
Abstract
Background
The pain induced by postoperative dressing changes adversely influence recovery and quality of life. In this study, we try to evaluate the pain alleviation effect of virtual reality (VR) distraction during postoperative dressing changes of patients who received surgical drainage of perianal abscess.
Methods
This was a prospective, randomized clinical trial. A total of 172 patients with perianal abscess were randomly assigned into control (only analgesics) and VR groups (VR distraction + analgesics). The pain and physiological measurements of all patients were collected before, during, and after the first dressing change following surgery. The difference in pain intensity and physiological parameters measurement between control and VR group was analyzed.
Results
The baseline characteristics of VR and control group were comparable (all P > 0.05). There was no significant difference in mean pain scores prior to and after dressing change between groups (both P > 0.05). Mean pain scores of 5, 10, 15, and 20 min measuring points during the first dressing change were significantly lower in the VR group compared with the control group (all P < 0.05). Pulse rates and oxygen saturation were not significantly different between groups.
Conclusion
VR can be used as an effective adjuvant pain distraction approach for postoperative dressing change.
Introduction
Perianal abscess severs as the most common anorectal abscesses, which are typically presented with excruciating pain around the anus and significant discomfort and exert an adverse effect on quality of life.1,2 Timely incision and drainage have been confirmed as the primary treatment for perianal abscess.3,4 Adequate drainage and prevention of premature healing of the skin over the abscess pocket is crucial target of postoperative treatments. 5 Therefore, postoperative wound care constitutes as a main effective competent of postoperative treatments.2,4 However, severe pain caused by repeated dressing changes was associated with adverse physical and psychological implications, thereby being harmful to efficacy of postoperative rehabilitation.6,7 Pain control was presented as a challenge for surgeons, especially for pain-related dressing change. 8 Moreover, another important challenge is coexisting anxiety, which is particularly obvious during the first dressing change. 9 It has been reported that anticipation of pain exacerbates patient anxiety, which in turn can exacerbate the pain. 10
Oral or topical analgesics were still used as the primary choice for postoperative pain control.11,12 However, oral or topical analgesics not only effectively relieve pain, but also bring up various adverse effects. Moreover, severe dependence on analgesics was associated with poor short-term prognosis, such as increased hospital stay, delayed wound healing, and high cost.13,14 Otherwise, simple low dosage analgesics administration usually cannot effectively control acute pain. 15 Therefore, a feasible adjunctive analgesic approach was required for postoperative care of patients with perianal abscess, especially for repeated wound dressing change.
Virtual reality (VR) is known as an immersive computer-generated virtual environment designed to make users be immersed in an interactive, simulated world or virtual scenario to achieve distraction from pain. 16 It has been shown that VR distraction could decrease reported pain levels during invasive medical procedures such as physical therapy, urological endoscopies, burn wound care, and surgery without anesthesia.17,18,19 However, to date, there was no study concerning on the significance of VR on pain control during postoperative wound care in patient with perianal abscess. Moreover, extremely severe pain resulted from dressing change severs as a significant risk factor for patients with perianal abscess. Therefore, in current study, we design a prospective study to evaluate the value of VR distraction on pain control during postoperative wound dressing change in patient with perianal abscess.
Material and methods
Patients
This study was set as a prospective, open label and randomized design, which was approved by the Institutional Review Board of ***, and in accordance with declaration of Helsinki. Written informed consent was signed by each enrolled subject. The sample size was calculated according to power of test (1 – β) as 0.9 and significance level (α) as 0.05. A total of 172 patients received surgical incision and drainage and postoperative dressing change at Day Treatment Centre of the *** between May 1, 2018, and May 1, 2020, and fulfilling the inclusion and exclusion criteria were enrolled. Consort flow chart of this study was presented in Figure 1. Inclusion criteria included adult patients, ability to effectively communicate in Chinese, qualified reading/writing ability, and compliance of postoperative wounds dressing changes in our department. Subjects with psychiatric disorders, unable to use VR sets, and hearing impairment were excluded. After surgical incision and drainage, a standard postoperative treatment protocol was conducted for each patient, including dressing changes, sitz baths, and oral analgesics (Flurbiprofen Axetil, Beijing, China). All 172 patients were randomized to receive either conventional dressing changes or dressing change under VR distraction according to the computer-generated-random number. Among whole subjects, 86 received postoperative conventional dressing changes were set as control group. Whereas another 86 received daily dressing changes under VR distraction was defined as the VR group. Considering that patients always had the most severe pain at the first dressing change after surgery, all evaluations were conducted during the first dressing change at postoperative second day during hospital stay.

Consort flow chart.
Dressing change procedures under VR system
VR system consists of a Pico G2 4K head-mounted display with a 101° view field, and a hand-held controller. Each patient can choose to view a favorite immersive 360° Cine-VR scene of movies via Pico G2 4K head-mounted display. All patients in VR group received a training about instructions for use of VR system prior to the first dressing change. The standard steps of dressing changes procedure included: first, removing the dressings and evaluating wound, then cleaning and sterilizing to achieve full drainage, and finally sterilized dressing covering. For patients in VR group, dressing changes were performed following fully immersing in VR distraction. Standard daily dressing changes were conducted for each patient in control group.
Outcomes evaluation
The primary outcome was defined as the pain intensity assessed by visual analogue scale (VAS). The VAS scale has verbal anchors at the beginning and end labeled “no pain (0)” and “unbearable pain (10 scores),” respectively. 20 Patients were required to indicate pain score between score 0 and 10, and the results of pain score was marked on a VAS scale with a 10 cm line by a nurse. The physiological measurements including pulse rates (PR) and oxygen saturations (SaO2), and patient satisfaction were considered as the secondary outcome. In details, PR and SaO2 were monitored by a pulse oximeter.
All outcome measurements were performed before the dressing change and then at 5 min intervals until end of the dressing change by the same nurse in our nursing team. At 5 min after the end of the dressing changes, outcome measurements were recorded as the post-dressing change outcome. Considering that patients always had the most severe pain at the first dressing change after surgery, all outcome measurements were conducted during the first postoperative dressing change.
Statistical analyses
All statistical analyses of all data obtained were conducted by using the IBM SPSS Version 21.0
(Armonk, NY: IBM Corp.). Normal distribution of continuous variables was evaluated by using the Kolmogorov–Smirnov test. Continuous variables were expressed as mean ± SD were compared by using of analysis of independent t-test, such as age, BMI, duration of symptoms, VAS score, duration of first dressing change. Categorical variables presented as frequencies and analyzed by using Chi-square test, such as sex, history of smoking and alcohol drinking. Repeated measures analysis of variance was performed to compare all the measurements over time between groups. Additionally, a two-sided p < 0.05 as considered as an indicator of a significant difference.
Results
Baseline data
The baseline demographic and clinical data of all enrolled patients were presented in Table 1. One hundred seventy-two patients with perianal abscess were enrolled, with a mean age of 45.6 ± 8.6 years and a male-to-female ratio of 1.8:1. The case number with history of smoking and alcohol drinking were 105 and 120, respectively. The mean duration of symptoms was 7.8 ± 2.2 days. The mean time of the first dressing change following surgery was 22.5 ± 4.3 min. No major difference in terms of baseline characteristics between the VR group and control group was observed, including baseline pain intensity by VAS measures at 4–6 h after surgery (all P > 0.05, Table 1).
Baseline data of all enrolled patients with perianal abscess.

BMI, body mass index; VR, virtual reality; VAS, visual analog scale.
Pain intensity evaluation
There was no significant difference in terms of pain intensity indicating by VAS score prior to dressing changing between groups (4.2 ± 1. 2 vs. 4.3 ± 1.3, P > 0.05). In process of dressing changes, the pain intensity at 5, 10, 15, and 20 min measure points after the beginning of dressing change in the VR group were significantly relieved, comparing with control group (all P < 0.05, Figure 2). A repeated measures test showed that pain intensity was significantly relieved over time in the VR group (P < 0.01, Figure 2). There was no difference in terms of mean VAS score measured at 15 min after surgery between groups (5.3 ± 1.2 vs. 5.2 ± 1.6, P > 0.05).
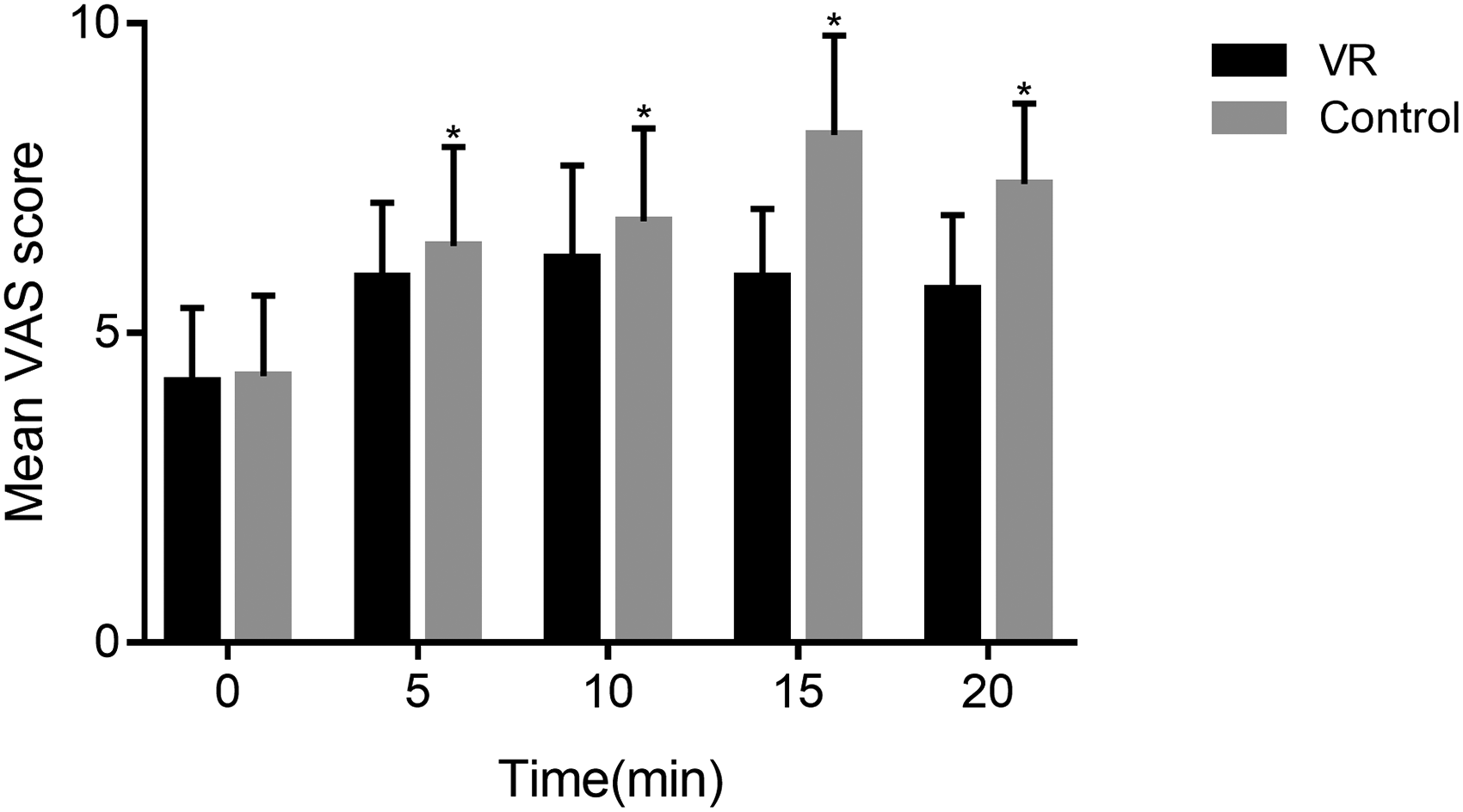
Pain scores at 0, 5, 15, and 20 min during the first dressing change in patients undergoing surgical drainage of perianal abscess. Patients in VR group had lower pain scores than control group at all measuring points (all P < 0.05). Data points are expressed as mean ± standard error. *, P < 0.05. VAS, Visual analog scale.
Physiological indicators measurements
After initializing the dressing change, all patients in both VR and control group have an increased PR level over time (both P < 0.05). However, there was no observable difference in terms of PR level between groups at all-time points during the process of dressing change (all P > 0.05, Figure 3). For SaO2 measurements, all enrolled patients had a stable and normal SaO2 level during dressing change.
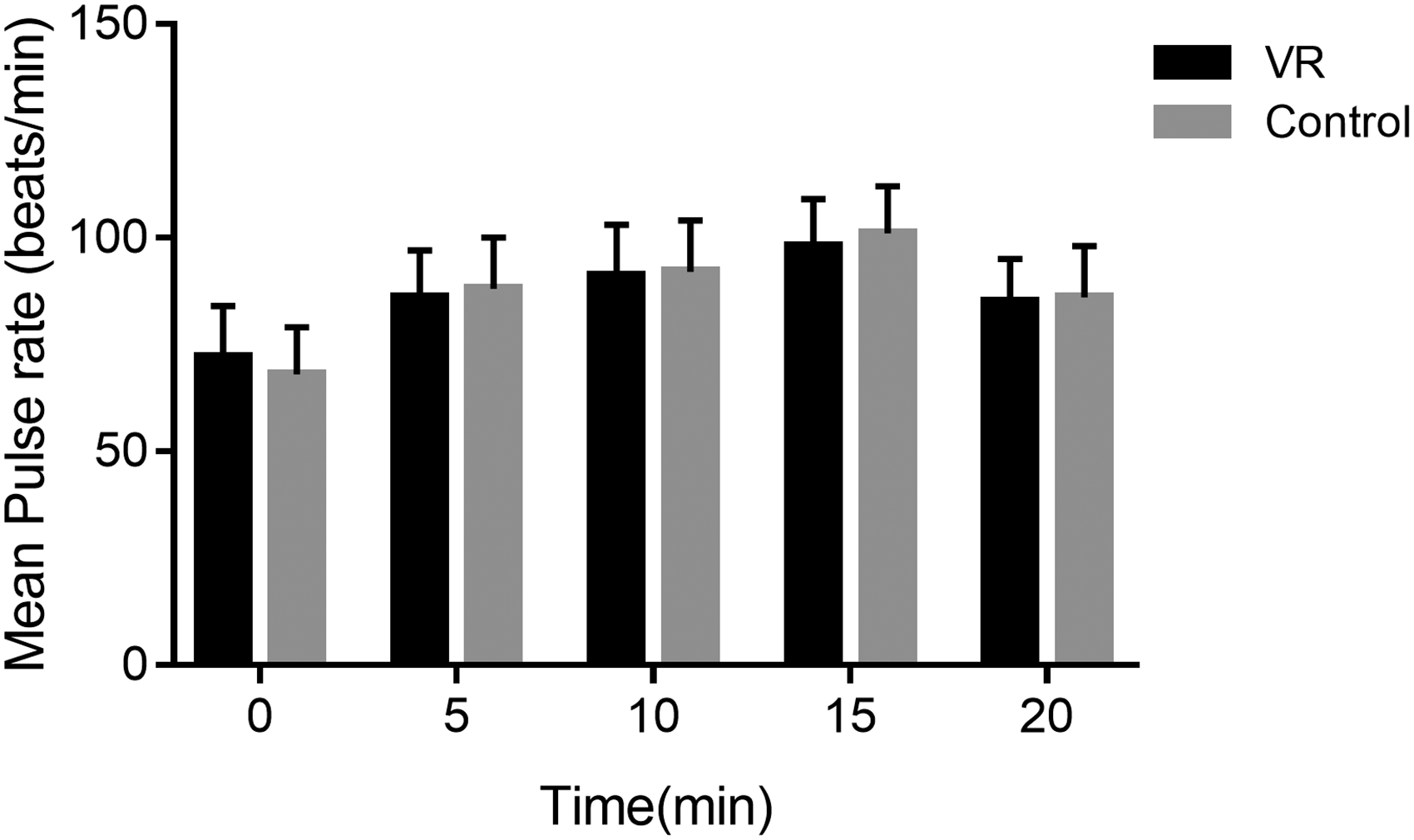
Pulse rates at 0, 5, 15, and 20 min during the first dressing change in patients undergoing surgical drainage of perianal abscess. There was no significant different in terms of pulse rates between groups at all measuring points (all P > 0.05). Data points are expressed as mean ± standard error.
Discussion
Dressing changes associated with pain present as a challenge for postoperative recovery in patients who received surgery for perianal abscess. 21 Therefore, effective pain management is an important part of postoperative treatments. In this study, we introduced VR set in postoperative dressing change, and prospectively evaluate its effect on pain alleviation in patients with perianal abscess and showed that patients in VR group had a significant lower pain intensity than that of control group. Furthermore, pain alleviation was more observable over time in the VR group compared with control group. Finally, we concluded that the VR distraction can be used as an effective adjuvant tool for postoperative pain management during dressing change in patients who received surgery for perianal abscess.
Patient who received invasive surgery always suffered from wound dressing changes related to severe pain, which is also considered as a challenge for postoperative managements.22,23 Pharmacologic analgesics including opioids remain the primary analgesia approach in such patients, however, which always exert inadequate pain alleviation and present severe side effects.24,25 VR has been introduced as an intervention for alleviating pain with relative satisfied efficacy.26,27 In this study, VR distraction significantly decrease pain intensity induced by postoperative dressing change. The results of our study are consistent with previous study. 28 VR may present a novel opportunity for decreasing patient pain suffering by presenting a focused aesthetic multisensory immersive stimulation, which might in turn induce emotions regulation, attention distracting, and engagement of patients. 29 Moreover, pain alleviation significance of VR was more observable during dressing change, compared with that of prior to dressing changes and following dressing changes, indicating that the significance of VR distraction on pain alleviation is more effective while patients suffered from increased pain intensity.
In entire process of dressing changes, there was no significant difference in terms of physiological measurements between VR and control groups. Physiological measurements are not significantly associated with pain intensity in setting of painful procedures, which also not be affected by application of VR. Moreover, the SaO2 was presented as a stable level at all measurement points and without significantly difference between groups, which would not be influenced by pain induced by dressing changes.
VR distraction is characterized by immersive and interactive, engaging several senses simultaneously, which enable patients to hear, see or feel stimuli from a visual audio or video, and can interact with the virtual setting and the virtual world's response in real time to those actions. 30 In perspective of potential mechanisms for pain alleviation, VR engages pain signaling pathways through distraction, and exerts a positive effect on cognitive variables, thus improve pain control through multiple senses. 31 Moreover, VR enables subjects away from their current state and dressing changes setting through immersion. Furthermore, it has been reported that VR decreases the neural activity in healthy subjects who received painful stimulations as compared to a no-VR condition. 32 Future studies with VR should explore the mechanisms through which multimodal approaches modulate pain-related and other processes in patients suffering from dressing change related pain.
There are several limitations to this study. The results of this single-center study cannot be generalized in clinical practice. Therefore, we will conduct a large-scale and multicenter study to furtherly confirm the evidence level of these results. Moreover, due to the application of the VR device, blind design is not achieved. Double-blind design will be an ideal research method to evaluate the effectiveness of interventions. Lastly, the application of VR in postoperative pain management is still limited in China. The VR device used in this study is not a dedicated medical device and may not be primary choice for patients with perianal abscess surgery. A more professional medical VR device that can establish specialized and individual immersed VR environments is required for optimal pain control during dressing changes.
Conclusion
VR distraction can observably improve pain management in postoperative dressing changes in patients with perianal abscess by providing an immersive computer-generated environment. Therefore, we suggested that VR distraction could be used as a useful adjunctive analgesic approach for dressing change-related pain.
Footnotes
Acknowledgements
The authors thank all the participating patients and nursing staff.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Ethical approval
This study was reviewed and approved by Committee on the Ethics of ***.
Guarantor
Dr Hailiang Liu is guarantor for this study.