
Abstract
Objectives
The aim of this study was to report the clinical outcomes in a series of traumatic elbow luxations in cats treated with closed reduction and a temporary transarticular type II external skeletal fixator (ESF).
Methods
A retrospective review was conducted of traumatic elbow luxation cases in cats at two referral centres. Data collected included signalment, history, clinical assessment, radiographic findings, surgical procedures and complications. Short-term follow-up was based on clinical evaluations at 2 and 6 weeks postoperatively. Long-term follow-up was based either on a telephone interview with the owner or a clinical evaluation.
Results
Eight cats were included. Five cats experienced lateral elbow luxation, while three cats had medial elbow luxation. All cats with medial elbow luxation exhibited radiographic signs of medial humeral epicondylitis. The median age was 9 years (range 3–15). The elbow luxation was treated by closed reduction and percutaneous placement of a temporary transarticular type II ESF, which was removed 2 weeks postoperatively. Two minor complications were recorded. Elbow reluxation and major complications were not encountered. The 6-week postoperative evaluation and long-term follow-up revealed a lameness of grade 1 in 1/8 cats and 0 in the remainder. Elbow range of motion was normal in all cats.
Conclusions and relevance
None of the cases treated with this protocol experienced recurrence of elbow luxation. All cats demonstrated an excellent outcome based on the lameness score, the low complication rate and the follow-up telephone interview. The technique is minimally invasive and carries a low incidence of complications. Concurrent orthopaedic disease, such as medial humeral epicondylitis, may predispose to medial elbow luxation.
Introduction
The feline elbow joint is a combination of several articulations comprising the humeroradial, humeroulnar and proximal radioulnar joints.1,2 It is an intrinsically stable joint, with uniaxial hinge-like movement. 3 The main stabilisers of the feline elbow joint are the collateral ligaments, which restrict medial and lateral translation as well as pronation-supination movements.2,4 Traumatic elbow luxation is an uncommon injury in cats. 5
Lateral elbow luxations account for approximately 65% of cases in cats because the distal slope and the relatively large size of the trochlea of the humerus prevent medial displacement of the radius and ulna. 5 Medial and caudal luxations have also been documented in cats. 6 A distinctive feature of the feline elbow is the arrangement of the collateral ligaments, which differs from that of dogs in their course and strength. 6 The ulnar part of the lateral collateral ligament is broader than the radial part, and it courses caudally to insert on the lateral coronoid process.7,8 The ulnar part of the medial collateral ligament is also broader than the radial part.7,8 The ulnar parts of the collateral ligaments are taut throughout the range of motion (ROM) whereas the radial parts are lax in flexion allowing an increased range of rotation of the radial head. 9 A cadaveric study reported that, in cats, both the medial and lateral collateral ligaments needed to be transected to induce an elbow luxation. 10 In dogs, luxation could be induced by transection of the lateral collateral ligament alone, but not by transection of the medial collateral ligament alone. 10 Cats lack a strong interosseous ligament between the radius and ulna. 8 The radioulnar joint allows rotation of the ulna around the radial head, which is necessary for a high degree of pronation and supination. 6 The annular ligament surrounding the radial head originates from the lateral collateral ligament and inserts on the medial coronoid processes of the ulna.6,7 This ligament, along with the oblique ligament (a cranial joint capsule reinforcement) 9 and the olecranon ligament act as important secondary stabilisers of the elbow. 4 The olecranon ligament is taut when the elbow is flexed and contributes substantially to the stability of the cat’s elbow. 9 Elbow luxation is a rather uncommon injury in cats, probably because of this particular feline anatomy.2,10
Although treatments for traumatic elbow luxation have been described in numerous case series in dogs,11–19 there is a paucity of information in the feline veterinary literature. In cases of acute traumatic elbow luxations without concurrent articular or periarticular fractures, closed reduction may be considered as an option.6,20 Surgical stabilisation has also been advocated as a primary option or in cases in which ongoing instability renders closed reduction unsuccessful. 6 However, according to a recent study, closed reduction is not recommended for initial treatment in cats owing to the high reluxation rate, which has been reported as 61%. 5 Moreover, as transection of both collateral ligaments is required for elbow joint luxation in cats, significant trauma is often associated, implying frequent major instability. 10 In both cats and dogs, any ruptured ligaments, joint capsule structures and muscles should be sutured.2,20 When epicondyle avulsion is noted upon radiographic evaluation, surgical management is recommended. 2
Surgical techniques described in cats include primary suturing of ligaments, 21 ligament prosthesis using screws and washers, 20 circumferential sutures using bone tunnels, 22 transarticular pinning 23 and elastic transarticular external skeletal fixation. 24 External immobilisation is advocated after closed reduction using either a spica splint, support bandage or Robert-Jones bandage.2,25,26 Although rigid external skeletal fixators (ESFs) have been mentioned in the field of veterinary medicine for the management of elbow luxation, 27 there are no published clinical reports describing their use in cats.
The objective of this study was to report the clinical functional outcome and complications of eight cats with traumatic lateral or medial elbow luxation treated with closed reduction and a temporary transarticular type II ESF.
Material and methods
Study design
Medical records from two referral centres were reviewed for cases of cats with traumatic elbow luxation treated between 2018 and 2022. Only cases amenable to management via closed reduction were included in the study. Closed reduction was attempted on cats presented with an acute traumatic luxation, without any concurrent articular/periarticular fractures and with an intact radioulnar joint. If reduction was successful, even if instability was still present, a temporary transarticular type II ESF was placed.
Data collected included history, signalment (breed, age, weight), clinical examination (including general examination, complete orthopaedic and neurological examination), additional pathology related to the joint and radiographic findings. Clinical evaluation at 2 and 6 weeks postoperatively and a long-term follow-up were required for each patient to be included. Lameness was scored as described by Montavon et al: grade 1 = hardly visible lameness; grade 2 = clearly visible lameness; and grade 3 = toe-touching or non-weight-bearing lameness. 6 Mediolateral and craniocaudal radiographs of the elbow joint were retrospectively reviewed by a board-certified radiologist (AB). The presence of concurrent lesions, such as avulsion of the epicondyle, presence of concurrent fractures/mineralisation fragments and presence of supinator sesamoids, was also assessed. The exclusion criteria encompassed any cat presenting with articular or periarticular fracture, epicondyle avulsion, caudal luxation or radioulnar dislocation. All owners signed an informed consent form after complete information was given about the surgical technique and the follow-up.
Surgery
Intravenous cefalexine 22 mg/kg (Ceporex; Intervet) was administered once perioperatively and discontinued postoperatively. Meloxicam 0.05 mg/kg (Metacam; Boehringer Ingelheim), methadone 0.2 mg/kg (Comfortan; Dechra) and midazolam 0.2 mg/kg (Midazolam; Mylan) were administered intravenously (IV). Anaesthesia was induced with propofol 2–6 mg/kg IV (Propovet Multidose; Zoetis) given to effect and maintained with isoflurane. The affected limb was clipped starting at the level of the carpus and extending distal to the shoulder joint. Closed reduction of the luxation was then performed. A Campbell test 19 was conducted for each patient to assess collateral ligament integrity. Pronation and supination angles were not quantified in the present study because of the significant interanimal variability. 10 The authors conducted a systematic subjective comparison of elbow stability, using the contralateral limb as a reference for each animal. 10
After closed reduction of the elbow, Steinmann pins were placed using the technique described by Vedrine in 2017. 24 While maintaining the elbow in an extended position, a smooth 2 mm Steinmann pin was inserted into the distal quarter of the humerus. The pin was cautiously positioned against the humerus in direct contact with the cis cortex, in a lateromedial direction, proximal to the supracondylar foramen and perpendicular to the long axis of the humerus. The pin was subsequently fully inserted into the humerus and emerged medially. A second smooth 2 mm Steinmann pin was then placed parallel to the first one in the centre of the olecranon, in a lateromedial direction. Two 2 mm connective stainless-steel bars were clamped to the pins using Meynard fixation clamps (Coapteur à flasque JAM 699089; Coveto) to construct a transarticular type II ESF. All surgical procedures were performed by a board-certified surgeon (MH or PP). Orthogonal radiographs of each affected elbow joint were obtained immediately postoperatively. Owners were instructed to clean the pin entry points twice daily using a 0.05% chlorhexidine solution and to carefully monitor for signs of migration or premature pin loosening. During the postoperative period, meloxicam 0.05 mg/kg PO q24h (Metacam; Boehringer Ingelheim) was administered for 5 days. Antibiotics were not prescribed. It was strongly recommended to provide an enclosed area to limit activities.
Follow-up
Two weeks postoperatively, every patient underwent clinical and radiographic assessment. A Campbell test 19 was performed with the connecting bars of the ESF removed to check the stability of the elbow. If the elbow was found to be stable, the ESF was removed. After removal of the ESF, the protocol involved a 15-day period of crate rest. This was followed by a transition phase of another 15 days, designed to facilitate a gradual resumption of the cat’s normal activity levels.
Six weeks postoperatively, an orthopaedic examination was performed and the lameness score was recorded following the previously described method. 6
For the long-term follow-up, either a telephone interview (see the protocol in the supplementary material) with the owners or a clinical evaluation was conducted at least 6 months after the surgical procedure.
Complications
Complications were classified following the study of Cook et al 28 as catastrophic (permanent unacceptable function, death, euthanasia), major (additional surgical treatment or medical treatment required) or minor (not requiring additional surgical or medical treatment to resolve).
Results
Study design
Eight cats met the inclusion criteria (Table 1). All patients were domestic shorthair cats (five male, three female). The median age at the time of surgery was 9 years (range 3–15). Five cats experienced a luxation of the right elbow, while the remainder had a luxation of the left elbow. Except for one patient that presented in shock, all patients presented with acute onset of unilateral thoracic limb lameness. A traumatic incident was observed by the owner in four cats and suspected in the remainder. Seven cats presented with a lameness grade of 3 out of 3. Lameness was not assessed on admission in the cat that presented in shock. Joint pain, swelling and crepitus were present in all cases. The neurological examination showed the presence of a withdrawal reflex and deep pain sensation in all cats. Two cases were initially managed by the referring veterinarian, who performed a closed reduction and applied a spica splint. One case presented with concomitant moderate caudal shoulder instability on the same limb. The owners chose not to pursue shoulder surgery. Lateral elbow luxation was encountered in five cases, while medial elbow luxation was present in three. Degenerative osseous proliferation medial to the epicondyle, consistent with chronic medial epicondylitis, was encountered in three cases (Figure 1). These three cases were the ones that had medial luxation. One case of the eight presented with a fragment consistent with the sesamoid bone within the supinator muscle. Marked degenerative arthropathy was present in three cases and absent in the remainder.
Overview of the study design
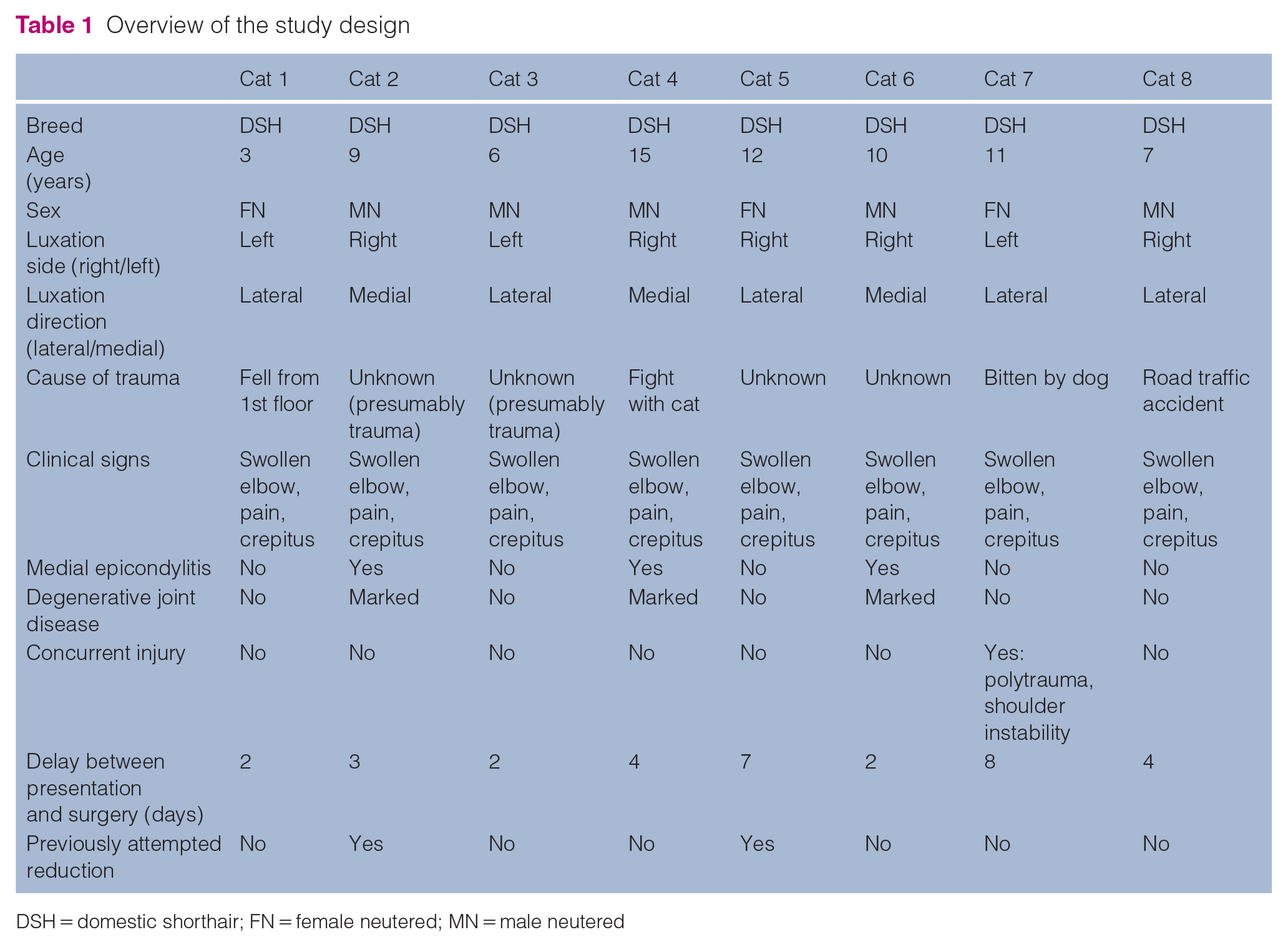
DSH = domestic shorthair; FN = female neutered; MN = male neutered
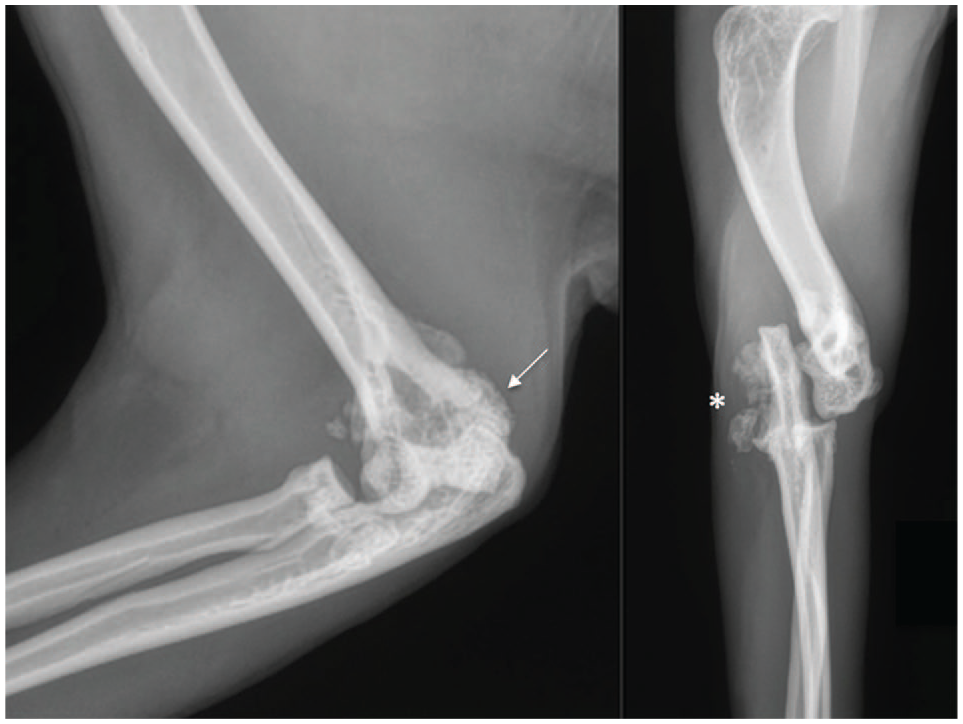
Lateral (a) and craniocaudal (b) radiographs of a complete medial luxation of both radius and ulna relative to the humerus, with a preserved radioulnar joint. Marked smooth and regular new bone formation with associated variably sized small rounded mineral structures is visible at the medial aspect of the ulna and elbow joint (asterisk). Chronic remodelling of the distal humerus with new bone formation at the caudal aspect of the medial epicondyle is also noted (arrow). All these findings are consistent with medial elbow luxation with marked degenerative joint disease and associated medial epicondylitis
Surgery and postoperative care
A closed reduction of the elbow luxation was performed in all cats. Rotatory stability of the affected elbows was deemed abnormal in comparison with the contralateral elbow in all cats. The ESF was inserted percutaneously and without any complications in all patients (Figure 2).

Immediate postoperative lateral (a) and craniocaudal (b) images of the transarticular type II external skeletal fixator with fixation clamps
Before recovery from anaesthesia, the fixation clamps were covered with adhesive tapes to prevent trauma from the pins’ sharp edges. Postoperative radiographs revealed satisfactory elbow reduction and alignment with accurate implant placement (Figure 3). All patients were discharged from the hospital the day after the surgery.
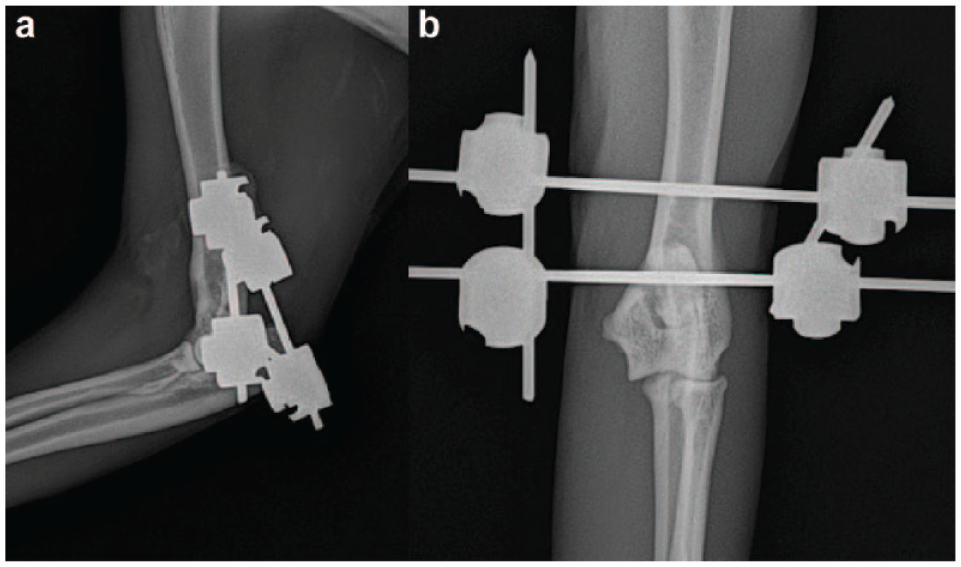
Postoperative (a) lateral and (b) craniocaudal radiographs reveal elbow luxation reduction. Anatomic relationships between the radius, ulna and humerus have been restored
Follow-up
At the 2-week postoperative assessment, very minimal translation movement of the pins was noticed. Neither pin migration nor breakage was observed. All connecting bars were removed under sedation. Clinical evaluation of collateral ligament integrity by Campbell’s test 19 was deemed to be normal in comparison with the contralateral elbow. The ROM for elbow flexion and extension was satisfactory but slightly diminished in all patients. After removal of the ESF, radiographs showed no elbow reluxation, mild soft tissue swelling and the presence of drill holes. The pins’ entry sites looked satisfactory in all cases except two, in which moderate drainage was present. Local disinfections using 0.05% chlorhexidine solution twice daily for 5 days was recommended. The wounds subsequently healed uneventfully through second intention.
Follow-up at 6 weeks postoperatively revealed a grade 1 lameness in one cat and grade 0 in the remainder. The grade 1 lameness was observed in the cat that presented with moderate shoulder instability and discomfort was identified as originating in the shoulder upon clinical examination. Campbell’s test 19 and ROM was considered normal in all cats. None of the cats exhibited pain upon manipulation of the elbow. Resuming a normal level of activity was advised for all cats.
The long-term follow-up consisted of a telephone interview with the owners of seven cats and a clinical evaluation in one cat. All owners contacted by telephone were very satisfied with the outcome after surgery and did not perceive a negative impact on their pet’s quality of life. All cats regained their normal activity (running, jumping, walking) and lameness was not noted. Time elapsed since surgery ranged from 23 to 69 months. One cat had a clinical evaluation 7 months postoperatively. The cat showed an intermittent grade 1 lameness. This was the cat that presented with concurrent moderate shoulder instability. It had a normal ROM of the elbow, no pain/crepitus upon elbow manipulation, and continued to exhibit moderate shoulder instability and associated discomfort.
Complications
Minor complications were observed in two cases. A small wound (<1 cm) was observed at the site of the medial entry of the proximal pin in these two cases. The wound healed within 5 days with topical treatment after removal of the ESF. No major complications associated with the ESF and no reluxation were reported in any of the cats.
Discussion
The application of a temporary type II ESF after closed reduction resulted in no recurrence of luxation among the eight cats involved in this study. Restoration of elbow ROM was achieved, and minimal postoperative complications were observed. To the authors’ knowledge, this is the first case series reporting the use of a temporary rigid transarticular external fixator as a sole method of stabilisation for elbow luxation in cats.
Elbow luxation is an uncommon injury in cats. 5 Approximately 65% of elbow luxations are reported to be lateral, which may be partially explained by a weaker medial collateral ligament.5,25 The current findings align with this observation, demonstrating a higher prevalence of lateral displacement, with 5/8 cases displaying lateral luxation; however, this may be biased by the small sample size in the study.
The three-point lameness grading system described by Montavon et al. 6 was chosen because of its simplicity and its approved use in cats. At the long-term follow-up, one cat exhibited grade 1 lameness during its clinical evaluation. The lameness was attributed to shoulder instability, which was managed conservatively. Although it can be an incidental finding, medial humeral epicondylitis can be another source of forelimb lameness in cats, resulting from avulsion and calcification of the antebrachial flexor tendons at their insertion site on the medial epicondyle of the humerus. 29 The precise cause of medial humeral epicondylitis in cats remains unknown, but is conjectured to be associated with either a traumatic event or an overuse of the limb, which can result in partial or complete avulsion of the flexor muscles.6,29 While epicondylitis has been presumed to be associated with subluxation of the humeroulnar and humeroradial joints, no direct link between epicondylitis and medial elbow luxation has been established. It is interesting to note that all cases of medial luxation in the present series exhibited radiographic signs of medial humeral epicondylitis as well as marked changes indicative of degenerative joint disease. Conversely, cats experiencing lateral luxation showed no such changes.
It has been reported that external coaptation (such as a Robert-Jones bandage, light bandage, spica splint and orthoses)2,4,14,16,17,30 is an alternative to transarticular ESF in limiting elbow joint movement. 24 Although external coaptation is thought to increase support after closed reduction, its efficacy in preventing elbow luxation recurrence has been questioned in dogs. 12 Furthermore, coaptation-related soft tissue injuries should not be neglected as they can cause significant morbidity and increased treatment costs. 31 In a series of 32 cats with elbow luxation, closed reduction was the treatment approach in seven cases, while surgery was pursued in 25 cases. 5 Eight cases benefited from external coaptation and one of the eight suffered coaptation-related soft tissue complications. 5 In the same study, reluxation of the elbow joint occurred more frequently after closed reduction with/without external coaptation than after open reduction and external fixation. 5 The authors of the present study believe that external coaptation is not well tolerated by cats, and this is supported by the aforementioned study. 5 In the present study, the elbow luxations were acute and amenable to closed reduction. It is possible that this technique may not be appropriate in chronic cases.
In this study, the authors used the technique initially described by Vedrine 24 but preferred a rigid transarticular ESF over an elastic transarticular ESF. In the authors’ experience, elastic bands can easily break and wounds are frequent as a result of friction between rubber plugs and the skin. Placement of the elastic bands is often tedious and ideal tensioning is unknown. It is generally advised to maintain the ESF for a period of 4–8 weeks to ensure joint stabilisation and support the healing of associated orthopaedic issues.32–34 However, extended use of the ESF can lead to complications such as joint stiffness, muscle atrophy and a reduction in joint ROM.2,13 Prolonged immobilisation may also result in decreased synovial fluid production, cartilage degeneration and, ultimately, degenerative joint disease. 35 Vedrine 24 suggested an immobilisation period of 2 weeks to mitigate these risks. Moreover, an ESF removed 28 days postoperatively in this study resulted in elbow ankylosis. 24 Despite the absence of reluxation, the occurrence of ankylosis prompted a reconsideration towards earlier ESF removal. 24 Following these insights, the present authors opted for a 14-day ESF application period. After ESF removal, and from a clinical perspective, ROM was quickly restored. This could be related to the fact that the pins were applied via a closed approach, thus creating minimal tissue damage.
Threaded pins have superior holding power compared with smooth pins. 36 The authors could have encountered translation of the ESF when using unthreaded pins but the decision to use unthreaded pins was based on the short-lived nature of the construct. Very minimal translation movement of the pins was noticed at the follow-up examination. Neither pin migration nor breakage was observed.
In cats, recurrence of elbow luxation is a frequent complication, encountered in 61% of cases after primary closed reduction; however, it is not encountered in cases treated with open surgical reduction techniques. 5 In the present series, no reluxation occurred after closed reduction in conjunction with a temporary ESF. This could be explained by the restriction of ROM induced by the transarticular constructs. Reported factors affecting reluxation rate include the luxation’s chronicity and the muscle contraction that can complicate the reduction. 30 In this series, all cases were acute luxations.
This study has several limitations, including its retrospective design, the small sample size and the absence of objective measures, such as a goniometer or gait analysis. A prospective larger feline series would be of great interest but might be difficult to complete considering the rarity of the condition.
Conclusions
The use of closed reduction in combination with a temporary transarticular type II ESF may offer an alternative to open surgical techniques for treating elbow luxation in cats and none of the eight animals reported herein experienced elbow reluxation. This technique carries excellent short-term clinical and long-term owner-assessed outcomes. Medial humeral epicondylitis may be a predisposing factor to medial elbow luxation.
Supplemental Material
sj-docx-1-jfm-10.1177_1098612X241265054 – Supplemental material for Outcome of traumatic elbow luxation managed with temporary transarticular external skeletal fixation in eight cats
Elbow luxation cat study telephone interview protocol.
Footnotes
Supplementary material
The following file is available as supplementary material:
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animals described in this work (experimental or non-experimental animals, including cadavers) for all procedures undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.