characteristic of this type showed to be the lack of technical requirements for the use of mobile nutrition or fitness tools, i.e., no ownership of mobile devices such as a smartphone, tablet, or smartwatch. Even if they owned mobile devices, participants belonging to this type were either not aware of the existence of mobile nutrition and fitness tools or demonstrated limited knowledge regarding potential features of such tools, as the following quote illustrates: “I wouldn’t get the idea at all. Well, I wouldn’t know that something like this exists and even if I knew […], I wouldn’t even think about checking something like that out.” (#2)
As this interviewee hypothesized, even if she was aware of potential features of mobile nutrition and fitness tools, she would anyways reject testing one. Such a relatively strong rejection showed to be a central characteristic of this type. The study participants’ disapproval seemed to be related to a variety of reasons: The desire for autonomy and self-determination played a key role as the individuals of this type frequently associated the use of mobile nutrition and fitness tools with a resulting “dependency” on mobile devices. Instead, they preferred self-managing their diets and exercise routines without being prompted by any digital support: “People make themselves dependent on such devices and programs and this whole knickknack, yeah. […] but you have a head to think for yourself […].” (#3) This participant rendered any mobile tools redundant because of her sufficient mental capacity. Her self-proclaimed knowledge on healthy lifestyle behaviors is representative for a high level of health-awareness displayed by this acceptance type. Thereby, the participants explicitly stressed their motivation for leading a healthy lifestyle had always been intrinsic and could not be externally generated or amplified by a technical device.
Another major objection against mobile nutrition and fitness tools expressed by this group were relatively profound privacy concerns. The use of those tools was associated with a loss of private information as other people might gain unauthorized access to read and collect data such as information on their daily movement profiles. As an example, one participant expressed her privacy concerns as follows: “And also, to me it's, you also don’t know, ‘um’, we also always talk about this among colleagues, how extensive the ongoing surveillance is, right. Apparently, there are people, who have these ‘um’ bracelets, that, that, ‘um’, where everything, breathing and, and, and heart rate and burnt calories and a thousand steps and [all] this is saved via the smartphone, yes, and others read along. Nope. Don’t need that.” (#3)
The interviewee considered mobile nutrition and fitness tools to be part of an “ongoing surveillance”, suggesting that user data is purposefully stored and viewed in order to continuously monitor the tool's users. According to the participant, this “surveillance” is not only limited to daily movement profiles but also includes sensitive information on vital signs.
Along with their rejection of mobile nutrition and fitness tools, study participants of this type showed a rather low interest in modern digital technology in general. This manifested in a relatively limited knowledge and low affinity regarding digital technology. Moreover, individuals belonging to this type disliked the concept of “constant reachability”, which they associated with the ownership of mobile devices (e.g., smartphones). Thereby, the ownership of a smartphone was viewed as pressure to immediately answer phone calls, text messages, and e-mails at all times. Even more so, they expressed their criticism toward the mobile device usage by others and particularly rejected high usage frequencies of smartphones by family members and friends. Within such social settings, participants belonging to the Rejection Type perceived other people's smartphone usage as an impolite, constant interruption of conversations and shared activities. Such smartphone usage behavior was seen as a “terrible” imposition as shown by this quote: “Actually, I am also always shocked, when you ‘um’, no matter where you are, ‘um’ people [laughing] that are visiting […] also within the family, at coffee parties or something, I say: my God. […] Yes, they sit down and first of all, the cell phone is put down. Terrible. […] Oh well, because that, so it gets constantly looked at, yes, you want to have a conversation and, and they just quickly type something, because they have just received a message” (#3)
While the Rejection Type represents a relatively strong rejection against mobile nutrition and fitness tools, our data analysis also revealed a more differentiated acceptance of said tools. Thereby, a rather positive yet also critical stance toward mobile nutrition and fitness tools could be identified and summarized under the umbrella of a second type of acceptance, which is described subsequently.
The selective acceptance type
The Selective Acceptance Type is characterized by a limited acceptance of mobile nutrition and fitness tools manifesting in selective use and a differentiated attitude toward those tools. Thereby, mobile fitness tools appeared to gain a higher acceptance compared to nutrition tools, since smartphone-based fitness apps and smartwatches were the most commonly used tools within this group – with step count as the most popular feature. Some participants used fitness tools that were pre-installed on their mobile devices (e.g., step count smartphone apps). Others actively downloaded such apps and/or acquired their fitness tools based on recommendations from friends or the media. Individuals of this type named monitoring their physical activity levels as the main objective for their use of fitness tools. While some participants used fitness tools on a daily basis to track their daily step count and their exercise performance (e.g., jogging pace), others made use of such tools on a more irregular basis. They usually checked their daily step and kilometer counts on days with high physical activity levels to receive gratification for their exercise achievements. Correspondingly, one interviewee said: “then I just quickly did five kilometers, right, quickly, and then I specifically looked at it, that was great. […] I walked around there [(a park in his hometown)] again. So, I was really great that day, I basically did 13, 14 kilometers, just walking. And I do like that sometimes, I then confirm that for myself. Then I check, today was really good.” (#18).
As demonstrated by this quote, the participants belonging to this type expressed overall positive feedback regarding their used mobile fitness tools. They described the usage as “enjoyable”, “time-efficient” and “helpful” in monitoring their daily physical activities. Most importantly, step count features were enjoyed due to their automatic functioning, thereby requiring no manual handling. Albeit subordinated, points of critique were also mentioned by this acceptance type. For instance, a lack of accuracy regarding step and kilometer count functions was mentioned – particularly when walking at faster speeds.
In contrast to their acceptance of mobile fitness tools, study participants of this type overall rejected mobile nutrition tools and did not use any. Similarly, they did not see a need for additional support in terms of nutrition tools as they considered their diet to be already healthy and balanced. Moreover, a shift toward a greater behavioral focus on diet was refused. Most individuals of this type lacked knowledge regarding potential features of mobile nutrition tools – similar to the participants belonging to the Rejection Type. When the interviewers referred to potential functions such as a diet diary, participants stressed the effort such functions would necessitate: In particular, the provision of daily food records met rejection, since this was perceived as too time consuming. In addition, estimations of the exact amounts consumed were found to be difficult, especially with respect to meals that were not prepared by themselves. Additionally, participants stated forgetting as hindrance to document meals on a daily basis, especially on stressful days or during working hours. As an example, one interviewee expressed his rejection toward such tools: “I don’t look at it enough for that, then, nope, everything is quite stupid then, […] no, that, for me, I can’t [(do anything)] with something like that, with charts and stuff like that. [(laughing for one second)] I live more out of the feeling, out of desire, so that's more my kind of thing, eh. Not that orderly sorted, rather having a look at what comes.” (#18)
As indicated by this quote, individuals from this type associated documenting their diets with efforts of pre-planning and structuring their daily routines. They rejected fixed structures in their everyday lives and instead preferred flexibility and spontaneity as part of an intuitive lifestyle guided by lust and situational needs.
Contrary to most study participants of this type, a small portion showed a rather positive attitude toward mobile nutrition tools, while rejecting mobile fitness tools. Similar to other participants, they did not use any mobile nutrition tools. However, they hypothesized that they would potentially use such tools in the future. Thereby they mentioned easy handling, practicability, and a fun factor as facilitators increasing the chance of a potential use. As an example, one study participant could imagine using a nutrition app – given two conditions: “Um, if it turns out, that an app is something funny, is uncomplicated, […] then why not, eh? Why not? [(pausing for two seconds)] I would give it a try.” (#12) Along with a rather positive attitude toward certain mobile tools, study participants of this type also showed a rather positive stance toward modern digital technology. They all strived to keep up with the times in terms of digitization and recounted a self-perceived transition toward an increased interest in mobile technology. Accordingly, ownership of at least one mobile device, most commonly a smartphone, was typical for those participants. The level of knowledge and affinity in dealing with mobile devices varied across this type: On the one hand, smartphones were frequently used on an increased skill level, i.e., by using a variety of apps and smartphone features in a private and/or occupational context. On the other hand, participants had just started to learn the basic handling. Participants with a lower skill level and affinity were attending or planning to take smartphone courses, as representatively illustrated by this quote: “So, I have
The Selective Acceptance Type thus demonstrated a certain degree of acceptance that appeared to be very specific to selected mobile nutrition or fitness tools. Our data analysis also exhibited a more extensive acceptance of all mobile nutrition and fitness tools, which could be outlined in a third type described below.
The comprehensive acceptance type
The Comprehensive Acceptance Type is characterized by a relatively broad acceptance of mobile nutrition and fitness tools, manifesting in an extensive use and overall positive attitude toward those tools. Participants of this type used mobile fitness tools, more specifically fitness apps or smartwatches. Similar to the Selective Acceptance Type, the main objective for using either of these tools was the tracking of physical activity, with step and kilometer counts as the most popular features. In addition, smartwatches were used for monitoring vital signs such as the heart rate and blood pressure. While the Comprehensive Acceptance Type used both tools regularly, the usage frequency differed considerably between the two: Fitness apps were used only when performing exercise, resulting in a rather low usage frequency (e.g., once or a few times per week for less than two hours). In contrast, smartwatches were worn almost every day for multiple hours. Fitness tools were bought or downloaded based on recommendations from family and friends.
Overall, participants of this type provided positive feedback on their used mobile fitness tools. According to them, reviewing their exercise performance via fitness apps served as a motivator for an increased level of physical activity. They also voiced positive feedback on the possibility to track different kinds of exercise in their fitness apps such as running, Nordic walking, and cycling. As an example, one participant used a tracking function to monitor the distance covered while Nordic walking. She emphasized this would motivate herself and her walking partner to set future goals: “This [(tracking function)] has motivated us to say: Oops, today it was only, don’t know, six kilometers. Next time we will choose another route and let's see, if it will be a few more [(kilometers)]” (#16) Moreover, the smartwatch was positively evaluated for continuously monitoring vital signs and detecting potential changes of bodily functions such as increases in blood pressure or newly emerging cardiac arrhythmias, thereby serving as an early disease recognition tool. Solely the necessity to frequently charge smartwatches was expressed as a point of criticism.
In contrast to their use of mobile fitness tools, mobile nutrition tools were not at all used by this type. However, each of the participants expressed a relatively high degree of openness and the wish for future usage thereof. To do so, receiving trustworthy recommendations for specific nutrition tools such as mobile apps was stressed as a facilitator. In some instances, participants asked the interviewers for concrete recommendations for nutrition apps: “If someone gives me a recommendation and says: Have a look at this nutrition app, there you can find tips and tricks and whatever, yes. But, ‘um’,
Individuals belonging to the Comprehensive Acceptance Type also presented specific ideas on possible features they would like to use in a mobile nutrition tool. The suggestions were introduced partly in response to immanent inquiries by the interviewers and partly directly expressed by the participants. In particular, participants wished for a reminder function, a recipe feature, as well as for a calorie count system. Thereby, such a count system was compared to the point systems of widely known weight loss programs, which they evaluated positively. Furthermore, emphasis was put on the handling of a calorie count: Overall, it should be “user-friendly” and, more specifically, “easy to use” and “compatible with their daily routines”. In this context, participants rejected efforts to scale every single food item in order to count calories – which corresponds to the stance of individuals belonging to the Selective Acceptance Type. Moreover, a reminder function was proposed as a means for a more regular dietary schedule and an incentive for an increased intake of healthy foods. As an example, classifying fruit as healthy, one individual mentioned the wish for a daily reminder preventing him from forgetting to consume at least one portion of fruit during a stressful day: “I think such a timer is quite good, […] you get reminded “here, do certain things”, right. And because otherwise for me, that gets lost in everyday life and I don’t remember; when you think, “oh man, you haven’t eaten an apple again today, haven’t eaten a banana”, and these contain relatively important ingredients, that are good for the body, I would believe.” (#1)
Besides, interviewees suggested a recipe feature as a tool that provides multiple ideas for simple, quickly prepared and healthy meals, potentially integrating ingredients already available at home. The need for such a feature was expressed due to a lack of ideas for meals with a greater variety.
In addition to their relatively broad acceptance of mobile nutrition and fitness tools, individuals of the Comprehensive Acceptance Type shared an interest in general mobile technology. They owned at least one mobile device i.e., a smartphone or tablet. Similar to participants of the Selective Acceptance Type, participants here showed relatively high levels of affinity and profound skills regarding the handling of their digital devices. This also manifested in the comparably great number of devices they owned and the variety of features and apps they regularly made use of.
Discussion
Principal findings
Living in the “digital age”, the use of mHealth tools has become increasingly integral to everyday life – not only for so-called “digital natives”, but also for adults of middle and older age. Among others, mobile health tools – such as nutrition and fitness tools – have been shown to be effective in facilitating healthy lifestyles in later life. 28 However, usage rates of these tools seem to be rather low among middle-aged and older adults. 24 As unhealthy dietary patterns as well physical inactivity remain two of the leading causes associated with the development of non-communicable diseases,29,30 it appears promising that mHealth tools gain greater popularity among the target group of middle-aged and older adults. It is therefore vital to gain a greater in-depth understanding of their acceptance of such tools, since a lack of comprehensive evidence remains. 24 Thus, the present study explored middle-aged and older adults’ attitudes and usage behaviors as well as associated facilitating factors and barriers by means of a qualitative study and developed a typology of the target group's acceptance.
Based on the emergent themes and (sub-)categories as well as their interrelations (see Figure 1) three types of acceptance could be reconstructed from the data material: The Rejection Type, The Selective Acceptance Type, and The Comprehensive Acceptance Type. The Rejection Type is characterized by a relatively low acceptance toward mobile nutrition and fitness tools, manifesting in non-usage and rather negative attitudes toward such tools. The Selective Acceptance Type displays a more differentiated level of acceptance. Study participants of this type selectively use certain types of mobile health tools while rejecting other tools and show overall mixed attitudes toward mobile nutrition and fitness tools. The Comprehensive Acceptance Type is defined by a relatively broad level of acceptance, reflected in an extensive use of mobile health tools and largely positive attitudes.
In order to investigate acceptance holistically, it is vital to address various dimensions shaping acceptance. Although previously described definitions and models of mHealth technology acceptance differ widely, several recurrent dimensions across multiple acceptance studies could be identified in a systematic review 15 : Perceived usefulness, intention to use, actual usage, user satisfaction, perceived ease of use as well as attitude towards using showed to be the most central characteristics, which largely correspond with the widely known “TAM” acceptance model. 18 Overall, our findings largely overlap with these dimensions, albeit on different hierarchical levels. This congruence underlines that our exploratory study encompassed relevant acceptance dimensions and hence holistically examined acceptance within the target group.
Facilitators for and barriers to mobile nutrition and fitness tool usage
This study identified several barriers and facilitators for mobile nutrition and fitness tool usage. The most prominent facilitators were high levels of usability (e.g., easy handling, practicability, fun factor), trustworthy recommendations (e.g., from friends, the media, or medical professionals), automatic functioning of the tools (e.g., step count), the individual's level of motivation and the perceived compatibility with daily routines (e.g., with respect to time-efficiency). The most commonly mentioned barriers were missing basic prerequisites (e.g., a lack of technical requirements such as smart device ownership, a lack of knowledge on the existence of mHealth tools), a desire for autonomy and self-determination, the perception of insufficient usability (e.g., time consuming tools, difficult handling) as well as privacy concerns. Overall, these findings are in accordance with those from previous research,21,23,31,32 which addressed facilitators and barriers across different age groups as well as for various mHealth tool domains – including nutrition and/or fitness tools.
A lack of knowledge regarding mobile technology, respectively mHealth tools, stood out as a prominent barrier, calling for educational public health measures in order to increase awareness and overcome reluctance. As trustworthy recommendations were also named as facilitators, a promising approach seems to be the education of the target group of middle-aged and older adults via healthcare professionals along with recommendations of specific mHealth tools tailored to the individuals’ needs. Accordingly, the findings from a previous systematic review show that healthcare professionals view mHealth tools as helpful in improving patient care and their interaction with the patients (e.g., quicker contact and communication). 22 At the same time, older adults have been shown to rate recommendations from their physicians highly. 33
Strikingly, some of the facilitators and barriers manifested differently across the three acceptance types. For instance, privacy concerns were strongly stressed as a barrier by participants of The Rejection Type, whereas individuals belonging to The Selective Acceptance Type and The Comprehensive Type barely mentioned privacy concerns. This divergence is also reflected in the literature: Previous research has shown that middle-aged and older adults are significantly more likely to hold greater privacy, respectively, data protection concerns in comparison to younger adults. 34 Yet, privacy concerns have not yet been mentioned as barriers in other studies specifically examining middle-aged and/or older adults’ attitudes toward mHealth tools.23,35
Divergent levels of acceptance between mobile nutrition and fitness tools
While the manifestation of acceptance varied across the three acceptance types, one consistency surfaced: Mobile nutrition tools were met with a relatively lower level of acceptance as in comparison to mobile fitness tools. Even though individuals belonging to The Comprehensive Type expressed a certain degree of openness for potential usage of mobile nutrition tools, none of the participants across all three types actually used any such tools. These findings are consistent with previous research targeting the general population. For instance, König et al. 36 found lower usage rates of mobile nutrition tools compared to mobile fitness tools in a sample of adults aged 18 years and older. Specifically examining attitudes as one dimension of acceptance, Cabrita et al. 35 found that older adults met mobile nutrition tools with less favorable attitudes as in contrast to mobile fitness tools.
In our sample, the reasons for the disparity in acceptance between the two types of tools showed to be many-faceted: Mobile fitness tools were largely positively evaluated for their automatic functioning (e.g., as implanted in step count tools) – a feature that appears not yet widely available in (German) mobile nutrition tools. Potentially due to the necessity of manual handling, nutrition tools were criticized as being too time-consuming and not compatible with the users’ daily routines. These findings are in congruence with the results found by König et al.21,36 Furthermore, our results showed that mobile fitness tools were mainly used to obtain feedback and motivation, thereby serving as an assistive device supporting already existing physical activity routines. At the same time, mobile nutrition tools were rejected as assisting devices. The interviewees emphasized that they already possessed sufficient levels of health awareness and extensive knowledge of healthy diets and therefore did not see a need for any technological support in terms of mobile nutrition tools. These findings are congruent with those by Cabrita et al. 35 : In their sample of older adults, nutrition tools were rejected if no need for technological support was seen due to the individuals’ perceptions of a well-working dietary self-management.
Another previously described explanatory approach for the divergent acceptance levels concerns the different types of feedback provided by mobile nutrition and fitness tools. 21 Fitness tools such as smartwatches and step count apps provide continuous feedback on daily physical activity levels as well as immediate feedback on exercise performance, thereby allowing for prompt and constant modifications to physical activity routines. 21 On the contrary, feedback provided by mobile nutrition tools such as calorie counts and diet diary apps is mostly limited to mealtimes and often delivered only after food intake. 21 Using a nutrition app for supporting the readjustment of eating behaviors thus proves more difficult and requires more complex planning than, for example, counting steps and may therefore be associated with greater barriers to usage, e.g., connected to a perceived excessive necessary time commitment.
Transition toward increased digital mobile technology usage among middle-aged and older adults
The so-called digital divide suggests that access to digital technologies varies greatly across populations based on sociodemographic characteristics – such as age, place of residence, and socioeconomic status. 37 In this context, older adults have been shown to be less likely to use modern digital technologies such as the internet or smartphones in comparison to younger people of the same population. 38 Yet, the number of digital technology users among middle-aged and older adults has increased over the last decades.39,40 Our findings may be contextualized against this background. Particularly participants of The Selective Acceptance Type reported to be in a self-perceived transition period toward increased mobile digital technology acceptance, thereby expressing a wish to keep up with the times in terms of digitization and frequently attending mobile technology courses such as smartphone classes.
Yet, the results of this study also point toward a pronounced divide within the target group of middle aged and older adults: While The Selective Acceptance Type, as well as The Comprehensive Type, demonstrated relatively high levels of acceptance toward mobile digital technology, participants from The Rejection Type strongly denied it. This divergence has also previously been described particularly with respect to the population of older adults.38,41 In this context, older age, a lower level of education as well as health conditions and disabilities have been negatively associated with the use of digital technology by older adults. 38
Friemel 38 argues that the digital divide is based on a generation cohort effect that might dissolve once younger generations grow older. The same conclusion has been drawn in other previous works.42,43 However, certain individual factors related to old(er) age that hinder mobile digital technology use – such as physical disabilities as well as decreasing cognitive skills - will remain across generational cohorts. 38 These limitations thus call for the development of more individualized mobile technology that better matches older adults’ physical and cognitive abilities. 38 At the same time, it also seems worthwhile to foster mobile technology usage already at younger age stages. As our study results indicate, there is also a need as well as potential to increase acceptance among middle-aged adults. Increased levels of acceptance among this particular age group, e.g., by promoting more positive attitudes toward mobile nutrition tools, may potentially lead to an increased familiarity and a broader set of skills regarding the handling of mobile technology. Such early usage practices may be beneficial in attenuating aforementioned age-related usage barriers.
Implications for future mHealth tool development
In order to effectively facilitate change toward healthier lifestyle behaviors in middle-aged and older adults, it is essential that mHealth tools are adapted and tailored to their specific needs and expectations. Many known tools were rejected for their difficult and time-consuming handling, whereas a high level of usability emerged as a key facilitator contributing to a higher level of acceptance within the target group. Therefore, more tools with easier, more time-efficient handling and the option for automatic functioning (e.g., implemented in step count tools) need to be developed. User testing specific to the target group and its heterogeneity, including differences between subgroups stratified for age and other sociodemographic characteristics, should thereby play a major role. For instance, a recent systematic review examining user testing as well as acceptance studies in regard to older adults’ experiences with wearable health devices has identified promising approaches for increasing usability: small tools with easy-to-read displays as well as long-living batteries were largely positively evaluated while inaccurate, uncomfortable devices with a lack of adequate operating instructions were broadly rejected. 31 Additionally, Moore 31 established various measures that can increase the acceptance within the target group, among which are easy-to-understand instructions, personalized feedback aligned with the users’ goals, and input from healthcare professionals to overcome usage barriers. Highlighting the importance of high levels of usability as well as additional support, e.g., from physicians, these findings are largely in congruence with our study results, involving middle-aged and older adults.
Moreover, our findings indicate that middle-aged as well as older adults prefer to choose from a range of features within mHealth tools to match their needs at the moment. For instance, some participants voiced the desire for a calorie count feature, while others wished for a recipe feature or a reminder function. Similarly, mobile fitness tools were positively evaluated for offering the possibility to track different kinds of exercise. Giving users the opportunity to choose from different feature options thereby increases the tools’ compatibility with their daily routines as well as their sense of autonomy. Both, consonance with daily routines as well as autonomy were stressed as important facilitators when using mHealth tools by our study participants as well as in previously conducted user testing studies within the target group of middle-aged and older adults. 31
Lastly, it seems worthwhile to better take middle-aged and older adults’ privacy concerns into consideration when developing mHealth tools, as they showed to be a central aspect of respective barriers to acceptance. Therefore, two measures appear particularly suited: On the one hand, the tools should be developed or approved by trustworthy institutions such as National Ministries of Health or other public health authorities. On the other hand, it seems promising that health care professionals, e.g., general practitioners, in their role as “gate keepers of health-care delivery” 44 recommend and also possibly prescribe mHealth tools to their patients. Previous research has shown that both patients, as well as healthcare professionals, view this opportunity as profitable. 45 By these trust-increasing means, privacy concerns, respectively data protection concerns, could be mitigated, particularly among middle-aged and older adults.
Strengths and limitations
The results of this study provide in-depth insights into middle-aged and older people's acceptance of mHealth tools, thereby exploring various acceptance dimensions and their manifestation across different acceptance types. The results are valuable for the future development of mobile nutrition and fitness tools, allowing developers to tailor the tools to the needs and expectations of middle-aged and older adults. Our findings can also guide future research, particularly with regards to the differences in acceptance within the target group as well as toward various mHealth tools.
Our study findings have to be seen in the light of some limitations: First, the participant recruitment process may have been vulnerable to a certain degree of selection bias. Since our study comprised health and nutrition-related research topics, individuals with a higher level of pre-existing health awareness and/or interest in dietary matters might have been more likely to participate. The participants of our study also had a higher socio-economic status and a higher level of education than the general population, both of which might also be associated with a more pronounced degree of health literacy. 46 While this study explicitly aimed at exploring our research questions with respect to middle-aged and older adults, the relatively broad age range of our sample may have affected the conclusiveness of our findings. Furthermore, all but one participants lived in an urban environment, which may have influenced their dietary patterns as well as their access to mobile technology, for instance with respect to a broader availability of high-speed internet as in comparison to rural areas. Additionally, the study participants were unevenly distributed across the three emerging acceptance types, with only two participants belonging to The Comprehensive Acceptance Type. However, since qualitative research does not strive to quantify, further quantitative research is needed in order to determine whether this unequal distribution can be validated and generalized. Finally, our cross-sectional study was based on retrospective data which only allows inferences to be made as snapshots.
Directions for future research
Since our findings point toward divergent levels of acceptance regarding mobile nutrition and fitness tools within the target group of middle-aged older adults, it seems worthwhile to further investigate factors that may differently shape the target group's acceptance toward these mHealth tools. For instance, future research should examine the acceptance of different age groups by taking a look at smaller age ranges within the target group of middle-aged and older adults, thereby aiming to identify the heterogenous needs and expectations regarding mHealth tools that are specific to various subgroups. Moreover, other social determinants, for example the socioeconomical status, place of residence, partnership status and the number of children, and their association with middle-aged and older adults’ acceptance of mobile nutrition and fitness tools should be further examined. It also seems promising to investigate how far biographical changes related to the transition to middle and older age as well as from middle-age to older age have an effect on the target group's acceptance of such tools. For instance, the transition to retirement might increase interest in health-related topics, which, along with a gain of leisure time, might increment older adults’ acceptance of mHealth tools. Moreover, with respect to biological changes when transitioning from middle to older age, such as decreasing feeling of hunger, potentially resulting in lower food intake for instance, mobile health tools might need to be adapted and specifically tailored to nutrition-related challenges arising in older age.
Additionally, there is a need for longitudinal investigations to gain a deeper understanding of middle-aged and older adults’ acceptance of such mHealth tools over time. Those studies are needed to analyze dynamics in attitudes and usage behaviors, thereby also addressing circumstances and facilitators that initiate usage or lead to changes in attitudes, for instance. While our findings as well as previous research indicate a rather strong divergence of acceptance between mobile nutrition and mobile fitness tools, only a few potential reasons for the discrepancy have so far been explored. Future research should therefore aim to better understand the differences in usage behavior and attitudes toward each of these tools, thereby creating the basis for mobile nutrition tool developers to address specific barriers and better tailor their tools to middle-aged and older adults’ needs and expectations.
Lastly, there is a need for further quantitative and especially mixed-methods studies with representative samples of populations from different global regions to validate the present body of knowledge and to facilitate generalized conclusions to be drawn.
Conclusion
To our knowledge, this is the first in-depth qualitative study yielding a typology on middle-aged as well as older adults’ acceptance of mobile nutrition and fitness tools. The three acceptance types identified provide insights into various dimensions of acceptance and their interrelations, thereby adding to the existing body of knowledge in the field of technology, respectively mHealth technology. Overall, our findings highlight a need for the future development of more individualized mHealth tools that are specifically tailored to middle-aged as well as older adults’ heterogeneous needs and expectations – particularly with regard to usability and privacy concerns. Finally, this study gives directions for future research activities that are crucial to address in order to improve public health strategies and thus support healthy aging using digital solutions.
Footnotes
Author contributions
Together with NB, the first author (JV) conducted the interviews. JV was responsible for the data organization, anonymization, the coding process, the typology development as well as the manuscript preparation. Where necessary, JV and NB analyzed the data intersubjectively. NB supervised the research process and regularly provided feedback on analyses and the writing process. LS was engaged with the (pre-)final manuscript preparation. LS and NB were involved in the funding acquisition and study preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of the Charité-Universitätsmedizin Berlin approved this study (REC number: EA4/151/16).
Funding
This study was conducted in the context of the NutriAct Competence Cluster – Nutritional Intervention, Behaviour and Products (Germany). The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Federal Ministry of Education and Research [grant number 01EA1806D].
Guarantor
JV
Abbreviations
mHealth: mobile health
TAM: Technology Acceptance Model
UTAUT: Unified Theory of Acceptance and Use of Technology