
Abstract
Objective
Digital literacy may be related to health behaviors, yet their associations remain less explored. This study examines the relationship between digital literacy and multidimensional health behaviors, including heterogeneous effects by gender, age group, and region. Furthermore, this study examines two mechanisms, drawing on self-determination theory and social capital theory.
Methods
We used data from the China Rural Revitalization Survey (CRRS). The relationships between digital literacy and health behaviors was examined via binary logistic regression models. Bias-corrected percentile bootstrap KHB mediation models investigated the mediating roles of life satisfaction and social capital.
Results
Digital literacy is positively and directly associated with all measured multidimensional health behaviors. The mediation analysis identified some significant indirect associations. Specifically, digital literacy is related to both physical exercise and physical examination through life satisfaction and relational social capital. Moreover, digital literacy is linked to dietary supplement intake through relational social capital and to physical examination and healthy diets through cognitive social capital. Heterogeneity analysis further revealed that digital literacy is more strongly associated with middle-aged adults’ physical examination, healthy diets, and dietary supplement intake, as well as males’ physical examination. Besides, stronger associations were found for residents in rural China's eastern and central regions, particularly for physical examination, healthy diets, and dietary supplement intake.
Conclusions
These findings offer theoretical insights into the relationships between digital literacy and multidimensional health behaviors and provide practical guidance for encouraging and fostering health behaviors.
Keywords
Introduction
The aging of the population is considered one of the most significant contemporary health and socioeconomic challenges. China has the largest number of older adults in the world and is one of the countries with the fastest aging rates. 1 Over the past few years, the proportion of the older Chinese population has increased from 6.96% in 2000 to 18.7% in 2020.2,3 While this proportion is lower than in some long-established aging societies such as Japan (28.7%) and Germany (21.7%) in 2020, 4 China's situation presents a unique challenge. The large absolute number of older adults places an enormous strain on healthcare services. Simultaneously, the rapid pace of aging profoundly impacts China's welfare and pension systems before the country has reached a high-income status. A prominent feature of China's population aging is the urban–rural inversion of the aging population, 5 indicating that the aging rate of the rural population is faster and more pronounced. According to the Seventh National Population Census of China, the proportion of people aged 60 years or older reached 23.81% in rural areas and 15.82% in urban areas. Moreover, rural middle-aged and older adults experience worse health outcomes and a higher prevalence of certain diseases compared to their urban counterparts. 6 The imbalanced population aging situation is accompanied by health disparities, making health concerns among middle-aged and older adults in rural areas an important issue. Therefore, urgent policy actions are needed to improve health and promote healthy aging among rural middle-aged and older populations.
Differences in health behaviors between urban and rural residents can partly explain the disparities in health outcomes.7,8 Health behavior is commonly defined as observable behavioral patterns, actions, and habits relating to maintaining, restoring, and improving health. 9 This includes behaviors such as smoking, alcohol use, diet, physical activity, sexual behaviors, doctor visits, medication adherence, screening, and vaccination. 10 These health behaviors play pivotal roles in influencing the health outcomes and well-being for both individuals and populations.11,12 These connections are particularly significant among middle-aged and older adults, as health behaviors are linked to declines in physical function in this demographic.13,14 Due to China's geographical location and hukou policies (the household registration system that categorizes citizens as either rural or urban, affecting their access to social services like healthcare and education), considerable disparities exist in health behaviors between rural and urban populations.15,16
In addition to health behaviors, the rapid development of internet technology and its application in promoting healthy aging in the digital era also provide new opportunities for health promotion among middle-aged and older adults in rural areas. In recent years, the steady advancement of digital information infrastructure construction in rural areas has led to a growth in the number of rural internet users. According to the latest 55th Statistical Report on Internet Development in China, the internet penetration rate in rural areas has reached 65.6%. 17 Fast-developing digital technology is an excellent channel for enhancing people's health investment because it offers significant potential to provide health information and resources.18,19 With the proliferation of the internet and mobile devices, digital health literacy has become a critical factor in accessing health information and resources. It is regarded as a “super determinant of health.” 20 In this context, super determinants refer to foundational factors that have implications for the wider social determinants of health and broadly influence health outcomes. 21
Digital literacy and health behaviors
In the digital age, the widespread influence of the internet on daily life has deeply extended into the realm of health, particularly for middle-aged and older adults. A comprehensive review of internet use among older adults highlights its positive associations with mental health, social connectedness, and access to health information. 22 Similarly, research conducted during the COVID-19 pandemic found that internet use was associated with better physical and mental health outcomes among older adults in Europe, particularly through access to online health resources and social support networks. 23 Digital services in healthcare and social welfare have also demonstrated high patient satisfaction. 24 Another study emphasized that whether older adults can access and utilize digital healthcare services will be key in assessing health equity. 25 Although these findings suggest that internet use and access to eHealth services are connected to older adults’ health outcomes, their digital literacy, in other words, how effectively they use these technologies, might be an even more important underlying factor.
The “digital divide” theory helps to conceptualize the link between digital literacy and health outcomes. This digital divide involves three levels: the first-level divide of physical access, the second-level digital divide related to differences in digital skills and literacy needed to use digital technology effectively, and the third-level divide of tangible outcomes. 26 Digital literacy is the central concept of this second-level divide. 27 However, its definition lacks a universal consensus, and its boundaries remain ambiguous. 28 Early conceptualizations, such as that pioneered by Gilster, 29 defined it narrowly as the skill set for processing digital information. Broader, more contemporary definitions, such as those by the United Nations Educational, Scientific, and Cultural Organization (UNESCO), expand this to encompass the multifaceted ability to securely and wisely utilize digital technology. Furthermore, recent scholarly work has underscored the importance of considering the unique characteristics of middle-aged and older adults when assessing their digital literacy.30,31 Therefore, integrating these perspectives, this study defines digital literacy as the fundamental operational ability of digital technology and the ability to access information resources effectively and utilize digital technologies in daily life.
Building upon this theoretical foundation, a growing but still limited body of research has explored the link between digital literacy (the second-level divide) and health behavior (the third-level divide). Early studies often employed simplistic proxies, such as device ownership or use, which limited their ability to determine the actual benefits of digital literacy. 32 A systematic review evaluating the use of digital literacy tools in existing studies found that current digital literacy assessment instruments targeting older adults have both strengths and weaknesses. 33 More recent and refined research offers clearer insights. For example, a survey conducted in Germany found that higher digital health literacy is weakly correlated with individuals’ specific behaviors, such as exercise routines, fruit consumption, and vegetable consumption, suggesting that these links may be complex. 34 In contrast, evidence from Korea has shown that older adults’ digital media literacy is positively correlated with their health-promoting behavior. 35 The latest study from Zhejiang Province in China revealed that digital literacy was notably and positively related to participation in digital health behaviors among rural residents. 36 Furthermore, a systematic meta-analysis revealed a moderate positive correlation between eHealth literacy and health-related behaviors, suggesting that eHealth literacy may mediate the association between health-related information and health-related behaviors. 37 These findings provide a solid foundation for exploring the links between digital literacy and multidimensional health behaviors among middle-aged and older adults in rural China.
In addition to evidence from China and high-income countries, experiences from other developing countries and regions highlight the potential of digital health interventions in low- and middle-income countries. For instance, digital interventions (including mHealth, eHealth, and telemedicine) for people living with non-communicable diseases in India have shown promising outcomes, such as improved self-management, increased communication between patients and healthcare providers, better adherence to medication, and reduced disease symptoms. 38 Similarly, primary care access (UBS + Digital Project) in Brazil has enhanced healthcare access in remote regions through teleconsultation. 39 In South Africa, mobile health interventions have substantially improved maternal and child health services. 40 These examples powerfully demonstrate the potential of digital health to improve outcomes in diverse low- and middle-income settings. However, the success of these interventions hinges on user engagement. As research has established, to engage effectively in digital health interventions, individuals need to possess the knowledge and skills to utilize information and communication technologies for health purposes.20,27 This highlights the critical role of digital literacy, which is foundational to understanding the link between digital interventions and health behaviors.
Despite these advances, most related research has been conducted in developed countries, such as Korea, and has focused primarily on the direct association between digital literacy and health behaviors. Digital literacy may be indirectly related to health behaviors through intermediary variables, and the underlying mechanisms have been less explored. Furthermore, prior studies on health behaviors have predominantly focused on everyday practices, including smoking, drinking, and exercise; this narrow lens overlooks the complex, multidimensional nature of health behaviors. Research that considers dietary habits and supplements, which robustly reflect individual health behaviors, 13 remains limited. This study aims to address these gaps by exploring the complex pathways connecting digital literacy to multidimensional health behaviors among middle-aged and older adults in rural China.
Mediating role of life satisfaction
Life satisfaction, which refers to a cognitive global evaluation of one's life, has been identified as an essential indicator of older adults’ subjective well-being. 41 A growing body of empirical research is emerging on the impact of internet adoption and use on general individual well-being and life satisfaction. Most studies have emphasized the positive association between internet use and life satisfaction, as well as the relationship between digital literacy and life satisfaction. Compared to those who did not use the internet, older adults who used the internet reported higher levels of life satisfaction. 42 Seeking information via smartphones may help improve life satisfaction by providing the necessary information on important areas of life, such as health and finances. 43 Research on older Korean adults also supports the finding that digital literacy is positively related to older adults’ life satisfaction.35,44 However, some studies presented different findings. A study found that internet use was negatively related to older adults’ life satisfaction because it reduced their perceptions of social justice. 45 Additionally, problematic social media use was also negatively linked to life satisfaction, 46 while others have noted no association at all for women living alone. 47 Although the relationship between internet use or digital literacy and life satisfaction shows mixed results, the specific link between digital literacy and life satisfaction is less studied. Given the potential for adverse outcomes from internet use, it is important to understand whether digital literacy can serve as a protective factor for middle-aged and older adults.
Self-determination theory (SDT) posits that humans have inherent potential for self-realization, which is unique and guides the transformation of behavior toward positive and upward development. 48 SDT suggests that satisfying users’ basic psychological needs fosters greater autonomous motivation. 49 According to this theory, individuals have three basic psychological needs that they desire to fulfill: competence (feeling proficient in their actions), autonomy (the freedom to choose their actions), and relatedness (experiencing acceptance and recognition). Competence and autonomy directly promote the change in and maintenance of health behaviors. 50 Furthermore, the three needs appear to be closely correlated with life satisfaction. 51 Individuals who have experienced autonomy, competence, and relatedness are likely to be more satisfied with their lives than those who have not experienced these psychological needs. 52 As digital literacy improves, individuals can more easily and effectively acquire and use necessary information about daily life, such as health information and resources, which can meet individuals’ needs for autonomy and competence, thus improving their life satisfaction.53,54 Therefore, from a theoretical standpoint, a higher level of digital literacy enhances an individual's life satisfaction by fulfilling psychological needs, boosting autonomous motivation, and facilitating health behaviors.
Previous empirical studies have emphasized that life satisfaction was positively related to health behaviors. Individuals with higher levels of life satisfaction tend to have greater confidence in their ability to engage in health behaviors. 55 Several studies have revealed the associations between life satisfaction and health behaviors. One study examined the relationship between life satisfaction and health behaviors among young adults across different cultures and reported positive associations with health behaviors. 56 Considering the connection between digital literacy and life satisfaction, as well as the connection between life satisfaction and health behaviors, life satisfaction may serve as a mediating factor in the relationships between digital literacy and health behaviors. In other words, digital literacy may be associated with health behaviors through an indirect association with life satisfaction.
Mediating role of social capital
Social capital refers to the connections and interactions between people and groups. It can be understood and measured at either a collective or individual level. 57 At the individual level, social capital is often viewed as a personal resource derived from social networks, enabling individuals to access resources, favors, information, or support from their connections more effectively. 58 In this study, we examined social capital at the individual level because individuals’ health and health behaviors are more likely influenced by their personal-level social capital. 59 Additionally, our focus is on the relational and cognitive dimensions of social capital, 60 which are important for health.61-63 However, these dimensions are less studied in the literature compared to structural social capital.64,65 The former relates to objective measures of available resources in a person's interpersonal environment; 66 the latter is measured through subjective indicators, such as trust, belongingness, and reciprocity.67,68
Social capital theory (SCT) highlights that social capital can improve social support and informal social control, strengthening individuals’ identification with mainstream values and reducing deviant behaviors. 69 From the perspective of relational social capital, a higher level of relational social capital means more social relationships that provide access to resources and support. 66 Middle-aged and older adults with higher levels of relational social capital often have larger social networks and more resources to help them adopt health behaviors.63,70 Regarding cognitive social capital, social trust is positively linked to health behaviors.71,72 Middle-aged and older adults with higher levels of social trust tend to keep closer contact with those around them, share more activities, spend more time together, and are more likely to improve their health practices through peer norms and modeling habits.73,74 Relational and cognitive social capital represent the quantity and quality of social relationships, respectively, providing middle-aged and older adults with various forms of social support that are related to their health behaviors.75-77
In the digital era, digital development has transformed the traditional social capital structure in rural areas. As a system of skills and strategies employed in a digital environment, 78 digital literacy significantly strengthens an individual's social communication, broadens their social networks, and thereby increases their social capital.79,80 This mechanism is particularly evident in specific populations, such as middle-aged and older adults. Studies revealed that greater digital literacy enables them to use technology to overcome the time and spatial restrictions of traditional socializing, which not only increases opportunities for social participation 81 but also helps them access a broader array of social resources 82 and accumulate substantial online social capital. 83 Crucially, this online capital can further facilitate the consolidation and accumulation of offline social capital. 84 Considering this positive connection between digital literacy and social capital, combined with the aforementioned association between social capital and health behaviors, social capital may play a mediating role in the relationships between digital literacy and health behaviors.
Present study
The relationships between digital literacy and health behaviors among middle-aged and older adults in rural China remain underexplored, particularly concerning the underlying mechanisms. Clarifying these associations and their pathways is crucial for developing effective strategies to promote healthy aging in an era of rapid digitalization. To address this gap, this study integrates SDT and SCT to propose a comprehensive model (see Figure 1). We hypothesize that digital literacy is associated with the health behaviors of middle-aged and older adults not only directly, but also indirectly through the mediating roles of life satisfaction and social capital. Specifically, in this study, we aims to address the following research questions:
Is digital literacy associated with health behaviors? Do these associations vary by gender, age, or region? Does life satisfaction mediate the associations between digital literacy and health behaviors? Does social capital (relational and cognitive) mediate the associations between digital literacy and health behaviors?
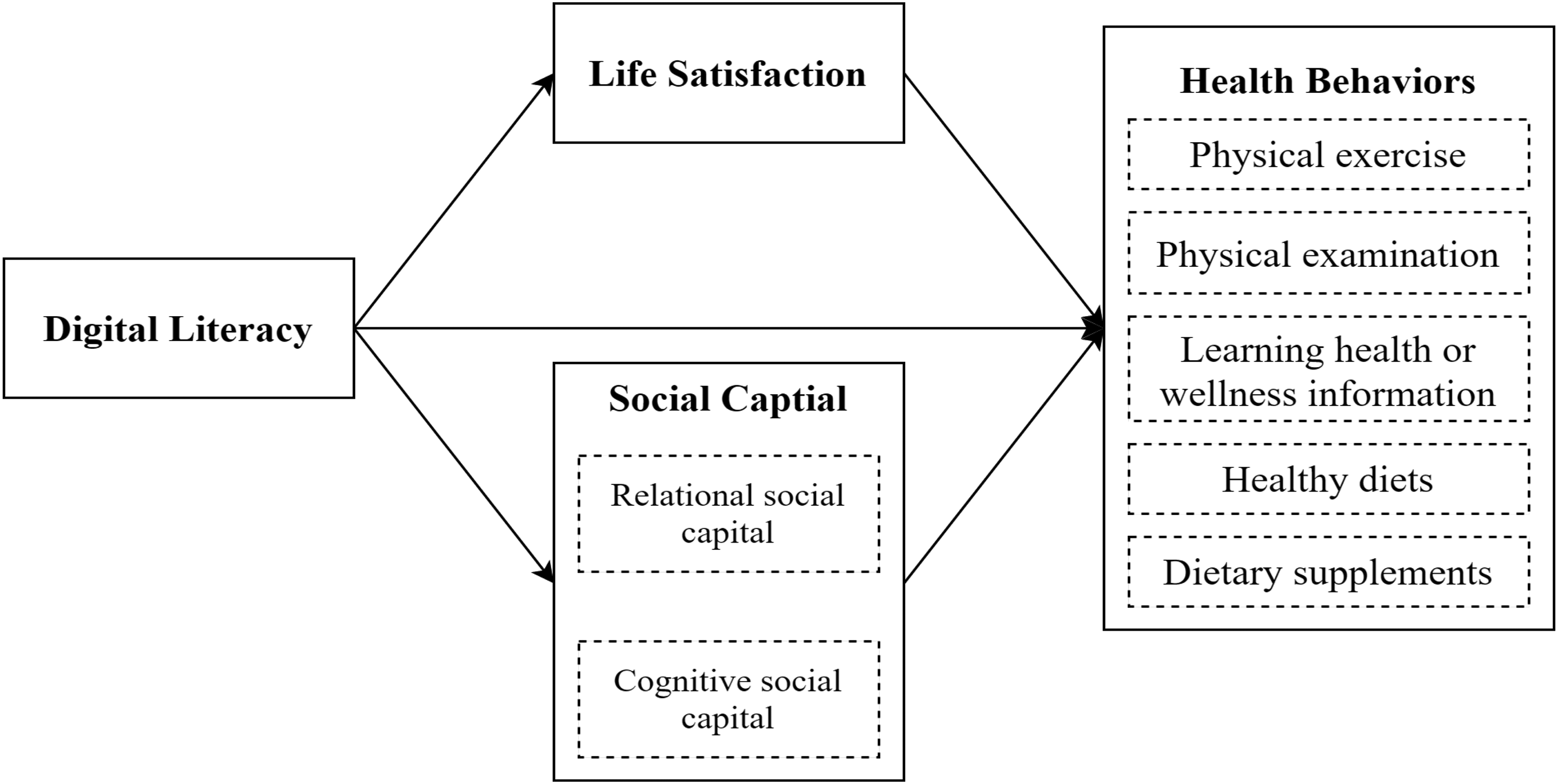
Conceptual model.
Methods
Sample and produce
We used data from the China Rural Revitalization Survey (CRRS) conducted by the Rural Development Institute, Chinese Academy of Social Sciences, from August to September 2020, covering 10 provinces (autonomous regions): Guangdong, Zhejiang, Shandong, Anhui, Henan, Heilongjiang, Guizhou, Sichuan, Shaanxi, and Ningxia Hui Autonomous Region. A multistage stratified random sampling approach was employed to get the samples, considering economic development, spatial distribution, and agricultural production. Provinces were selected by random sampling, resulting in 10 provinces. Within each province, counties were stratified by per capita Gross Domestic Product (GDP) into five groups (high, medium–high, medium, medium–low, and low), with one county randomly selected from each group to ensure spatial coverage, resulting in a total of 50 counties. Townships were stratified by per capita GDP into three groups (high, medium, and low), with one township randomly selected from each group per county, taking into account location and industrial layout, for a total of 150 townships. Villages were stratified into two groups (better and poorer economic development), with one village randomly selected from each group, considering location and industrial layout, resulting in 300 villages. From each village, 14 households were randomly selected from residency rosters provided by village committees, totaling 4200 households.
The survey encompasses a comprehensive range of topics, including agricultural production, rural development, farmer livelihoods, and social welfare, collectively providing a solid representation. The survey was primarily conducted through one-on-one interviews, with each questionnaire taking approximately 1.5 h to complete. To ensure data quality, investigators underwent rigorous training, and surveys were limited to four per investigator daily, with three rounds of quality checks (self-review, peer cross-check, and team leader review) to maintain high reliability and representativeness. Finally, the survey data encompass 300 villages and 3833 household survey questionnaires. The survey achieved a response rate of 91.26%. We restricted the analytic sample to individuals aged 45 years or older in the 2020 survey. We further screened the sample by conducting rigorous data cleaning to address outliers and missing values. Finally, 2728 middle-aged and older adults were included in our study.
Measures
Multidimensional health behaviors
Combined with the accessibility of data and drawing lessons from existing research,10,63 five indicators (physical exercise, physical examination, learning health or wellness information, healthy diets, and dietary supplement intake) represented by seven questions were selected as proxy variables for multidimensional health behaviors.
Physical exercise was measured as “Have you engaged in any physical exercise or fitness activities for thirty minutes or longer within the past week?” Those who met the criterion were coded as 1; otherwise, they were coded as 0.
Physical examination refers to routine health check-ups, typically including clinical assessments such as blood pressure measurement, blood tests, and other health screenings. In rural areas, individuals can choose either a private physical examination (conducted individually, e.g., at clinics) or a community-based physical examination (group screenings at the village level, such as at local health service centers). Therefore, the physical examination was measured by the question, “Have you undergone a physical examination within the past year?” The original coding for physical examination in the survey was as follows: 1 = participation in a private physical examination, 2 = participation in a collective physical examination, and 3 = no physical examination. The physical examination variable was dichotomized as “1,” indicating participation in any physical examination, and “0,” indicating no participation.
Learning health or wellness information was measured by the question, “Do you consciously learn health or wellness information?” Those who consciously learned health or wellness information were coded as “1” and “0” otherwise.
Healthy diets were measured by three questions: “Do you consciously control sugar intake?” “Do you consciously control salt intake?” and “Do you consciously control edible oil intake?” The study coded the variable as a dichotomous one, labeling respondents who were controlling for either “sugar intake,” “salt intake,” or “edible oil intake” as “1,” and if respondents did not control for any of these variables, they were assigned “0.”
Dietary supplements refer to the consumption of products (e.g., pills), such as vitamins, minerals, or herbal supplements, taken to address nutrient deficiencies that may not be sufficiently obtained through food alone. It was measured by the question, “Do you consume dietary supplements daily?” Participants who consumed dietary supplements in daily life were coded as “1” or “0” otherwise.
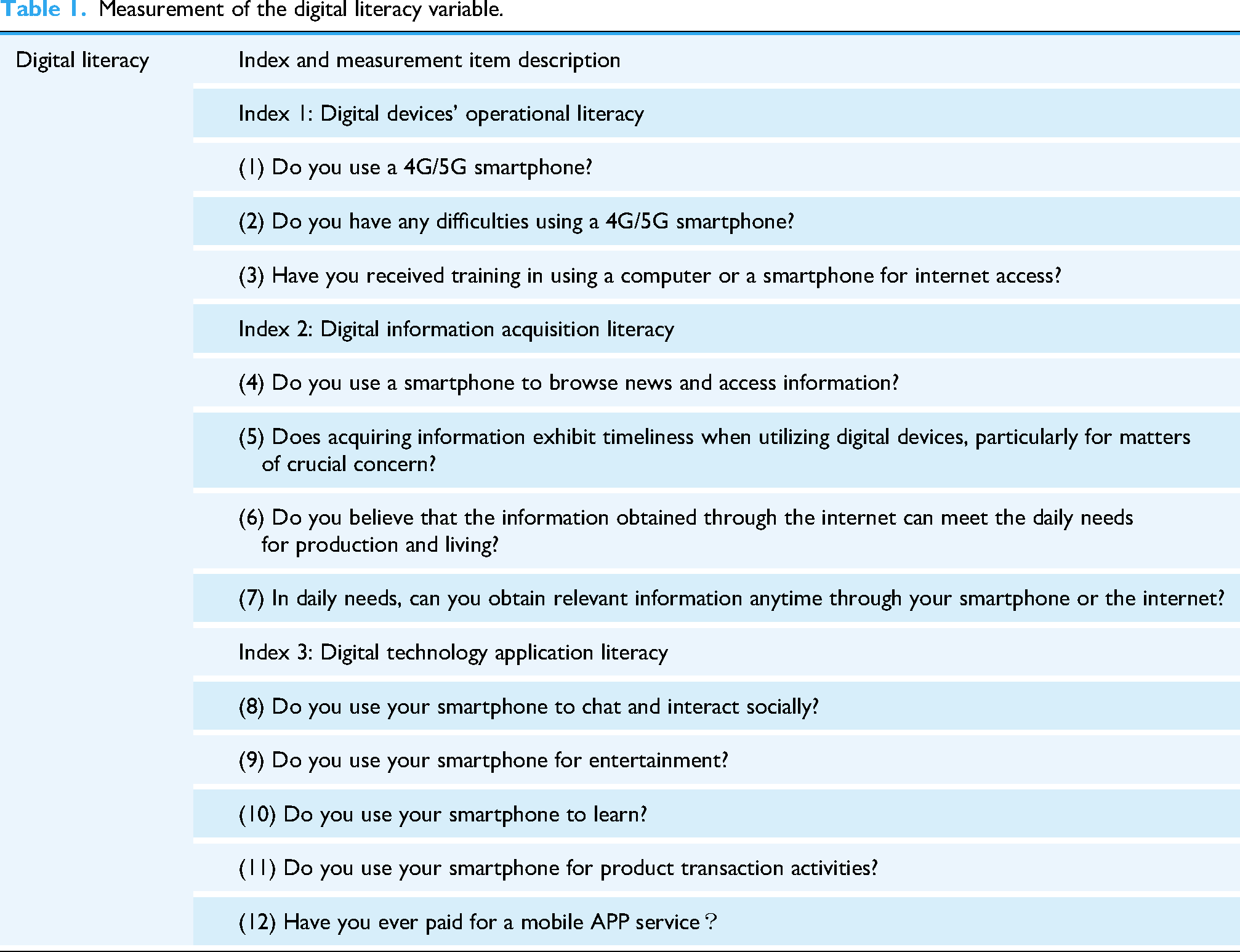
Digital literacy
The measurement of digital literacy in this study follows the Digital Competence Framework for Citizens by the European Union in 2022 (the DigComp 2.2), which combines measurement indicators from previous studies.85,86 We construct a comprehensive evaluation indicator system for the digital literacy of middle-aged and older adults in rural areas.
The digital literacy indicator system encompasses three dimensions: digital device operational literacy, digital information acquisition literacy, and digital technology application literacy. Digital device operational literacy refers to the accessibility of digital devices to middle-aged and older adults. This paper measures this literacy by assessing whether middle-aged and older adults use digital devices, the difficulty they experience using digital devices, and whether they have received training in using mobile phones or computers. Digital information acquisition literacy refers to the ability of middle-aged and older adults to search for, identify, acquire, and utilize information from the internet to solve real-world problems. This study evaluates this ability by examining the proficiency with which older adults use digital devices to access information, whether they utilize smartphones to obtain information resources, and the availability and timeliness of digital information. Digital technology application literacy refers to the adoption behavior of middle-aged and older adults toward digital technologies. This study assesses this literacy by examining whether middle-aged and older adults possess proficient skills in digital entertainment, social interaction, digital learning, and digital commerce, and whether they have paid for digital software.
This study selected 12 specific items through the survey questionnaire. All the answers “Yes” were assigned a value of 1, and “No” were assigned a value of 0. Given the complexity of digital literacy, this paper follows previous methods 85 and employs principal component analysis (PCA) to extract key information from various dimensions of digital literacy. PCA is a method that succinctly extracts the most important features from complex data. The largest principal component contains the richest information from the raw data and has the strongest data interpretability. Consequently, we can compress the information from three dimensions of digital literacy into a composite index.
The samples were assessed via the Kaiser‒Meyer‒Olkin (KMO) test and Bartlett's sphericity test. The KMO value was 0.721 > 0.7, and the p-value of Bartlett's test was 0.000, indicating that the sample data were suitable for PCA. After PCA, we obtained a total digital literacy score ranging from 1 to 10. Higher scores indicate greater digital literacy. The specific descriptions of the 12 items are shown in Table 1. The detailed eigenvalues, variance explained, and factor loadings for all components are provided in Supplementary Tables S1 and S2 for comprehensive review.
Measurement of the digital literacy variable.
Life satisfaction
In the CRRS questionnaire, life satisfaction is measured by a single item: “How satisfied are you with your life, in general, these days?” It was measured using a 5-point Likert scale (1 = not at all satisfied to 5 = very satisfied); higher scores indicate greater life satisfaction. This simple measurement has been confirmed to have high validity and reliability.44,53
Social capital
In the Chinese sociocultural context, social capital refers to the network of social relationships that are fundamentally rooted in close ties among family members, extended relatives, neighbors, and fellow townspeople. 87 Therefore, we classify social capital into relational social capital and cognitive social capital based on Nahapiet and Ghoshal's 60 categorization of social capital and consider the questionnaire in the CRRS survey.
Following previous studies,88-90 we have chosen the “borrowing money network size” as a measurement of relational social capital. In rural China, the “acquaintance society” is defined by robust kinship and geographical ties, which foster a pervasive culture of mutual support among relatives and friends. 87 The scale of an individual's borrowing money network is a significant indicator of the abundance or scarcity of their relationship between social capital and social resources.91,92 Specifically, in the CRRS questionnaire, the question “How many relatives and friends can lend you RMB 5000 (approximately $720) or above?” was utilized to measure the relational social capital among middle-aged and older adults. A larger size of the borrowing money network means more affluent social capital.
Following Chen and Zhou's approach, 93 cognitive social capital was measured by the sense of trust. This measurement approach has demonstrated good reliability and validity among Chinese rural residents. 64 Specifically, in the CRRS questionnaire, participants were asked, “Do you think the people around you are trustworthy?” The answers were assessed by a 5-point Likert scale (1 = very trustful, 3 = neutral, 5 = very distrustful). We reverse-encoded the options for better understanding: 5 for very trustful and 1 for very distrustful.
Control variables
Several covariates identified in the literature as relevant to digital literacy and health behaviors are used as controls. Among the demographic factors, we include age (a continuous variable), age-squared, gender (1 for male, 0 for female), marital status (1 for married or partnered, 0 for otherwise), and the highest educational level (below the elementary school, elementary school, middle school, and high school and above). Among the family factors, we include family member size (a continuous variable) and household income (logarithmic). Among the health factors, we include chronic disease status (1 for individuals suffering from chronic conditions, 0 for those not suffering from chronic conditions) and disabled status (0 for individuals not disabled, 1 for those who are disabled). Among the social security factors, we include pension insurance (1 for having pension insurance, 0 for no pension insurance) and medical insurance (the number of family members with medical insurance, a continuous variable).
Analytic strategy
The analyses proceed in four stages. First, we performed descriptive statistics on the sample and presented the relationships between digital literacy and health behaviors among middle-aged and older adults by calculating correlation coefficients. Second, five binary logistic regression models were constructed to examine the associations between digital literacy and health behaviors of middle-aged and older adults. Odds ratios (ORs) with 95% confidence intervals (CIs) were used to analyze the relationships between digital literacy and health behaviors. All control variables were included in the five models. Based on existing literature suggesting that the relationships between age and health behaviors may be non-linear, 94 we included both a linear (age) and a quadratic (age-squared) term for age in our logistic regression model. This approach allows the model to capture a potential U-shaped or inverted U-shaped effect of age, thereby providing a more accurate estimation of the main effect of digital literacy by appropriately controlling for the confounding influence of age. Third, in the heterogeneity analysis, we employed Fisher's permutation test to compare the differences in coefficients between different groups for gender, age, and regional areas, which is a non-parametric test and maintains validity under sample size imbalances.95,96 Fourth, to further explore the mediating effect of life satisfaction and social capital on the relationship between digital literacy and health behaviors, using the Karlson–Holm–Breen (KHB) method of mediation for binary outcomes, 97 this study adopted a bias-corrected percentile bootstrap method to test the mediating, valid, and robust effect of life satisfaction and social capital by setting Model 6–10. In this study, all analyses were performed using STATA 17.
Results
Descriptive statistics
A descriptive analysis of all variables is presented in Table 2 (n = 2278). The mean digital literacy score was 3.22 (SD = 1.56), indicating that middle-aged and older adults’ digital literacy was low. The average life satisfaction score was 4.09 (SD = 0.82), the mean value of relational social capital was 7.05 (SD = 8.02), and the average cognitive social capital score was 4.22 (SD = 0.76). These results revealed higher life satisfaction and cognitive social capital but lower relational social capital among middle-aged and older rural adults. Concerning the five specific health behaviors, 60.71% of the participants engaged in physical exercise. The proportion of those who had undergone physical examination in the past year was 65.67%. A total of 48.07% of the respondents consciously learned health or wellness information. Over half of the respondents (68.70%) consciously maintained healthy diets. Only 13.26% of the respondents consumed dietary supplements.
Descriptive statistics of the participants.
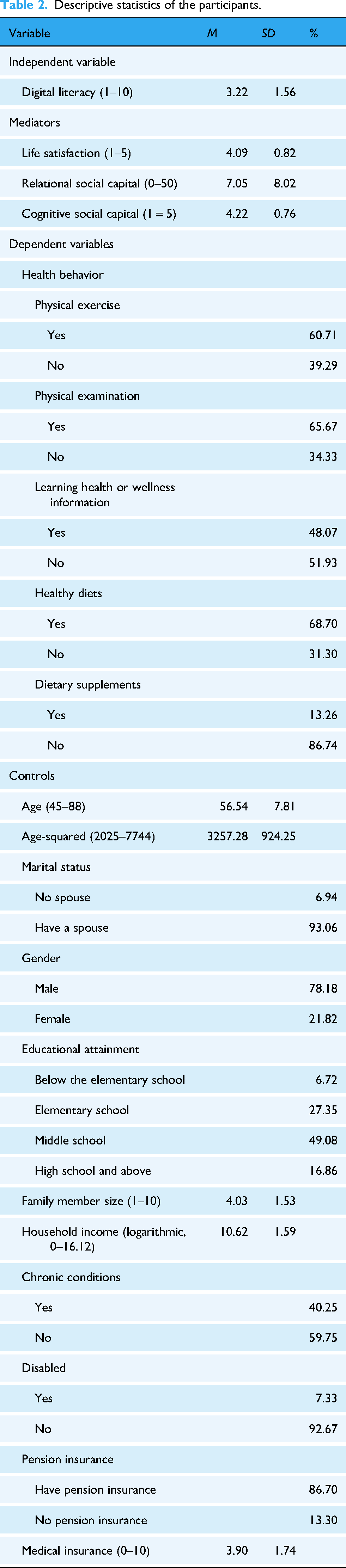
Regarding the control variables, the mean age of the sample was 56.54 years (SD = 7.81), and 93.06% of the participants had a spouse. The majority of the sample (78.18%) was male. Among all respondents, 6.72% had not completed elementary education, 27.35% had completed elementary school education, 49.08% had completed middle school education, and 16.86% had completed high school education and above. The mean value of family member size was 4.03 (SD = 1.53), and the mean value of the number of family members with medical insurance was 3.90 (SD = 1.74). This result suggests that our sample was relatively active in participating in medical insurance. The proportion of those who met the disability criterion was 7.33%, and 40.25% of the sample had chronic conditions. The average value of the logarithm of family income was 10.62 (SD = 1.59), indicating that middle-aged and older adults’ family income is relatively lower.
Correlative statistics
Table 3 presents the Pearson correlation coefficients among key variables, showing that digital literacy is significantly correlated with most health behaviors, except for physical examination. All five types of health behaviors are significantly and positively connected. Additionally, digital literacy has significant and positive correlations with life satisfaction, relational social capital, and cognitive social capital. Both life satisfaction and relational social capital are significantly and positively correlated with most health behaviors, except for dietary supplement intake. Cognitive social capital significantly and positively correlates with most health behaviors, except for physical examination. Furthermore, life satisfaction, relational social capital, and cognitive social capital are significantly and positively correlated.
Correlation analysis for the core variables.

Note. DL: digital literacy; PEXE: physical exercise; PEXA: physical examination; LHWI: learn health or wellness information; HD: healthy diets; DS: dietary supplements; LS: life satisfaction; RSC: relational social capital; CSC: cognitive social capital.
p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001.
Logistic regression results
Table 4 presents the regression results for the associations between digital literacy and health behaviors, controlling for confounders. Models 1–5 explore the relationships between digital literacy and different health behaviors, respectively. Model 1 showed that digital literacy was significantly and positively associated with the odds of participating in physical exercise (OR = 1.140, p < 0.001, 95% CI [1.072–1.213]). Similarly, in Model 2, digital literacy was significantly and positively correlated with the odds of undergoing physical examination (OR = 1.108, p = 0.002, 95% CI [1.038–1.182]). Model 3 revealed a significant positive relationship between digital literacy and the odds of learning health or wellness information (OR = 1.208, p < 0.001, 95% CI [1.136–1.285]). With respect to Model 4, digital literacy was significantly and positively linked to the odds of adopting healthy diets (OR = 1.115, p = 0.002, 95% CI [1.043–1.192]). Finally, in Model 5, digital literacy was found to have a significant positive association with the odds of dietary supplement intake (OR = 1.133, p = 0.005, 95% CI [1.039–1.236]).
Logistic regressions of digital literacy on health behaviors.

Note. 95% CI values are given in parentheses. PEXE: physical exercise; PEXA: physical examination; LHWI: learn health or wellness information; HD: healthy diets; DS: dietary supplements; OR: odds ratio; Ref.: reference category; CI: confidence interval.
*p < 0.05, **p < 0.01, ***p < 0.001.
For the control variables, the odds of adopting healthy diets (OR = 0.784, p = 0.041, 95% CI [0.622–0.989]) were higher for females than for males. The relationship between age and physical examination was found to be non-linear and statistically significant. While increasing age was associated with lower odds of taking physical examination (OR = 0.758, p < 0.001, 95% CI [0.638–0.900]), the significant positive OR for age-squared (OR = 1.003, p < 0.001, 95% CI [1.001–1.004]) confirmed a non-linear association. This suggests that an initial decrease in the odds of taking physical examination as age increases, followed by an increase at older ages (U-shaped curve). At the same time, although the coefficient for age and learning health or wellness information is not significant, age-squared showed a significant positive OR (age-squared OR = 1.001, p = 0.044, 95% CI [1.000–1.002]). This indicates that the overall linear relationship between age and learning health or wellness information is weak. However, a significant U-shaped relationship suggests that the odds of learning health or wellness information increase with age. High school and above educational level was significantly and positively associated with participating in physical exercise (OR = 1.963, p < 0.001, 95% CI [1.311–2.939]), taking physical examination (OR = 2.234, p < 0.001, 95% CI [1.467–3.403]), learning health or wellness information (OR = 2.757, p < 0.001, 95% CI [1.823–4.170]), and adopting healthy diets (OR = 2.498, p < 0.001, 95% CI [1.623–3.845]). However, educational attainment was not significantly associated with dietary supplement intake. A higher level of household income was significantly and positively associated only with taking physical examination (OR = 1.086, p = 0.006, 95% CI [1.026–1.151]). Furthermore, having a chronic disease was significantly and positively associated with odds of engaging in physical examination (OR = 1.370, p = 0.001, 95% CI [1.135–1.654]) and adopting healthy diets (OR = 1.685, p < 0.001, 95% CI [1.388–2.046]). Individuals with disabilities had lower odds of participating in physical exercise (OR = 0.553, p < 0.001, 95% CI [0.400–0.764]). Pension insurance was significantly and positively associated with taking in physical examination (OR = 1.772, p < 0.001, 95% CI [1.371–2.290]), learning health or wellness information (OR = 1.421, p = 0.008, 95% CI [1.099–1.836]), and adopting healthy diets (OR = 1.562, p < 0.001, 95% CI [1.204–2.027]). Compared with western region, middle-aged and older adults in the central region were significantly less likely to undergo physical examination (OR = 0.671, p < 0.001, 95% CI [0.543–0.829]). In contrast, those in the eastern region showed higher odds of adopting healthy diets (OR = 1.563, p < 0.001, 95% CI [1.234–1.981]) and dietary supplement intake (OR = 1.492, p < 0.001, 95% CI [1.116–1.994]) than individuals in western region.
Heterogeneity results
We further investigate whether the aforementioned associations vary by gender, age, and region. In line with the definition of middle-aged and older adults recommended by the World Health Organization (WHO) and Chinese legal regulations, we further categorize middle-aged adults as those aged 45–59 years (n = 1574, 69.1%) and older adults as those aged 60 years and above (n = 704, 31.9%) in this study. According to previous studies98,99 and the National Bureau of Statistics of China, this study divides the samples into three regions: the eastern (n = 616, 27.1%), central (n = 713, 31.3%), and western (n = 949, 41.6%) regions.
Table 5 presents the grouped regression results for digital literacy and health behaviors, controlling for covariates. This study further employs Fisher's permutation test to investigate the differences in coefficients across different groups when the coefficients are significant within each group. In terms of gender heterogeneity, digital literacy showed stronger associations with health behaviors in males than females, specifically for participating in physical examination (OR = 1.118, p = 0.004, 95% CI [1.037–1.205]) and dietary supplement intake (OR = 1.132, p = 0.018, 95% CI [1.022–1.254]). Compared to older adults, middle-aged adults exhibited stronger associations between digital literacy and participating in physical examination (OR = 1.105, p = 0.003, 95% CI [1.025–1.192]), adopting healthy diets (OR = 1.146, p = 0.009, 95% CI [1.057–1.243]), and dietary supplement intake (OR = 1.212, p < 0.001, 95% CI [1.088–1.350]). Regarding regional heterogeneity, digital literacy was more strongly associated with middle-aged and older adults’ participation in physical examination in the central region (OR = 1.175, p = 0.004, 95% CI [1.054–1.310]) and with adopting healthy diets in the eastern and central regions (eastern: OR = 1.150, p = 0.032, 95% CI [1.019–1.295]; central: OR = 1.162, p = 0.010, 95% CI [1.036–1.303]), as well as dietary supplement intake in the eastern region (OR = 1.171, p = 0.038, 95% CI [1.009–1.359]).
Heterogeneity analysis of the effects of digital literacy on health behaviors.

Note. 95% CI values are given in parentheses. PEXE: physical exercise; PEXA: physical examination; LHWI: learn health or wellness information; HD: healthy diets; DS: dietary supplements; OR: odds ratio; Ref.: reference category; P: p-value of differences in coefficients across different groups; CI: confidence interval.
*p < 0.05, **p < 0.01, ***p < 0.001.
Mediation results
The mediating effects of life satisfaction and social capital on the relationships between digital literacy and health behaviors were tested using the KHB method, with 95% CIs estimated via a bias-corrected percentile bootstrap approach (5000 repetitions). The detailed results are presented in Table 6 and visualized in Figure 2.
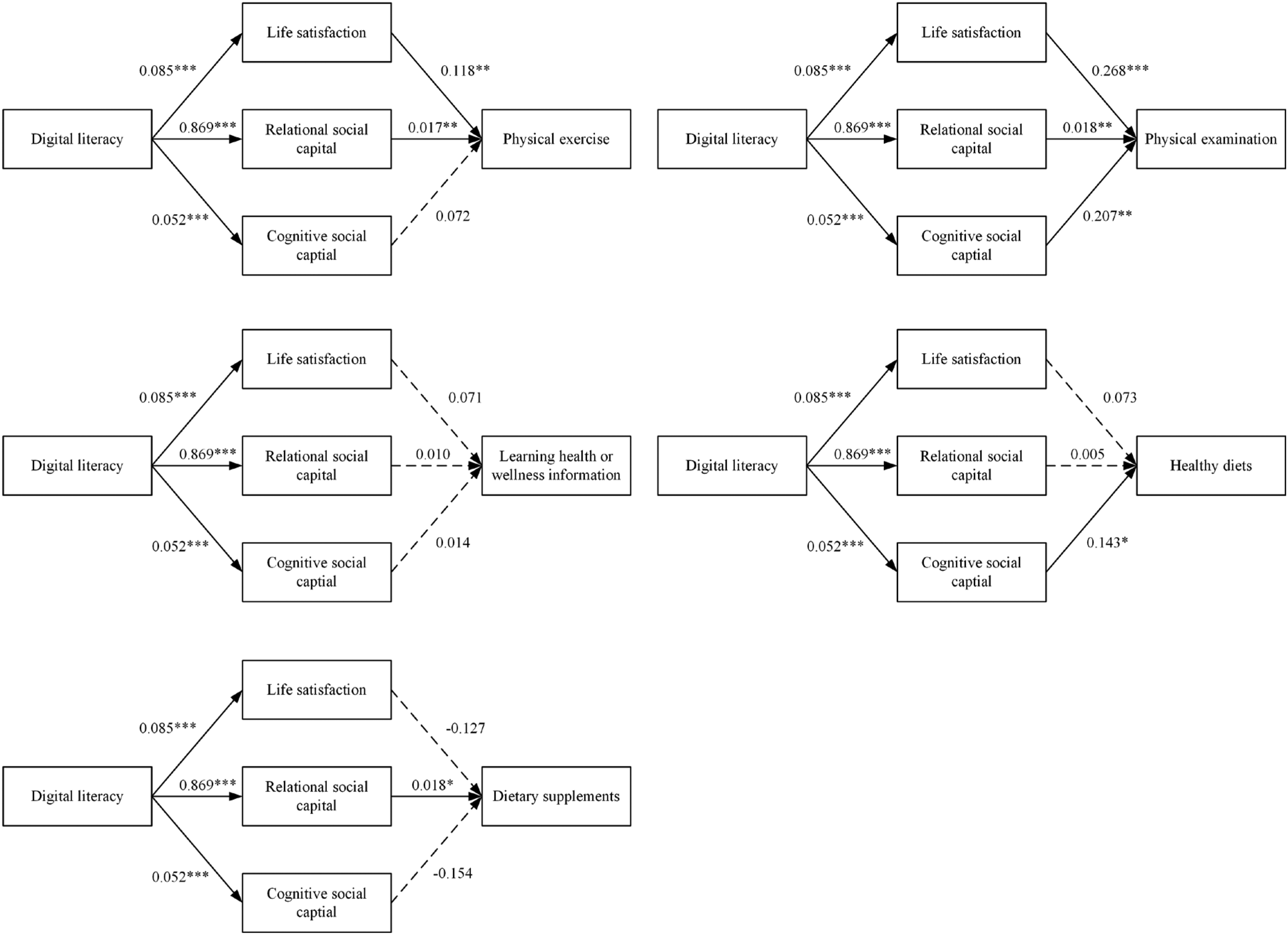
The results of the mediation analysis.
Indirect effects of life satisfaction, relational social capital, and cognitive social capital.

Note. Indirect effects were unstandardized. Boot SE: bootstrap standard error; LLCI: lower limit confidence interval; ULCI: upper limit confidence interval; PEXE: physical exercise; PEXA: physical examination; LHWI: learn health or wellness information; HD: healthy diets; DS: dietary supplements.
*p < 0.05, **p < 0.01.
Across Models 6–10, the bootstrap 95% CIs revealed varying mediating effects of life satisfaction, relational social capital, and cognitive social capital on relationships between digital literacy and health behaviors. Specifically, in Model 6, the mediating roles of life satisfaction and relational social capital were significant, whereas the mediating effect of cognitive social capital was not significant. In Model 7, all three mediators showed significant mediating effects on the relationship between digital literacy and participation in physical examination. Conversely, Model 8 indicated that the indirect effects for all three mediators on the relationship between digital literacy and learning health or wellness information were insignificant. In Model 9, only cognitive social capital had a significant mediating effect on the relationship between digital literacy and the adoption of healthy diets. In Model 10, only relational social capital significantly mediated the relationship between digital literacy and dietary supplement intake. These findings highlight the context-specific roles of these mediating mechanisms.
Discussion
Principal results
Based on a probability-based sample from the 2020 CRRS, this study employed the binomial logistic regression model to investigate the relationships between digital literacy and multidimensional health behaviors among middle-aged and older adults in rural China. The mediating roles of life satisfaction and social capital were also examined. Our results indicated that digital literacy was positively associated with multidimensional health behaviors. However, due to the cross-sectional design of this study, causality cannot be established. Additionally, we found that life satisfaction and social capital partially mediated these associations. These findings may contribute to the design of improvement strategies to improve the health behaviors of middle-aged and older adults in the context of the rapid development of the digital era.
First, digital literacy is positively and significantly associated with multidimensional health behaviors. Individuals with higher digital literacy are better able to obtain, analyze, and integrate health-related information. They tend to be more aware and are more likely to engage in health behaviors. This finding partly supports previous research on the links between digital literacy and health behaviors.34,36 However, most earlier studies have concentrated on one aspect of this relationship, such as digital media literacy and health-promoting behavior 35 or digital health literacy and health behaviors, 34 making it hard to understand the full association between digital literacy and multidimensional health behaviors. Using a probability-based sample, our study developed a digital literacy index for this demographic and substantiated the significant positive associations between digital literacy and health behaviors, thereby providing more robust and dependable empirical evidence for these associations. In addition, previous research often centered on common health behavior indicators such as smoking, drinking, and dietary habits. 34 In contrast, this study included a broader and more representative set of health behavior indicators, such as participating in physical examination, engaging in physical exercise, and learning about health or wellness information. Nonetheless, the current digital literacy levels among middle-aged and older adults in rural China remain relatively low, which likely suppresses the empowering effect of digital literacy on health behaviors. Therefore, policymakers should develop targeted strategies to enhance the digital literacy of middle-aged and older adults, thereby improving their health behaviors and promoting healthy aging. These strategies could include increasing access to internet devices (e.g., providing government subsidies for purchasing smartphones and reducing the costs of internet access services for rural residents); enhancing their skills to use the internet (e.g., conducting community-based training programs, promoting peer-to-peer teaching, supporting family-based tutoring, and adopting task-oriented learning approaches); and strengthening the ecosystem of internet-enabled services (e.g., expanding broadband infrastructure in rural areas, encouraging internet service providers to create age-friendly interfaces, and developing user-friendly health applications).
Second, the heterogeneity results indicate that the associations between digital literacy and health behaviors vary across different genders, age groups, and regions. Specifically, digital literacy has stronger associations with males’ physical examination and dietary supplement intake. This may be because males’ digital literacy is relatively higher than females, and the gap is more pronounced among older groups. 100 Concerning age, digital literacy is more significantly related to middle-aged adults’ physical examination, healthy diets, and dietary supplement intake. This may be related to lower digital literacy levels among older adults. In contrast to their younger counterparts, older adults are not “digital natives” and typically have less exposure to modern digital technologies throughout their careers and daily routines, as these technologies were less widespread during their formative years. 101 Consequently, older adults often exhibit lower internet-related skills compared to younger adults.31,102 Additionally, the associations between digital literacy and health behaviors vary significantly across regions. For example, digital literacy shows stronger associations with healthy diets among middle-aged and older adults living in central and eastern areas, and it has a significant relationship only with dietary supplement intake among middle-aged and older adults in the eastern region. These differences can be attributed to the considerable disparity in the economic development of the different regions, with an enormous gap between areas in terms of education levels and digital technology development. 103 A recent study revealed that the digital literacy levels of Western older adults in rural China are relatively lower than those in other areas, and the positive associations between digital literacy and health behaviors for Western older residents lags behind that of those in central or eastern regions. 86 Our findings offer a more in-depth and nuanced understanding of the positive relationships between digital literacy and health behaviors among middle-aged and older adults. Considering these substantial heterogeneous effects, it is crucial to recognize the diversity among middle-aged and older adults and provide more sophisticated and tailored education and support to improve their digital literacy.
Third, life satisfaction mediates the associations between digital literacy and health behaviors (including physical exercise and physical examination). Consistent with previous studies, our results support the positive link between life satisfaction and physical exercise or activity, 56 as well as preventative health services such as physical examination.104,105 Middle-aged and older adults with higher digital literacy tend to have more information about health behaviors and remain highly health-conscious. They are also more likely to participate in social activities more extensively, which provides psychological benefits, reduces social loneliness, and enhances overall life satisfaction.42,44 Based on SDT, life satisfaction is a psychological objective that can increase older adults’ engagement in preventive and health behaviors.106,107 Previous research indicates that lower life satisfaction is linked to a higher prevalence of unhealthy behaviors, such as smoking, physical inactivity, and heavy drinking. 108 In contrast, higher life satisfaction is associated with a more proactive stance on health management, thereby enhancing autonomous motivation for adopting health behaviors.109,110 Since life satisfaction mediates the relationships between digital literacy and health behaviors (including physical exercise and physical examination), interventions aimed at enhancing life satisfaction among middle-aged and older adults are essential.
Fourth, another key contribution of this study lies in revealing that relational social capital and cognitive social capital play different mediating roles in the relationships between digital literacy and health behaviors. Specifically, relational social capital mediates the associations between digital literacy and health behaviors (including physical exercise, physical examination, and dietary supplement intake), whereas cognitive social capital mediates the associations between digital literacy and health behaviors (including physical examination and healthy diets). These findings are partly consistent with previous research suggesting that cognitive and relational social capital may have different associations with various individual health behaviors.74,77 Our findings suggest that social capital is associated with health behaviors and further extend this relationship by specifying the mediating roles of cognitive and relational social capital in the relationships between digital literacy and health behaviors. According to SCT, individual social capital, as the resources embedded in social networks, plays a vital role in the accessibility and mobilization of resources. 92 Concerning relational social capital, previous studies have shown that it has positive effects on physical activity and physical examination, 77 as well as dietary supplement intake. 111 Owing to the larger social networks embedded in relational social capital, the accelerated and comprehensive dissemination of health information among members of social networks enables individuals to acquire health-related knowledge, augment their self-health management awareness and capabilities, and consciously engage in health behaviors. 18 Regarding cognitive social capital, a study in Sweden found that cognitive social capital promotes young men's physical examination (sexually transmitted infection testing) 112 and is significantly associated with adopting healthy diets. 113 Cognitive social capital encompasses shared objectives and culture among network members. 60 A higher level of cognitive social capital is associated with greater adherence to collective norms, 58 and thus an individual's health behavior is linked to these internalized social norms.75,114,115 Considering that relational social capital and cognitive social capital serve as mediators in the relationships between digital literacy and health behaviors, it is imperative to implement effective strategies to bolster both relational social capital and cognitive social capital among middle-aged and older adults.
Finally, contrary to our expectations, our study reveals a noteworthy finding that neither life satisfaction, relational social capital, nor cognitive social capital mediates the relationship between digital literacy and learning health or wellness information. This may be partly explained by the diversity and complexity of health behaviors, which are not homogeneous; thus, the influencing channels and factors are also diverse.10,12 Additionally, life satisfaction and social capital may not be determinants or significant influencing factors for specific health behaviors, such as learning health or wellness information. Learning about health or wellness is often an individual, low-cost activity driven by immediate curiosity or a practical need, which may not require the same deep motivational drivers, such as a sense of life satisfaction or a sense of community. Our correlation analysis results also support this view to some extent. Specifically, life satisfaction and relational social capital were only weakly and positively correlated with adopting healthy diets. Unexpectedly, life satisfaction and cognitive and social capital were negatively, though not significantly, associated with dietary supplement intake. The observed patterns indicate that the relationships between digital literacy and health behaviors may involve more intricate mechanisms than originally hypothesized, possibly mediated or moderated by other unidentified factors. This finding underscores the importance of future investigations into more proximal mediators, such as health consciousness or perceived information need.
Strengths and limitations
This study has several notable strengths. First, to the best of our knowledge, this study is one of the first to systematically investigate the associations between digital literacy and multidimensional health behaviors among middle-aged and older adults in rural China, drawing on a large-scale, probability-based survey dataset. Second, this study developed a comprehensive index to measure digital literacy and utilized multiple indicators for health behaviors, which provides great potential for exploring the associations between digital literacy and health behaviors in-depth. Third, by integrating SDT and SCT, this study begins to uncover the mediating roles of life satisfaction, relational social capital, and cognitive social capital in the associations between digital literacy and health behaviors, illuminating key psychological and social pathways through which digital literacy may be related to health behaviors. Finally, this study moves beyond individual-level heterogeneity in age and gender by incorporating an analysis of regional disparities, offering a more comprehensive examination of heterogeneity than is typically explored in prior research.
This study has several limitations that should be acknowledged. First, this study relies on self-reported data, which may introduce potential social desirability and participant prejudice. Future research could validate these findings by employing diverse information sources, such as objective measures or third-party reports, to reduce these biases. Second, while we controlled for a range of socio-demographic factors, the potential for omitted variable bias remains, which may introduce endogeneity. For example, respondents with higher digital literacy may differ from those with lower digital literacy in several unobservable factors (e.g., health literacy), which may be correlated with health behavior. Future studies could incorporate additional covariates or employ advanced methods, such as instrumental variable approaches, to further mitigate omitted variable bias and address endogeneity concerns. Third, due to the cross-sectional design, this study is limited to describing associations and cannot establish causality among variables. While some cross-sectional studies can assess causation using advanced designs (e.g., instrumental variable approaches, Mendelian randomization, or natural experiments), our study did not employ such methods. Future research should employ longitudinal designs or advanced causal inference methods to more thoroughly explore the causal relationships between digital literacy and multidimensional health behaviors. Finally, our exploration of mechanisms was not exhaustive. While our model identified two significant mediating pathways, the link between digital literacy and the specific behavior of learning health or wellness information remains unexplained. More possible influencing mechanisms should be considered in future studies. Nevertheless, our findings could aid in measuring future interventions aimed at changing the unhealthy behaviors of individuals and provide new and essential insights into health behavior changes in the digital era.
Conclusions
Using a probability-based survey dataset, our study investigated the associations between digital literacy and multidimensional health behaviors among middle-aged and older adults in rural China. Additionally, heterogeneity in the associations by age, gender, and region was also examined. We also tested two linking mechanisms based on SDT and SCT. Our empirical analysis revealed that digital literacy was positively related to participating in physical exercise, taking physical examination, dietary supplement intake, learning health or wellness information, and consciously adopting healthy diets. However, these associations exhibit considerable heterogeneity in terms of age, gender, and region. Furthermore, our studies partly revealed the mediating role of life satisfaction and social capital in the associations between digital literacy and health behaviors. Our findings offer additional and in-depth insights into the relationships between digital literacy and health behaviors, as well as the underlying mechanisms that drive these connections. Our findings contribute to the literature by highlighting the positive relationships between digital literacy and health behaviors and emphasizing the need for tailored interventions to enhance digital literacy levels, life satisfaction, and social capital while considering the diverse needs and contexts of middle-aged and older adults.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251374114 - Supplemental material for Digital literacy, life satisfaction, social capital, and multidimensional health behaviors among middle-aged and older adults in rural China: A nationwide cross-sectional study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251374114 for Digital literacy, life satisfaction, social capital, and multidimensional health behaviors among middle-aged and older adults in rural China: A nationwide cross-sectional study by Zhibin Li, Dong Li and Zuxian Li in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors thank the data from the China Rural Revitalization Survey research team. Collecting this data was an enormous project that required the efforts of many people. The authors would like to express their gratitude to everyone who contributed to this study. “A Comprehensive Survey on Rural Revitalization and China Rural Revitalization Survey (CRRS) Database” (Project Number: GQDC2020017), Major Economic and Social Investigation Project funded by the Chinese Academy of Social Sciences.
Ethics approval
We utilized de-identified data from the China Rural Revitalization Survey conducted by the Rural Development Institute, Chinese Academy of Social Sciences. All participating studies were approved by Institutional Review Boards, and the respondents provided written informed consent. Ethical approval was not required for the analysis of the anonymized data.
Consent to participate
All participating studies were approved by Institutional Review Boards, and the respondents provided written informed consent.
Contributorship
ZBL contributed to writing—review and editing, writing—original draft, visualization, software, methodology, formal analysis, data curation, and conceptualization. DL contributed to review and editing, supervision, methodology, and formal analysis. ZXL helped revise the manuscript. All the authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.