
Abstract
Background
Immersive Virtual Reality (VR) has been applied in pain management for various conditions, but its use in fibromyalgia (FM) remains underexplored. While physical activity plays a role in treating FM, patients’ low tolerance often limits its effectiveness. After reviewing the literature on VR and games for FM, we designed a novel VR exergame to assist FM patients in performing physical activity, and evaluate its feasibility.
Materials and Methods
This pilot study involved three female subjects with FM and four healthy female volunteers. The main outcomes included qualitative assessments of exertion, pain levels, psychological states experienced during the VR session, but also device comfort.
Results
Improvements in perceived exertion and pain intensity were observed during the VR exergame session in comparison to pre-exergame levels, along with a reduction in depression, stress and anxiety levels while using the VR immersive system. Most participants experienced also increase of relaxation and positive emotions during the exergame. Only one participant was not able to complete all levels of the exergame due to musculoskeletal pain exacerbation; nevertheless, this patient reported an improvement in motivation and enjoyment during the gameplay. Many participants expressed a greater motivation to perform the exercises in the VR environment compared to traditional training methods.
Conclusion
The proposed VR exergame is a feasible system that might reduce depression, stress and anxiety, while boosting motivation and relaxation in both healthy and FM subjects. A calibration protocol is required to tailor the system to each user's pain levels and physical abilities.
Introduction
Fibromyalgia (FM) is a chronic musculoskeletal disease of unknown aetiology, characterized by widespread nociplastic pain, and tender points in muscles and soft tissues. 1 Diagnosing FM can be challenging due to its numerous symptoms and comorbidities, including sleep disturbances, fatigue, muscle rigidity, and cognitive issues like anxiety and depression. Affecting an estimated 2% to 8% of the population, this syndrome significantly reduces quality of life and presents a substantial socio-economic burden through decreased productivity and increased healthcare use. 2 Considerable efforts have thus been made to establish a comprehensive diagnostic and therapeutic approach that addresses all aspects of FM, with a particular focus on pain reduction. 3
As pain involves both sensory and emotional components, pharmacological treatments should be complemented by non-pharmacological strategies such as physical activity, cognitive-behavioural therapy, and relaxation techniques.1,4–6 The attentional modulation approach has been shown to reduce pain and influence patients’ perceptions, thoughts, and emotions. Techniques such as cognitive distraction, mindfulness, and guided meditation, where a voiceover aids relaxation, are frequently employed.7,8 In recent years, traditional interventions have been integrated with emerging technologies, including both immersive and non-immersive virtual reality (VR) systems. Previous studies that explored the potential of video games have shown the positive effect of distraction on the perception of pain; furthermore, past research on VR analgesia has shown how VR can modulate the processing of nociceptive stimulation, offering effective pain management by increasing pain threshold and tolerance both in FM patients and pain-free individuals.8,9 Exergames are video games that require physical exercise to progress, offering low-impact, controlled movements that can effectively distract players from pain. 10 A VR exergame can combine the characteristics of physical training with the benefits of VR and make players perform specific movements recommended in motor rehabilitation. 10 Recent studies have explored immersive and non-immersive systems in contexts such as motor training,6,11–18 relaxation, 8 cognitive-behavioural therapy support,1,5 pain awareness 19 and spatial memory research. 4
This paper proposes a new immersive VR exergame as a tool to educate FM patients in daily motor training. The main objectives are: enabling users to learn and perform the suggested motor activities correctly; exploiting storytelling and missions in the game to increase motivation; promoting relaxation thanks to a virtual natural environment; and enabling home use by using a portable, self-contained, and low-cost VR headset.
The article is organized as follows. First, we survey previous video games and VR systems developed in the context of FM treatment. Then, the Method section describes the proposed immersive VR exergame design for patient education and the design of the pilot test to assess acceptability of the system. The Results and Discussion sections present and discuss the outcomes of the study. The last section concludes the paper, outlining limitations and future research.
Related work
Different previous studies have explored the acceptability of non-immersive video games for FM patients, assessing their effectiveness in improving quality of life, mood, or even physical abilities. In this context, the use of immersive VR with a Head-Mounted Display (HMD) remains limited. In some cases, the games incorporated complementary interventions, such as biofeedback, guided meditation or mindfulness, and showed good potential in reducing acute pain.1,5,7,8,19 Table 1 categorizes video games and immersive VR systems used with FM patients, and Table 2 summarizes the results of related studies.
Categorization of systems used with FM patients.

FM: fibromyalgia.
Studies about the use of video games or VR systems with FM patients.

BFD: biofeedback; CBT: cognitive behavioural therapy; CG: control group;
FM: fibromyalgia; GM: guided meditation; VR: virtual reality.
Exergames for physical and muscular strengthening
As previous studies have shown, exercise training through exergames can boost energy, improve quality of life and cognitive function, and reduce anxiety, depression, and pain.8,16 The standard physical training protocol for FM includes exercises focused on flexibility, strength maintenance, endurance and aerobic conditioning. 8 Motion-controlled video games require autonomous movement of different parts of the body, increasing user's muscle tone, and compliance and reducing movement-related fear caused by continuous pain. 22 Video games and exergames used for training include two immersive VR exergames to improve balance and mobility, 15 one non-immersive exergame specifically designed for FM, with expert-led videos to guide physical conditioning11–14 and several commercial motion-controlled video game consoles that offer exercises to improve mobility and resistance.6,16–18 The studies involving these systems demonstrated the capability of exergames to contribute to treatment both in reducing depression 16 and in reducing pain-related emotions. 18 The results obtained in Gulsen et al. 15 showed that immersive VR systems are promising as an adjunctive therapy for FM patients, in combination with other exercises, with improvements regarding kinesiophobia, pain, level of physical activity and the mental component of quality of life.
Video games for visual-spatial memory
Cánovas et al. 4 used two non-immersive virtual maze environments to examine learning and spatial memory in patients with FM. The environments were navigated in first-person view and contained landmarks to facilitate spatial learning, while auditory feedback was provided. 4 The study identified spatial navigation as a specific cognitive process that appears to be disrupted by FM because patients with FM made more errors than the control group, even though the study demonstrates a reduction in the number of errors and a decrease in searching time with more trials. 4
Video games for relaxation and pain management
Six different studies highlighted how video games and immersive VR are well accepted as a complementary treatment by patients with FM; they also showed an increase in relaxation,5,21 an improvement in perceived quality of life,1,20 a reduction in anxiety,8,19 and a reduction in pain-related sleep interference. 21 Two non-immersive systems used Cognitive Behavioural Therapy (CBT) techniques for the treatment of FM with the aim of offering coping strategies to improve quality of life, achieve relaxation and improve mood.1,5,19,20 Engaging Media for Mental Health Applications (EMMA's) World was originally used for mood induction and emotion activation and processing: users see different natural scenarios where instructions are intended to reduce anxiety, focusing their attention on elements such as sound and images.1,5,20 All the studies that exploit this system1,5,20 revealed its positive effect in reducing FM impact on patients’ lives, making participants more involved during CBT; additionally, the system helps to recall virtual scenario images for practising relaxation and mindfulness at home.1,5 The VirtualPain system was used to reduce pain intensity and associated symptomatology in FM patients. The patient specified the features of the pain experienced by selecting colours and sounds, but the system reported the level of pain experienced using the Visual Analogue Scale (VAS): by modifying the virtual representation of the pain, the patient could modify the perception of its intensity. 19
Darnall et al., 21 through the AppliedVR system, investigated the viability of a self-administered VR program integrating content and skills informed by evidence-based behavioural treatment for chronic pain. Subsequently, the efficacy of the VR program was assessed in terms of improvements in pain intensity, pain-related interference with activity, stress, mood, and sleep, as well as its impact on pain-related cognition and self-efficacy, compared to an audio-only treatment. Patients underwent treatment involving a program that combined skills rooted in pain CBT training, relaxation exercises, and mindfulness. The study demonstrated high engagement, feasibility, and acceptability of the at-home VR intervention, coupled with a reduction in chronic pain outcomes over the 21 days of VR compared to the audio-only version. 21
The EaseVRx system contains two environments, one for the guided meditation and the other for biofeedback, a self-regulation technique by means of which patients can learn how to control no conscious body processes, such as heart rate, muscle tension and breathing. 8 Finally, most of the systems used for FM1,5,6,8,16–18,20 exploit virtual natural environments to stimulate relaxation and encourage anxiety reduction.
Materials and method
The exergame proposed in this paper was designed and developed in the HCI Lab of the University of Udine. The pilot test was conducted in a gym and was aimed to qualitatively assess user acceptability and experience with the proposed VR exergame, focusing on exercise comprehension and the game's strengths and limitations. Additionally, we collected individual measures relevant to FM management. In total, the project spanned seven months.
The proposed exergame
This section introduces our exergame, designed to help FM patients learn motor activities that enhance muscle strength and joint flexibility. The exergame guides patients in executing movements correctly within an immersive virtual environment, supporting accurate practice and physical improvement. Two kinesiologists collaborated in selecting exercises for the exergame and setting guidelines for correct execution. To our knowledge, no prior immersive system has been designed to integrate both physical exercise and relaxation education tailored specifically for FM patients. As highlighted in the Related Work section, prior systems generally lacked a focus on the educational component. Most relied on off-the-shelf video games that were not specifically designed for the needs of FM patients, and only VirtualEx-FM11–14 was an original system developed for this purpose. However, VirtualEx-FM is a non-immersive training, while our exergame is designed to exploit immersive experience.
The design of the system is based on four main decisions.
First, we selected a virtual forest as the setting, enhanced with 3D natural sounds (e.g., wind and bird songs). This choice is supported by previous studies suggesting forest therapy as an effective non-pharmacological treatment for reducing depression and anxiety. 23 Moreover, the selection of a virtual natural environment is typical of many systems developed for FM,1,5,6,8,16–18,20 as it facilitates relaxation among users.
Second, we integrated narrative elements to create an engaging exergaming experience, where motor exercises are embedded in activities designed to advance the storyline. Rewards were included for both individual activities as well as for extended use of the system. Additionally, a voice-over provides encouragement regardless of activity execution, aiming to motivate users and to enhance their self-efficacy.
Third, we paid particular attention to the choice of device, opting for a consumer headset (Oculus/Meta Quest HMD) to develop an exergame that users can potentially use independently in a domestic setting. We chose this device for its lightweight, wireless design, eliminating the need for additional external devices, further increasing the potential for home use. Moreover, the HMD is equipped with in-built cameras that we exploited to track the execution of the exercise. In this way, users of the exergame do not need to hold controllers in their hands, as required by other systems. This allows a more natural execution of the exercises, and also the possibility to use small weights to strengthen muscles during activities. To ensure patients’ safety, and considering that the HMD cameras do not allow to track user's legs, the selected exercises focused on joint mobility of the upper limbs 24 and included three specific movements: forearm flexion and extension, horizontal shoulder circumduction and horizontal arm abduction. Previous studies have demonstrated the effectiveness of dynamic and active stretching aimed at strengthening muscle and improving joint mobility in FM patients16,24; however, experts recommend a level of physical exertion that allows to perform motor activity without excessive pain, along with a gradual progression that provides physiological adaptation, especially for users who may experience physical inactivity due to their symptoms. 25 To enhance adaptability, together with the kinesiologists, we defined three levels of difficulty that can be selected for each session (as shown in Figure 1), allowing the training intensity to be tailored to the user's perceived potential. Before the start of the exergame activities, users are prompted to choose their preferred level of difficulty (simple, moderate or intense) as shown in Figure 1. To ensure a wide range of movement and improve muscle and joints flexibility, the system detects hand position and movement through the in-built cameras of the headset, calculating the total displacement of the limb in the space while performing the different exercises. The number of repetitions is determined by the total displacement of the limb rather than by the difficulty level, as relying solely on difficulty could result in small movements and an inadequate total volume, below recommended levels. Consequently, increasing or decreasing the level of difficulty may result in a corresponding increase or decrease in the number of repetitions of the exercises. Each exercise is designed to be completed in two minutes on each side, according to the physical capabilities of each user and the level selected. Furthermore, to allow for recovery time during training, we introduced specific pauses.

Adapting the difficulty of the experience: (a) Users can select the starting level (easy, moderate or intense) in the central hub; (b) the system proposes a recovery time of 30 seconds when the participant keeps his/her hands below a certain threshold for a given time.
Finally, the system monitors the correctness of performance and provides auditory and visual feedback to educate patients about their motor activity (Figure 2 provides two examples). Specifically, movements should not be performed too fast, and, during the horizontal arm abduction exercise, the palm must be correctly rotated to ensure muscular strengthening.
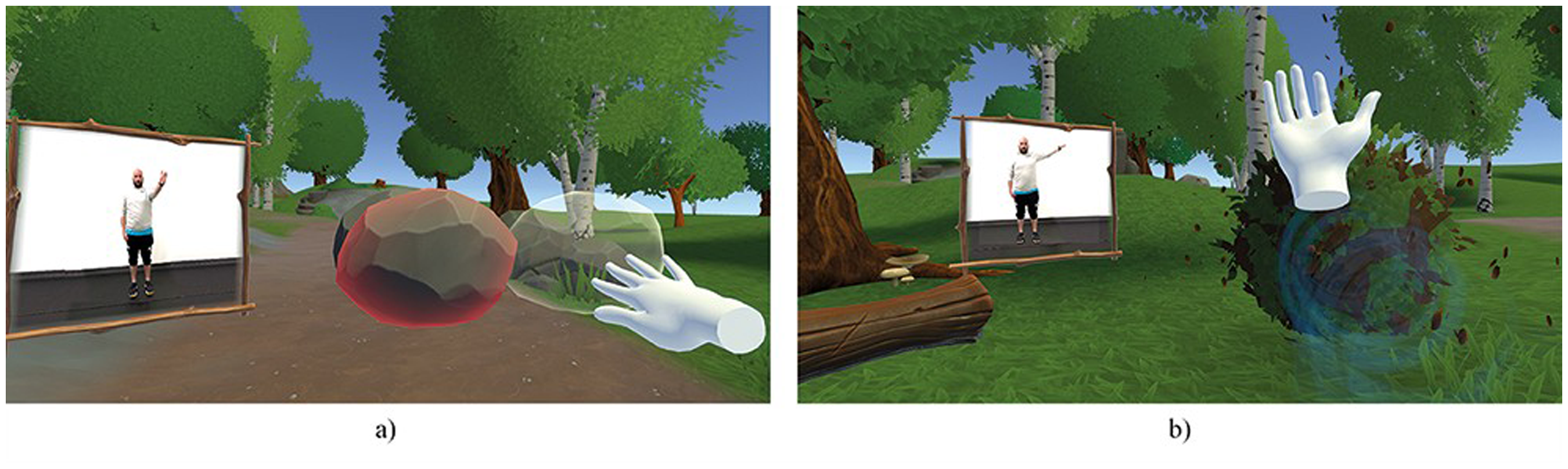
Visual and auditory feedback: (a) Negative feedback example: incorrect speed and execution of the abduction exercise makes the manipulated object glow red, accompanied by an unpleasant sound. (b) Positive feedback example: the bush grows greener when the circumduction exercise movement is performed correctly. The changes occur during arm movement.
To ensure that the exergame supports correct and safe performance, its development followed an iterative approach in which new versions were repeatedly tested by the kinesiologists.
The final game environment is organized in two main areas: a central hub where the user is introduced to the story and can select the level of difficulty, as shown in Figure 1, and an enchanted forest where activities take place. Within the forest, an old magic tree spreads lifeblood throughout its surroundings, sustained by a crystal cluster embedded in its roots. However, a terrible storm has weakened it. The user must complete challenges in order to acquire ‘light points’ which are accumulated inside a crystal that follows the user throughout the adventure. This crystal allows the user to transfer energy to the old magic tree, as shown in Figure 3. As a final reward, at the end of each session, which comprises all three exercises, the user sees the magic tree regaining its vigour proportionally to the energy transferred.

The user collects energy as light points by correctly performing each task during his/her journey in the forest. The energy is released and channelled into the old tree, with visible positive effects on its health.
Within the virtual world, a magic screen (see Figure 2) reproduces real-life videos of each exercise performed by an expert trainer, accompanied by a voice-over to clearly instruct the user about the physical exercises.
A video demonstration of the game is available in the additional materials of this paper.
Participants
Participants were volunteers recruited at the University of Udine and at the rehabilitation section of a fitness centre. The pilot test involved seven female participants aged between 14 and 69. Among them, three were diagnosed with FM according to the 2016 Modified Diagnostic Criteria of the American College of Rheumatology (ACR), 26 while four were healthy volunteers similar for gender, age and Body Mass Index (BMI). Eligibility criteria excluded individuals with major psychiatric disorders affecting reality perception (e.g., schizophrenia, bipolar disorder), conditions limiting joint mobility or physical endurance (e.g., orthopaedic, cardiac, rheumatic, neurological, or respiratory issues), and conditions posing risks for VR exposure (e.g., epilepsy). These criteria were established to exclude participants unsuited for the proposed exergame.
Measures
The demographic characteristics of participants were collected anonymously before the experience.
The protocol included eight FM-related measures: pain level, fatigue, physical strength, muscle stiffness, tiredness, anxiety, stress, depression, each rated on 10 cm Visual Analogue Scale (VAS). Participants marked the eight VAS to reflect what they were experiencing at that moment, before wearing the HMD. When the immersive experience ended, they were asked to do the same, considering the maximum value experienced during the exercise. VAS is a validated tool for assessing subjective experiences, particularly for measuring pain, 27 anxiety and stress. 28
To measure the perceived intensity and effort of each exercise we used the Borg CR scale (R) (CR10) (© Gunnar Borg, 1982, 1998, 2004),29,30 where 0 corresponds to no perceived exertion and 10 is the maximal perceived exertion. This perceived exertion evaluation scale is widely validated and has been used extensively in exercise science to assess perceived exertion. The license to use the scale for measuring the Rate of Perceived Exertion (RPE) was obtained from BorgPerception AB (www.borgperception.se).
The final semi-structured qualitative interview was organized into two modules (as shown in Online Supplemental Material 1): the first explored the immersive VR experience, including strengths and weaknesses and focusing on possible effects on pain and mood, while the second explored participant's opinion of the proposed VR training, as well as comments on device comfort and experience.
Procedure
The pilot test involved individual sessions with each participant. Formal ethical approval was provided by local Institutional Review Board (IRB: 325/2024; Tit III cl 13 fasc.209/2024). Participants provided written informed consent. For the minor participant, a parent provided consent and attended the session. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki. After completing initial questionnaires, participants tried the VR experience, which lasted about 10 min, using an Oculus/Meta Quest 2 HMD. At the end, VAS and RPE scores were recorded, followed by a qualitative interview.
Results
All participants completed the exercises, except for the recently diagnosed, 14-year-old FM participant who found the abduction exercise too difficult. Most participants used the system without issues, and feasibility was further supported by the low exertion levels reported on the Borg CR scale (R) (CR10) (see Table 3).
Table of participants with demographic information (age, gender, level of education and FM), the chosen difficulty level inside the VR training (easy, medium or hard) and RPE results for each exercise using the Borg CR scale (R) (CR10).
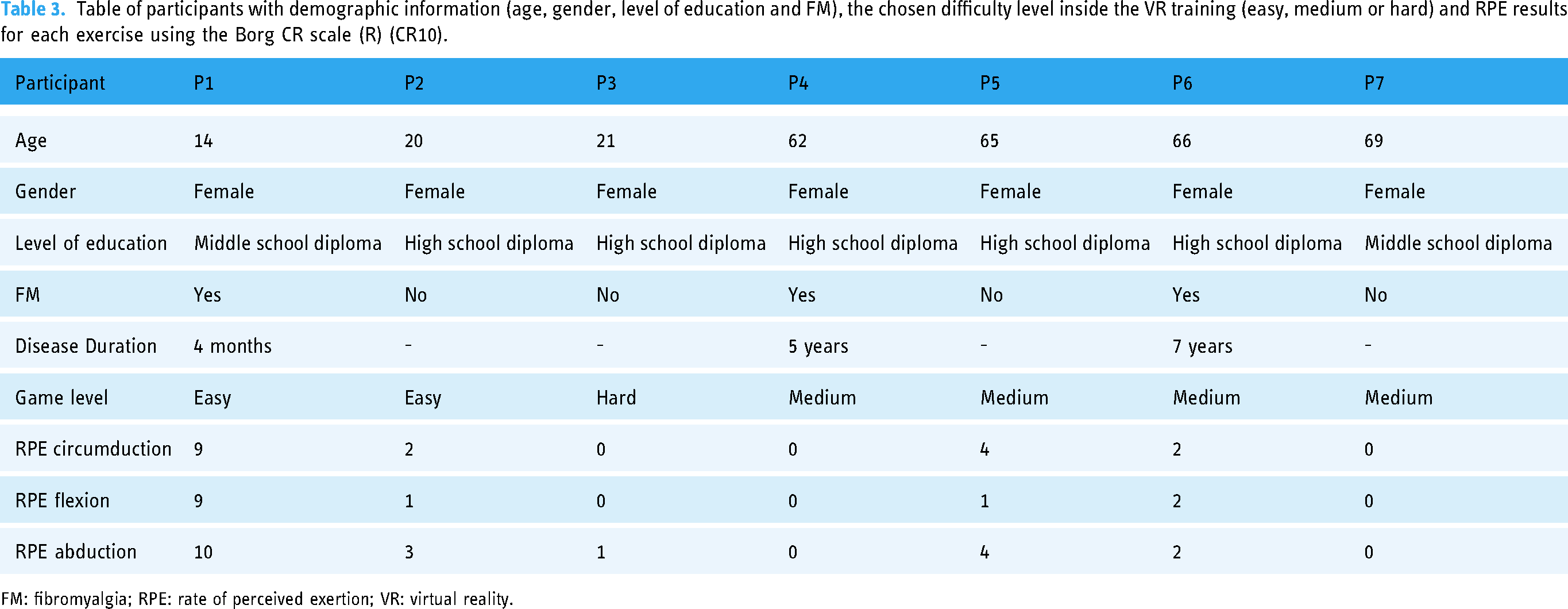
FM: fibromyalgia; RPE: rate of perceived exertion; VR: virtual reality.
Table 4 and its visual representation in Figure 4 report the variation between the values obtained from the VAS questionnaires before the VR experience (pre) and the highest level perceived during the VR experience (max). Participants completed self-evaluations twice: before the VR experience, indicating the highest level for each measure at that moment, and after, noting the highest levels perceived during the exergame. Of the participants, three out of seven reported a slight reduction in pain from baseline to peak levels, two showed stable values, and the remaining two reported an increase, one mild and the other more pronounced. Regarding fatigue and stiffness, a reduction was observed in four out of seven participants, while a minor increase was recorded in the remaining three. Muscle strength was the only characteristic that showed a decline in most participants: two out of seven reported an improvement, four out of seven showed a subjective reduction, and one experienced no change from pre to max. For emotional state, five of seven participants reported improvements in tiredness and stress, with only two showing mild worsening. Anxiety and depression levels improved in four participants. Anxiety remained stable in two participants, with only minimal worsening in one participant; depression remained stable in three participants, with no recorded worsening.
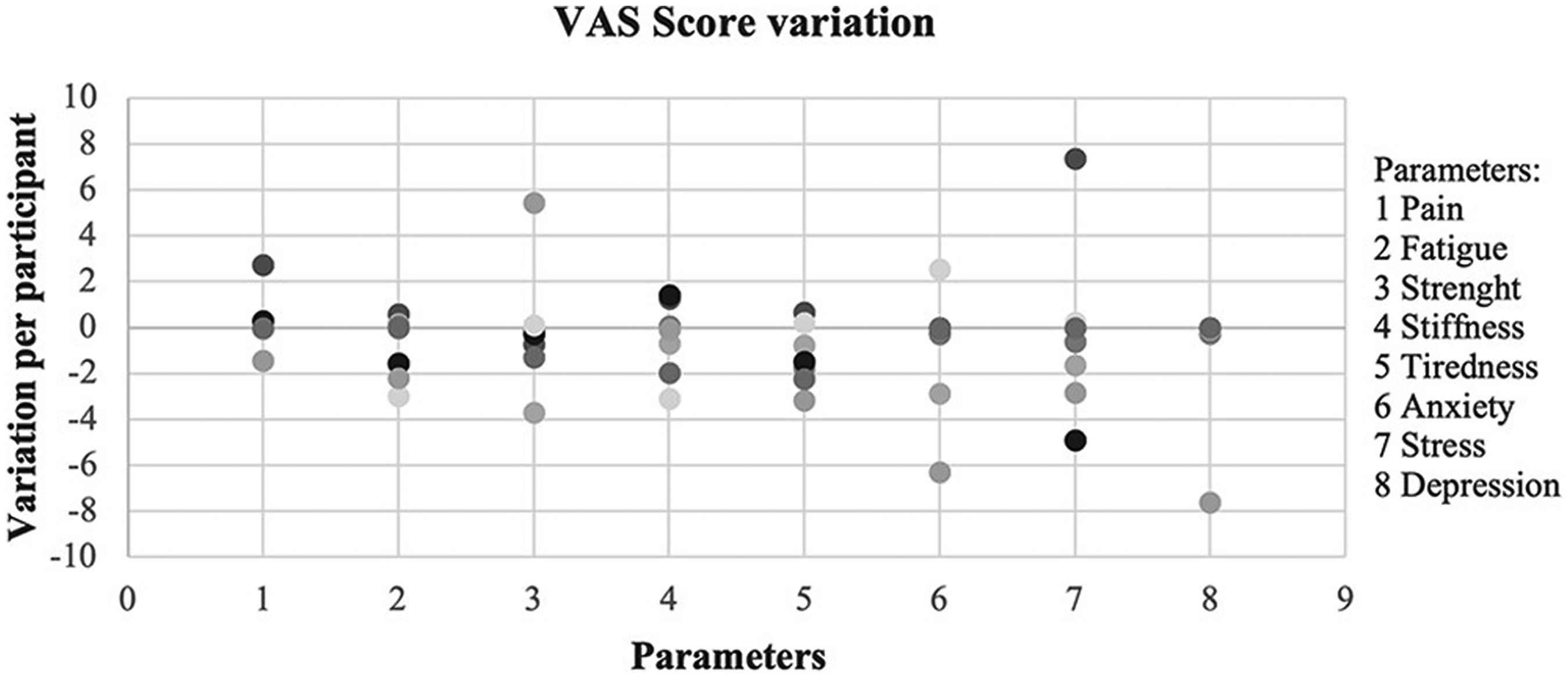
Visual representation of the data in Table 4 showing the variation in VAS scores across eight parameters for each participant. The horizontal axis of the graph displays each parameter's results for individual participants as separate points. The vertical axis indicates the positive or negative change in VAS scores, comparing pre-assessment results with the maximum values recorded during the experience.
Variation of VAS scores across eight parameters (pain level, fatigue, muscle strength, tiredness, stiffness, anxiety, stress and depression). Values represent the difference between pre-assessment level and highest level perceived during the VR experience. Each parameter's variation is shown for all participants.

VAS: Visual Analogue Scale; VR: virtual reality.
Qualitative analysis
Semi-structured interviews were transcribed verbatim and analysed following Braun and Clarke's method
31
: we performed a thematic analysis on the transcripts, identifying prominent themes. In the following interview extracts, the portions in square brackets are words or phrases added to clarify the sentence. The themes that emerged from the interviews are:
Relaxation: participants reported how the exergame promotes a greater relaxation compared with traditional training. Four participants stated that the virtual natural environment helped them to relax: the contributing elements include the virtual forest, sounds and colours. About the exergame, the 66-year-old FM user said: ‘[the exergame] provides greater serenity [than traditional training] because you are more isolated [compared a gym class]. It relaxes you, if it does not include heavy exercises’. Motivation in performing motor activities: participants highlighted the motivational component in performing motor activities. Three participants stated that the game component helped them to finish each activity, motivating them to achieve the goal of the activity, while two participants considered the exercises too simple for them, even compared to traditional training. The 14-year-old FM participant reported that she was able to perform a greater number of repetitions per exercise compared to the weekly gym sessions, which is why the level of pain increased. She said she generally did not enjoy traditional motor activity, but she felt more involved in the exergame than traditional training, and consequently less distracted during the workout. Likewise, the 21-year-old user without FM stated: ‘When I go to the gym, I think that if I do one more repetition I am going to struggle, instead [using this system] I perform a movement without thinking about the effort I am making, so perhaps it leads me to move more’. Increased self-efficacy: visual feedback of each exercise helps reinforce the abilities of participants. Three participants experienced greater self-efficacy because of the tasks. For example, the 21-year-old healthy user stated: ‘I felt a sense of achievement to see the exercise completed […] and the visual feedback of the increased energy in the crystal’. Positive moods: the exergame promotes calmness, contentment, serenity in most of participants. Six participants reported happiness and serenity, five of them also felt satisfied and pleased. For example, the 66-year-old healthy participant said: ‘[I felt] satisfied [because] I succeeded. Pleased because I breathed life back into the tree’. Fun and enjoyment: the game component of the experience is perceived as fun. For example, the 14-year-old FM participant said that the game and fun component engaged her despite experiencing pain and that she felt involved inside the game: ‘You are feeling pain, but you are also having fun’. The two 20-year-old participant without FM stated that ‘it feels like you are not struggling but playing’. Additionally, the 66-year-old FM user said: ‘I feel like a child again […] It was nice to live in that world’. Pain: the exergame impact on pain perception varies depending on the initial pain level before using the game. The participant with higher initial pain levels perceived more pain during the exergame, while those with lower initial pain levels experienced a reduction in pain. Indeed, only the 14-year-old FM participant reported negative sensations like fatigue and catastrophism. Before using the VR system, she reported pain: she could not stand for long, so she asked to play the exergame while sitting. She reported constant pain during her everyday life: ‘I do not like doing motor activity [in general] […] I always feel pain’. Regarding the immersive VR training, she stated: ‘I felt more pain because I did more repetitions [than usual]’. Moreover, in response to the question ‘How capable did you feel in performing the activities?’ the user answered, ‘Very poorly. [I succeeded] with great, great sacrifice and effort’. For these reasons she felt much more pain and was disappointed.
Tables S1 and S2 in the Online Supplemental Material (Qualitative Analysis) list the main responses obtained from the semi-structured qualitative interview on immersive experience and VR training.
Discussion
Consistent with previous studies,1,5,8 our qualitative analysis supports that the immersive VR experience can help distract from pain, while virtual natural environments can enhance relaxation. The immersive nature of VR allowed two participants to report better concentration and relaxation compared to traditional gym training. Our results align with previous findings 18 on exergames’ ability to entertain and distract users from pain and worries. Six participants reported positive emotions, and three emphasized the game's capacity for distraction. The game's rewards also motivated participants, particularly those without FM, enhancing their sense of self-efficacy and satisfaction in contributing to the virtual forest improvement.
The participant who did not complete all three exercises reported that the game dynamics and the isolation from the real environment led her to increase the number of repetitions of the exercises compared with her usual training, despite the higher pain level. She also mentioned that, based on her personal interest, dance exercises would probably have encouraged her more. Interestingly, the youngest participant had a negative experience, while older users reported mostly positive feelings. This suggests that age is not necessarily a limiting factor for this approach and highlights FM's complexity, requiring multifaceted treatment strategies. A range of interventions should therefore be available to address this form of chronic pain. It is interesting to note that a clinical cluster of FM (identified through an unsupervised machine learning approach) has been recently described by Hugle et al. 32 to be more prone to respond to VR interventions, thus highlighting the opportunity of a tailored treatment strategy also in FM. 32
The exercise instructions were clear to all participants, aided by videos of a live instructor within the virtual environment. Two participants, one with FM, reported less muscle pain during the VR experience and found the exercises easier than some they performed regularly in the gym. For this reason, they said they would not consider using the exergame again because it was too easy for them, and one of them considered the training less stimulating because of the absence of direct contact with the instructor. The other five participants stated that they would instead use the exergame again, as an adjunct to traditional gym training or independently at home, to relax through exercise. Finally, the exergame appeared to be generally well accepted both for motor activities and for relaxation. In terms of overall experience, all users reported a high level of enjoyment of the immersive exergame and a sense of satisfaction and accomplishment. Three users without FM reported that they were happy to have contributed to creating a more beautiful and stronger forest, indicating a sense of involvement within the immersive experience. In addition, two participants reported a shorter perceived experience, a phenomenon known as time compression. 33 The findings demonstrated the overall feasibility of the proposed exergame for both healthy individuals and FM participants. Notably, users reported improvements in depression, stress and anxiety levels during the use of the immersive exergame, which were lower than their pre-immersive VR experience values. This highlights the potential of the intervention to provide immediate psychological benefits even during the activity.
According to the most recent European recommendations for the management of FM, exercise is strongly recommended as a non-pharmacological treatment capable of improving pain and physical function. 3 However, patients with FM often exhibit a greater tendency toward sedentary behaviour compared to healthy individuals, which is related to fear of movement due to potential pain exacerbation, fatigue and associated depressive states.34–36 Our exploratory study suggests that immersive exergames could help address these limitations by making physical activity more engaging, providing a distraction from chronic pain and promoting relaxation, self-efficacy, and motivation. The potential to use a low-cost, self-contained headset at home to independently perform immersive exergame interventions, combined with the opportunity to offer a wide variety of exercises across adjustable difficulty levels in customizable, engaging virtual environments, may improve treatment adherence and sustain patient motivation over the long term. Indeed, longitudinal efficacy studies in FM patients with longer durations, as well as clinical trials comparing exergames with traditional physical exercise, are necessary to confirm the possible benefits suggested by our exploratory pilot study.
To improve efficacy and motivation through our approach, future research and development should include a calibration protocol to adapt the difficulty of each exercise to individual pain levels and physical capabilities. At the beginning of the experience an initial tutorial to familiarize users with basic game movements could also be included, in order to perform key and standardized movements (e.g., arm raises) to assess patient's limits and motor capabilities, along with a posture check to ensure comfort and stability during the experience (e.g., standing or seated position). Based on the data collected, the difficulty of each exercise could be customized to the user's potential and current capabilities, allowing for both the intensification and simplification of training as needed. This initial calibration could be important, because users with FM may experience varied and inconsistent joint and muscle pain across different sessions. Moreover, an extension of the system with lower limb sensors, as current consumer headsets unfortunately do not track legs, would support full body dynamic training for users with greater physical strength and less joint pain. Finally, the integration with other non-pharmacological interventions, which can be delivered by smartphone apps, should be considered. 37
Some limitations of this study need to be mentioned. First, the pilot study involved a small sample size of heterogeneous participants that does not allow for a quantitative statistical analysis of within- or between-groups comparisons. The small sample size and participant heterogeneity also make it difficult to generalize our qualitative findings to a larger clinical population. The participant group consisted exclusively of females, so future studies should aim for a larger sample that better reflects the gender distribution, various FM diagnoses, and age ranges. Second, we did not consider a control group that performed the same exercise without using VR. Moreover, our data come from a single VR session, without a long-term evaluation. Third, although the VAS is validated for measuring pain and various emotional states, the self-formulated order of assessment (level of pain, fatigue, physical strength, muscle stiffness, tiredness, anxiety, stress and depression) may limit the findings. Finally, this pilot study primarily aimed at exploring whether VR exergaming could be used as a patient education tool for FM, rather than to demonstrate its efficacy.
However, this study also introduces, for the first time, an immersive exergame as a potential non-pharmacological, multimodal treatment for FM, addressing some limitations of conventional physical therapy. Additionally, the ability of the immersive exergame to promote relaxation, positive mood, enjoyment and engagement may provide psychological benefits for FM patients. Notably, there were reductions in depression, stress and anxiety for most participants during the immersive experience, suggesting potential for early relief, at least in a subset of patients.
Conclusions
This study proposed a new immersive VR system for independent home use, designed to engage and educate FM patients in recommended physical activities. To our knowledge, this is the first immersive VR exergame for FM patients that uses in-game narrative to enhance user experience. Our preliminary findings are promising, supporting the feasibility, motivational potential, and benefits of an integrated immersive VR exergame system for both healthy individuals and FM patients. If these promising results are confirmed, a refined system that automatically adjusts activities to individual patients could be tested in clinical trials. Such a system could become part of multidisciplinary rehabilitation or physiotherapy programs for FM patients. Future studies with larger samples and longer follow-up will be essential to confirm these findings and explore the potential of immersive VR exergames in FM treatment protocols.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241304904 - Supplemental material for An immersive virtual reality exergame as a patient education approach in fibromyalgia: Pilot study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241304904 for An immersive virtual reality exergame as a patient education approach in fibromyalgia: Pilot study by Cassandra Lucia Bardelli, Luca Chittaro, Simone Longhino and Luca Quartuccio in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241304904 - Supplemental material for An immersive virtual reality exergame as a patient education approach in fibromyalgia: Pilot study
Supplemental material, sj-docx-2-dhj-10.1177_20552076241304904 for An immersive virtual reality exergame as a patient education approach in fibromyalgia: Pilot study by Cassandra Lucia Bardelli, Luca Chittaro, Simone Longhino and Luca Quartuccio in DIGITAL HEALTH
Supplemental Material
Footnotes
Acknowledgements
We are grateful to Andrea Costabile and Giuseppe Currò for sharing their expert knowledge on physical training and providing feedback that proved very valuable in developing the application.
Contributorship
CLB: Software, formal analysis, investigation, writing – original draft.
LC: Conceptualization, methodology, resources, writing – review & editing.
SL: Writing – review & editing.
LQ: Methodology, writing – review & editing.
Consent to participate
All adult participants provided written informed consent prior to participating, and a written informed consent to participate in this study was provided by the legal guardian of the minor participant.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was provided by local Institutional Review Board (325/2024; Tit III cl 13 fasc.209/2024).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Guarantor
CLB.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.