
Abstract
Introduction
A novel telerehabilitation service provides wayfinding and self-management advice to persons with neurological, musculoskeletal, or coronavirus disease 2019 related rehabilitation needs.
Method
We utilized multiple methods to evaluate the impact of the service. Surveys clarified health outcomes (quality of life, self-efficacy, social support) and patient experience (telehealth usability; general experience) 3-months post-call. We analysed associations between, and within, demographics and survey responses. Secondary analyses described health care utilization during the first 6 months.
Results
Sixty-eight callers completed the survey (42% response rate). Self-efficacy was significantly related to quality of life, interpersonal support and becoming productive quickly using the service. Becoming productive quickly was significantly related to quality of life. Education level was related to ethnicity. Survey respondents’ satisfaction and whether they followed the therapist's recommendations were not significantly associated with demographics. Administrative data indicated there were 124 callers who visited the emergency department before, on, or after their call. The average (SD) frequency of emergency department visits before was 1.298 times (1.799) compared to 0.863 times (1.428) after.
Discussion
This study offers insights into the potential impact of the telerehabilitation service amidst pandemic restrictions. Usability measurements showed that callers were satisfied, corroborating literature from pre-pandemic contexts. The satisfaction and acceptability of the service does not supplant preferences for in-person visits. The survey sample reported lower quality of life compared with the provincial population, conflicting with pre-pandemic research. Findings may be due to added stressors associated with the pandemic. Future research should include population-level comparators to better clarify impact.
Introduction
In 2020, the global rate of disability was 15% with 22% of Canadians experiencing some functional impact on daily activities.1,2 Globally mandated social distancing during the coronavirus disease 2019 (COVID-19) pandemic suspended clinics, homecare and other support services, which are critical for individuals with health and medical needs. Vulnerable populations, such as individuals living with chronic health conditions, are at risk for negative health outcomes during the pandemic,1,2 such as health deterioration, possible hospitalization and unnecessary emergency department (ED) visits. The COVID-19 pandemic has also inevitably affected rehabilitation services. In order to maintain social distancing and avoid possible contacts, numerous rehabilitation interventions have been postponed. 3
Rehabilitation is ‘a set of interventions designed to optimize functioning and reduce disability’. 4 COVID-19 survivors will increase demands for rehabilitation due to prevalent and diverse post-acute COVID-19 sequelae.5–13 The Public Health Agency of Canada's living systematic review (n = 36) suggests that individuals with laboratory-confirmed COVID-19 (both hospitalized and non-hospitalized patients) experience fatigue, general pain or discomfort, shortness of breath, sleep disturbances, anxiety and persistent cough for 4–12 weeks after diagnosis. 13 Minus persistent cough, these symptoms tend to continue longer-term (>12 weeks post-diagnosis) alongside other symptoms: depression, post-traumatic stress disorder and hair loss. 13 These symptoms, along with the continued presence of patients with acute and chronic conditions requiring rehabilitation unrelated to COVID-19, will result in a confluence of increasing rehabilitation needs during, and after, the pandemic.
The pandemic catalysed the rapid adoption of telehealth practices to advance continuity of care. 14 Telehealth initiatives include telephone advice lines; virtual meetings using online platforms; and patient portals, for example. A randomized, single-blinded trial of veterans with stroke (n = 52) found significant improvements in disability (p < 0.05) and near significant improvements in function (p < 0.06) in the telerehabilitation group compared to the normal therapy group. 15 A randomized, controlled trial (n = 52) of a 12-week home-based telerehabilitation programme for stroke survivors demonstrated statistically significant improvements in function in the telerehabilitation group compared to the control group. 16
Telerehabilitation has been shown to be at least equivalent to in-person care for musculoskeletal conditions, inflammatory arthritis, and orthopedic surgery.17–20 A systematic review (n = 13 studies) found that telerehabilitation for musculoskeletal conditions was effective in improving physical function while being slightly more favourable, compared to traditional therapy. 21 Another systematic review (n = 12 studies) noted similar improvements in motor function with telerehabilitation for total knee arthroplasty. 22
These studies outline the impact of telerehabilitation. However, little research has been published analysing the impact of telerehabilitation: (a) within a pandemic climate; (b) on health service utilization; or (c) looking at telehealth usability alongside of patient-reported quality of life outcomes.
Organizational context
In response to the pandemic, provincial rehabilitation stakeholders from a single, provincial health-system in Canada co-designed a novel telerehabilitation service. This telerehabilitation service (the Rehabilitation Advice Line) provides wayfinding (information on rehabilitation services that are open for in-person and/or virtual visits) and self-management advice to adults with musculoskeletal, neurological, or post-COVID-19 needs. The service is staffed with occupational therapists and physiotherapists who provide: (a) information on activities and exercises to address physical concerns; (b) strategies to self-manage daily activities; and (c) referrals to rehabilitation and community services, as needed.
This study aimed to evaluate the mid-term impacts of the service amidst the global pandemic. We wanted to understand callers’ perceived experience of the service 3-months post-call as well as patient health outcomes and health service utilization in the 4 months after using the service.
Methods
We used multiple methods, which are described in detail in a published study protocol. 23 Methods included surveys and secondary data analyses on health service utilization. The University of Alberta Research Ethics Board approved this study (Pro00102178). A waiver of consent was obtained for secondary data analyses. All survey participants provided informed written consent.
Study population
The study population included adult callers who accessed the telerehabilitation service within the first 6 months of operation. Only callers who consented to future contact at the end of their first call were eligible for the follow-up surveys. Inclusion criteria included being able to read and speak English.
Surveys
All callers who consented to future contact were invited to complete follow-up patient-reported measures 3-months post-call. These surveys measured telehealth experience and usability (10-Item Telehealth Usability Questionnaire (TUQ-10) 24 and general Patient Experience Survey) 25 ; quality of life (European Quality of Life Five Dimension Five Level (EQ-5D-5L)) 26 ; social support (12-Item Interpersonal Support Evaluation List (ISEL-12)) 27 ; perceived self-efficacy with conditions (6-Item Self-Efficacy for Managing Chronic Disease Scale (SEMCD-6))28,29; and general demographic information (Table 1). The experience and usability surveys targeted the first research aim, while the remaining targeted the second research aim. Survey responses were captured through Research Electronic Data Capture. 30 All surveys were compared descriptively to existing population-level data (either provincial, national or international). The surveys are considered valid and reliable in comparable populations (Table 1).24–29
Items measuring experience included in follow-up survey package.

TUQ-10: 10-Item Telehealth Usability Questionnaire; EQ-5D-5L: European Quality of Life Five Dimension Five Level; ISEL-12: 12 Item Interpersonal Support Evaluation List; SEMCD-6: 6-Item Self- Efficacy for Managing Chronic Disease; ISEL-12: 12 -Item Interpersonal Support Evaluation List.
We calculated descriptive statistics, measures of central tendency, or frequency, where relevant. The ED-5D-5L user guide was followed for analysis. 26 We conducted analyses to test for associations between survey responses and patient demographics using SPSS 26.
Health service utilization
Secondary data analyses were used to explore mid-term health service use pre- and post-calls. All callers from the first 6 months were included in analyses. Personal health numbers were retrieved from the service's clinical charts to identify the timing and frequency of ED visits.
We calculated the average frequency of ED visits and the number of unique patients who visited the ED, pre- and post-call. We calculated the average number of days before and after someone visited the ED relative to their call date, as well as the mean difference in days (mean days after minus mean days before). Inferential analyses were not performed due to data limitations.
Results
Surveys
In total, 162 callers were eligible for follow-up survey recruitment; 68 responded (42% response rate). Six (8.82%) returned surveys that contained no responses and eight (11.76%) were partially incomplete. The completeness of survey responses aligned with their order of presentation. The EQ-5D-5L (quality of life) had the most complete responses (n = 62; 91.2%) followed by the SEMCD-6 (self-efficacy; n = 60; 88.2%), the ISEL-12 (social support; n = 58; 85.3%), the Patient Experience Survey (n = 57; 83.8%), the TUQ-10 (telehealth usability; n = 54; 79.4%), and the demographic questionnaire (n = 54; 79.4%).
Survey respondents had a mean [standard deviation (SD)] age of 54.8 [16.4] years, comparable to the population average of 55.3 [18.1] years for all callers from the first 6 months of operation. Most respondents were female (45.6%), married (legal/common-law) (51.5%), from a metropolitan centre (44.1%), of European origin (61.8%), and had at least some post-secondary or apprenticeship training (61.8%). See Appendix A for the range of scores on each survey compared to provincial, national, or international comparators.
Based on the Patient Experience Survey data, if the service did not exist, most respondents would have called a public health centre (14.7%), used the internet (13.3%), or were unsure of what they would have done (14.7%). Most respondents called the service for a new or acute issue (39.7%) or a chronic issue (23.5%). Clinicians provided education and self-management advice to treat at home for 41.1% of respondents; 38.2% of the total respondents (92.9% of those given advice) followed the therapist's advice.
In the TUQ-10 survey, respondents noted that the telerehabilitation service was highly usable (Figure 1). The majority of respondents were satisfied overall (94.4%) and found the line simple to use (94.4%) while providing them with a tool to express themselves (98.1%). The greatest variability in responses was for the question about whether the encounter was the same as in-person visits (53.7% disagreed, 44.4% agreed).
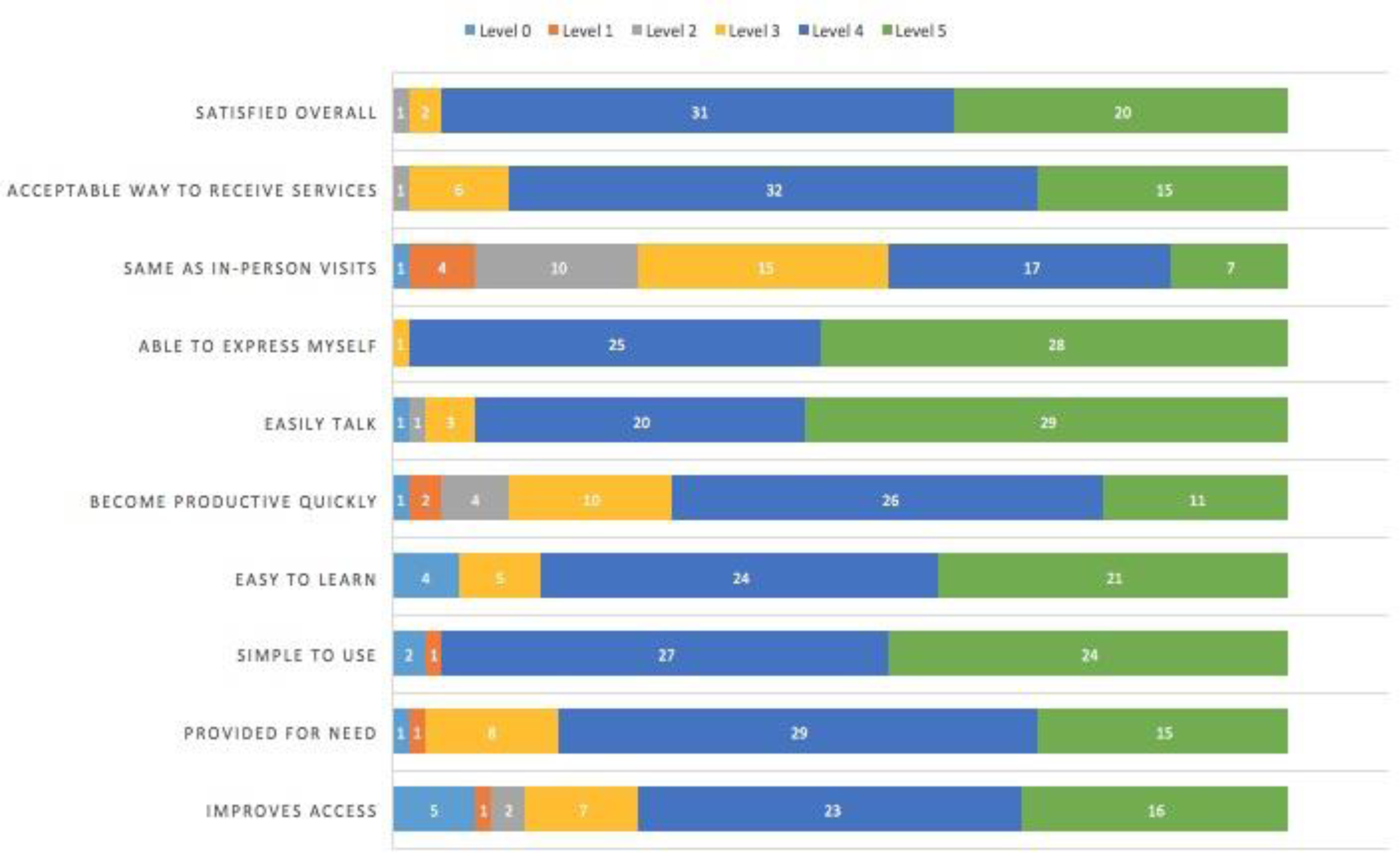
Ten-Item Telehealth Usability Questionnaire (TUQ-10) responses by domain.
The mean [SD] EQ-5D-5L Visual Analogue Scale (VAS) score (quality of life) for the survey sample and the general Alberta population was 65.5% [21.9%] and 77.4% [17.1%], respectively. The mean [SD] EQ-5D-5L Index score for the survey sample and the general Alberta population was 0.69 [0.23] and 0.84 [0.14], respectively.
Problems in the mobility dimension of the EQ-5D-5L were absent for 35.4% and 72.8% of the survey respondents and the general provincial population, respectively (Figure 2). Similar variability between responses from the survey population and the general provincial population indicating ‘no problems' was found for the self-care dimension (60.4% and 94.1%, respectively), the usual activity dimension (26.5% and 74.0%, respectively), and the anxiety/depression dimension (33.9% and 62.8%, respectively). The closest ‘no problems' value to the general provincial population was on the pain/discomfort dimension. Problems were absent for 14.7% of the survey respondents versus 36.0% of the general provincial population.

European Quality of Life Five Dimension Five Level (EQ-5D-5L) scores by dimension and population.
The mean [SD] SEMCD-6 score (self-efficacy) for the survey sample was 6.56 [2.47]. The mean [SD] SEMCD-6 score for the Canadian comparator is 6.4 [2.3]. Figure 3 compares the mean survey scores on each domain of the SEMCD-6 to the Canadian comparator. The greatest difference between respondents and the national comparator data is in the confidence to manage without medication domain (mean [SD] = 7.3 [2.5] and 6.9 [2.6], respectively). More respondents were confident that they could manage their concerns without medication in comparison to the national population. This domain had the highest score. The lowest scored domain related to caller confidence in keeping the pain and discomfort from interfering with activities (mean [SD] = 6.1 [2.9]).
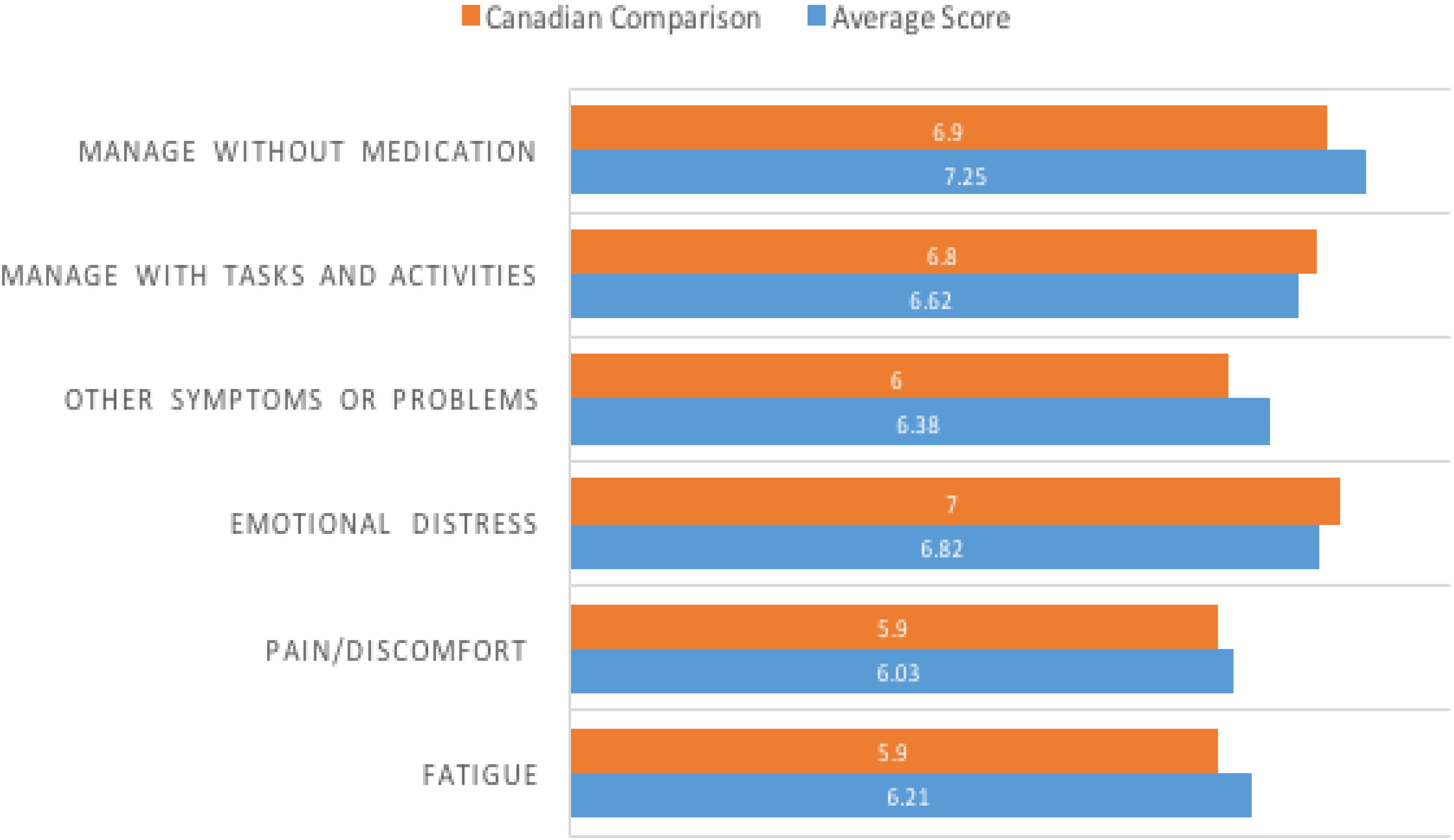
Six-Item Self-Efficacy for Managing Chronic Disease Scale (SEMCD-6) average scores and Canadian comparisons.
The mean total [SD] ISEL-12 score (social support) for the survey sample was 32.72 [6.28]. Regarding perceptions of social support via the ISEL-12 tool, the highest domain score was for the item about having someone to call if stranded (mean [SD] = 3.28 [0.96]). The lowest domain score on the ISEL-12 for callers was for the item related to finding someone to help them move (mean [SD] = 2.04 [1.03]).
Relationships. Spearman's rank-order correlations were used to determine whether there were any statistically significant relationships between patient demographics and total survey scores. Since the TUQ-10 (telehealth usability) does not have a total score, Spearman's rank-order correlations examined the associations between each TUQ-10-item and patient demographics or any of the other total survey scores.
Becoming productive quickly using telerehabilitation was significantly related to quality of life (EQ-5D-5L Index Score (r = 0.428, p < 0.01) and VAS score (r = 0.399, p < 0.01)) and self-efficacy to manage chronic disease (r = 0.281, p < 0.05). Self-efficacy for managing chronic disease was significantly related to the quality of life (EQ-5D-5L Index Score (r = 0.748, p < 0.01) and VAS score (r = 0.792, p < 0.01)), and interpersonal support (ISEL-12 (r = 0.323, p < 0.05). Education level was significantly related to ethnicity (r = 0.337, p < 0.05). Survey respondents’ overall satisfaction with the telerehabilitation service and whether or not they followed the therapist's recommendations were not associated with age (p = 0.71 and 0.28, respectively), gender (p = 0.59 and 0.54, respectively), marital status (p = 0.15 and 0.66, respectively), geographical location (p = 0.22 and 0.61, respectively), employment status (p = 0.32 and 0.27, respectively), education level (p = 0.33 and 0.99, respectively), or ethnicity (p = 0.37 and 0.36, respectively).
Health service utilization
There were 124 callers (23.1%) who visited the ED before, on, or after their call (94 before call and 54 after). The average (SD) number of ED visits before was 1.298 times (1.799), with the highest number of visits being 17. The maximum and minimum number of days between the call and the ED visit was 104 days before and 1 days before, respectively.
The average (SD) number of ED visits after was 0.863 times (1.428), with the highest number of visits being 8. The maximum and minimum number of days visited on or after the call were 114 days after and 1 days after, respectively. The average (SD) mean difference in days between visiting the ED post-call and visiting the ED pre-call was 38.952 days (29.416).
Discussion
This study offers insights into the potential mid-term impacts of a novel telerehabilitation service amidst pandemic restrictions. Measurement of the usability of the service showed that callers were satisfied and found it acceptable. This corroborates literature from pre-pandemic contexts. A study assessing a telephone-based physiotherapy service found that participants viewed it as acceptable since it was defined by their preferences and priorities. 31 A systematic review (n = 44 studies) exploring the association between telehealth and patient satisfaction found that patients were satisfied when using telehealth modalities as they improved outcomes, were simple to use, were affordable, improved communication, and decreased travel time, thus increasing efficiency. 32 Simplicity of use and therefore efficiency of the service was echoed in the current study. However, this satisfaction and acceptability of telerehabilitation did not supplant preferences for in-person visits. In the current study, the survey question about the service being comparable to in-person visits had the most variability in responses. In another study, some participants found a physiotherapy phone line impersonal and that it prevented rapport-development compared to in-person visits. 31 However, a randomized, controlled trial (n = 205) found that service satisfaction for both telerehabilitation and in-person therapy was similar and was high (over 85%) 33 which may support the idea that there is a role for both telerehabilitation and traditional in-person therapy, especially as health systems transition to a new normal post-pandemic that values virtual care delivery.
The follow-up survey data showed similar perceived self-efficacy with chronic illness scores to a study assessing whether a telehealth chronic disease self-management programme would improve self-efficacy in Northern Ontario, Canada. 34 The authors utilized the same SEMCD-6 measure as we used in the current evaluation. 34 This study had both baseline and follow-up SEMCD-6 scores and reported a statistically significant increase in self-efficacy among the study population after experiencing the telehealth self-management programme. 34 Our study results show very similar self-efficacy scores, which suggest that we may have had similar findings if we collected data on the SEMCD-6 at two timepoints instead of cross-sectionally. However, the lack of pre-telehealth SEMCD-6 scores limits the interpretation therein.
Our results show that there is a lower quality of life between the survey respondents and the general provincial population (taken in pre-pandemic times). The number of responses indicating ‘no problems' on the EQ-5D-5L was the most similar between the survey respondents and the provincial population on the pain and discomfort domain. However, survey respondents still had higher levels of pain compared to the provincial population. The survey results indicated a higher presence of problems in all domains compared to the provincial population. This result conflicts pre-pandemic literature. A prospective study assessing the effect of a telephone-based intervention on the quality of life among elderly individuals with multiple chronic conditions showed that there was a significantly better quality of life in the telehealth group compared to the control group at follow-up. 35 Our findings may be due to a number of factors including the added stressors associated with the pandemic. An ongoing study aims to clarify the effects of the COVID-19 pandemic on quality of life using the EQ-5D-5L. 36 While this study's results are pending, another study utilizing the EQ-5D-5L to measure the quality of life during the pandemic has shown an increase in reported problems, which corroborates our findings. 37 Because our study did not include pandemic-era controls, it is unclear whether the telerehabilitation service had an impact on quality of life (positive or negative), or if the callers are sicker and have more needs than the provincial population.
Our correlational analyses showed that self-efficacy was significantly related to the quality of life, social support, and the ability to become productive quickly. This finding is not surprising. It is more likely that someone with high self-efficacy to manage chronic conditions would seek social support as required to help them manage. In addition, quality of life would be a direct reflection of someone's ability to manage their condition. This finding is consistent with the literature. A study of individuals with spinal cord injury found that those with higher perceived levels of health, self-efficacy, and social support also had high levels of subjective well-being. 38 This finding is significant because if the telerehabilitation service improves patients’ self-efficacy by providing them with self-management and wayfinding advice, this may influence their overall well-being. Our results also showed that becoming productive quickly using the telerehabilitation service was related to the quality of life. This finding is also not surprising as productivity is a common goal and the inability to be productive can negatively impact someone's quality of life. Our results also indicated that survey respondents’ overall satisfaction with the service and whether or not they followed the therapist's recommendations were not associated with age, gender, marital status, location, employment status, education level, or ethnicity in a statistically significant manner. This finding suggests that empowering individuals with self-management and wayfinding advice through the service is possible no matter their background or demographics.
Limitations
The current study lacked control groups for comparison to clarify confounding factors. A control group would have been ideal for both the 3-month follow-up surveys as well as the health care utilization pre- and post-analyses. This study notes associations, but cannot prescribe causal relationships. Second, we could not connect the issues that callers contacted the service for versus the issues for which they visited the ED. Third, selection bias was possible. However, for the immediate and follow-up surveys, the non-responder populations had similar age and gender distributions. Other important personal or experiential characteristics may have distinguished non-responders from the study participants. Recall bias may have impacted participants recall on telehealth usability and experience at 3-months post-call, but for feasibility and to promote response rates, the study was limited to one follow-up point for the health outcome surveys.
Conclusion
In conclusion, this study illuminates an early experience of providing self-management and wayfinding advice via telerehabilitation services during pandemics, wherein social distancing limits access to in-person services. Providing self-management advice allows callers to take ownership of their health care. Since self-efficacy is directly related to self-management and was found to be significantly related to the quality of life, future efforts should focus on evaluating the effectiveness of the self-management advice provided to callers using the telerehabilitation service in order to understand how it directly impacts the quality of life. At 3-months post-call, callers revealed comparable levels of social support and self-efficacy, but lower levels of quality of life, relative to established population comparators. However, all comparator data is from pre-pandemic contexts and the ultimate impact of the telerehabilitation service remains unclear, thus warranting future research.
Footnotes
Acknowledgments
We would like to acknowledge the Rehabilitation Advice Line steering committee and leadership as well as PRAXIS Spinal Cord Institute for funding this study.
Contributorship
The manuscript was prepared by KB, JC and KPM. KC, ALS, PO, EP, RM, MT, CH and KPM contributed to the conception and outline of the manuscript. KB is the Guarantor for this study. All authors contributed to manuscript revision as well as read and approved the submitted version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the PRAXIS Spinal Cord Institute (grant number G2021-22).
Ethical approval
The University of Alberta Research Ethics Board approved this study (Pro00102178).
Informed consent
All survey participants provided written informed consent to participate in this study.