
Abstract
Objective
While mobile health-based human immunodeficiency virus (HIV) interventions are often designed to promote health equity, systematic differences in the use of and access to mobile technologies may counteract that and widen treatment gaps. This systematic review applies an equity lens to investigate whether existing research provides adequate evidence on the ethical implications of mHealth technologies in HIV treatment and prevention.
Methods
This study included a two-stage methodology, consisting of (a) a systematic review of systematic reviews and (b) an evidence synthesis of primary studies. For the review of reviews we searched eight electronic databases, eight electronic journals and Google Scholar. We also screened reference lists and consulted authors of included studies. Primary studies were extracted from eligible reviews. We based our data extraction and analysis on the Place of residence, Race, Occupation, Gender/Sex, Religion, Education, Socioeconomic status, Social capital and other disadvantage related characteristics (PROGRESS-Plus) framework and the use of harvest plots, focusing on the socio-demographic distribution of mHealth effects.
Results
A total of 8786 citations resulted in 19 eligible reviews and 39 eligible primary studies. Existing reviews did not provide any analyses of the equity impacts of mobile health-based HIV initiatives. Information availability was higher in primary studies, predominantly suggesting no social gradient of mobile health-based HIV interventions. Overall, evidence remains weak and not sufficient to allow for confident equity statements.
Conclusions
Despite the negative force of socio-demographic inequities and the emerging nature of mobile health technologies, evidence on the equity implications of mobile health interventions for HIV care remains scarce. Not knowing how the effects of mobile health technologies differ across population subgroups inevitably limits our capacities to equitably adopt, adjust and integrate mobile health interventions towards reaching those disproportionally affected by the epidemic.
Introduction
As access to mobile devices increases, new digital interventions and the digitalization of health are perceived as a unique opportunity to reduce human immunodeficiency virus (HIV) incidence and improve antiretroviral treatment. 1 , 2 Mobile health (mHealth) is one of the most rapidly expanding digital health domains and is defined as the use of mobile communication devices for a wide range of healthcare purposes. 3 Its application in the field of HIV care has been pioneering, employing a variety of technologies such as text messaging, remote voice counselling, reminder systems and multifunctional health applications (apps). 2 ,4–6 Existing research highlights the value of mHealth tools for HIV treatment and prevention, with evidence suggesting reduced sexual risk, improved adherence to antiretroviral therapy, 1 , 2 stronger educational and community outreach, enhanced retention to care and better overall surveillance. 5 Considering the required resources for effectively providing conventional HIV programmes, digital alternatives are expected to improve fidelity at lower costs and at increased scale and personalization. 7 , 8 Promising to improve access to HIV services, mHealth interventions should facilitate the inclusion of hard-to-reach groups and disadvantaged populations, promoting equitable care. 9 Despite their potential, that promise is not without challenges. Various socio-demographic, behavioural and structural factors might hinder accessibility and use, leading to an inequitable distribution of mHealth benefits, limiting their overall potential, and raising ethical concerns. 10
Applying an equity lens
The World Health Organization (WHO) defines health equity as ‘the absence of avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically’. 11 Inequities are a key driver of the HIV epidemic and are primarily rooted in socio-demographic factors (e.g. income, employment, gender, ethnicity, education, place of residence, etc.), which in turn lead to differential health outcomes (e.g. better health outcomes for higher educated, higher income subgroups).12–15 These are further exacerbated by stigma and marginalization, primarily targeting vulnerable populations, including men who have sex with men (MSM), sex workers, injecting drug users and ethnic minorities. 16 While mHealth promises to facilitate equitable healthcare, robust evidence on the validity of that promise remains insufficient. 9 , 10 , 17 In fact, determinants that drive the HIV epidemic, such as poverty, social exclusion and stigma, are also factors that limit the use of and access to mHealth technologies, further widening existing health disparities, even if improving overall health outcomes. 18 Those disparities are rooted in the ‘digital divide’ phenomenon, defined as the gap between those who benefit more and those who benefit less from digitalization, leaving the more disadvantaged with fewer benefits. 10
Acknowledging the equity dynamics of both the HIV epidemic and mHealth interventions, this study aims to identify, assess and synthesise existing research evidence on the distributional effects of mHealth interventions, targeting HIV treatment and prevention, across a set of core socio-demographic and equity-related determinants. This study also aims to underline potential evidence gaps and emphasise the importance of addressing equity in health research and practice. This will ultimately facilitate our understanding on the ability of mHealth interventions to equitably reduce the global burden of HIV and acquired immunodeficiency syndrome (AIDS).
Methods
Our method has been successfully applied in previous equity-focused research 19 , 20 and entails two stages, hereafter referred to as Stages 1 and 2. The first stage consisted of a systematic review of systematic reviews and the second of an evidence synthesis of eligible primary studies, pooled from the included reviews. In both stages, we aimed to explore the equity implications of mHealth-based HIV care. We identified and synthesised information on the distribution of the effects of such interventions across equity-relevant socio-demographic variables that are associated with being disproportionally affected by HIV. For the purposes of this study, disadvantage is conceptualised as any determinant, context or circumstance that increases exposure to HIV, risk of infection, risk of disrupted treatment, and risk of disease progression. Our justification for the second stage is based on previous research, suggesting that although equity evidence should ideally be reflected in existing systematic reviews, this is not guaranteed and often not the case. 21 Reviewing the primary studies in the included reviews allowed us to investigate whether systematic reviews collected, analysed and reported all available equity-relevant information. 22 Our study follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 23
Search strategy and information sources
For Stage 1, we systematically searched eight electronic databases, including Medline, EMBASE, CINAHL, PsycINFO, Web of Science, Global Health, the Cochrane Database of Systematic Reviews and WHO Global Index Medicus. Targeting comprehensiveness and sensitivity, the selected set of databases was chosen to allow for a broad and multidisciplinary scope. We also hand-searched the Journal of Medical Internet Research, the International Journal of Electronic Healthcare, E-Health Telecommunication Systems and Networks, the e-Journal of Health Informatics and SAGE Health Informatics Journal. Google Scholar was used to complement the electronic search. Finally, we screened all reference lists of included reviews and contacted nine authors for potentially missed or unpublished reviews. The search strategy was designed to combine mHealth, digital health, and HIV terms and is available in Supplemental Material Appendix A. The searches were run on 25 October 2017.
Study selection and eligibility criteria
We defined mHealth interventions as any intervention using mobile devices for communication, consultation, and education purposes; 6 the target group of these are either healthy individuals (at risk to contract HIV) or HIV positive patients. Interventions that targeted healthcare providers were excluded. Other technological devices (i.e. computers/laptops) were also excluded as they are predominantly treated as a distinct category, referred to as computer-based interventions. 5
HIV treatment and prevention were conceptualised as any intervention or policy that aims to reduce HIV incidence and risk, as well as improve treatment outcomes through retention and adherence. Relevant outcomes included any prevention or treatment-related measures, whether subjective, directly observed or objective (e.g. testing uptake, HIV incidence, behavioural change, CD4 cell counts, cluster of differentiation 4 (CD4) loads, pill counts, pharmacy refills and electronic monitoring).
At both stages, studies went through a two-step selection process, consisting of (a) title and abstract screening and (b) full-text appraisal. Studies were screened by two independent reviewers and disagreements were resolved by consensus. To be included in Stage I, reviews required a clearly articulated research aim and a search strategy of at least (a) two or more databases or (b) one database and at least one complementary source (e.g. hand searching). In addition, eligible reviews had to examine the effects of mHealth interventions for either HIV prevention or treatment. To be included in Stage 2, primary studies had to be included in at least one of the eligible systematic reviews. In addition, they had to examine the effects of mHealth interventions for either HIV treatment or prevention, using experimental or quasi-experimental methods. Studies from either stage have been excluded if they were not written in English.
Data extraction and quality appraisal
Data extraction was guided by previous reviews on health equity implications of social interventions. 19 , 20 , 22 To explore the equity implications of mHealth-based HIV initiatives, we used a framework introduced by Evans and Brown (2003) and expanded by Oliver and colleagues (2008). 24 , 25 It includes the following set of socio-demographic and other inequity-driving determinants: Place of residence, race/ethnicity, occupation, gender, religion, education, socioeconomic status (SES) and social capital. 26 The framework is called PROGRESS-Plus, using the first letter of each determinant and the ‘plus’, which denotes additional equity-relevant characteristics. We added three further relevant variables, including age, sexual orientation and substance abuse. To explore equity implications, we searched for data on the distribution of intervention effects across PROGRESS-Plus elements, which we labelled as ‘equity evidence,’ as well as for any other addressing of PROGRESS-Plus elements, labelled as ‘equity-relevant information.’ We conceptualised equity evidence as (a) the results subgroup and (b) interaction analyses; and equity-relevant information as (a) the availability adjusted associations and (b) the provision of baseline demographics. These four data types were extracted from all included reviews and primary studies.
When reviewing existing evidence, whether retrieved from primary research or reviews, it is essential to consider its quality. Synthesising larger quantities of evidence without any quality assessment bears the risk of misleading interpretations, such as significantly overestimating evidence strength, especially if most of it is based on low-quality methodologies. Therefore, at Stage 1, the quality of systematic reviews was assessed using a measurement tool to assess systematic reviews (AMSTAR). 27 , 28 At Stage 2, the quality of primary studies was determined by their methodological rigour, described in Table 1. 19 , 20 , 29 , 30

HIV: human immunodeficiency virus.
Data synthesis
Our data synthesis followed a narrative approach. Equity evidence of primary studies was visualised in harvest plots, which evaluate equity implications through three social gradient hypotheses. 31 The null hypothesis represents ‘no social gradient’ (e.g. no differential effects between subgroups), meaning no impact on inequities, reflected by non-statistically significant subgroup or interaction analyses. The first alternative hypothesis supports a ‘positive gradient’, suggesting better outcomes (effects) for advantaged groups and indicating widening inequities. The second alternative hypothesis supports a negative social gradient, which suggests better outcomes (effects) for disadvantaged groups and thus, a narrowing inequity gap. 31 The harvest plot also incorporates the quality appraisal score and outcome metrics of each primary study, which visually illustrates evidence strength. All plot elements are detailed in Table 1.
Results
Stage 1: review of reviews
Our search strategy yielded 8786 citations and the final inclusion of 19 systematic reviews, published between 2007–2017. Most of them have adopted a comprehensive approach to HIV, concurrently focusing on HIV treatment and prevention (n = 10), followed by a smaller number of studies exclusively addressing treatment (n = 7) or prevention (n = 2). Broadly classified, six reviews addressed mHealth in general, not focusing on specific mHealth components, such as messaging. Five reviews specifically focused on mobile text messaging interventions, and eight addressed mHealth within a wider digital and electronic health (eHealth) context, including electronic reminder devices, mobile applications, and voice-based mobile phone counselling. The methodological quality of reviews ranged between zero (very low) and 11 (very high) AMSTAR-points, with an average of five points. That indicates a large between-study variation and an overall tendency towards mid- to low methodological quality, suggesting the need for careful interpretation. Supplemental Material Appendix B provides a list of all included reviews. Figure 1 presents the PRISMA flow diagram of the screening and review process. 23

Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram of screening and review process of systematic reviews. HIV: human immunodeficiency virus; m-Health: mobile health.
Equity evidence and equity-relevant information in systematic reviews
The included systematic reviews were neither purposively developed to assess differential mHealth effects across equity-relevant socio-demographic variables nor included any form of evidence on HIV-related equity impacts. In fact, the word ‘equity’ or ‘inequality’ was not mentioned in any of the study backgrounds or methodology sections. None of the identified reviews conducted or retrospectively reported subgroup analyses or interaction effects across any of the PROGRESS-Plus items. Based on these findings, it remains uncertain whether there is a relationship between mHealth interventions and HIV inequities related to treatment and prevention.
Equity-relevant information
None of the reviews reported adjusted associations and only four provided detailed baseline demographic data across six out of 11 PROGRESS-Plus items. Ethnicity (n = 4) and gender (n = 3) were the most commonly reported characteristics, followed by sexual orientation (n = 2), education (n = 1), occupation (n = 1) and place of residence (n = 1). Ten studies included less-detailed information on baseline demographics by commenting on the overall target population without providing information on sample compositions. Two out of all included studies focused on vulnerable subgroups, including MSM, 32 pregnant women, ethnic and sexual minorities, incarcerated, transgender, and injecting drug users. 33 None but two of the reviews had a specific regional focus, both on Africa. 34 , 35
Several reviews directly or indirectly acknowledged the importance of addressing equity, either by highlighting evidence gaps, by providing recommendations or expressing equity concerns. 5 , 33 ,35–39 Catalani et al. and Devi et al. suggest a missing focus on key disadvantaged populations, such as injecting drug users and MSM, despite lower chances of intervention uptake due to stigma and discrimination. 5 , 39 Similarly, Forrest et al. underline the need to address equity and highlight that the drivers of health inequities also restrict access to, and reduced use of, mHealth interventions. 35 This pattern implies that many researchers in the field are aware of, and often concerned about, differential effects of mHealth technologies. The review’s second stage aimed to assess if the lack of equity focus is due to missing attention by reviews or insufficient evidence from primary studies.
Stage 2: primary study evidence synthesis
The 19 included systematic reviews examined a total of 513 primary studies, of which 39 fulfilled all eligibility requirements and were synthesised. Most interventions addressed either treatment and medication adherence (n = 29) or prevention (n = 10), with one addressing both. As reflected in the systematic reviews (Stage 1), the majority of studies evaluated the effects of text messaging (n = 21). Most studies applied randomised experimental designs (n = 36), with the remaining (n = 3) being quasi-experiments. In terms of methodological quality, most studies (n = 29) scored four points or higher, suggesting a relatively high evidence strength. Supplemental Material Appendix C includes individual study scores and applies a data extraction matrix adapted from Humphreys and Ogilvie. 19
Equity evidence synthesis
Although the availability of subgroup analyses and interaction effects across PROGRESS-Plus items remains limited, the primary studies contained greater information than the systematic reviews, visualised in Figure 2. Nonetheless, none of the studies exclusively focused on equity, while five assessed mHealth effectiveness across one or more PROGRESS-plus-defined subgroups and another five tested interactions between PROGRESS-Plus variables and the respective mHealth interventions. These data act as indications on whether intervention effects significantly vary across different levels of socio-demographic determinants.
Harvest plot of subgroup analysis results in primary studies. Each bar represents a primary study. Bar position represents the supported hypothesis. Bar color reflects the utilized human immunodeficiency virus (HIV) outcome measure (white = observation, grey = self-reported, black = objective measures). The numbers within each bar correspond to the study number provided by Supplemental Material Appendix C. The number above each bar represents study quality. A more detailed account of each harvest-plot element is provided by Table 1.
Subgroup analyses
Within the five studies that included subgroup analyses, only two referred to a priori definitions. 40 , 41 Three studies did not refer to any protocol-based justification and are therefore categorised as ‘post-hoc’ analyses, which are less trustworthy and prone to biases.42–44 Figure 2 synthesises the subgroup analysis results in line with the three social gradient hypotheses.
As Figure 2 displays, all reported subgroup analyses support the null hypothesis of no social gradient. While this suggests that mHealth interventions have no impact on HIV-related inequities, the confidence of this statement is reduced by the small number of studies reporting subgroup analyses.
Interaction effects
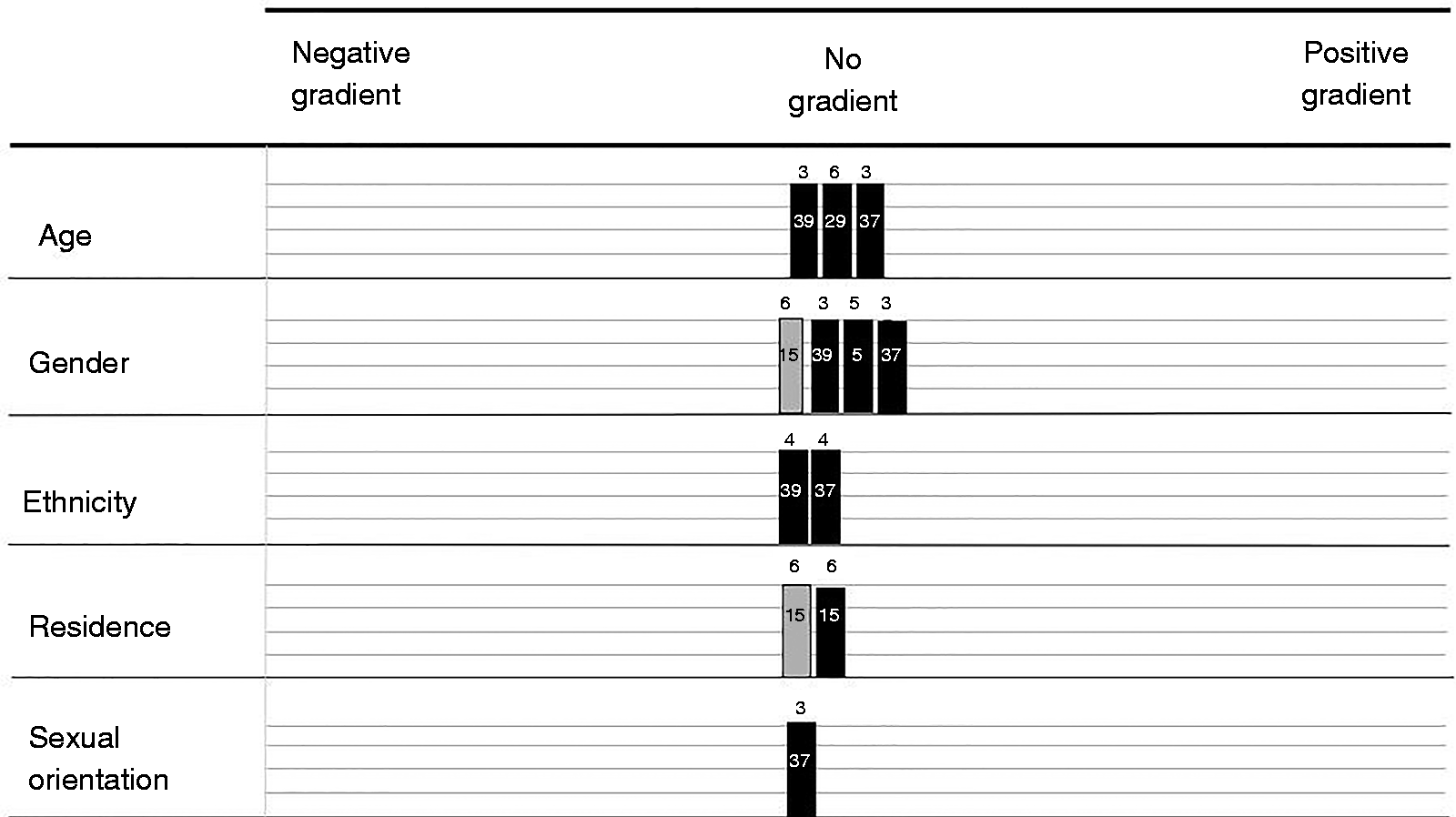
The five studies that reported interaction terms covered all PROGRESS-Plus items except religion, social capital and occupation. As the second harvest plot (Figure 3) shows, all analyses that tested interactions with place, gender, ethnicity, sexual orientation, substance abuse and SES (conceptualised as income) were non-significant.45–48 This was also the case in three out of four studies that tested interactions with age, 41 , 47 , 48 while one 45 found that mobile phone call reminders result in higher healthcare uptake with increasing age, suggesting that young people were left behind. Interactions with education were mixed, with one study supporting the null hypothesis 48 and one study indicating a positive gradient (better outcomes for higher educated). 47 None of the interaction analyses support the negative social gradient hypothesis (better outcomes for disadvantaged subgroups).

Harvest plot of interaction effects results in primary studies. Each block represents a primary study; Bar position represents the supported hypothesis. Bar color reflects the utilized human immunodeficiency virus (HIV) outcome measure (white = observation, grey = self-reported, black = objective measures). The numbers within each bar represent the study citation, corresponding to the study numbers provided by Supplemental Material Appendix C. The number above each bar represents study quality. A more detailed account of each harvest-plot element is provided by Table 1.
Equity-relevant information
The availability of adjusted associations and baseline demographics across PROGRESS-Plus items is proportionally greater in primary studies than in the systematic reviews. Several studies reported intervention effects adjusted for age (n = 8), gender (n = 6), education (n = 5), residence (n = 2), SES in form of income and employment (n = 2), substance abuse (n = 2) and race and ethnicity (n = 1). Four out of the eight studies that reported age-adjusted associations found significant links between age and HIV outcomes. 43 ,48–50 Three linked higher age to improved medication adherence, lower viral loads and higher healthcare attendance, 43 , 48 , 50 while one linked higher age to increased sexual risk. 49
Three out of five education adjustments found significant associations between education and HIV outcomes, 41 , 45 ,47–49 linking education to better healthcare uptake and lower sexual risk. 45 , 47 , 49 Only one out of of six gender adjustments reported significant results, with females being more likely to adhere less to medication and have higher viral loads. 43
These results do not provide any evidence on actual equity impacts of mHealth interventions, but rather offer indications of how socio-demographic variables might present an advantage or disadvantage through their relation to study outcomes. In fact, most significant results suggested associations between socio-demographic disadvantage, such as young age, female gender or lower education, and worse HIV-related outcomes. All but one study provided baseline socio-demographics for at least one PROGRESS-Plus item, in total covering all 11 PROGRESS-Plus items. 51 The wide availability of baseline demographics suggests that determinants related to HIV-inequities are comprehensively and routinely reported in primary research.
Discussion
Evidence on the distribution of mHealth effects across factors that drive health inequities should act as an important resource for the development of interventions and policies that can reach those disproportionally affected by HIV and AIDS. Nonetheless, in line with previous equity-focused research, 21 , 52 the first part of this study highlights that systematic reviews provide no evidence on potential equity impacts of mHealth interventions. Although most reviews provide brief sample characteristics, only a few reported detailed socio-demographic information. The observed scarcity of detailed baseline data inevitably limits our ability to apply the findings to socially disadvantaged subgroups. Only 20% of the identified mHealth reviews focused on disadvantaged populations, which is surprisingly low compared to the general HIV literature; a review of reviews on HIV prevention interventions highlights that almost 50% of all identified studies specifically targeted vulnerable and socially disadvantaged subgroups. 53 Reviews focused on subgroups are often excluded from equity-focused search because of apparent limitations of conducting distributional analyses. 19 Nonetheless, this review did not exclude any focused review because HIV-related inequities can equally occur within socially disadvantaged groups as within the general population.
Primary research versus systematic reviews
Eligible primary studies provided proportionally more equity-relevant information than the systematic reviews. Nonetheless, only two studies were designed to evaluate differential mHealth effects across PROGRESS-Plus items, 40 , 41 while three conducted less trustworthy post-hoc analyses42–44 and only five reported interactions between mHealth effects and socio-demographic variables. 41 ,45–48 This suggests that the missing equity focus in systematic reviews is potentially attributable to limited primary evidence. While one could argue that reviews could have synthesised existing evidence, albeit scarce, it is likely that the methodological and conceptual challenges did not incentivise authors to do so. Most primary evidence supported the null hypothesis of no social-gradient and is in total too scarce and of limited methodological quality to allow for any confident statements on the role of mHealth in HIV disparities.
Equity lens: methodological and conceptual challenges
To better understand why the identified mHealth studies fail to comprehensively account for equity, it is essential to acknowledge the methodological and conceptual challenges of equity-focused research. Conducting subgroup analyses, which rely on fulfilling a strict set of methodological criteria, is one of such challenging and debatable approaches. 21 , 54 , 55 Inadequate sample sizes, often only powered to the primary outcome of medication adherence, are potentially a key obstacle to conducting and reporting reliable subgroup analyses with regard to this study’s question. Petticrew and colleagues describe subgroup analyses as a dilemma, which forces researchers to choose between policy relevance and statistical rigour. 21 Despite those challenges, the question of why prospectively designed trials are not sufficiently powered to comprehensively address the theoretically sound topics of equity and digital divide remains unclear. Is it lack of awareness, practical challenges, methodological and conceptual obstacles or simply missing prioritization? This question remains to be explored and should be addressed by future studies.
Missing equity evidence: the implications
The overall missing equity focus is surprising for several reasons. First, the digital divide is a well-established topic, with evidence clearly suggesting that discrepancies in eHealth literacy and utilization skills remain dominant. 56 Those gaps potentially limit e- and mHealth benefits to already better-off socio-demographic groups, dismissing those in highest need. 18 Second, mHealth interventions are often specifically based on the promise of flexibility and reach, enabling the inclusion of vulnerable and remote populations. 9 , 17 Not assessing whether that promise of inclusiveness and equitability holds, hinders our understanding of whether mHealth technologies reach their fullest potential. In fact, interventions and programmes that aim to improve health but widen inequity gaps should be categorised as ineffective (or only partially effective). Third, although current mHealth studies evaluate small-scale initiatives, international organizations recommend scale-ups (e.g. their integration with existing national-level HIV programmes). 57 Such large-scale approaches may inevitably exert larger population-health effects, which in turn require careful consideration of structural barriers for socially disadvantaged subgroups. 18 In other words, the prospect of scale-ups might increase the unintended equity consequences of mHealth interventions, further increasing, instead of reducing socio-demographic health discrepancies. Fourth, HIV remains a disease that disproportionally affects socially marginalised groups. It is an ethical responsibility to conduct and foster research that is sensitive to those inequalities. Capturing differential effects at early stages can counteract such barriers, ensuring that those disproportionally affected by HIV benefit equally, ultimately mitigating further marginalization. Ignoring differential effects will most likely limit our abilities to create a global HIV response that will truly impact on HIV-related inequities.
Limitations
The results of this study need to be viewed in consideration of the following methodological and conceptual limitations. Interpretations require full awareness of the applied mHealth conceptualization, which was purposively restricted to mobile technology devices. Primary studies have been exclusively extracted from the reference and inclusion lists of the 19 examined systematic reviews. This may not be representative of, and generalisable to, the overall primary literature on mHealth technologies for HIV treatment and prevention.
Synthesising evidence according to three social gradient hypotheses cannot be interpreted as statistical hypothesis testing. Although primary data result from statistical tests, the harvest plots are not based on statistical synthesis, confidence intervals, or overall effect sizes. 31 Statistical validity requires further analysis and more primary evidence. The evidence synthesis approach adopted by this study is described by Humphreys et al. as a short-term, however, practical solution to overcoming the statistical constraints of conducting subgroup analyses. 19 Efforts must be made not to over-interpret potentially unreliable data in the harvest plots.
Conclusions
Our findings emphasise a substantial evidence gap in the equity impact of mHealth-based HIV treatment and prevention interventions. Neither systematic reviews nor their primary studies provide evidence of adequate quantity or quality on whether mHealth-based HIV initiatives differentially affect socio-demographically disadvantaged subgroups. Nonetheless, equity-relevant information, especially baseline socio-demographics, was larger in primary studies than in systematic reviews, suggesting that valuable data are available and potentially underused. It should be in the interest of those who develop and apply those interventions, including policy-makers and public health professionals to better understand whether, how and under what circumstances mHealth interventions can indeed overcome the digital divide and fulfil their potential. That knowledge gains in importance when targeting diseases that are grounded in inequities, such as HIV and AIDS. As mHealth-based HIV interventions mature, effective scale-ups will depend on informed policy-making, requiring reliable and robust evidence on how mobile technologies operate within diverse communities and heterogeneous populations. Future research should equip policy-makers and practitioners with the needed evidence-base to adopt, adjust, and integrate promising mHealth solutions to tackle the HIV epidemic. Not knowing how mHealth effects distribute across factors that drive health inequities inevitably limits our capacities to timely adjust new and promising interventions towards reaching and benefiting those disproportionally affected by HIV.
Supplemental Material
sj-pdf-1-dhj-10.1177_2055207620942360 - Supplemental material for Exploring the equity impact of mobile health-based human immunodeficiency virus interventions: A systematic review of reviews and evidence synthesis
Supplemental material, sj-pdf-1-dhj-10.1177_2055207620942360 for Exploring the equity impact of mobile health-based human immunodeficiency virus interventions: A systematic review of reviews and evidence synthesis by Vasileios Nittas, Vira Ameli, Madison Little and David K Humphreys: EUROTRACS Investigators in Digital Health
Supplemental Material
sj-pdf-2-dhj-10.1177_2055207620942360 - Supplemental material for Exploring the equity impact of mobile health-based human immunodeficiency virus interventions: A systematic review of reviews and evidence synthesis
Supplemental material, sj-pdf-2-dhj-10.1177_2055207620942360 for Exploring the equity impact of mobile health-based human immunodeficiency virus interventions: A systematic review of reviews and evidence synthesis by Vasileios Nittas, Vira Ameli, Madison Little and David K Humphreys: EUROTRACS Investigators in Digital Health
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
VN contributed to the conception and design of the study and drafted the article. DH contributed significantly to the conception and design of the study and critically revised it for important intellectual content. VA and ML contributed to the design and conception of the study and critically revised it for important intellectual content. All authors have provided final approval of the submitted version.
Ethical approval
The study was reviewed by the ethics committee of the Department of Social Policy and Intervention (University of Oxford) and ethical approval was waived.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Guarantor
VN.
Peer review
Agata Ferretti, Swiss Federal Institute of Technology, have reviewed this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.