
Abstract
Objective
Dietary assessment is important for identifying patterns that can influence an older adult's medical conditions. Existing assessments are dependent on the recall limit of the current use of dietary tools. This pilot study aimed to compare the short-term usability and acceptability of a novel voice-based dietary recall tool (DataBoard) to the traditional Automated Self-Administered Dietary Assessment Tool (ASA-24) in older adults.
Methods
Participants aged over 65 years old, meeting specific criteria, were recruited through Research For Me and Research Match across a six-month period in 2023–2024. During the session on Zoom, they were randomly assigned to complete either a voice-based recall via DataBoard or use ASA-24 first, followed by a semi-structured interview. DataBoard enables survey completion using speech input through shared links. We obtained data on meal choices, participant feedback, and preferences for either method using a 1–10 rating scale (low to high agreement). Descriptive statistics and qualitative coding were conducted.
Results
We recruited 20 participants (mean age 70.5 ± 4.26 years, 55% female and 35% non-White). Feasibility and acceptability of DataBoard's voice-based recall were rated as 7.95/10 and 7.6/10. Participants rated the overall performance of DataBoard as easier than the ASA-24, with an average rating of 6.7/10. Participants preferred using DataBoard; they felt it could be used more frequently to report food than ASA-24 (mean 7.2/10). Dedoose analysis revealed preferences, challenges, and usability insights for DataBoard.
Conclusion
Older adults supported voice-based recall as a means to evaluate dietary intake. Further evaluation with larger cohorts of older adults could provide additional opportunities to create a better tool for food recall.
Introduction
Dietary assessments are used by healthcare practitioners to assess the nutritional status of older adults. 1 These are crucial since they help identify dietary patterns that can identify nutritional deficiencies. Older adults experience physiological changes such as reduced appetite, altered taste and smell, and difficulties with chewing and swallowing.2,3 Chronic conditions such as diabetes, cardiovascular disease, and osteoporosis require specific dietary interventions to manage symptoms and improve quality of life. 3 Since malnutrition and weight loss in older adults increase hospitalization, functional decline, and mortality, understanding macro- and micronutrient intake is essential for targeted treatment. 4
A widely used dietary tool in nutritional studies is the web-based Automated Self-Administered Dietary Assessment Tool (ASA-24). ASA-24 is a publicly accessible survey tool that prompts users to report their meals, snacks, and supplements in specified time windows during a given day. 5 ASA-24 recognizes an extensive list of foods with pictures of portions to help accurately quantify how much a respondent has intaken. 5 While extensively validated, the ASA-24 has its drawbacks. 6 One study showed there is difficulty completing the ASA-24 unassisted, where usability issues included not knowing what to do next without an interviewer present, misunderstanding questions, and having inaccurate dietary items. 6 The multi-step process of inputting meal context, then details, can be time-consuming and frustrating. 6 Other screening tools include the Malnutrition Universal Screening Tool (MUST), Mini Nutrition Assessment (MNA), and Malnutrition Risk (SCALES). 7 However, the MNA tends to overestimate malnutrition, while MUST and others lack validation in older hospitalized populations. 8 While many tools are self-administered, few have been tested for reliability, sensitivity, or sample size justification for older populations.8,9
Voice assistant systems (VASs) may offer a promising alternative with the use of artificial intelligence (AI) for processing and responding to voice commands. 10 VAS can support older adults in medication adherence, self-managing pain, and in nutrition monitoring.10,11 In dietary settings, studies show older adults prefer voice-only reporting over touchscreen-based methods. 12 Interactive voice response (IVR) calls promote healthy eating habits and weight loss, with participants losing up to 3% of body weight in 3 months. 13 Amazon Alexa-based systems have been tested too, but often interrupt users or fail to capture detailed data and long phrases spoken. 14 VAS tools for dietary assessment remain largely in prototype stages, not yet tailored for older adults. Digital literacy challenges, cognitive decline, and memory-dependent reporting can make traditional assessments difficult for this population. 15 Despite expanding dietary assessment technologies, older adults remain disproportionately affected by the digital divide, which limits equitable access. The presence of age-related changes in vision, hearing, cognition, and motor skills for older adults may mean that the use of screen-based interfaces is challenging. Memory-based dietary recall tools can be impacted by the compromised cognition in aging populations. This collectively highlights the growing need for tools that are accessible for older adults for proper representation in nutrition and care. VASs have the potential to be accessible to them.
Dietitians have previously shared feedback that using VAS for assessing dietary intake in older adults may enhance food intake reporting, portion recall, and efficiency during clinic visits. 10 In this study, we propose using SurveyLex, a voice survey developer and distributor. Our research question aims to determine whether older adults prefer using voice-based recall or ASA-24. We propose testing the usability of older adults’ use of the novel voice-based tool DataBoard when recalling their meals over the past 24 hours compared to the standard ASA-24 online-based tool. DataBoard, from SurveyLex, is the application where dietary surveys can be created. Our goal was to assess whether older adults could effectively use voice-based tools for dietary reporting by collecting both quantitative ratings and qualitative feedback. Older adults would test DataBoard's platform for the first time, allowing surveys to collect audio-recorded responses to help us evaluate the voice-based intervention. The project's aim was also to determine if voice-based recall, using DataBoard, can be acceptable in the short term as a better user-friendly dietary intervention tool to recall meals in the past 24 hours for older adults. By using this system, SurveyLex will further dietary assessment research in the field of voice-based recall for older adults, providing better insight into a new technology-assisted structure for dietary assessment, guiding future research in digital monitoring.
Methods
Study setting and design
This usability pilot study was conducted remotely by the lead author (female, BSPH student at UNC Chapel Hill) over Zoom between September 2023 and December 2024. We recruited older adults and focused on the usability of using DataBoard, an online platform system, in one single session. There were two study arms, and participants were randomly assigned 1:1 to each of the two sequences: (a) a recall of what they ate the previous day using either DataBoard followed by the Automated Self-Administered 24-hour dietary recall (ASA-24), or the reverse sequence (see Figure 1). At the conclusion, all participants engaged in a semi-structured acceptability interview. All participants provided informed consent. The study was IRB approved (21-2034) by the University of North Carolina at Chapel Hill's Office of Human Subject Research.

Study flow.
Participant recruitment
Participants were recruited through Research For Me and Research Match Research For Me, a University of North Carolina (UNC) at Chapel Hill and UNC Health specific website that allows volunteers to get connected to research opportunities. Research Match is from the National Institute of Health and serves to help people across the United States connect to research. Inclusion criteria were ages 65 years or older, having access to the internet, and an ability to complete all study procedures. Participants needed to be able to converse and understand English. Exclusion criteria included psychiatric diagnosis (major depression, schizophrenia, bipolar disorder), life-threatening illness (including those receiving palliative care or hospice services), movement disorder (Parkinson's), epilepsy, severe traumatic brain injury, or dementia. All participants provided informed consent electronically before enrollment and completed the Callahan cognitive test to determine if they could complete the study by themselves or if they needed a caregiver/family member to give assent. A REDCap link detailing electronic consent was sent for participants to sign prior to study visits. Participants consented to both audio and video recording through Zoom.
Study procedures
Participants received demonstrations for both ASA-24 and DataBoard before testing them independently. Participants were asked what they ate for breakfast, lunch, and dinner to create the individual DataBoard links while on Zoom. DataBoard is a voice-based survey tool that allows participants to input their dietary data using speech, while ASA-24 is a validated web-based 24-hour dietary recall tool. Participants provided meal intake data from the previous day using both methods.
For the DataBoard arm, participants were texted or emailed links to the individual surveys that had prompts for them to answer general meal times/locations, and specific breakdowns of breakfast, lunch, and dinner. Once the question was read aloud to them, participants were able to record their response as they spoke into the microphone of their device. The system maintained spoken responses in the cloud. For ASA-24, each participant received a unique login and password. The platform walks users through a detailed questionnaire about food intake, meal timing, media usage during meals, ingredients, preparation methods, portion sizes, and commonly forgotten foods. Participants concluded ASA-24 by reviewing how representative the day's intake was compared to their typical diet.
Randomization procedures
Participants were randomly allocated to one of two groups (A or B) using Microsoft Excel (Redmond, Washington). Group A consisted of conducting the ASA-24 first, followed by using the DataBoard platform. Group B completed DataBoard first, followed by the ASA-24. This design allowed for comparison of user experiences with both methods. The investigator was not involved in coding the randomization, and the randomization order was revealed just prior to each study session.
Study assessments
Upon completing both dietary recall tools, participants reviewed the prompts used by DataBoard for each meal and shared feedback on how clear or difficult they were to understand (Supplemental Appendix A). They were asked to suggest improvements to wording, layout, or question flow. Next, participants indicated which method they preferred, in what context, and why (Supplemental Appendix B). Participants were directed to a REDCap link where they completed questionnaires on the feasibility of the voice-based technology compared to ASA-24 and the effectiveness of the study session (Supplemental Appendices B and C). The session ended with an exit interview where participants shared their insights into how they felt about the study, voice-based recall, and AI use in healthcare (Supplemental Appendix D). Participants also expressed their willingness or reluctance to use voice-based recall again for dietary assessment in the future. Additionally, demographic data was collected. Upon completion of a study session, each participant received a $25 Amazon gift card for their participation. Audio files of the recordings were downloaded from Zoom. The semi-structured interview questions were adapted from validated usability frameworks, including the Conceptual Model (following user-centered design principles of study, stimulate, prototype, evaluate, and will), the Roy Adaptation Model (how users adapt to learnability changes), the Technology Acceptance Model (perceived efficiency), the Unified Theory of Acceptance and Use of Technology (user experience), and the Theory of Planned Behavior (how technology use is impacted by attitudes towards technology).16–20 The questionnaires were previously tested in other studies done by our group.16,21 Theoretical data saturation was achieved.
Researcher reflexibility statement
The primary researcher was a female BSPH student at UNC Chapel Hill studying biochemical nutrition and public health. To minimize any bias, the researcher adhered to the questionnaires and followed the study protocol.
Data analysis
Descriptive statistics, including mean and standard deviation, were used to summarize participant feedback from the Likert scale questions. Survey responses were analyzed using a structured data analysis protocol to assess transcription accuracy, response relevance, and response quality. These had word error rate (WER) measured, relevance of answer to prompts, answers that needed explanation, average word count of answers, and average audio length.
The protocol aimed to evaluate the performance and accuracy of the Whisper Automated Speech Recognition (ASR) system in transcribing meal recall responses through comparison of ASR's output with ground truth data provided by human translators. WER was calculated to compare ASR text with ground truth text to measure the effectiveness of ASR in recognizing specific labeled entities. This is done through coding using a general formula: (S + D + I)/N. 22 S stands for substitutions (words in ASR output text that were different than ground truth text), D stands for deletions (words in ground truth text that were not found in ASR text), I stands for insertions (additional words found in ASR text but not ground truth), and N stands for total words of the ground truth text). 22 WER compares ASR output with human transcription in order to evaluate the overall accuracy of the ASR system. The labeled entities data was used to ensure that the transcribed responses aligned with the context of the questions asked. Coding was carried out by a single research assistant (RA), without the involvement of multiple coders or consensus procedures.
First, spoken responses were transcribed into text using an ASR tool, with each transcription having an identifier linking it to the corresponding audio file and metadata. The ground truth text had mostly one-word responses, so contextual labeling was done to check if responses were in or out of context in relation to the prompt. Responses were manually labeled based on relevance to the survey question (relevant/irrelevant) and scope coverage (complete/partial/off-topic). The same labeling criteria were applied to both datasets for consistency. To evaluate the effectiveness of ASR, the labeled entities in the ground truth text were compared to those in the ASR transcript. The percentage of relevant responses was determined with this formula:

Similarly, responses requiring clarification or additional explanation were identified through manual tagging. Their percentage was calculated using this formula:

To determine the verbosity of responses, the average word count per response was calculated:

To assess the duration of responses, the average audio length was calculated:

Any outliers in response duration were flagged for further qualitative review.
For the qualitative analysis, Dedoose was used to systematically identify patterns and themes within participants’ open-ended responses in the semi-structured interview. Audio recordings from the interviews were professionally transcribed using TranscriptNinja to ensure accuracy and completeness. These transcripts were uploaded to Dedoose with no identifying information present. Codes were developed based on recurring keywords, phrases, and contextual cues. This allowed for a deeper understanding of participant sentiments about DataBoard compared to ASA-24. Dedoose enabled the identification of common themes, preferences, and challenges expressed by participants. This thematic analysis provided valuable insights into the user experience and key motivations for participating in the study. Participants reflected on how easy or accessible the DataBoard was. They also offered suggestions for future use and pointed out interface problems. Dedoose highlighted key aspects of user experience.
Results
Participant demographics are presented in Table 1. The average age of participants was 70.5 years ± 4.26 years (55% female) at the time of screening. Participants were 25% African American. Table 2 presents Dedoose code frequencies to display common sentiments amongst several participants. Participants provided mixed feedback on the voice-based recall tool compared to the ASA-24. While seven out of 20 participants (35%) preferred the ASA-24, 13 participants (65%) indicated they would use the voice-based recall tool again. The majority (19/20, 95%) did not find it difficult to answer questions using the voice-based tool, and 16 out of 20 (80%) reported no difficulty in understanding the questions. However, some challenges were noted: six participants (30%) found the interface challenging, and another six (30%) felt the tool was too long to sit through. A smaller subset (3/20, 15%) mentioned that the tool felt confusing when prompts were not followed exactly. Privacy concerns were minimal, with 16 out of 20 (80%) reporting no issues. No participants failed to use either tool. One participant withdrew from the study due to being uncomfortable on camera. No interviews were incomplete.
Baseline characteristics of enrolled participants, N = 20.

One participant chose to not answer this question in the demographics survey.
One participant chose to not answer this question in the demographics survey.
Participant feedback on Automated Self-Administered Dietary Assessment Tool (ASA-24) versus voice-based recall. Count: N = 20.
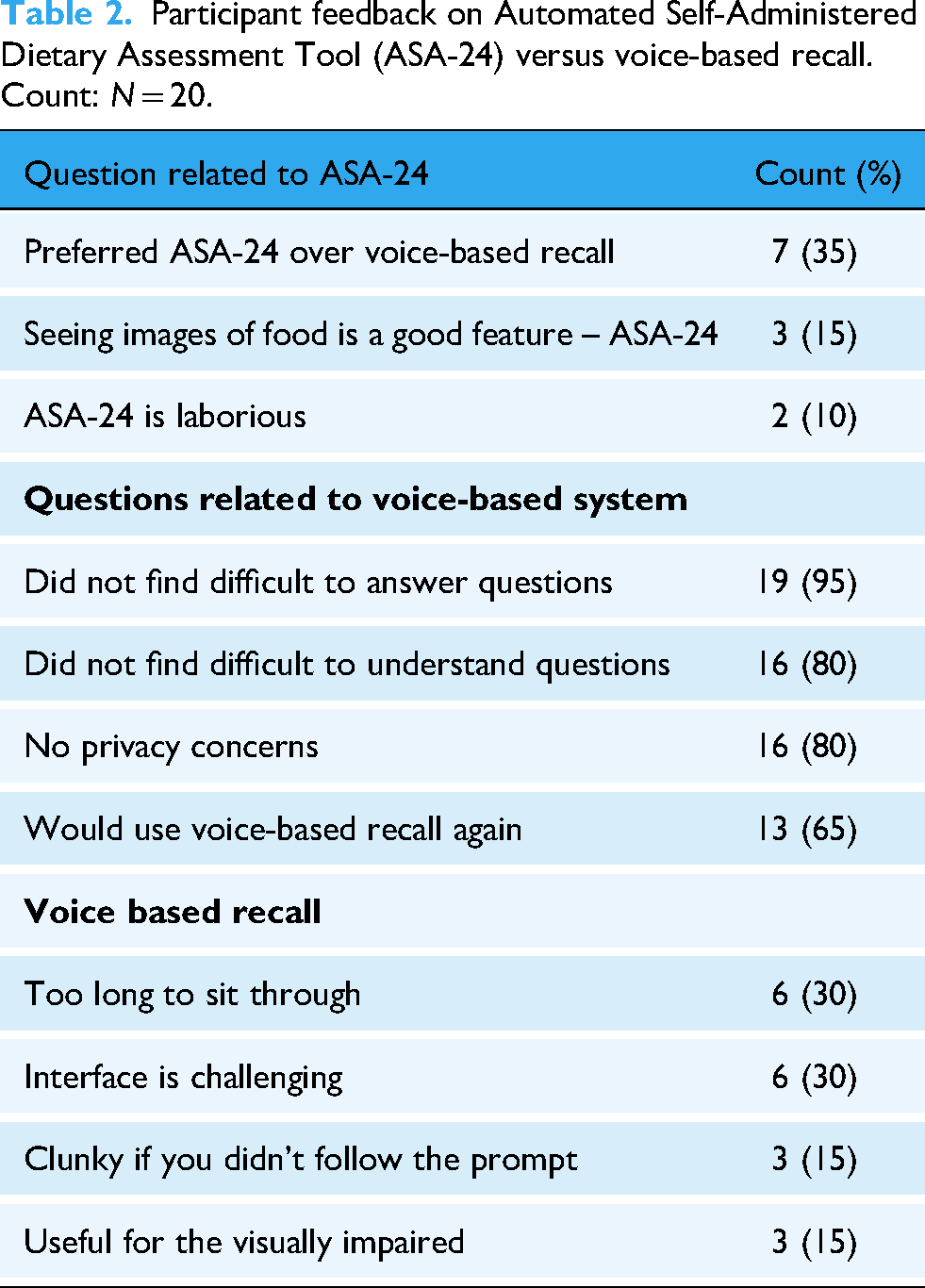
As shown in Table 2, participants expressed difficulties in maintaining consistent meal tracking due to memory lapses or time constraints. Voice-based recall was generally seen as a convenient alternative, with many noting its ease of use. However, limitations included word recognition errors, uncertainty about whether recordings had started, and a lack of speed control were observed. Some participants found the interaction human-like, reminiscent of devices like Amazon's home assistant Alexa or Apple's Siri. Participants highlighted the potential for voice-based recall in allowing meal patterns to be tracked and shared. To improve the tool, nutritional feedback, such as calorie and macronutrient breakdowns, was mentioned. Some found the web-based ASA-24 more reliable, while others viewed it as time-consuming. A hybrid model combining both voice and text input could be an effective approach.
Figure 2 displays the self-reported ratings participants gave in response to questions comparing voice-based recall to ASA-24. No participants rated all items the lowest (1), indicating the absence of floor effects. Two participants rated all items the highest (10), indicating the presence of a small ceiling effect. On average, participants rated the ease of voice-based recall the highest at 8.0/10 (range 1–10). Other aspects that received high ratings included AI being more acceptable for older adults (7.6/10) and participants’ willingness to use voice-based recall more frequently for food reporting (7.3/10). Moderate ratings were observed for accessibility to perform voice-based recall (7.6/10) and performing voice-based recall when cooking/eating is more accessible (7.8/10). Participants rated voice-based recall as being easier to perform than ASA-24, the lowest (6.7/10).

Participant average ratings (scale of 1–10) in response to survey questions comparing voice-based recall and ASA-24, N = 20. Rating: 1–10, where 10 is most easy/most agreed with questions asked (left to right): ease of VB, performing VB is easier than ASA-24, when cooking or eating performing VB is easier, accessibility to perform VB, performing VB is more accessible than ASA-24, when cooking or eating VB is more accessible, would use VB more frequently to report food, AI is more acceptable for adults. VB: voice-based; ASA-24: Automated Self-Administered Dietary Assessment Tool; AI: artificial intelligence.
Table 3 outlines the perceptions of voice-based recall. Participants reported various challenges and benefits associated with meal recall using the voice-based tool. A common difficulty was maintaining consistent tracking voice-based recall was perceived as a convenient alternative for older adults who are less comfortable with computers. There were issues with intonation and pronunciation, impacting comprehension. Usability preferences varied as some found the tool intuitive while others experienced difficulties adapting to its interface. Participants expressed frustration at being unable to adjust the pace of the questions being read aloud. Participants saw potential clinical applications for caregiver communication and meal tracking, but suggested adding features that provide nutritional feedback. Finally, some participants suggested that a hybrid model may be the most effective approach for dietary tracking.
Perceptions on voice-based recall.

The WER was 36.5%. This is on the higher end, indicating the answers participants provided were too short to gather a true comparison to the ground text. The relevance of responses to survey questions given by participants was 98.0%. The percent of responses needing further clarification was 3.3%. The average number of words used by participants while answering questions was 5.32 words, while the average audio length of a response was 4.9 seconds.
For those performing the ASA-24 first, ratings on how easy to use the DataBoard ranged from two to 10, with a mean score of 8.25. While the majority rated the tool highly, three participants (25%) gave low-to-moderate scores (≤4), suggesting some difficulty. For those who used DataBoard first, ratings on how easy the use of DataBoard was ranged from one to 10, with a mean score of 7.63. Although most participants rated it positively, two participants (25%) gave very low scores (1 and 3), indicating challenges with the interface. Overall, both groups showed similar variability, with a majority finding DataBoard easy to use, but a small subset in each sequence reporting difficulty.
Higher education post-college and with a college degree led to mixed ratings. Some preferred DataBoard strongly (scores 9-10) while others rated it low (1-2), suggesting difficulty with it. Some College participants had the most consistent positive view of voice-based recall. Education levels may have influenced perceptions of DataBoard. Those with College and Post-College Degrees had more variable experiences. When examining willingness to use the voice-based recall tool again by education level, mean ratings were highest among participants with Some College (7.6) and College Degree (7.8). In contrast, participants with Post-College Degrees provided a lower mean rating (6.5) and demonstrated greater variability, ranging from very low (1-2) to the maximum rating (10).
Discussion
AI has the potential to be a powerful tool in medicine and in medical outreach. Emerging voice-based technologies have been developed. For instance, the Mayo Clinic launched a First Aid Alexa voice skill set that can answer verbal questions and give step-by-step instructions on the treatment of conditions like cuts or burns. 23 In times of emergency, having instructions to hear while actively following them can be critical for care. VASs are also utilized according to the fact that speech deficits have been documented for detecting early Alzheimer's disease. 24 A study used data analytics and machine learning algorithms to infer cognitive status in participants with mild impairment from Alexa's audio transcripts. 24 In populations of older adults, early detection is critical to help determine interventions to allow for quality care. Advancements in AI, such as domain-aware intermediate pretraining, can improve dementia detection by training language models to detect decline through speech and linguistics. 25 These resources highlight the growing roles and capabilities of voice-based technology in delivering accessible information and interpreting findings for clinical use. Our findings on older adults’ short-term perceptions of usability and accessibility on voice-based recall reinforce that implementation of AI in dietary interventions requires greater attention to user-centered design and adaptability to diverse user needs.
We acknowledge that voice-assistant systems specifically for dietary assessments may still be a novel paradigm.10–12 One study aimed to create an AI-powered assistant to provide caregivers of older adults with dementia a tool that can give instructions on cooking and nutritional advice for their residents. 23 Another application of AI in dietary tracking involves a mobile app called Recaller, which allows users to take pictures of their meals. 26 These platforms align with DataBoard, aiming to simplify dietary tracking. Yet, common issues in the use of voice-based systems include the time to gain familiarity with interfaces. This may be why DataBoard was rated higher for acceptability and ease of use but lower for being easier to perform compared to the ASA-24. Future studies may need to plan training sessions in advance to familiarize participants with the tools being tested. By integrating features like automated reminders, real-time feedback, and images, voice-based recall can help improve adherence to dietary tracking. It is important to recognize that technology-based dietary tools can offer flexibility and efficiency but may create concerns about privacy and user proficiency. 27 Research in this field should further explore how to bridge the digital divide and enable older adults who have varying levels of digital literacy to feel equipped for engagement with dietary tools that require technology. It may lead to improvement with adherence to dietary routines and long-term adoption.
Perceived ease of use for DataBoard was generally high across both task orders, with comparable proportions of participants in each group reporting difficulty, suggesting that challenges with the tool were not strongly influenced by the sequence of use.
Education level may shape participants’ willingness to adopt DataBoard for future use, with those holding college or post-college degrees showing more variable experiences, while participants with some college provided the most consistently positive ratings.
Our study has a number of strengths. First, we conducted a mixed-methods approach that incorporated both quantitative and qualitative data. It offered unique perspectives and insights into how older adults felt about the use of DataBoard and voice-based assistants in general, but also provided objective measures of ease of use, accessibility, and accessibility when multitasking. The study was designed with the goal of keeping older participants in mind; it reflects the needs of this population and is patient-centered. The study utilizes AI, which is emerging across all fields and has been shown to be an evolving prototype that can be strengthened. To our knowledge, this study is the first of its kind in which voice-based recall with AI is compared with ASA-24 in the population of older adults.
While the novelty of the study and its findings are promising, we acknowledge a number of limitations. This study's sample size of 20 participants is small, limiting generalizations to other populations. In addition, there is a lack of racial and ethnic diversity among participants, as 35% of the sample identified as persons of color. The evaluation relied on older adults’ memory to recall their diet in just the past 24 hours. This raises the question of how DataBoard and voice-assistant systems in general may be applied in long-term use. Herein, we specifically included older adults with intact cognitive function and acknowledge that others with degenerative or psychological disorders are not represented in the sample and may require adaptations in the technology. Recruitment through online platforms specifically for signing up to participate in research may have attracted more digitally literate participants or those with access to technology. A further limitation of an ASR-based dietary recall is the potential impact of high noise levels, or different speech patterns and accents, on transcription accuracy. Furthermore, ASA-24 offers pictures of portion sizes for users to select, while DataBoard does not have this feature and relied on participant reporting for portion sizes. Another notable limitation included participant struggles with the interfaces of DataBoard and ASA-24, encountering WiFi connectivity issues, limited familiarity with Zoom, and difficulty in navigating the two software despite thorough demonstrations. These barriers sometimes extended the timing of sessions, potentially influencing perceptions of the study as a whole. Participants may have also been influenced by the novelty of DataBoard or social desirability, given the innovative nature of voice-based tools. As older adults have varying levels of digital literacy, we highlight a need to address and educate on user-friendly interfaces in dietary assessments. Although the semi-structured interview protocol was adapted from validated frameworks, researcher reflexivity and confirmation bias may have influenced the conduct or tone of interviews. Coding for the ASR was done by a single research assistant, which is a limitation.
These findings suggest that while the voice-based recall tool was generally accessible and understandable, improvements in user interface and engagement duration may enhance its usability, allowing users to feel that voice-based recall is more accessible, especially when multitasking. In this pilot study, voice-based recall was perceived as easier than ASA-24, indicating that voice-based recall may be acceptable for short-term dietary assessment in older adults. This can greatly help researchers and practitioners who need to track dietary intake. With reliable dietary data, providers can implement interventions to prevent further decline in aging populations.
Future studies in VAS could focus on having improved and usable interfaces that are more intuitive to use. Expanding study populations to include a more diverse population would serve to create a more inclusive tool. Taking into account participant perspectives, modifying DataBoard to include tracking of users’ food categories consumed or how they felt about certain foods would provide more insightful details. Due to the large movement in technology in current healthcare, it is predicted that VAS can be integrated into mobile health applications. Both patients and providers can access such a wide array of data easily.
It is imperative that dietary recall assessments continue to evolve. Looking ahead, voice-based dietary assessment tools can be integrated into broader dietary surveillance or clinical workflows. This can reduce patient burden while offering easily accessible and real-time data collection. Voice-based tools may inform and enhance clinical care, care coordination, and an individual's healthy choices. Reliable dietary data informs public policy and initiatives on nutritional education and food accessibility. The population of older adults needs a dietary assessment tool that is accurate and easy to use. This is critical to identify, assess, and intervene in nutritional health concerns in our older adults.
Conclusions of the study
The findings from this study suggest that a voice-based recall system has significant potential to help improve dietary tracking for older adults who may struggle with memory or technological barriers. DataBoard's high acceptability and ease of use indicate that voice-based recall could serve as a viable alternative to the traditional web-based dietary assessments that often are technologically complex, require significant cognitive abilities, and take a long period of time.
The percentage of participants who expressed that they were willing to use DataBoard again was 65%, which, at a prototype stage, is acceptable. A majority of participants found it easy to answer the prompts about meal recall and understand the questions. DataBoard was rated highly for ease of use and acceptability for older adults, with lower scores in terms of being easier to perform when directly compared to ASA-24. However, using DataBoard was thought to be too long to sit through, indicating feelings of impatience. There was a high word error rate, indicating the transcripts of audio through DataBoard were only 63.5% accurate. This shows that DataBoard's ASR did not perform that well. This may limit feasibility in large-scale settings, as inaccuracies may require additional correction, reducing efficiency and diminishing user confidence. Further refinement of speech recognition, language processing algorithms, and accounting for background noises would be necessary to improve accuracy before widespread implementation. While the average response length was quite short, optimizing speech recognition and user interface design could subsequently enhance usability to allow for longer, detailed responses. This includes offering real-time feedback about responses, as confirmed to be recorded or anticipated troubleshooting prompts for common issues such as WiFi connectivity.
Our qualitative findings highlight further advantages and limitations of voice-based dietary recalls in using DataBoard for older adults. Several participants expressed that tracking their meals can be challenging because of memory issues or time constraints. Voice-based recall was thought to be a convenient alternative to ASA-24, as it was faster and more accessible to use. However, there were mixed feelings about the interface of DataBoard. Participants were sometimes unsure whether their responses were being recorded, frustrated that they could read prompts faster than DataBoard read them aloud, and confused about the pronunciation of certain words. Participants expressed potential for improving DataBoard through the incorporation of personalized tracking, like matching food groups and logging how they felt about what they ate. Utilizing a hybrid model of both voice-based and written components (like ASA-24) was suggested to improve dietary tracking overall. The findings from this study align with the broader goal of developing AI that can be applied to nutrition and other medical conditions.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251393342 - Supplemental material for Feasibility and usability of a voice-based dietary recall tool in older adults: A pilot comparison with ASA-24
Supplemental material, sj-docx-1-dhj-10.1177_20552076251393342 for Feasibility and usability of a voice-based dietary recall tool in older adults: A pilot comparison with ASA-24 by Simone G Khandpekar, Rishank Singh, Caroline E Summerour, Jim Schwoebel, Xiaohui Liang and John A Batsis in DIGITAL HEALTH
Footnotes
Abbreviations
ORCID iDs
Ethical considerations
The study was IRB approved (21-2034) by the University of North Carolina at Chapel Hill's Office of Human Subject Research.
Consent to participate
The study was conducted in the United States. Written informed consent was obtained from all participants.
Consent to publication
Not applicable.
Authors’ contributions
Khandpekar: Substantial contribution to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Singh: substantial contribution to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Summerour: substantial contribution to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Schwoebel: substantial contribution to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Liang: substantial contribution to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Batsis: Substantial contribution to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Nutrition Obesity Research Center (P30DK056350-23), the National Institute on Aging of the National Institute of Health (R01-AG- 067416) and University of North Carolina at Chapel Hill Center for Aging and Health.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This research was presented in part at the ObesityWeek 2024.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.