
Abstract
Objective
To summarize the current status of, and the current expert opinions, recommendation and evidence associated with the use and implementation of electronic health (eHealth), telemedicine, and/or telehealth to provide healthcare services for chronic disease patients during the COVID-19 pandemic.
Materials and methods
We searched four electronic databases (PubMed, Google Scholar, Science Direct, and Web of Science Core Collection) to identify relevant articles published between 2019 and 2020. Searches were restricted to English language articles only. Two independent reviewers screened the titles, abstracts, and keywords for relevance. The potential eligible articles, papers with no abstract, and those that fall into the uncertain category were read in full text independently. The reviewers met and discussed which articles to include in the final review and reached a consensus.
Results
We identified 51 articles of which 25 articles met the inclusion criteria. All included articles indicated the promising potential of eHealth, telehealth, and/or telemedicine solutions in delivering healthcare services to patients living with chronic diseases/conditions during the COVID-19 pandemic. We synthesized the main findings into ten usages and eight recommendations concerning the different activities for delivering healthcare services remotely for those living with chronic diseases/conditions in the era of COVID-19.
Discussion and conclusions
There is limited evidence available about the effectiveness of such solutions. Further research is required during this pandemic to improve the credibility of evidence on telemedicine, telehealth, and/or eHealth-related outcomes for those living with chronic diseases.
Introduction
The novel coronavirus (COVID-19) outbreak firstly appeared in Wuhan, China in December 2019, and has been spreading globally to the extent that it met the epidemiological criteria of being a pandemic.1,2 On March 11, 2020, the World Health Organization (WHO) declared that coronavirus disease (COVID-19) becomes a pandemic. 2
As of May 27, 2020, 216 countries had reported 5,596,550 confirmed cases and 353,373 confirmed fatalities. 3 The COVID-19 is primarily transmitted via the human-to-human route through close contact and respiratory droplets. This has disrupted the way health care services are delivered and prioritized the urgency of preventing community transmission. 1
Patients with chronic disease conditions, such as patients living with diabetes and/or heart condition, may be vulnerable to the COVID-19 pandemic, which means that they are a high-risk population. 4 In response to the existential health threat of a global pandemic, social distancing is a key factor to slow the spread of COVID-19, with the result that medical visits have been changed from in-person to remote medical appointments. Thus, electronic health (eHealth), telehealth, and/or telemedicine technologies are ideal ways to adopt in this era of communicable disease. The advantages of using such technologies in the face of disasters and pandemic situations have been well documented.5,6
Researchers have published numerous articles on the role of eHealth, telehealth, and/or telemedicine in delivering healthcare services to patients with chronic diseases/conditions during the COVID-19 pandemic. Yet, due to the developing nature of the crisis, policymakers, researchers, and/or practitioners among others urgently need a synthesis of evidence to help in producing policies, decisions, and/or guidance practices in the delivery of healthcare services for patients with chronic diseases. This calls for the need to conduct a rapid systematic review of recent articles to elucidate the status of evidence regarding the role of eHealth, telehealth, and/or telemedicine technologies in managing patients with chronic diseases/conditions during the COVID-19 pandemic.
To continue providing chronic disease patients with the healthcare services needed during the COVID-19 pandemic, this rapid systematic review aimed to: 1) summarize the current status of the usage and implementation of eHealth, telemedicine, and/or telehealth; 2) summarize the current expert opinions, recommendations, and/or evidence associated with the usage and implementation of eHealth, telemedicine, and/or telehealth technologies for those patients.
Background
eHealth, telehealth, and telemedicine
According to the World Health Organization (WHO), eHealth refers to “cost-effective and secure use of information and communications technologies in support of health and health-related fields, including health-care services, health surveillance, health literature, and health education, knowledge and research”. 7 Therefore, eHealth includes all types of information and communication technology (ICT), for example, apps and websites for health promotion, screening, assessment, and therapists’ video-chat sessions. 8 Recently, there has been a huge use of these technologies across the world since there are many positive effects of the usage of eHealth, such as reducing costs and replacing face-to-face healthcare contacts and communications. 8
According to the health resource services administration (HRSA), telehealth refers to “the use of electronic information and telecommunications technologies to support long-distance clinical health care, patient and professional health-related education, public health and health administration”. 9 Researchers sometimes use the terms telemedicine and telehealth interchangeably. 10 However, there is a slight difference between these two terms. Telehealth is a broader term than telemedicine in that it can denote both remote non-clinical services (such as administrative meetings) and remote clinical services. The term telemedicine, in contrast, is limited to remote clinical services only. 9
Materials and methods
We employed a rapid systematic review methodology to provide the best available evidence within a shortened period 11 to synthesize and communicate the role of eHealth, telehealth, and/or telemedicine in delivering healthcare services to chronic disease patients during the COVID-19 pandemic. Rapid systematic reviews refers to “a form of knowledge synthesis that accelerates the process of conducting a traditional sysmatic review through streamlining or omitting a variety of methods to produce evidence in a resource-efficient manner” 12 (p.80). In this rapid review, we followed streamlined classic systematic review methods to synthesize evidence in a timely manner to inform decision makers in making emergent decisions in healthcare settings. 13 Since this is a rapid systematic review and due to the urgent nature of the pandemic and time constraints, this review was not registered on PROSPERO.
Search strategy and eligibility criteria
The literature search was conducted on April 20, 2020, and again on May 15, 2020. We conducted an electronic search using four electronic bibliographic databases: PubMed, Google Scholar, Science Direct, and Web of Science Core Collection to identify relevant articles. Searches were restricted to English language articles only. The keywords that were employed include: “eHealth,” OR “telemedicine,” OR “telehealth,” AND “COVID-19,” OR “coronavirus,” AND “chronic disease.”
Results obtained from the electronic search were downloaded into EndNote bibliographic software version X8 (Thomson Reuters, Philadelphia, USA). Inclusion criteria were as follows: articles were required to 1) focus on any chronic disease or condition; 2) be related to the COVID-19 pandemic; 3) focus on the use of eHealth, telemedicine, and/or telehealth; and 4) have been completed between December 1, 2019 and May 15, 2020. Because of the evolving nature of the pandemic and the lack of an available number of experimental and complete studies, we included all articles that met the indiscriminate inclusion criteria regardless of the study design, such as preprint articles, commentary, and opinion papers.
Selection of articles for reviews
Initial screening for articles was performed by two independent reviewers (HB and SA) based on titles, abstracts, and keywords for relevance. The selected articles were based on the information obtained from the title, abstract, and keywords to see if the pre-defined inclusion criteria were met. Papers with no abstract available were added to a full-text review. We categorized articles into three categories: eligible, not eligible, and uncertain. To confirm eligibility, the potential eligible articles, papers with no available abstract, and those falling into the uncertain category were read in full text independently. Then, the reviewers met and discussed which articles to include in the final review and reached a consensus.
Data extraction
Data were extracted from the included articles on: author’s name, publication year, paper type, country of the study, population and/or chronic disease, type of technology, current status of the use of eHealth, telemedicine, and/or telehealth, and outcomes (expert opinions, recommendation and/or evidence associated with the use of eHealth, telemedicine, and/or telehealth technologies).
Results
Overview
The majority of the included articles were reviews and experts’ opinions; thus, the quality of evidence was not assessed due to the absence of included trails. Of the 51 retrieved articles, 25 met the inclusion criteria. Figure 1 illustrates the selection process using the PRISMA flow diagram.

Selection process using PRISMA flow diagram.
Most of the articles used the term telemedicine (n = 17; 68%) to describe the used technology or recommended to use in providing healthcare services needed for chronic disease patients.14–30 Fifteen articles used the term telehealth (53.8%),15–17,27–38 while two articles used the term eHealth (7.7%).18,32 However, some of these articles used more than one term (e.g., 17 ).
The settings included the United States,16,17,20,30,31,34,37,38 Western China, 25 developing countries, 21 Europe,14,15,18 Australia, 32 Canada, 18 Mexico, 18 and Asia. 18 Twelves articles had no defined setting.19,22–24,26–29,33,35,36,38 Six articles focused on cardiovascular disease (CVD),15,28,30,32,33,36 two on cancer,17,18 two on chronic orthopedic conditions,31,38 two on chronic neurological disorders,20,27 one on chronic pain, 19 one on cystic fibrosis, 16 one on urologic chronic conditions, 22 one on mental health disorders, 34 one on chronic diseases requiring occupational therapy, 29 one on allergies, asthma, and immunodeficiency, 23 two on cirrhosis and chronic liver diseases,24,35 one on diabetes, 26 and one on high-risk pregnancies. 37 Three articles focused on chronic diseases in general.14,21,25
The types of paper were varied including six review paper,22,23,28,32,35,37 three articles,13,14,36 four expert opinions,18,19,27,34 two viewpoints,24,26 one brief correspondence, 21 one commentary, 33 one position statement, 31 one feasibility study, 15 one perspective, opinion, and commentary, 20 one clinical practice statement, 29 one research letter, 16 one short survey, 17 one quantitative study, 30 and one mini review. 25
Tables 1 to 3 detail the current status of the use and implementation of eHealth, telemedicine, and/or telehealth technologies to manage chronic disease patients during the COVID-19 pandemic as well as the main findings and/or recommendations regarding the use of eHealth, telemedicine, and/or telehealth technologies in providing care to patients living with chronic disease/condition during the pandemic.
Included opinion based on current observation articles.

Included expert opinion articles.

Included articles about the description of e-health actions conducted during the COVID-19 crisis.

The current status of eHealth, telemedicine, and/or telehealth solutions
Most of the included papers used eHealth, telemedicine, and/or telehealth to provide a healthcare services for chronic disease patients during COVID-19 crisis. We summarized these services into six usages of eHealth, telemedicine, and/or telehealth as reported in the included articles (see Figure 2). The following items outline the usages of such technological solutions, which are: follow-up visits, training, consultations, medications, communication, and caregiver support. The majority of the included articles reported that they use such technological solutions as a medium vehicle to consult their patients18,20,28,32,34,37,38 using videoconferencing or telephone. Five articles reported the use of virtual visits for patient’s follow-up appointments;17,18,34,37,38 three stated the use of virtual communication tools (e.g., chatbot) to communicate health information,23,28,38 and one noted the utilization of video calls to help provide caregiver support virtually; 18 two referenced the importance of ensuring access to medications as well as tracking the prescription of medication electronically.18,32
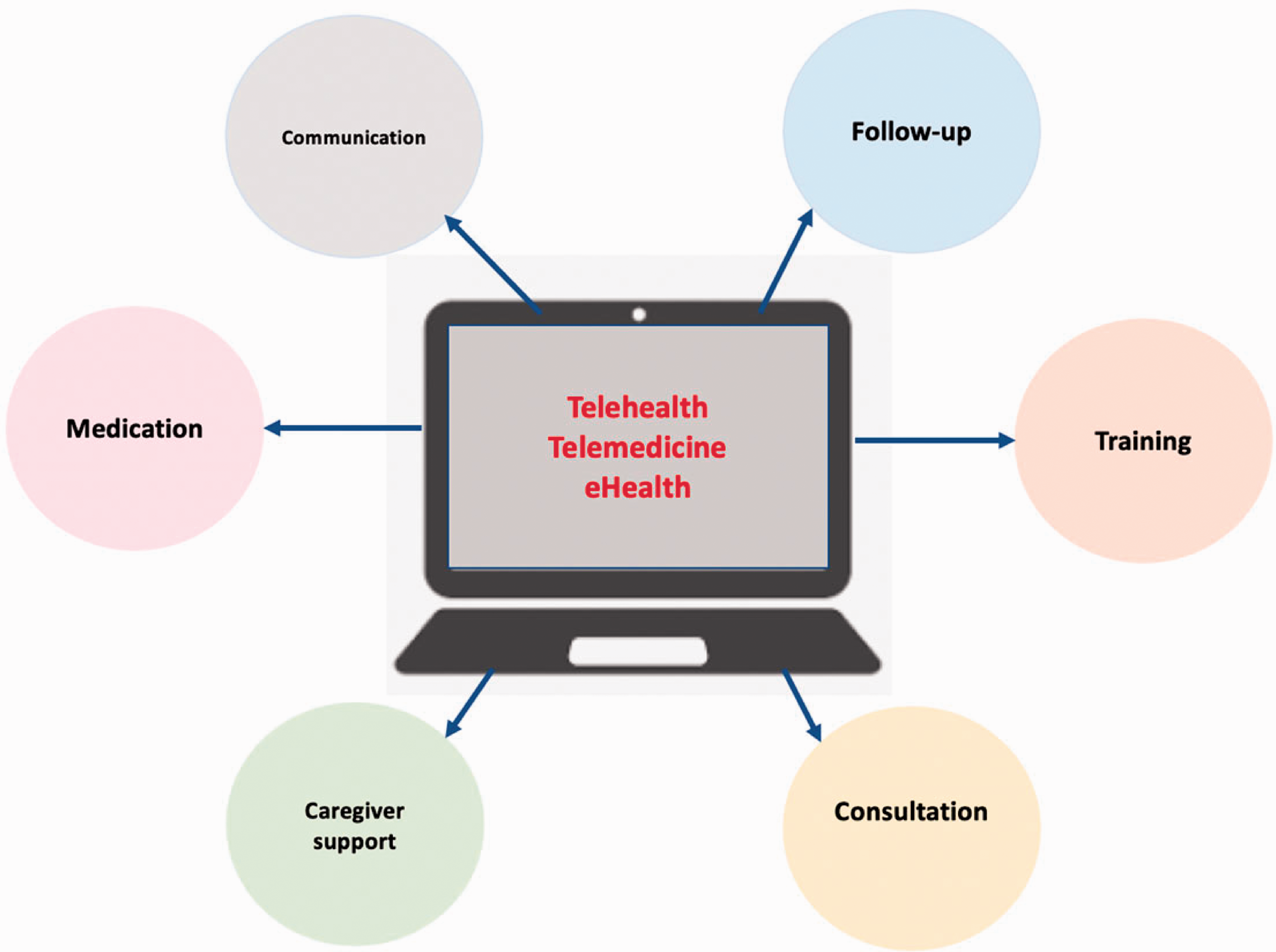
The six usages of eHealth, telemedicine, and/or telehealth solutions during the COVID-19 pandemic.
Two articles reported the importance of using such technological solutions for training purposes for both healthcare providers and patients.37,38 For instance, training patients on how to use a home blood pressure cuff become important for pregnant women with hypertensive disorders receiving telehealth care; thus, such training can facilitate the provision of virtual prenatal care. 37 Furthermore, one reported the use of virtual reality to provide surgical training for surgeons as well as to remotely deliver physical activity sessions to patients at home. 38
The top recommendations of eHealth, telemedicine, and/or telehealth solutions
We synthesized the main findings of this rapid review into eight recommendations in accordance with the remote healthcare delivery life cycle for chronic disease patients during the pandemic (see Figure 3). The remote healthcare delivery life cycle consists of three stages: pre-, during, and post- medical visits, for which each has a set of activities. Pre-medical visits refer to the period before patients with chronic diseases visit the clinic or the building phase of the telemedicine, telehealth, or eHealth system. The stage during medical visits refers to the time when healthcare professionals use this technology to deliver healthcare services to patients. Lastly, post-medical visits are defined as the period after the patients’ visit and take into account the services that this technology has provided. There can be an overlap between these stages, and some activities can take place in multiple stages. The activities of this technology are as follows: 1) system integration, 2) remote outpatient care, 3) billing reimbursement, 4) continuity of care, 5) standardized transition process, 6) cost-effectiveness, 7) simplicity, and 8) privacy and data sharing.

The top recommendations of eHealth, telemedicine, and/or telehealth solutions.
Most of the included articles concentrated on the provision of continuity of care due to the nature of the diseases and conditions that were examined in this research.14,15,17,19–22,26–28,30–34,37 Ten articles recommended focusing on remote outpatient care activity;17,23,24,28,32,33,35–38 four of the included research articles reported system integration,13,15,32,33 three articles stated the standardized transition process,13,15,18 and two articles highlighted the need to conduct more cost-effectiveness studies,16,31 and studies on privacy and data sharing.14,32 Lastly, one article also emphasized billing reimbursement, 15 while another article stated the importance of simplicity in the technology. 32
Discussion
The present paper has undertaken a rapid review to summarize the role of mHealth, telehealth, and/or telemedicine solutions in the delivery of healthcare to chronic disease patients during the COVID-19 pandemic. This rapid review confirms that researchers from several specialties across the world have made a huge effort to improve healthcare services for chronic disease patients. All included articles indicated the promising potential of eHealth, telehealth, and/or telemedicine solutions in delivering healthcare services to patients living with chronic diseases/conditions during the pandemic. Some of these articles also support and encourage the continuity of using such technological solutions in the future when the COVID-19 crisis is over.
The authors of the available literature included their key findings and recommendations regarding the use of such technological solutions to ensure the continuity of delivering services to chronic disease patients during the pandemic. We synthesized these results and determined the top eight recommendations concerning the different activities for delivering healthcare services remotely for those living with chronic diseases/conditions in the era of COVID-19. However, there is limited evidence available about the effectiveness of such solutions; quantitative data were limited and no experimental design studies were found. Having more experimental studies as one of the articles noted 29 is required to improve the credibility of evidence on the outcomes for telemedicine, telehealth, and eHealth.
We aimed to include all chronic diseases in the search strategy. However, there were a limited and under-represented number of papers about some chronic diseases/conditions compared to others. Evidence on the role or effect of using such technological solutions to deliver healthcare services to patients during the pandemic may vary based on the type of chronic disease/condition. If more research were available, it would be possible to group the evidence of the role of eHealth, telehealth, and telemedicine on the delivery of healthcare services based on the type of chronic disease/condition. It is important to note that the term “chronic disease” was the only diagnosis specific search keyword used to search in the databases, which may result in excluding articles that only use the exact diagnosis term (e.g., diabetes) in their papers. Future work should address this limitation by using more specific chronic disease diagnosis keywords to search in the databases.
The majority of the included articles (n = 12; 46.1%) had no specified country; reporting the country of the study may assist in identifying which technology(ies) is/are the best fit in a specific context. It could aid in highlighting some recommendations and challenges associated with designing telehealth, telemedicine, and/or eHealth solutions. 39
Furthermore, it is very important to improve the healthcare system infrastructure for developing and even some developed countries, such as Italy. Infrastructure refers to “the built environment and supporting elements: equipment, access, information technology (IT), systems and processes, sustainability initiatives and staff” 40 (p.4). A lack of infrastructure in addition to other factors (e.g., less educated patients 41 ) would affect the quality of health care delivered to these patients—it could be more harmful than beneficial. 42 The literature cites some recommendations regarding the design and development of the infrastructure for this technology. First, the evidence points to the importance of incorporating intelligence, mobility, usability, adaptability, and interoperability features into the infrastructure. 43 Second, it advises against the inclusion of an upper limit of quality of services measurements for infrastructure, such as bandwidth. 43 In addition, there are various recommendations related to the use of eHealth in developing countries, such as avoiding the use of a restricted number of Internet service providers and poor telecommunication infrastructure. 44 Other evidence points to the valuable additions of superior customer service and customization features on products and services while developing the eHealth system. 44 Moreover, there are additional important issues that researchers, designers, and developers must consider while building telemedicine infrastructure. First, it is necessary to monitor and manage the costs, since these projects can be expensive. 45 In addition, they must focus on leveraging existing information and communication technology (ICT) infrastructure to take advantage of the value of telemedicine technology, especially in developing or undeveloped regions, such as Sub-Saharan Africa. 46
Most of the included articles used the term telemedicine, followed by telehealth, whereas few articles used the term eHealth. In fact, there were variations in using these terms in which some seemed to use them interchangeably while others distinguish between them. It may be the case that these variations can infer the ambiguity and the lack of clarity in the terms’ definitions and their concepts. 10
To our knowledge, this is the first review that explores the role of eHealth, telehealth, and telemedicine technology in the delivery of healthcare services to patients living with chronic diseases/conditions during the COVID-19 crisis. However, this study had some limitations. This is not a comprehensive review, as the search was limited to articles published in English. Thus, we may have excluded relevant articles published in other languages. Furthermore, the quality of the included articles is not known; hence, we should exercise caution when interpreting this evidence.
Although much literature is being published on the role of eHealth, telehealth, and/or telemedicine during the COVID-19 crisis, there is a lack of evidence of quantitative, qualitative, and mixed-methods studies, which underscores the need for more rigorous studies. However, this rapid review was conducted in a short timeframe, and more articles are rapidly emerging daily. The justification of the present paper is that the spread of the pandemic creates the need to rapidly assess and synthesize the evidence that has been generated. Future work should address the limitations of this work using a traditional systematic review to further synthesize the role of eHealth, telehealth, and/or telemedicine during the pandemic, a context for which the digitalization in the health care system has exploded.
Despite these limitations, we highlight critical gaps in the literature, including the lack of studies focusing on the effects of using eHealth, telehealth, and/or telemedicine in delivering healthcare services to chronic disease patients during the COVID-19 pandemic. In other words, this rapid review offers some opportunities for future research. Further significant evidence is needed on the effectiveness and cost-effectiveness of mHealth, telehealth, and/or telemedicine-based solutions.
Conclusion
This rapid review summarizes the existing role of eHealth, telemedicine, and/or telehealth in the continuity of delivering healthcare services to patients with chronic diseases or conditions during the era of the COVID-19 crisis. The literature lacks studies on the effects of eHealth, telemedicine, and/or telehealth on delivering health services such as medical consultations to chronic disease patients during this crisis. However, experts concur that the use of such technologies is likely to offer an opportunity to warrant the continuity of delivering the needed healthcare services to patients living with chronic health diseases or conditions during and after this pandemic. This emphasizes the urgency of conducting further research during this pandemic to assess the role of these technologies in improving access to service for those living with chronic diseases.
Footnotes
Contributorship
All authors contributed substantially to all stages of the review, and helped to draft and revise the manuscript. All authors approved the final version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
None required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of the article.
Guarantor
HB.
Peer Review
This manuscript was reviewed by reviewers who have chosen to remain anonymous.