
Abstract
Case summary
Major avulsion of the triceps tendon insertion was diagnosed in a 7-year-old domestic shorthair cat 3 weeks after developing sudden severe weightbearing lameness of the left thoracic limb. Diagnosis was confirmed with orthopaedic, radiographic and ultrasonographic examinations. The absence of adequate bone stock prevented the use of conventional techniques for tendon reinsertion. Instead, the tendon was reattached using an ultra-high molecular weight polyethylene (UHMWPE) ExtraTape prosthesis. It was stitched into the triceps tendon and superficial fascia, then passed through a bone tunnel drilled in the olecranon and secured with a preassembled cortical button. No external coaptation was used. Although the cat experienced temporary mild lameness, pain-free and satisfactory use of the left thoracic limb was observed 4 weeks postoperatively. By 12 weeks, the cat’s gait had returned to normal, with no gap between the tendon and the olecranon. The cat resumed normal gait and range of motion 8 months postoperatively.
Relevance and novel information
Triceps tendon disruption is difficult to manage. Conventional repair techniques consist of suturing the tendon ends and prolonged immobilisation with an external fixator, which may cause postoperative complications. This option is particularly difficult to implement in cats, which represents a challenge in postoperative management. The successful outcome obtained here suggests that surgical repair using the ExtraTape prosthesis, without external coaptation, may be a viable alternative for similar cases.
Introduction
Triceps tendon disruption is a rare disabling condition in dogs and cats that causes lameness, reduced extension of the elbow, soft tissue swelling and pain. 1 Disruption may occur either within the tendon at the musculotendinous junction or at the osteotendinous junction as tendon avulsion. 2 Tendon avulsion occurs when a tendon pulls away from the bone, occasionally taking small bone fragments with it. It may be due to trauma, bite wounds or abscess formation near the triceps muscle. 1 It may also occur as a collateral result of treatments performed near the triceps region, such as surgical placement of an intramedullary pin to repair a radius and ulna fracture. 1 In addition, prolonged administration of high doses of systemic corticosteroids, as reported in dogs, 3 can contribute to tendon weakening. Diagnosis can be confirmed using medical imaging techniques such as radio-graphy,4,5 MRI6,7 or ultrasonography. 8
Surgical repair of tendon avulsion is challenging as tendons heal slowly, 9 needing sufficient tensile strength to minimise excessive scar formation and preserve the gliding function necessary for limb movement. 10 Mostly described in dogs, conventional repairs involve reapposing the tendon ends using tendinous suture patterns passed through bone tunnels, such as the modified three-loop pulley,1,8,11 horizontal mattress polyester sutures 7 or the Krackow suture technique. 12 For chronic triceps tendon ruptures with retracted ends, mesh grafts have also been used. 6 Tendon reapposition is often supported by rigid external coaptation using splints, casts or transarticular external fixators.1,8,12
External coaptation is difficult to implement in cats, which represents a challenge for postoperative management. Recently, an ultra-high molecular weight polyethylene (UHMWPE) implant sutured in the triceps tendon and fixed through a bone tunnel on the olecranon was used to reappose a retracted triceps tendon avulsion in a dog. 13 Unlike conventional repair techniques, this option avoided long immobilisation of the affected limb with an external fixator and allowed immediate weightbearing to promote recovery. 13
This article reports the surgical procedure and clinical outcome of a triceps tendon avulsion in a cat treated with UHMWPE suture tape, without postoperative immobilisation of the affected limb.
Case description
Clinical history and orthopaedic examination
A 7-year-old spayed female domestic shorthair cat weighing 4.6 kg was presented 3 weeks after having developed sudden severe weightbearing lameness of the left thoracic limb (graded 3/5) 14 with no elbow extension. Its left elbow collapsed on every step (Figure 1; see also video 1 in the supplementary material). On palpation, the olecranon appeared more prominent, and a palpable defect was noted at the triceps tendon insertion site. The triceps muscle was retracted cranio-proximally to the olecranon. No additional orthopaedic abnormalities or wounds were observed, and the neurological examination results were normal.

Preoperative weightbearing lameness. Left elbow collapses at each step
Diagnostic imaging procedures under general anaesthesia
Mediolateral radiographs (Vet-Tech 250HFG3; GER) of the left elbow showed triceps tendon avulsion associated with a thickening of the muscle mass (Figure 2). Ultrasonography (microconvex probe PVT-712BT 7 MHz; Toshiba, and CUS-AA000; Canon) did not allow the identification of the triceps tendon at its insertion on the olecranon (Figure 3). Ultrasound revealed a small quantity of hypoechoic fluid and hyperechoic disorganised tissue at the site, with the triceps tendon located 1 cm cranial to the olecranon (Figure 3). Radiographic and ultrasonographic evaluation of the right elbow was normal. Surgical reapposition of the triceps tendon was decided.

Preoperative radiographs of both elbows in full flexion, flexion and extension. Radiographic examination of the affected left elbow shows triceps tendon avulsion associated with thickening of muscle mass compared with contralateral limb. No fracture is visible. L = left; R = right

Preoperative ultrasound imaging. (a) Identification of the triceps tendon is not possible at its physiological insertion site in the olecranon (green O). A small quantity of liquid and disorganised tissue are present (blue arrow). (b,c) The triceps muscle (purple arrow) is visible 1 cm cranial to the olecranon. A small quantity of liquid and disorganised tissue are present (blue arrow). (d) The contralateral triceps muscle is normal. L = left; R = right
Premedication and anaesthesia
The cat received medetomidine (5 µg/kg IV, Sedator; Dechra), ketamine (1 mg/kg IV, Clorketam; Vetoquinol) and methadone (0.2 mg/kg IV, Comfortan; Dechra). Anaesthesia was induced with a titration of propofol (Proposure; Axience) and maintained with isoflurane (Isorane; Axience) using an endotracheal tube. The cat received amoxicillin and clavulanic acid (1 g/200 mg, Levmentin; 12.5 mg/kg IV, Delbert) during surgery.
Surgical treatment
The left thoracic limb was aseptically prepared for surgery and draped in a standard manner. The cat was positioned in right lateral recumbency. A caudolateral approach to the left elbow was performed and extended cranially to the proximal third of the humerus. The retracted triceps tendon was identified (Figure 4a) and incised on its caudal half-thickness along its entire length. A 2 mm tunnel was drilled from the medial to the lateral side of the olecranon. An ExtraTape prosthesis (Novetech Surgery) was placed extra-capsularly to reattach the triceps tendon to the olecranon. This 2 mm wide prosthesis was made of medical grade UHMWPE preassembled with a titanium cortical button and a suture needle (Figure 4b). It was slid laterally to medially through the tunnel using a wire loop. The cortical button was placed against the lateral side of the olecranon. With the elbow in hyperextension, the triceps tendon was reattached to the olecranon. The prosthesis was sandwiched in the thickness of the tendon using simple Fibertech 2.0 stitches (Novetech Surgery) (Figure 4c,d), one of which was anchored in the cortical button. The suture was continued through the superficial fascia of the triceps using Fibertech 2.0 (Novetech Surgery) with a Bunnell–Meyer suture pattern (Figure 4e). A knot was made proximally at the end of the prosthesis before sectioning the proximal end. The surgical site was rinsed abundantly before routine closure. No external coaptation was applied. Postoperative radiographs showed satisfactory prosthesis placement and triceps tendon position (Figure 5).

Peroperative procedures. (a) Identification of retracted triceps (blue arrow) and olecranon (green arrow). (b) Preparation of the prosthesis before sliding it through the olecranon tunnel. (c,d) Prosthesis sandwiched in the thickness of the tendon. (e) Prosthesis sutured through the triceps superficial fascia

Immediate postoperative radiographs confirming satisfactory position of the prosthesis and satisfactory triceps tendon reapposition. L = left
Postoperative management
The cat received methadone (0.2 mg/kg IV q4h, Comfortan; Dechra) for 24 h. One day after surgery, lameness had already improved (graded 2/5) and the elbow no longer collapsed (Figure 6; see also video 2 in the supplementary material). The cat was discharged 48 h after surgery, with instructions for room rest for 3 months. Antibiotics (q12h, Clavaseptin; Vetoquinol) for 7 days and meloxicam (1.5 mg/ml, Meloxidyl, and 0.05 mg/kg q24h, Ceva Santé Animale) for 5 days were prescribed.

Gait at 24 h postoperatively: left elbow no longer collapses during locomotion
Postoperative follow-up examination
At 4 weeks postoperatively, the cat seemed pain-free with satisfactory use of the left thoracic limb. Temporary lameness (graded 1/5) was still present. At 12 weeks postoperatively, the gait was normal (graded 0/5). The cortical button was palpated laterally to the olecranon. The palpation of the triceps and its tendon was painless. No gap between the olecranon and the triceps tendon was observed during ultrasound examination. After this follow-up control, full resumption of activity was authorised. At 8 months postoperatively, the cat had resumed normal activity. No lameness of the thoracic limb was observed by both owners and surgeons (graded 0/5). The left elbow was pain-free and without swelling. The cortical button was felt on the lateral side of the left elbow with no signs of pain. Radiographs showed satisfactory button placement and a 0.5 cm long mineralisation of the triceps tendon (Figure 7a). No gap was observed between the olecranon and the triceps tendon on ultrasound examination (Figure 7b).
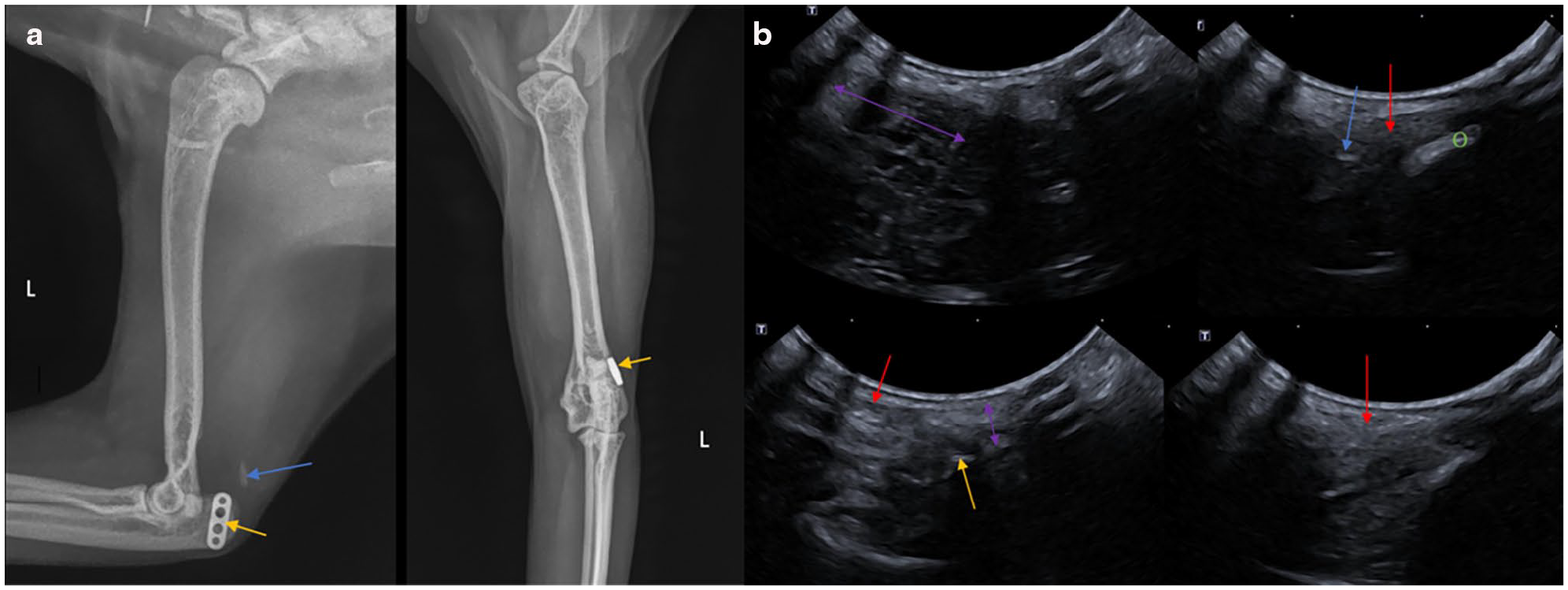
Radiographs and ultrasonography at 8 months postoperatively. (a) Radiographs show mineralisation of triceps (blue arrow) and good position of the prosthesis (yellow arrows). (b) Ultrasonography shows satisfactory reapposition of the triceps tendon on the olecranon [triceps muscle (purple arrows), triceps tendon (red arrows), olecranon (green O), prosthesis (yellow arrow), mineralisation (blue arrow)]
Discussion
The use of a synthetic prosthesis allowed satisfactory reinsertion of the triceps tendon without postoperative immobilisation of the limb. The cat showed excellent clinical and functional recovery, resuming normal gait and activity at 3 and 8 months postoperatively, respectively.
Orthopaedic and radiographic examinations confirmed the diagnosis of triceps avulsion and excluded any concomitant injuries.4,5,11,13 Ultrasonography provided additional information about the complete avulsion of the affected tendon from its physiological insertion site.1,8 Although MRI6,7 and CT 15 could have also provided this information, they were not used in this case. These findings helped in choosing an appropriate surgical treatment tailored to the nature and severity of the condition.6,7
The prosthesis was preassembled with a suture needle at one end and a cortical button at the other, facilitating its passage through the tunnel into the olecranon. The use of the cortical button avoided the risk of using an oversized interference screw for fixation. 16 The prosthesis was long enough to be sutured in the tendon and strong enough (800 N reported by the manufacturer) to provide stable reinsertion of the triceps tendon at its physiological insertion site. This resulted in a functional, pain-free elbow with no gap between the olecranon and the triceps tendon.
While a postoperative gap larger than 3 mm after triceps tendon reapposition has been reported in dogs, 1 functional clinical outcomes have been often good in both dogs and cats when repairs were performed using nylon, 11 polyester, 7 polypropylene,5,6 polyamide4,8 or UHMWPE implants.13,16,17 Previous reconstructions in dogs have also incorporated autogenous thoracolumbar fascia grafts 18 or polyurethane mesh. 6 Unlike the abovementioned clinical reconstructions, except for one, 16 the triceps tendon reapposition in the present case did not involve postoperative external coaptation. This was made possible by the UHMWPE prosthesis, which provided enough strength and stability for a functional repair according to the cat’s size. This approach is in line with the findings from ex vivo biomechanical testing of larger UHMWPE implants used in canine Achilles tendon repairs. 19
The decision to use the ExtraTape prosthesis was made to reduce the risk of complications associated with external coaptation, such as cutaneous irritation 15 and infection due to possible contamination from organic fluid on the pins. 20 In addition, the use of an external fixator requires a second surgical procedure for removal. Complications associated with spica splints include skin laceration, 11 skin necrosis and/or infection. 1 Side effects after the removal of external coaptation, resulting from limb immobilisation, have also been reported. These include amyotrophy,1,5–8,13 reduced range of motion of the elbow joint,1,4,6,15,17 lameness,1,6,15 pain on palpation1,17 and tendon thickening.1,4,8,18
The technique used in this cat resulted in a satisfactory functional clinical outcome with no complications or side effects observed during the 8-month follow-up. Biomedical-grade UHMWPE is a biocompatible material well tolerated by the organism 21 and the cat showed no signs of reaction. Although the braided structure of the prosthesis may increase the risk of infection,17,22 strict asepsis was applied during the surgery and there were no postoperative complications.
Radiographs taken 8 months postoperatively revealed mineralisation of the triceps tendon, which could indicate early tendinopathy, as reported in previous triceps tendon repairs.1,4,8 A longer-term follow-up might have helped to determine how this condition evolved over time.
Conclusions
Although further studies are needed to determine its reproducibility, the satisfactory outcome of this technique suggests that the surgical repair of feline triceps tendon avulsion using an ExtraTape prosthesis without external coaptation may be a viable treatment option in similar cases.
Footnotes
Acknowledgements
The authors thank Emilie Cooke-Martageix for copyediting this article.
Supplementary material
The following files are available as supplementary material:
Video 1: Severe weightbearing preoperative lameness, with left elbow collapsing on every step.
Video 2: Gait one day after surgery, with lameness that had already improved and the elbow no longer collapsing.
Conflict of interest
BG and AC are employed by Novetech Surgery. The authors have no additional conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.