
Abstract
Background
Digital therapeutics (DTx) are software-based interventions that aim to prevent or treat especially non-communicable diseases. Currently, no framework for reimbursement of DTx exists in Austria. The aim of this study was to gather a comprehensive perspective on regulatory considerations of Austrian stakeholders with regard to reimbursement of DTx and to outline strategies for establishing a national reimbursement framework.
Methods
Based on a stakeholder analysis, seven semi-structured interviews with Austrian experts from the digital health-related fields medicine, public health, health technology assessment, health industry and social security providers were conducted. Interviews were analyzed according to seven predefined themes.
Results
Overall, participants agreed that reimbursement of DTx by the public insurance in Austria is desirable. Prerequisites are (i) a high user and prescriber acceptance of DTx, which must be integrated into a transparent and interoperable Austrian e-Health infrastructure, (ii) a sufficient, risk-based level of evidence for clinical effectiveness, (iii) national authorities that transparently provide evidence-base, indications, contra-indications and potential risks, (iv) adopting European regulations about data security, secondary use of data and use of artificial intelligence and (v) a health-economical evaluation of DTx.
Conclusion
A comprehensive national strategy for reimbursing DTx will need to consider technical, scientific and socio-economical requirements, patient safety and liability, secure health data handling and use of artificial intelligence in order to establish a sound framework with equitable access also for socioeconomically disadvantaged persons in order to address the growing burden of non-communicable diseases.
Introduction
Healthcare systems worldwide are facing unprecedented challenges, mainly due to aging population and the growing prevalence of non-communicable diseases (NCD). This is particularly driven by the population-wide worsening of behavioural and thus modifiable risk factors, such as obesity, diabetes, arterial hypertension, smoking, unhealthy eating habits and physical inactivity. 1 The growing disease burden and healthcare expenditures challenge health care systems that increasingly lack staff and funding. 2 Thus, innovative, evidence-based and well-regulated solutions as well as implementation strategies into national health care systems that provide equitable access are urgently required to overcome this societal challenge.
Digital therapeutics (DTx) are software-based interventions that aim to prevent and/or treat a disease, 3 hold promise to play a key role in offering solutions and thus, to improve healthcare delivery. DTx may empower patients in making behavioural changes, self-managing their risk profiles and thereby improve clinical outcomes. 4 Furthermore, DTx can utilize additional data, derived from mobile devices, sensors and other tools and deliver well-personalized health services tailored to the patient's needs, increasingly by techniques from artificial intelligence (AI) and machine learning. Recently, the COVID-19 pandemic shifted the digital health landscape by stimulating and accelerating the delivery of consumer- as well as medical grade DTx, emphasizing the need for regulatory frameworks. At the European level, the Medical Device Regulation (MDR) 2017/745, which categorizes medical devices in three different risk classes, regulates clinical investigation and sale of software as a medical device for human use. 5 On the national level, different regulation and reimbursement models in the EU exist. 6 An example from a European country with similar social security system as the Austrian one is the German Digital Healthcare Act, which not only regulates specific requirements for the use of DTx, but also reimbursement by public health insurances. 7 The German initiative started in 2019 by a legal act and was further facilitated by a fast-track assessment by the German Federal Institute for Drugs and Medical Devices. As of September 2023, there are 49 digital health apps (DiGA) listed in the German DiGA-registry, all CE-certified as a medical device with low to medium (MDR class I and IIa) risk and demonstrating different levels of scientific evidence for clinical effectiveness. 8 In contrast, in Austria, as in most other European countries, no national regulation or strategy for assessing and reimbursing DTx currently exists, opening up a regulatory grey area between consumer- and medical-grade digital interventions and precluding physicians from prescribing their patients refundable DTx with proven effectiveness and low patient risk, apart from selected DTx that are part of model projects. Thus, within the compulsory and social Austrian health insurance system, patients currently have to cover the expenses for DTx privately. Considering the higher burden of NCD in socioeconomically disadvantaged persons, the potential of DTx to counteract the growing NCD burden remains underutilized, which adds to an unequitable health care system.
To this end, this study aimed to gather comprehensive perspectives including ideas and opinions from a variety of national stakeholders about reimbursement of DTx for NCD prevention and management in Austria. Based on the results, strategies are summarized, which might inform policy-makers to establish a process that facilitates regulation and implementation of DTx and hence improve healthcare delivery.
Methods
Study design and ethical approval
We conducted a qualitative, interview study with national experts and stakeholders from different digital health-related fields representing medicine, public health, health technology assessment, health industry and social security providers. The study protocol was reviewed and approved by the ethics committee of the Paracelsus Medical University (reference 1095/2020). Participants were informed of the purpose and possible risks of the study prior to signing an informed consent document, which was obtained from all participants, in accordance with the Declaration of Helsinki. 9
Sampling and recruitment
We used a purposive sampling approach, aiming to search for experts with experience across a range of disciplinary backgrounds allowing for complementary and alternative perspectives. Therefore, we first conducted a stakeholder analysis 10 based on the inclusion and exclusion criteria highlighted in Table 1.
Inclusion and exclusion criteria of the participants.

Stakeholders were asked for participation through emails that were sent to publicly available email addresses. We sent a total of 16 emails to potential participants. A follow-up email was sent to non-responders between one to two weeks later. Stakeholders from the following fields could not be recruited despite being elected as relevant by the stakeholder analysis: health law and national authority for health care safety. Finally, seven expert interviews were conducted, with Table 2 outlining their diverse occupational backgrounds.
Occupational background of the interview partner (N = 7).

P indicates interview partner.
Data collection
Data were collected through in-depth, semi-structured, one-to-one, qualitative interviews from June to September 2022. The first author (MS) performed all interviews. The interviews were conducted virtually using Google Meet (n = 5), by phone (n = 1) or in person (n = 1) in German language and recorded using a digital audio recorder. The interview questions focused on key issues with regard to reimbursement strategies derived from scientific literature and experience with the German DiGA-model. All participants were asked if they want to receive the transcripts of the interviews in order to provide further comments. Three participants accepted the offer but did not offer further comments in response to the original interview.
Data analysis
The digitally recorded and anonymized audio files (median (range) duration 35 (27–42) min) were transferred for professional transcription to an online service. Transcripts were analyzed following the steps of thematic analysis as outlined by Braun and Clarke 11 by the first author (MS; professional and scientific background in preventive cardiology and digital health). First, data familiarization was performed by reading and re-reading the transcripts. Second, all data from the transcribed interviews were thematically coded by predefined codes based on key issues with regard to reimbursement strategies in scientific literature and from the German DiGA-model, considering the similar social security system to the Austrian one. Third, if appropriate and following repetitive reading of the transcripts, names and definitions for each theme were adapted. Thus, a primarily deductive approach with inductive refinement was chosen. A concise elaboration of the final themes and description of relevant digital health-related terms based on a narrative literature review was performed for better contextualization of subsequent interview quotes and added to the results section. Compelling examples of the interviews were extracted and extracts analyzed in light of the research question and literature. Finally, thematic comparison and theoretical generalization was performed with regard to strategies for reimbursement decisions of DTx in Austria. MaxQDA (Version 2022.0.0; VERBI – Software, Berlin, Germany) was used for software-supported data organization and analyses.
Original quotes used for publication were translated from German into English by the first author of the study (MS) and results were reported according to the consolidated criteria for reporting qualitative research (COREQ checklist 12 ; Supplemental Table 1).
Results
Overall, most participants agreed in principle that reimbursement of DTx by the public insurance is desirable, if the considerations summarized in the themes shown in Figure 1 are addressed. In each theme, participants’ responses encompassed several relevant considerations for decision-makers. Supporting quotes related to issues of corresponding themes are highlighted in textboxes (textboxes 1–6) together with an elaboration of the themes.

Illustration of the final themes resulting from the qualitative analysis.
Theme 1: Technical requirements
Technical user and prescriber acceptance is a critical enabler to adherence and linked to technical features, such as stability, usability and user experience and thus, an important consideration for reimbursement decisions. 13 Interoperability, defined as how healthcare information can be exchanged between different IT-systems regardless of how it is stored in those systems, 14 is relevant for the health care provider and policy makers, since it plays a pivotal role for enabling an integrated healthcare system. In Austria, healthcare information can be stored within the Austrian electronic health record (ELGA) and ELGA holds promise to be the platform for an inter-operable digital health infrastructure and subsequently facilitating an integrated health delivery system. Textbox 1 provides a selective summary of quotes regarding technical requirements for reimbursement of DTx in Austria.
Issues related to technical requirements.
‘Health care providers want a single platform, where he/she can provide the digital service’. [P2] ‘With Austria ID a unique identification/login number, with which data could be connected exists in Austria’. [P3] ‘Technical standards should be compatible with the Austrian electronic health record’. [P4] ‘Interoperability holds great potential but not a prerequisite for reimbursement’. [P5] ‘Usually, information about technical stability and usability of digital health applications are drawn from studies. Thus, post-market surveillance is necessary for digital health applications, as requested in other medical devices’. [P5] ‘Need for transparent guideline about relevance for inter-operability with the electronic health record or hospital information system and one must adhere to relevant standards’. [P6] ‘If we manage to develop ELGA as a central hub, I would suggest interoperability of DTx as a prerequisite’. [P6] ‘Need to develop the Austrian e-Health infrastructure in a way that a health app supports an integrated healthcare process providing relevant health information for a patient summary’. [P6]
P indicates interview partner.
Theme 2: Scientific evidence for effectiveness
DTx must apply the rules of evidence-based medicine in the same way as non-digital therapies. Defining what level of evidence to require before not only offering a digital intervention but also reimbursing them by the public sector is essential, not only to inform the health care provider and the patient, but also guide the industry during early stages of DTx development. Considering the realm of DTx from simple data storing tools for disease self-management to higher risk applications, the level of evidence needs to be adjusted to the associated risk. Textbox 2 provides a selective summary of quotes regarding scientific evidence for effectiveness needed for reimbursement of DTx in Austria.
Issues related to scientific evidence for effectiveness.
‘According to the Austrian social security act, services are reimbursed by a social insurance carrier as long as they conform to scientific standards. And observational studies are not the scientific standard (for proving effectiveness of an intervention; addition from the first author for clarification). That's why there is the need for a RCT’. [P7] ‘Some DTx might have a large organizational benefit… but when I require a randomized, controlled study for reimbursement, the company has to calculate the associated costs and might decide to offer the service in another country’. [P5] ‘In Germany, the system is innovation-friendly, as DTx are risk classified as 2a and no randomized, controlled studies are necessary and observational studies are considered sufficient. However, almost all apps in Germany conduct RCTs because they are aiming to prove medical benefit and expect better leverage for price negotiations’. [P6] ‘It is important to assess what the DTx is aiming for, such as substituting or adding to a service, and subsequently choose the control and the primary outcome. In DTx with higher risk, adverse events and safety aspects should be evaluated as secondary outcomes’. [P4] ‘Supporting the DTx engineer company that aims for reimbursement with regard to study design before starting a trial should be considered’. [P4] ‘According to the German DiGA act you could compare it with no treatment at all, rather than usual care, taking into account potential organizational benefits’. [P6] ‘It is important to consider the whole process: First, does the DTx address a relevant health delivery issue? If yes, start with the existing evidence and subsequent financial aids may carry the evidence further, if necessary with a RCT. The financial aids might derive from co-financing, innovations funds or by the reimbursed prices when introduced to the market’. [P6]
P indicates interview partner.
Theme 3: Patient safety and medical liability
The increasing availability and usage of mobile health technology that is often employed for medical decision-making whilst not necessarily being certified for the medical purpose 15 opens up areas of uncertainty, as safety and liability issues. Health technology assessment beyond CE-certification within a reimbursement evaluation framework has the potential to address safety and medical liability concerns. Textbox 3 provides a selective summary of quotes regarding safety and liability in the context of reimbursement of DTx in Austria.
Issues related to scientific evidence for effectiveness.
‘Some stakeholder are reluctant to establish an official Austrian App-registry due to liability issues and leave it up to the market. However, market entrance is more difficult due to the new MDR 2017/745-act what might help’. [P6] ‘At the end, no matter if monitoring devices or decision-support systems, the physician needs to look at the output and take responsibility for medical recommendations’. [P3] ‘It is like prescribing drugs, as soon as you prescribe a DTx the prescribing physician is in charge for the correct indication and interpretation and the company for technical issues in case of adverse events/complications’. [P5] ‘Each patient needs to be informed about potential associated risks and consent using the app before starting’. [P7] ‘As a physician, I prefer using my own medical devices, in contrast to looking at some reports from devices I do not know, also not knowing if the patient was really using these device. That needs to be solved legally and will face resistance. That's why I think lifestyle-related apps, including sensors like activity trackers, will be a nice to have and probably offered in the private health sector where also persons with higher health literacy show up, without being reimbursed by the social insurance’. [P2] ‘In comparison with using an ECG which is written by the physician himself, by prescribing a DTx the physician hardly earns money but takes full responsibility’. [P2]
P indicates interview partner.
Theme 4: Data security and secondary use of data
DTx produce and process a high amount of personal health data, which are considered to deserve special protection against misuse. Thus, health data security poses a big concern. On the other hand, secondary use of data, defined as processing anonymized and thus privacy-preserving health data for purposes other than the initial medical purpose for which the data were collected, holds promise to be used to inform public health and research and thus, improve quality of care. 16 Textbox 4 provides a selective summary of quotes regarding data security and secondary use of data in the context of reimbursement of DTx in Austria.
Issues related to data security and secondary use of data.
‘Requires same regulations as existing health solutions such as cardiac pacemakers’. [P1] ‘What the company is doing with the data should be highly regulated’. [P1] ‘Need to shift away from the belief, that the owner of the server where the data is located owns the data’. [P3] ‘What I refuse is if companies use the data to improve their product and then sell it for more money’. [P3] ‘Data belongs to society, in case DTx are reimbursed from tax money’. [P3] ‘Should be clear, what kind of data are collected and the user should always be able to consent or reject’. [P4] ‘Important to comply with current European regulations (GDPR)’. [P4] ‘There exist effective technical data security preserving solutions like pseudonymization and anonymization’. [P3] ‘If the consent policy is designed well and the user is able to follow what he/she is consenting to, I think it is worth to go towards opt-in data transmission’. [P6] ‘European Health Data Space will change quite a bit, since the patients will have their health data better structured with the opportunity to forward the data if they see value in it’. [P6] ‘Pseudonymized, anonymized or consent-based which will be the new-normal within the European Health Data Space and as long as there is a legitimate scientific purpose’. [P6]
P indicates interview partner; GDPR = General Data Protection Regulation.
Theme 5: Use of artificial intelligence
AI tools are a fast-growing part of healthcare, are frequently part of DTx and are expected to impact the entire healthcare system in the coming decades on the journey towards more personalized and preventive medical care. 17 Furthermore, the surge in health data derived from DTx and wearable devices are an opportunity to provide ‘trainable’ data to further develop and improve AI applications. However, AI comes with several drawbacks, such as the risk of black box algorithms, bias within the algorithms based on poor model training and liability issues. 18 Textbox 5 provides a selective summary of quotes regarding AI in the context of reimbursement of digital health applications in Austria.
Issues related to artificial intelligence.
‘In the Germany DiGA system the algorithms are rarely described. This is not surprising, since this is the intellectual business property/trade secret’. [P4] ‘That is in the realm of business secret and problematic to disclose’. [P5] ‘If you do not know the AI algorithm you cannot assess the associated risk’. [P4] ‘It also depends how the AI algorithm was trained. The results from an AI algorithm might be reproducible in a certain study population but not necessarily be transferred to another population’. [P4] ‘In the EU AI-act certain AI-systems need to be registered and will be assessed, also ethically if there are bias- or discrimination effects’. [P6]
P indicates interview partner.
Theme 6: Ethical and health economical considerations
Considering that Austria has a compulsory and social health insurance system, equitable access to effective medical therapeutics, regardless of pharmaceutical or digital, should be warranted. However, considering that healthcare spendings continue to rise, it is increasingly important that new health technologies demonstrate that the incremental costs associated with a new technology weighs the potential clinical benefits, such as improvement in quality of life or increased life expectancies. Textbox 6 provides a selective summary of quotes regarding ethical and health economic considerations in the context of reimbursement of DTx in Austria.
Issues related to ethical considerations.
‘As soon as an additional medical benefit is proven, it is unethical not to provide it to people who are publicly health insured’. [P1] ‘As long as a low-threshold access exists to effective digital tools, additional features might be offered by extra payment’. [P5] ‘On the long run, digital therapies might be the new normal and we have to take care that not only rich people may afford the non-digital services’. [P6] ‘Reimbursement is currently requested by the industry, rather than physicians/patients’. [E4] ‘Austrian economical patient care act says that in case two therapies are equal the cheaper one has to be chosen. Does two therapies have the same expenses, the more effective one has to be chosen’. [P2] ‘A step-wise approach would be to prove effectiveness and safety first, and in case its proven, to assess cost effectiveness’. [P4] ‘An important question for assessing cost-effectiveness is, whether the DiGA is complementary or compensating non-digital therapies. In case of compensating, there will be conflicts with healthcare providers who offer the analog therapy’. [P6]
P indicates interview partner.
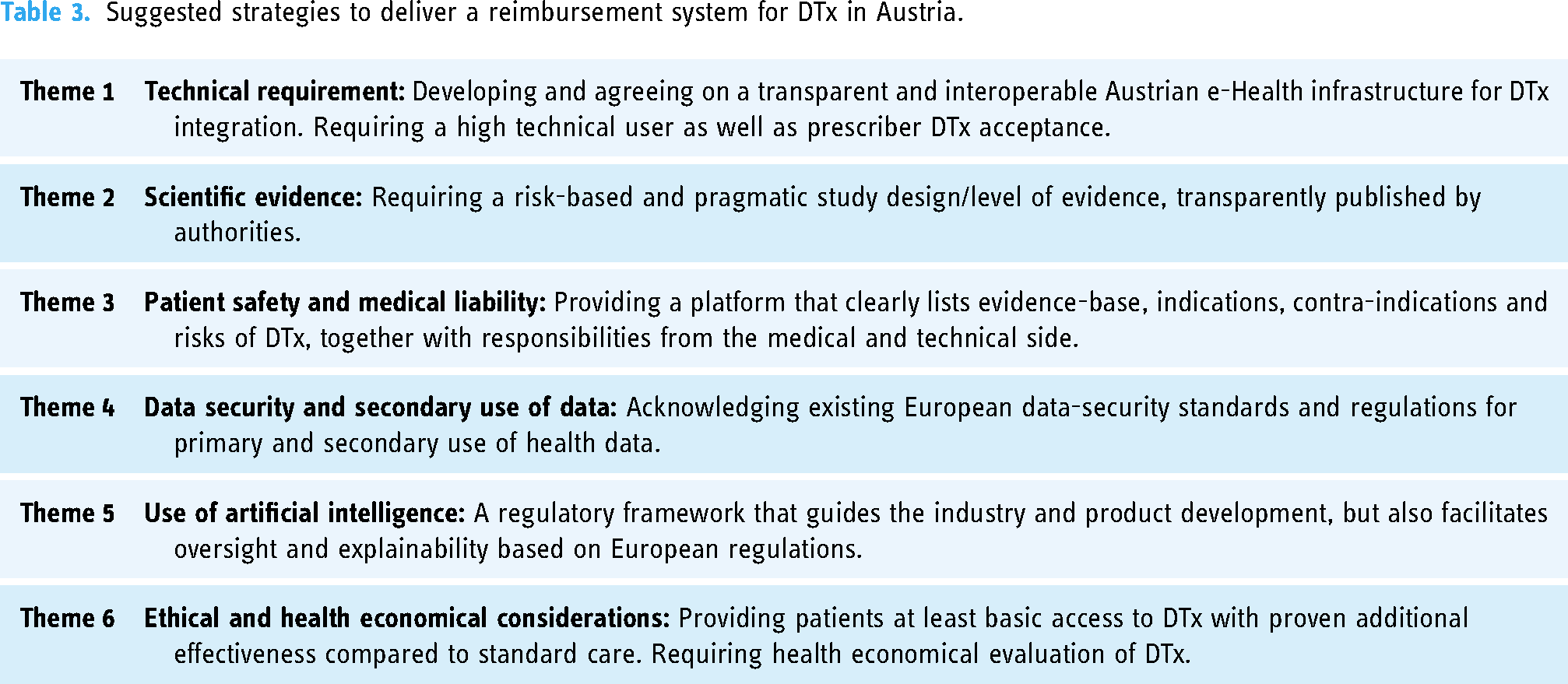
Based on the supporting quotes, potential strategies to implement a reimbursement system for DTx in Austria were elaborated and are indicated in Table 3.
Suggested strategies to deliver a reimbursement system for DTx in Austria.
Discussion
The overall aim of this qualitative and formative expert interview study was to assess ideas and opinions of key stakeholders about relevant barriers and chances with regard to reimbursement of DTx for NCD prevention and management by the public sector in Austria and outline strategies to establish a national reimbursement system therefrom.
Most participants agreed in principle that reimbursement of DTx by the public insurance is desirable. However, a technical barrier also addressed by most participants, is the underdeveloped Austrian e-Health infrastructure, which does not currently enable DTx to be effectively linked with other systems including the Austrian electronic health record (ELGA). One participant stated ‘If we manage to develop ELGA as a central hub, I would suggest interoperability of DTx as a requirement’ [P6]. Indeed, a connected health model using patient-generated health data, defined as health data collected from a patient outside the clinical setting to help address a health concern, 19 has shown to improve clinical outcomes in cardiovascular diseases through empowering patients and providing clinical decision support. 4 Especially Scandinavian countries have made significant progress in developing advanced e-health infrastructures for connected health. 20 However, considering the different stakeholders and interests involved in building up such an Austrian e-Health infrastructure, ELGA as the hub for such an e-Health infrastructure is currently in question and subsequently predicting a timeline remains difficult. Thus, in case of starting reimbursement before establishing an efficiently communicating e-Health infrastructure, at least current technical standards should made a requirement and transparently reported for reimbursement of DTx. In the German DiGA-model, all DTx are standalone systems and no inter-operability is required from authorities. Thus, already permanently listed German DTx without fulfilling current technical standards will hamper establishing a sound e-health infrastructure in the future, including data from personal health records. Notably, in the German DiGA-model currently no reimbursement strategy for combined DTx (e.g. combined with other health services or devices) exists.
A high technical user as well as prescriber DTx acceptance is essential for successful uptake, which requires technical stability and usability. One participant stated ‘Health care providers want a single platform, where he/she can provide the digital service’ [P2]. Indeed, a criticism about the German DiGA-model is, that physicians were not adequately represented in the policy-making process, leading to a rather low prescription rate of DTx in Germany. 7 Thus, an overall strategy addressing technical requirement for reimbursement is developing and agreeing on a transparent and interoperable Austrian e-Health infrastructure for DTx integration and preconditioning high technical user as well as prescriber DTx acceptance.
Randomized-controlled trials (RCTs) are considered to provide the most reliable evidence on the effectiveness of interventions. However, considering that many innovative DTx derive from small to medium-sized enterprises, conducting a time-consuming and costly RCT especially for low-risk DTx may interfere with entrepreneurial drive. One participant highlighted that in the German DiGA-model ‘no randomized, controlled studies are necessary and observational studies are considered sufficient. However, almost all apps in Germany conduct RCTs because they are aiming to prove medical benefit and expect better leverage for price negotiations’ [P6]. Another expert suggested to ‘start with the existing evidence and subsequent public financial aids may carry the evidence further, if necessary with a RCT, in case a relevant health delivery issue is addressed’ [P6]. Overall, it is key to outline transparent and clear rules, what level of evidence and study design is required, including what the DTx should be compared with and required endpoints, in order to guide the industry in their ambition and reduce entrepreneurial risk. Furthermore, novel and innovative study designs hold potential to facilitate generating scientific evidence compared to highest but also time-consuming and costly standards, such as RCTs. 21 Thus, an overall strategy addressing scientific evidence for effectiveness requires a risk-based and pragmatic study design/level of evidence, which is transparently disclosed by authorities. In this regard, currently employed established research methods fall short of assessing the impact of personalization of an intervention and novel research designs and platforms that enable integration of continuous patient-generated health data hold promise to pave the road for providing evidence for the personalized effect of a DTx intervention. 22
Concerns about patient safety and medical liability are barriers for physicians to prescribe DTx, mainly because the majority of physicians are not sufficiently trained in assessing technical specifications, such as validity and usability of DTx. As highlighted by one participant ‘market entrance is more difficult due to the new MDR 2017/745-act’ [P6] and in the German DiGA model, only medical devices approved by MDR 2017/745 as low to medium risk (class I and IIa) are eligible to be listed for reimbursement. One participant stated ‘As a physician, I prefer using my own medical devices, in contrast to looking at some reports from devices I do not know also not knowing if the patient was really using these device’ [P2] and another participant stated ‘at the end, no matter if monitoring devices or decision-support systems, the physician needs to look at the output and take responsibility for medical recommendations’ [P3]. Indeed, in parallel to traditional interventions, the prescribing physician needs to know about evidence-base, indications, contra-indications and risks before prescribing a DTx to inform the patient.
Of note, there is still a lack of harmonization in regulatory requirements between European countries due to differences in interpretation of the MDR 2017/745 23 and experiences with DTx malpractice lawsuits are scarce. 24 Thus, an overall strategy addressing safety and medical liability concerns, providing a platform that clearly specifies evidence-base, indications, contra-indications and risks as well as advanced training in prescribing DTx to support physicians in informing the patient about potential risks and safely prescribing DTx is required to reduce concerns about patient safety and medical liability.
A substantial barrier to DTx reimbursement within health systems is the concern related to data privacy and security, considering the requirement of storing data in centralized databases. However, participants acknowledge that well-established data-security standards and regulations exist ‘There exist effective technical data security preserving solutions like pseudonymization and anonymization’ [P3] as well as international regulations such as the General Data Protection Regulation (GDPR). 25 With regard to secondary use of health data, one participant noted: ‘Need to shift away from the believe, that the owner of the server where the data is located owns the data’ [P3] and further ‘Data belongs to the society, in case DTx are reimbursed from tax money’ [P3]. Furthermore, one participant addressed the requirement of a well-designed consent policy and the evolving European Health Data Space [P6], which supports individuals to take control of their own health data and strives to make use of safe and secure health data exchange to unleash its full potential. 26 Thus, an overall strategy addressing data security and secondary use of data is acknowledging and making use of existing data-security standards and regulations.
AI will play an increasing role in medicine but knowledge about AI within the healthcare system differs largely. Its broad application within a reimbursement system faces challenges as indicated by some quotes of the participants concerning liability, ethical and regulatory considerations. Before prescribing health-related AI, physicians have to educate their patients about potential risks and short-comings and obtain informed consent. Therefore, knowledge about the AI is required, as stated by one participant ‘If you do not know the AI algorithm you cannot assess the associated risk’ [P4]. However, most participants agree that full disclosure of underlying algorithms is problematic ‘That is in the realm of business secret and problematic to disclose’ [P5]. Thus, a regulatory framework is required not only for guiding the industry and product development, but also for facilitating oversight and explainability of these complex applications. In April 2021, the European Commission presented a regulatory proposal for AI in the European Union (EU) and provides transparency requirements for the provision of information to users, but to date does not include requirements on the explainability of the model in the sense of having insight into how it comes to a prediction, for example, which features, parameters and weights were involved. 27 Thus, an overall strategy addressing use of AI is establishing a framework that not only guides the industry and product development with regard to protecting their intellectual properties, but also facilitates oversight and explainability.
Considering the evolving evidence for clinical effectiveness of certain DTx, lack in reimbursement by public health insurance risks to exacerbate existing health inequities, as one participant stated ‘as soon as an additional medical benefit is proven, it is unethical not to provide it to publically health insured’ [P1]. However, almost all participants agreed that cost-effectiveness is necessary, also indicating a potential compromise ‘As long as a low-threshold access exists to effective digital tools, additional features might be offered by extra payment’ [P5]. Notably, the cost-effectiveness of several DTx has been established 28 and implementing DTx in patient care facilitates value- and performance-based payment models, that aim to improve quality care and efficiency at reduced operating costs. 29 Thus, an overall strategy addressing ethical and health economic considerations would be providing patients at least basic access to DTx with proven additional effectiveness to standard care.
Finally, within different themes the European Health Data Space was mentioned, for example, ‘The European Health Data Space will change quite a bit, since the patients will have their health data better structured with the opportunity to forward the data if they see value in it’ [P6]. National strategies need to be aligned to EU standards and requirements such as the European Health Data Space to enable collaboration between EU member states, to harmonize clinical evidence requirements including real-world evidence, data sharing to realise the full potential of data generated by DTx and strategies on pricing and reimbursement. 30
A potential limitation of this study is the lack of formal assessment of data saturation. Given our purposive sampling approach as we aimed to include experts from diverse disciplinary backgrounds, the goal was to capture a broad range of perspectives rather than seek thematic saturation. As such, data saturation was not applicable in this context, as each interview was intended to provide unique insights from different fields, reflecting the diversity of expertise relevant to the topic of DTx reimbursement. Another limitation of this study is the potential lack of direct transferability of the results to health policies outside of Austria. While the findings are grounded in Austria's social security system and informed by the German DiGA model, differences in healthcare structures, regulatory frameworks and digital health adoption across countries may limit the broader applicability of the insights. Future studies should consider cross-national comparisons to enhance the generalizability of findings to other healthcare systems. Additionally, the absence of patient and citizen representatives is a limitation of this study, and future research should consider their inclusion to capture valuable insights into decision-making processes surrounding digital health policy.
Conclusion
The political will and a well-defined strategy involving all relevant stakeholders and acknowledging the lessons-learned from frontrunners in digital health will be required to establish a framework for reimbursing DTx, which holds promise to help addressing the current pandemic of NCD. Based on the expert interviews conducted in this study, a transparent and interoperable national e-Health infrastructure, a risk-based and pragmatic study design/level of evidence requirement, clearly listing evidence-base, indications, contra-indications to address patient safety and medical liability issues and uptake of international regulations with regard to data security, secondary use of data and use of AI are strategies to provide equitable access to evidence-based DTx and thus, improve health care delivery. Finally, creative, cross-sectional funding models need to be developed to promote enthusiasm at health care provider level, health care organizational level and industry partner level.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241299062 - Supplemental material for Opportunities and barriers for reimbursement of digital therapeutics in Austria: Findings From expert interviews
Supplemental material, sj-docx-1-dhj-10.1177_20552076241299062 for Opportunities and barriers for reimbursement of digital therapeutics in Austria: Findings From expert interviews by Mahdi Sareban, Gunnar Treff, Jan David Smeddinck, Rada Hussein and Josef Niebauer in DIGITAL HEALTH
Footnotes
Acknowledgements
The methodological expertise and support provided by Dr Stefan Tino Kulnik (Ludwig Boltzmann Institute for Digital Health and Prevention, Salzburg, Austria) and Priv.-Doz. Dr Claudia Wild (Austrian Institute for Health Technology Assessment, Vienna, Austria) are gratefully acknowledged.
Contributorship
MS contributed to the conception and design of the study, acquisition of data, analysis and interpretation of data, and drafting the article. GT, JDS, RH and JN contributed to the interpretation of data, revised the article for important intellectual content and made final approval of the version to be submitted.
Data Availability
We used a qualitative research design, and therefore the data generated are not suitable for sharing beyond that contained within the report. Further information can be obtained from the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the ethics committee of the Paracelsus Medical University (reference 1095/2020).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MS
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.