
Abstract
Background
To overcome the challenge of psychotherapist scarcity in applying pain psychotherapy in clinical practice, we developed a virtual reality (VR) program delivering weeks of pain psychotherapy without psychotherapists, with a focus on minimizing the risk of motion sickness.
Objectives
We conducted a single-arm pilot study to assess the efficacy and motion sickness associated with a VR session delivering guided imagery and breathing techniques selected from the initial course of our VR program, involving patients suffering from various acute and chronic pain.
Methods
Patients underwent a 15-min VR session. Pain-related and anxiety ratings using a 0–10 numerical rating scale were collected pre-, during-, post-VR and in 6-h follow-up. Motion sickness symptoms were assessed using Simulator Sickness Questionnaire pre- and post-VR.
Results
Patients (n = 73) reported their perceived pain intensity and anxiety reduced significantly from pre- to post-VR by 22.9% and 45.0% (all p < 0.0001), respectively. Such modulatory effects of VR in pain perception and anxiety persisted at 30 min, 1 h, 2 h, and 6 h post-VR (all p < 0.0001). The pre-post beneficial effects of VR were independent from patients’ demographic characteristics and their pain duration. Importantly, only six patients (8.2%) had post-VR motion sickness symptoms, and only one patient reported moderate level of severity.
Conclusion
These findings suggest the selected VR session delivering pain psychotherapeutic techniques may be effective and tolerable for patients with varying pain conditions, which provides initial evidence for the development of future randomized controlled trials of the complete VR program.
Introduction
Effective pain management poses a significant challenge within the clinical environment. More than 70% of individuals with pain conditions experience persistent moderate to severe pain. The prevalence of chronic pain is nearly 40%, and approximately one-third of these individuals struggle with intractable neuropathic pain. 1 The conventional reliance on pharmacological interventions, predominantly opioids, often fails to achieve satisfactory pain relief. 2 This shortfall prompts patients to resort to increased doses or alternate medications, resulting in adverse effects, such as respiratory and central nervous system depression.3,4 In response to these challenges, a shift toward a multimodal pain management strategy, incorporating psychological therapies as complementary adjuncts, is recommended. Approaches, such as behavioral therapy and relaxation techniques, have demonstrated the ability to modify cognitions and behaviors that influence the perception of pain, and they empower patients with self-efficacy skills to mitigate mood disturbances associated with pain.5,6 Traditionally, these psychological therapies are delivered in a face-to-face fashion by psychotherapists. However, a critical shortage of psychotherapists, particularly those specialized in pain psychotherapy, severely restricts the widespread application of psychological interventions in clinical settings. There arises an urgent need for pain management strategies that are not only effective but also accessible and low risk.
In recent years, virtual reality (VR) has emerged as an effective nonpharmacological treatment modality for pain. 7 Offering an immersive, multisensory, three-dimensional environment, VR creates a profound sense of presence, capturing attention and diminishing the focus on pain. An example of a VR application is “Snow World,” in which patients engage in throwing snowballs at animated characters during a virtual journey down an icy river. This specific application has demonstrated efficacy in pain reduction in patients undergoing burn wound debridement. 8 Advancements in mobile high-performance computing have significantly reduced the size and cost of VR devices, enabling their integration into routine clinical settings. Virtual reality has proven to be a valuable intervention for various acute pain conditions, 9 including acute procedural pain, 10 burn pain,11,12 and labor pain,13,14 as well as for persistent pain. 15 This widespread applicability underscores the potential of VR as a versatile and accessible tool for pain relief in diverse clinical scenarios.
While VR has demonstrated effectiveness in numerous pain studies, these investigations are subject to several limitations. Most VR pain studies employed distraction through VR games or movie clips to divert patients’ attention away from pain. 16 However, for persistent or refractory pain states, which are common occurrences in the pain department, relying solely on distraction might prove insufficient. 17 Furthermore, a notable gap exists in the exploration of more sophisticated psychotherapeutic techniques. Existing studies have often focused on specific indication of pain types, raising questions about the broader applicability of VR across various pain conditions. Additionally, the durability of VR's benefits beyond the immediate period of device usage remained inadequately established. Finally, a critical aspect that warrants further exploration is the safety of VR use in the context of pain management. While motion sickness is a well-recognized issue associated with VR, its prevalence and severity have not been extensively studied in the realm of pain management. Given that patients in the pain department may already be predisposed to vertigo or nausea due to underlying conditions (e.g. cancer-related pain) or the side effects of analgesics, understanding and mitigating the risk of motion sickness with VR is crucial for its effective and safe utilization in this population.
Building upon these considerations, we developed a VR program designed as an adjunctive therapy for pain management. This program amalgamates various pain psychotherapies, commonly endorsed by pain psychologists and is administered for weeks aligning with traditional psychotherapy programs.6,18,19 It adheres to principles formulated specifically to minimize the risk of motion sickness. Notably, the selected psychotherapies were delivered to patients by VR without the need for guidance from psychotherapists. In the present pilot study, we selected a single session from initial course of the complete VR grogram to evaluate its benefits and safety. The selected VR session integrates guided imagery and breathing techniques, designed with the expectation of rapidly reducing pain and anxiety. We hypothesized that the rapid pain relief achieved by the selected VR session would encourage patients to adhere to the VR program at the outset of the psychotherapeutic course lasting for weeks.
The efficacy of the selected VR session has been validated through a recent study wherein healthy adult volunteers experienced reduced intensity and unpleasantness ratings in response to experimentally induced pain while immersed in the VR environment, as opposed to a two-dimensional video. 20 To further examine the efficacy and safety of the selected VR session in clinical population, the present single-arm pilot study recruited patients with various pain conditions in pain department. Additionally, we conducted an assessment of potential baseline correlative factors associated with efficacy and safety of VR. The outcomes of this study serve as a foundational step to understand the analgesic and safety properties of the initial session of our VR program, supporting the prospect of future investigations into the VR program's efficacy and safety in weeks’ use in comparative studies against active controls among patients with chronic pain.
Methods
Study design
This is a single-center, prospective, self-controlled interventional study among patients with moderate to severe pain for any reason to assess the impact of a single VR session on patients’ experience of pain and the safety of using VR. This study was conducted between December 2021 and March 2022 at Shanghai Xinhua Hospital, which is a large tertiary hospital in Shanghai, China. This study was approved by the ethics committee of Shanghai Xinhua Hospital (XHEC-C-2021-094-2) and prospectively registered with ClinicalTrials.gov on September 21, 2020 (NCT05157893).
Patients
Patients were identified for enrollment if their pain was being managed at the Department of Pain Treatment of the study site. The inclusion criteria were patients aged 18 years or above; average pain intensity score of ≥4 on a 0–10 numerical rating scale (NRS) during the past 24 h, being able to communicate in Chinese. Patients were excluded if they met any of the exclusion criteria: pre-VR pain intensity score on a 0–10 NRS <4; injury to eyes, ears, face, or neck that impedes comfortable use of VR device (including shingles or trigeminal neuralgia); diagnosis of epilepsy, dementia, migraines, or other neurological diseases that may prevent the use of VR; severe vision or hearing impairment; history of severe motion sickness; and females currently pregnant.
Study interventions
The VR session was administered using the all-in-one head–mounted VR device Pico Neo 3 Pro and headphones (Figure 1(a)). The VR device presents the resolution of 3664 × 1920 pixels and the refresh rate of 90 Hz with the 98° field of view. It is equipped with two 6 degree-of-freedom touch controllers, supporting positional tracking and interaction with the VR environment. Noise reduction headphones were used to optimize the immersive experience, which are connected to the VR device via Bluetooth. Disposable sanitary cap and a silicone cover on the VR helmet were used. Both VR device and headphones were sanitized with alcohol between patient uses.
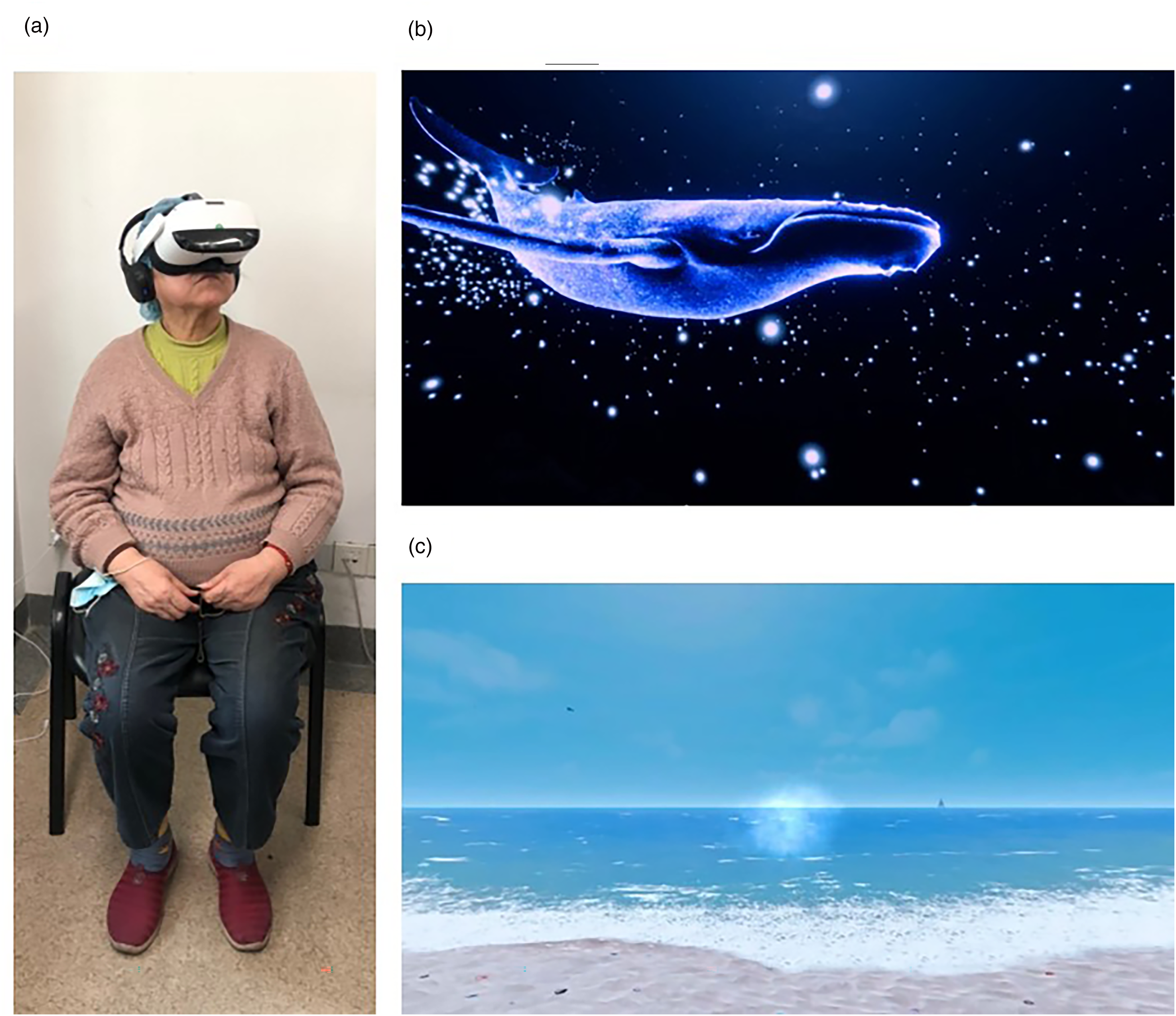
The VR intervention used in the study: a patient wearing a study VR device and headphones (a); screenshots of the first VR module (b) and the second VR module (c) included in the pain psychotherapy-based VR session.
The VR session used in this study integrates guided imagery and breathing techniques with the aim of inducing both mental and physical relaxation quickly, reducing pain and negative emotions effectively. The psychologist in our research team converted the face-to-face protocols into a computerized version and incorporated it into the VR session. We created attractive virtual environments integrated with calming music and/or nature-based sounds intended to enhance the effects of distraction therapy with VR. The VR session was designed using principles that sought to minimize motion sickness. These principles include reducing the need to excessively move the patient's head within the VR environment; avoiding abrupt scenery changes that exaggerate a sense of motion; and avoiding rapid movements of virtual objects that force rapid eye tracking.21,22 Patients wore VR device and headphones in a sitting position. They were instructed to feel free to look around in the VR environment but avoid hasty movements.
The VR session is composed of two modules delivered sequentially. The first VR module is a 7-min immersion in an underwater virtual world. In the deep blue ocean, various marine animals swim around the patient, accompanying with calming music. It helps patients expand the physical awareness and enter a state of deep embodiment to induce mental relaxation, consequently diverting the attention from pain (Figure 1(b)). Following the first module is another 8-min VR module. On a virtual sunny beach, patients receive a hint of comfort and relaxation. A female voice guides patients to focus on slow and paced breathing. Visual effects simulating breathing air synchronized with sound of sea waves guide patients’ rhythm of breathing (Figure 1(c)). This module was designed to guide patients on regulating the breathing and arousing relaxation response quickly.
Measures
The primary outcome is the change in pain intensity ratings from pre- to immediately post-VR. The secondary outcomes include (a) changes in anxiety from pre- to during- and immediately post-VR; (b) changes in pain intensity, pain unpleasantness, and time spent thinking about pain from pre- to during VR; (c) patients’ satisfaction with VR. Additionally, the present study set exploratory outcomes: one is changes in pain intensity, anxiety, pain unpleasantness, and time spent thinking about pain across time up to 6 h post-VR; the other is the correlations between baseline characteristics and pre-post changes in pain intensity and anxiety.
Pain and anxiety assessments
Pain was assessed for its sensory, affective, and cognitive components using pain intensity, pain unpleasantness, and time spent thinking about pain, respectively. 23 Anxiety, which is the most common accompanying negative emotion with pain, was also assessed. These measures were evaluated by scoring on a 0–10 (integers) NRS. The four measures were explained to patients literally with visual cues helping them to understand the incremental severity levels. Patients rated symptom severity from 0 to 10 (0 = nonexistent, 10 = most severe) for each measure.
Satisfaction with VR
How patients felt about the presence (to what extent patients felt like “going into” the virtual world) and fun in the VR were assessed. The extent of the metric ranges from none to the highest by the 0–10 NRS. Patients’ willingness to use VR in the future was also evaluated using the question, “Are you willing to use VR for alleviating your symptoms in future?,, with the answer as “Yes” or “No.”
Pain-related psychological characteristics
The experience of pain is shaped by a host of psychological factors. Vigilance, catastrophizing, beliefs concerning controllability of pain, state anxiety, and depression are recognized as the most important psychological factors that have been incorporated into pain models that may explain pain perception and treatment benefits. 24 Well-validated and widely used instruments were selected to evaluate these important psychological characteristics: the Hospital Anxiety and Depression Scale 25 for state anxiety and depression, the Pain Vigilance and Awareness Questionnaire 26 for pain vigilance and awareness, the 6-item Pain Catastrophizing Scale 27 for pain catastrophizing, and the Pain Self-Efficacy Questionnaire 28 for pain self-efficacy.
Safety assessment
The motion sickness induced by VR was evaluated by the Simulator Sickness Questionnaire (SSQ). The SSQ is the most used subjective questionnaire for assessing VR-induced symptoms. 29 It allows patients to rate the severity of 16 symptoms reflecting the digital version of motion sickness (including headache, eyestrain, nausea, and vertigo) at four levels (none, mild, moderate, and severe). Severity of each symptom was rated on a 4-point (0–3) scale and scores of 16 symptoms were computed to get a total score by the researcher. The three distinct symptom clusters were labeled as Oculomotor (eyestrain, difficulty focusing, blurred vision, headache), Disorientation (dizziness, vertigo), and Nausea (nausea, stomach awareness, increased salivation, burping). The Nausea, Oculomotor, and Disorientation scores were then calculated. The higher SSQ scores reflect more severe motion sickness. Patients were coded as positive for each symptom if the corresponding score on SSQ elevated from pre- to post-VR. The severity of the symptom was coded as mild, moderate, and severe corresponding to 1, 2, and 3 points of pre-post symptom score elevation, respectively. Besides the motion sickness collected by SSQ, patient-reported adverse events (AEs) were also collected.
Patients’ motion sickness susceptibility at the baseline was assessed to analyze the correlation with post-VR motion sickness severity. The short version of Golding's Motion Sickness Questionnaire (MSSQ-short) which is among the most common in motion sickness research was used in this study. 30 Patients’ motion sickness history was also collected at the baseline to perform the correlation analysis with post-VR motion sickness incidence. Patients were asked to answer “Yes” or “No” to the question, “Do you have a history of motion sickness?.”
Study procedure
The study recruitment was conducted by investigators and trained research assistants. Investigators identified eligible patients via the clinic schedule and inpatient census. Prescreened patients were invited to meet a research assistant to be confirmed about the eligibility and given an introduction to the study. Finally, eligible patients signed the informed consent to complete the enrollment.
The research assistants accompanied enrolled patients to a distinct isolated room. As shown in Figure 2, enrolled patients completed a baseline survey of their demographic characteristics, disease history, pain and anxiety perceptions, pain-related psychological characteristics, motion sickness symptoms, motion sickness susceptibility, and history. After that, patients were given a tutorial on the VR device use. They were instructed to remove the VR device for any discomfort felt during VR. The VR session lasted 15 min. After the end of VR session, the VR device was removed, and patients received an assessment immediately on pain and anxiety perception both during- and post-VR. To avoid breaking patients’ immersive experience with VR, we did not collect data directly during the VR session but at post-VR. Subsequently, motion sickness symptom reevaluation and patients’ satisfaction with VR use were performed. In the phase of pre- and post-VR, data were collected through face-to-face method. Patients who completed the post-VR assessment were compensated for 100 China Yuan.

Study procedure.
After the completion of post-VR assessment, patients were free to leave the study site and received follow-up assessments remotely on their pain and anxiety perceptions at four timepoints that were 30 min, 1 h, 2 h, and 6 h post-VR. In the phase of follow-up, data were collected by phone or WeChat (a popular social software). We did not take reevaluation of patients’ psychological characteristics post-baseline, considering a very short time of intervention would be insufficient to change patients’ psychological characteristics. Adverse events, if any, were collected from the time when patients put on VR device to the last follow-up timepoint. During the study, patients received analgesic treatments prescribed by their physicians in charge. We did not interfere with any analgesic treatment but collect the treatment information. The study procedure and data collected across the study are presented in Figure 2 and Table 1.
Timeline of data collection.

Pain unpleasantness and time thinking about pain were evaluated using the question, “During the most recent pain experience, how unpleasant you felt /how much time you spent thinking about your pain?.” As post-VR phase immediately followed during-VR phase, patients commonly reported that their most recent pain experience was during-VR at post-VR phase. Therefore, pain unpleasantness and time thinking about pain were evaluated only during-VR.
Statistical analysis
Since pain intensity and anxiety ratings were obtained in three occasions (i.e. pre-, during-, and post-VR), repeated-measure analysis of variance (ANOVA) was used to assess the effect of VR on these two ratings, followed by post hoc t-tests if ANOVA revealed significant effects. Paired sample t-tests were used to analyze the change of pain unpleasantness and time spent thinking about pain between pre- and during VR. Random intercept mixed-effect models were adopted to examine the effect of VR on pain ratings from pre-VR to 6 h post-VR, with participants as random effects. Pearson's correlation coefficients were used to exploratively assess the association between pre-post/pre-during session pain rating changes and the association between baseline characteristics and motion sickness. Nonparametrical tests such as Kruskal–Wallis one-way ANOVA and Mann–Whitney U tests were used to examine the relationship between categorical variables (e.g. gender) and pre-post/pre-during session pain rating changes, since the sample size differed considerably between groups. When applicable, multiple comparisons problems were addressed using Holm correction. 31 All statistical analyses were conducted in the open-source software jamovi (ver. 1.8.1.0) (https://www.jamovi.org/).
Results
Patient characteristics
Seventy-three (N = 73) patients were enrolled and received the VR intervention in this study (Figure 3). Of these patients, 49 (67.1%) were women, and the mean age was 59.3 ± 13.2 (mean ± SD, the same hereafter). The demographic and pain characteristics in the baseline are listed in Table 2.

Participant flow diagram of the study.
Baseline characteristics (N = 73).

Of all 73 patients, 47 (64.4%) had chronic pain (i.e. ≥3 months of pain). The types of pain varied considerably among patients. Five most common types of pain were as follows: acute herpes zoster in 15 patients (20.5%), postherpetic neuralgia in 11 patients (15.1%), chronic low back pain in 9 patients (12.3%), chronic lower limb pain in 9 patients (12.3%), and chronic cervical spondylosis in 7 patients (9.6%). Patients had a mean baseline pain intensity rating of 5.6 ± 1.4, anxiety rating of 3.3 ± 2.1, pain unpleasantness rating of 4.6 ± 2.0, and time thinking about pain rating of 5.6 ± 2.3. The baseline psychological characteristics are summarized in Table S1 in Supplement Information (SI).
Primary outcome: pre-post change in pain intensity
Immediately post-VR, pain intensity was significantly reduced (pre-VR, 5.6 ± 1.4; post-VR, 4.3 ± 1.8; t71 = 8.4; pHolm < 0.0001; Figure 4(a)), resulting in an average of 22.9% reduction. As much as 68.5% (50/73) of patients reported a pre-post decrease in pain intensity to some degree. Specifically, 28.8% (21/73) of patients achieved 30% or more reduction, and 16.4% (12/73) achieved 50% or more reduction in pain intensity post-VR.

Changes in average NRS ratings of pain intensity (a), anxiety (b), pain unpleasantness (c), and time spent thinking about pain (d) from pre- to during- and post-VR. Compared with pre-VR, average NRS ratings of pain intensity and anxiety decreased significantly post-VR; pain intensity, anxiety, pain unpleasantness, and time spent thinking about pain all significantly decreased during-VR. ****: compared with pre-VR; p < 0.0001 (the p values were all based on the 72 patients who provided complete rating data). The average pre-post reduction in pain intensity and anxiety was 22.9% and 45.0%. The average pre-during reduction in pain intensity, anxiety, pain unpleasantness, and time spent thinking about pain was 40.6%, 64.9%, 51.5%, and 61.6%. The whiskers represent the standard errors.
Secondary outcomes
Pre-during change in pain intensity
From pre- to during-VR, the average pain intensity decreased significantly (pre-VR, 5.6 ± 1.4; during-VR, 3.3 ± 2.2; t71 = 9.7; pHolm < 0.0001; Figure 4(a)), leading to an average of 40.6% reduction. Specifically, 77.8% (56/72) of patients reported lower pain intensity during-VR to some degree, and 15.3% (11/72) even reported 100% pain relief.
Anxiety
The VR session significantly lowered the average anxiety ratings from 3.3 ± 2.1 pre-VR to 1.3 ± 1.8 during-VR and 1.9 ± 2.0 post-VR (F(2,142) = 63.1; p < 0.0001;
Pain unpleasantness
Compared with pre-VR (4.6 ± 2.0), patients reported significantly less pain unpleasantness during-VR (2.1 ± 2.0; t71 = 9.6; p < 0.0001; Cohen's d = 1.1; Figure 4(c)). Excluding two patients reporting pain unpleasantness ratings of 0 at pre-VR, the remaining 70 patients had an average reduction of 51.5% in the level of pain unpleasantness. Specifically, 62.9% (44/62) of patients had 30% or more pain unpleasantness reduction, and 51.4% (36/62) achieved 50% or more reduction.
Time spent thinking about pain
Patients reported significantly less time spent thinking about pain during-VR (2.3 ± 2.0) than pre-VR (5.5 ± 2.4; t71 = 11.8; p < 0.0001; Cohen's d = 1.4; Figure 4(d)). From pre- to during-VR, the 71 patients who had nonzero pre-VR ratings demonstrated a 61.6% reduction in average in time spent thinking about pain. The 76.1% (54/71) of patients reported 30% or more reduction of time spent thinking about pain, and 60.6% (43/71) had 50% or more reduction.
Satisfaction with VR
The average ratings on engagement and fun in the virtual world were 6.7 and 5.7, respectively. Overall, 81.7% (53/72) of patients confirmed their willingness to use VR relieving pain in the future.
Changes in pain and anxiety across time
Linear mixed models revealed that pain intensity (F(6, 324.3) = 20.9; p < 0.0001), anxiety (F(6, 319.41) = 20.1; p < 0.0001), pain unpleasantness (F(5, 251.48) = 35.1; p < 0.0001), and time spent thinking about pain (F(5, 253.06) = 37.3; p < 0.0001) all significantly differed in different periods pre-, during-, and post-VR and in the follow-up. Notably, at follow-up timepoints of 30 min, 1 h, 2 h, and 6 h post-VR, ratings of pain intensity, anxiety, pain unpleasantness, and time spent thinking about pain were all significantly lower than pre-VR (Figure 5, Table S4 in SI).

Changes in average NRS ratings of pain intensity (a), anxiety (b), pain unpleasantness (c), and time spent thinking about pain (d) across time. Compared with pre-VR, average NRS ratings of pain intensity, anxiety, pain unpleasantness, and time spent thinking about pain all significantly decreased in the 6-h follow-up. ****: compared with pre-VR; p < 0.0001. The whiskers represent the standard errors.
Baseline characteristics correlated with changes in pain intensity and anxiety
No correlation was found between pre-post change in pain intensity or anxiety and baseline variables, including demographic variables, pain duration, and pain-related psychological characteristics. On the other hand, pre-post change in pain intensity was significantly correlated with baseline moderate pain intensity score of 4–6 (r = 0.36; pHolm = 0.036). In other words, greater change was observed in patients who had higher levels of moderate baseline pain intensity. Such a significant association was not found among patients with severe baseline pain intensity score of >6 (r = 0.24; pHolm = 1.00). These findings seemed to suggest that for patients with moderate pain, those with higher baseline pain intensity scores would benefit more from VR. Additionally, the baseline level of anxiety was also associated with pre-post change in anxiety, with those who had higher baseline anxiety scores having more decline in anxiety from pre- to post-VR (r = 0.43; pHolm = 0.001).
Analgesic treatment and the effect on changes in pain intensity and anxiety
A total of 19 (27.1%) patients had taken analgesic medications pre-VR. Our analysis revealed no significant impact of pre-VR analgesic use on pre-post change in pain intensity or anxiety. During the entire follow-up period, 41 (58.6%) patients did not take any analgesic medication. Between 1 h and 2 h post-VR, 15 (21.4%) subjects reported using analgesic medications; however, the analgesic use did not significantly affect changes in pain intensity or anxiety from pre- to 2 h post-VR. At other follow-up timepoints, few patients took analgesic medications (Table S5 in SI), so we refrained testing their impact on pain or anxiety at these timepoints. The specific analgesic medications used pre-VR and during follow-up are detailed in Table S6 in SI. Notably, no patients employed nonpharmacological analgesic treatments either pre-VR or during follow-up.
Safety
Motion sickness induced by VR and other AEs
Immediately post-VR, 6 of 73 (8.2%) patients reported motion sickness symptoms considered related to VR, including general discomfort, fatigue, headache, eyestrain, increased salivation, nausea, dizziness, and vertigo. Only one patient (1.4%) reported symptom classed as moderate (vertigo), whereas five patients (6.8%) reported symptoms as mild. Motion sickness symptoms post-VR are listed in Table 3. During the VR session, one patient (1.4%) reported an AE of tachycardia which was probably related to VR. No patients discontinued VR use due to motion sickness or any other AE.
Motion sickness symptoms post-VR by severity.

In the follow-up phase, 6 of 70 (8.6%) patients reported AEs, all of which were mild AEs, including vertigo (2.9%), nausea (2.9%), sore throat (1.4%), fatigue (1.4%), tinnitus (1.4%), and fullness in the head and eyes (1.4%). All these patients, except for one, did not report any motion sickness symptoms post-VR; however, they did report motion sickness like symptoms such as vertigo, nausea, fatigue, and fullness in head pre-VR. Therefore, it is likely that most of these AEs reported during follow-up were not related to VR but rather to the patients’ preexisting conditions. There were no serious AEs observed during the study. Adverse events occurred across different phases of the study are summarized in Table S7 in SI.
Baseline characteristics correlated with motion sickness induced by VR
Higher baseline motion sickness susceptibility scores were associated with less increase in motion sickness level from pre- to post-VR (r70 = −0.25; pHolm = 0.033), as revealed by the relationship between baseline MSSQ scores and motion sickness level of disorientation (r70 = −0.33; pHolm = 0.015), but not the level of nausea (r70 = −0.18; pHolm = 0.282) or oculomotor (r70 = 0.05; pHolm = 0.710). Further analysis suggested that this association was driven by the correlation between baseline MSSQ scores and baseline SSQ-Disorientation scores, since the partial correlation between MSSQ scores and SSQ-Disorientation change did not reach significance after baseline SSQ-Disorientation scores were controlled (r70 = −0.099; pHolm = 0.411). Pre-post SSQ score change and baseline MSSQ score are summarized in Tables S2 and S3 in SI.
Pre-post SSQ score change was also related to motion sickness history. Compared with those who did not have motion sickness history (N = 50), patients who did (N = 22) reported smaller SSQ score increase (patients with motion sickness history, −3.29 ± 4.55; patients without motion sickness history, −1.45 ± 4.04; U = 388; pHolm = 0.040; rrb = 0.30).
Discussion
The present study demonstrates the effectiveness and safety of pain psychotherapeutic techniques delivered by VR for a heterogeneous cohort of patients with varied pain conditions. Our findings indicate that a single VR session lasting 15 min resulted in a marked reduction of both pain intensity and anxiety levels. These results constitute the initial dataset on the analgesic properties and side effect prevalence of a selected VR session from our VR program among patients receiving care at the pain department, which is integral to informing the development of future clinical studies of the complete VR program.
VR-induced analgesia is believed to primarily operate through the mechanism of distraction. 32 By presenting visual and auditory stimuli, VR diverts the patient's attention away from painful stimuli, leading to a reduction in perceived pain intensity. 33 However, the efficacy of VR-induced distraction is limited and of short duration. 34 Incorporating pain-reducing strategies beyond distraction, such as pain psychotherapy, into VR interventions may promote sustained pain relief. 35 Multiple psychotherapeutic approaches have been shown to generate analgesic effects in patients with chronic pain when delivered by VR, including guided imagery, biofeedback, and techniques for emotional regulation.36–38 Garcia et al. found that an 8-week course of cognitive behavioral therapy-based VR was effective in reducing chronic low back pain throughout the treatment period and up to 6 months post-treatment.39,40 The ability of VR to deliver complex pain psychotherapy and provide long-term benefits even after the removal of the VR device has been demonstrated. To this end, we have developed a VR program that is specifically designed for adjunctive pain management, delivering psychotherapies commonly used for pain management. This VR program is designed to be administered for weeks aligning with traditional psychotherapy programs. In this study, we aimed to test the efficacy and safety of a single session selected from the initial course of the VR program. We hypothesized that the rapid pain relief achieved by the selected session at the start-up phase would encourage patients to adhere to the VR program lasting for weeks. Specifically, we chose guided imagery and breathing techniques as the strategies for the selected VR session, given their well-established ability to induce feelings of empowerment and relaxation, increase endorphins, and reduce pain and anxiety.41,42 These techniques influence the autonomic balance of the body by redirecting focus to the mind, leading to physiologic relaxation via changes in neurochemical and peptide regulation of the sympathetic and parasympathetic nervous systems.43,44 The effectiveness of guided imagery and breathing techniques can be achieved quickly, making them valuable adjunctive tools for reducing pain and anxiety in acute-care settings, such as post-surgery care.45–47
In this pilot study, a 15-min VR session resulted in an average reduction of 23% in pain intensity from pre- to post-VR. However, this reduction did not reach the threshold of clinical significance typically defined as a 30% decrease in pain. 48 Conversely, the average reduction in anxiety from pre- to post-VR was 45%, indicating a larger effect size compared to pain intensity reduction. Similar findings were reported in a separate study investigating VR-delivered guided meditation and biofeedback in patients with rheumatology. 49 One possible explanation for these results is that the psychotherapeutic techniques employed in these VR sessions have established therapeutic effects on mood regulation, 50 which may explain the greater efficacy in reducing anxiety with psychotherapy-based VR interventions. Virtual reality has demonstrated usefulness in psychiatric settings, particularly for individuals with anxiety-related disorders. 51 However, it should be noted that a reduction in anxiety only partially contributes to a decrease in pain 52 ; therefore, the inconsistent magnitude of reduction in anxiety and pain is not surprising. Most patients in the present study were experiencing chronic pain, which requires multidimensional psychological interventions that address mood regulation, revision of catastrophizing beliefs, and coping strategies with pain to regulate pain perception. 24 Cognitive and behavioral interventions for chronic pain should be implemented over an extended period of time. As such, it was challenging for a single VR session in this study to deliver these psychological interventions, which likely contributed to the limited analgesic effect observed. However, it is worth noting that patients reported a high likelihood of using VR again to relieve pain in the future, possibly due to the significant improvement in negative mood, which contributed to their overall satisfaction with the VR effects. We will pursue larger and sustained effects for patients with chronic pain using our complete VR program that delivers multidimensional psychotherapies.
Furthermore, apart from integrating analgesic strategies with VR, this study tried to address several gaps in VR research on pain diseases that have not been adequately explored so far. These gaps are discussed below. Firstly, previous VR pain studies have inadequately examined the safety of VR use. 53 For instance, motion sickness, which is associated with the use of VR, led to dropouts in trials conducted by Sarig Bahat et al.. 54 Most VR pain reports did not mention adverse reactions. 53 A significant number of patients with pain are susceptible to motion sickness due to underlying conditions or the side effects of analgesics. To mitigate this issue, we developed the VR program based on principles aimed at minimizing motion sickness. The safety outcomes demonstrated the effectiveness of our strategies. Among the vulnerable patients, primarily elderly and female individuals with persistent pain, only a small percentage reported post-VR motion sickness symptoms, with the majority experiencing mild severity. No patients withdrew from the study due to intolerance of wearing the VR device. Additionally, we investigated if any association existed between patients’ baseline characteristics and the severity of motion sickness post-VR. An interesting finding emerged, indicating that patients with a history of motion sickness tended to experience lower levels of motion sickness after VR, contrary to common sense. However, we did not observe an association between baseline motion sickness susceptibility levels and the severity of post-VR motion sickness. Further investigation is warranted to explore the factors influencing motion sickness induced by VR in patients with pain.
Secondly, the majority of previous studies on VR for pain management have primarily focused on measuring pain intensity immediately after the VR intervention. 55 Only a limited number of studies have examined the duration of pain relief induced by VR by measuring its effects at different time points. For instance, a study conducted in women with endometriosis demonstrated that a single session of VR led to a significant reduction in pain perception for up to 4 h post-treatment. 56 Similarly, in our study, we also observed a sustained effect of VR on pain relief. Comparing the follow-up levels to the baseline, we found significantly lower levels of pain and anxiety that lasted for at least 6 h. It is important to note that the distraction effect of VR is unlikely to persist for hours after the removal of the device. Consequently, the prolonged effects observed in our study can be attributed, at least in part, to the pain psychotherapeutic techniques delivered through the VR intervention.
Finally, the correlation between patients’ characteristics and the beneficial effects of VR remains unknown. One study reported that patients in the emergency department with less than a high school education experienced the greatest decline in pain from pre- to post-VR intervention, 57 which was not observed in our study. We found that the pre-post effects of VR on pain and anxiety reduction were independent of patients’ gender, age, education status, marital status, or employment status. In a randomized comparative effectiveness trial conducted with hospitalized patients, 58 it was noted that VR was particularly effective in a subgroup of patients with the most severe baseline pain scores (≥7 points). However, our findings differed significantly. In our study, among patients with moderate baseline pain scores (4–6 points), those with higher baseline pain intensity experienced a greater decrease in pain intensity from pre- to post-VR. However, we did not observe such an association among patients with severe baseline pain scores (>6 points). Regarding pre-post anxiety reduction, VR was more effective in patients with higher baseline levels of anxiety, irrespective of subgroups divided by baseline anxiety scores. With respect to other baseline pain characteristics, we found that the pre-post beneficial effects of VR were independent of patients’ pain duration. Unfortunately, we did not identify any psychological factors correlated with the pre-post reduction in pain intensity or anxiety. This may be attributed to the selected scales not fully reflecting patients’ psychological characteristics at the baseline. Future studies should further investigate the varying benefits of VR among patients with different levels of pain and psychological status.
Limitations
The primary limitation of this study is the absence of a control group, which precludes drawing definitive conclusions regarding the causal relationship between VR and the observed reductions in pain and anxiety. It is essential to note that this study was designed as a pilot investigation aimed at evaluating the safety and efficacy of a single session selected from our VR program for pain management. The outcomes from this study provide a foundation for conducting future randomized controlled trials comparing the comprehensive VR program against active controls to establish the effectiveness of VR in pain management. Another potential limitation of our study could be related to the selection of patients. Specifically, we chose to enroll individuals experiencing moderate to severe pain, which may introduce a selection bias. By excluding patients with mild pain at the baseline, it is possible that we have overestimated the effects of VR. However, our findings suggest a correlation between the baseline pain intensity level and the degree of reduction observed, highlighting the need for future studies to include patients across different levels of pain intensity to ensure generalizability of findings. Finally, during the follow-up period, patients were away from the study site and may have engaged in activities such as watching TV or listening to music which could have alleviated their pain or anxiety. Future studies should be better controlled to eliminate the influence of such activities on pain reduction.
Conclusions
This pilot study showed potential effectiveness and acceptability of a single VR session delivering guided imagery and breathing techniques selected from our pain psychotherapy-based VR program among a diverse group of patients suffering from different types of pain. Minimal side effects and high tolerance toward the VR device were observed. Importantly, the reductions in pain and anxiety experienced by the patients seemed to persist for at least 6 h following the cessation of VR use. These beneficial effects were possibly consistent across various demographic characteristics and pain duration. The data collected in this pilot study provide valuable insights for the design of a subsequent multicenter randomized controlled trial aimed at investigating the complete VR program administered for weeks in greater detail.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241308703 - Supplemental material for The benefits and safety of a virtual reality intervention in patients suffering from acute and chronic pain: A pilot study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241308703 for The benefits and safety of a virtual reality intervention in patients suffering from acute and chronic pain: A pilot study by Bingjie Ma, Libo Zhang, Yun Ji, Xuehua Huang, Luandi Yao, Wei Cheng, Li Hu, Xuejing Lu and Ke Ma in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors extend their gratitude to all the patients, family members, and investigators who participated in this study. Additionally, the authors would like to acknowledge Yongjing Hu and Hong Sun for their invaluable assistance with patient recruitment, as well as Jing Ding for providing guidance on the use of the VR device.
Consent to participate
Prior to their involvement in the study, all participants were provided with comprehensive information regarding the study procedures and provided written consent to participate.
Consent for publication
The informed consent process included provisions for the use of data and materials for reporting and publishing study findings, and all participants provided written consent for the utilization of their data in publications. All authors have approved the manuscript for submission.
Contributorship
The article was written by BM and LZ, who also acquired and evaluated the data. YJ and XH conducted the study and acquired the data, while LH revised and edited the manuscript. LY and WC contributed to the manuscript by revising and editing it for important intellectual content and providing technical support. XL and KM conceived, designed, and supervised the study. All authors have read and approved the final manuscript.
Declaration of conflicting interests
Luandi Yao and Wei Cheng were employees of Ultimate Therapeutics, Co., Ltd during the study.
Ethical approval
This study was approved by the ethics committee of Shanghai Xinhua Hospital (XHEC-C-2021-094-2).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
No guarantors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.