
Abstract
Objectives
The aim of this study was to develop guidelines for the optimal location of drill entry and exit points for insertion of a transcondylar screw across the feline humeral condyle.
Methods
Multiplanar reconstruction of feline elbow CT scans performed between 2016 and 2021 at one referral institution were reviewed. The optimum medial and lateral epicondylar entry and exit points for transcondylar screw placement were determined. These values were normalised to the humeral condylar diameter (HCD) for each elbow to determine the transcondylar screw placement guidelines. These guidelines were applied to each elbow and tolerance angles were determined in the transverse and frontal plane CT images to determine the safe corridor for screw placement.
Results
Twenty elbows from 12 cats were evaluated in this study. The guidelines for transcondylar screw placement were as follows: the medial entry/exit point was 0.38 × HCD cranial and 0.16 × HCD distal to the medial epicondyle, and the lateral entry/exit point was 0.3 × HCD cranial and 0.16 × HCD distal to the lateral epicondyle. Tolerance angles were statistically significantly (P <0.05) larger in both frontal (34.5% larger) and transverse (21.1% larger) planes when drilled from a lateral to medial direction compared with drilling from a medial to lateral direction.
Conclusions and relevance
The guidelines determined from this study may aid clinicians in the placement of humeral transcondylar screws in cats. Where possible, drilling from a lateral to medial direction is recommended owing to the higher tolerance angles reducing the likelihood of articular surface damage. Further studies are warranted to determine whether these guidelines are clinically useful and result in the safe insertion of a transcondylar screw in the clinical setting.
Introduction
Distal humeral condylar fractures, including lateral, medial or bicondylar Y-T fractures, are rare in cats.1,2 Differences in the anatomy of the feline distal humerus have been proposed to be one reason for the low frequency of distal humeral fractures.2,3 Cats lack the perforated olecranon fossa and have straighter and wider epicondylar ridges, which have been proposed to offer greater resistance to fracture. 3 Compared with dogs, which can suffer relatively low-energy humeral condylar fractures, 4 feline condylar fractures are mainly reported following significant trauma, including road traffic accidents or falls from a height.1,5
Comminuted distal humeral fractures have been reported in cats following high-energy trauma. 1 Oblique condylar fractures, with no history of trauma, have been reported in cats with patellar fracture and dental anomaly syndrome, and are thought to be a form of insufficiency fracture. 6 A lateral condylar fracture has also been reported secondary to an intracondylar fissure in a cat with no history of trauma. 7
Similar to dogs, condylar and Y-T fractures are complex articular fractures requiring accurate anatomical reduction. 1 The limited amount of bone in the humeral condyle (HC) makes fracture repair particularly challenging in a cat. Methods of repair include internal fixation with the use of unilateral or bilateral locking plates with a transcondylar screw placed in lag fashion.1,5 Other methods of repair include placement of a transcondylar screw with Kirshner wire or locking plates to stabilise the supracondylar fracture fragment. The use of external skeletal fixators8,9 or transarticular linear-circular (hybrid) external skeletal fixators have also been reported. 10
Landmarks for the safe insertion of a transcondylar screw across the humeral condyle have been reported in dogs. 11 To our knowledge, definitive calculated landmarks for inserting a transcondylar screw across the feline HC have not been described previously. Considering that the feline distal HC is quite different from that of the dog, the aim of this study was to determine safe corridors for placement of a transcondylar implant in the feline HC.
Materials and methods
The Institutional Animal Care and Use Committee guidelines were followed. At the time of the investigations, informed written and verbal consent were obtained from each owner. CTs of cats that had clinical investigations unrelated to this study which included the elbow from 2016 to 2021 were evaluated. If cats had a CT scan for elbow pathology of one limb, the normal contralateral elbow was used. The elbows were reconstructed using a bone algorithm for assessment and measurements. Cats were excluded if there was elbow pathology present. All CT scans were performed under sedation or general anaesthesia. Prior to May 2018 a 16-slice multidetector row unit CT scanner (M×8000 IDT; Philips Healthcare) was used; for CTs performed after May 2018 a 320-slice multidetector row unit CT scanner was used (Aquilion ONE, Genesis Edition; Canon Medical Systems). Slice thickness ranged from 0.5 mm to 0.8 mm. Multiplanar three-dimensional reconstructions (MPR) and measurements were performed on one computer using a medical image viewing software (Horos [Horos Project; Nimble]). All measurements were performed by one reviewer. All measurements were recorded to one-tenth of a millimetre. Study measurements were extrapolated from a previous canine study. 11
Image orientation
MPR images were oriented as follows: the frontal plane was aligned such that the proximal MPR line was positioned in the centre of the humeral medullary canal parallel to the lateral and medial humeral diaphyseal cortical borders. The transverse plane was oriented perpendicular to the frontal plane and parallel to a line drawn between the two epicondyles. The sagittal plane image was initially oriented so that the proximal MPR line was in the centre of the humeral medullary canal and followed the same angulation of the humerus proximally. Once the correct proximal angulation of the humerus was achieved, the intersection of the MPR lines was positioned in the centre of the humeral condylar isthmus at its smallest diameter.
Measurements
Calibrated measurements were in millimetres. The smallest diameter of the HC was determined using the sagittal MPR images and the diameter at the isthmus was measured in a cranial to caudal direction (Figure 1). The epicondylar width was measured from the medial epicondyle (ME) to the lateral epicondyle (LE) in the transverse plane images.

Sagittal multiplanar reconstruction image of the feline elbow. The smallest diameter of the humeral condyle was identified. The humeral condylar diameter (HCD) at the isthmus was measured and recorded
The optimal drill line (ODL) for placement of a transcondylar screw was established on the MPR images using the MPR reference lines (Figure 2). The MPR lines, mimicking the line for placement of a transcondylar screw, were oriented so that the screw would pass through the centre of the HC isthmus at its smallest diameter in the sagittal plane. In the transverse plane, the line was placed so that it was at an equal distance between the epicondyles. In the frontal plane, the line was placed so that it was at an equal distance between the epicondyles. Once the MPR reference lines were placed in the optimum position for screw placement, the sagittal images were reviewed (Figure 3). The ME, at its most abaxial point, was identified in the sagittal plane and the distance cranially and distally between the ME and the ODL was recorded in millimetres. This was defined as the ME entry point and expressed as a cranial and distal measurement. This was repeated for the LE, and the LE entry point was recorded as cranial and distal measurements to the ODL.

CT multiplanar reconstruction images showing the correct image orientation for the (a) frontal, (b) transverse and (c) sagittal planes, and position of the optimal drill line (ODL)
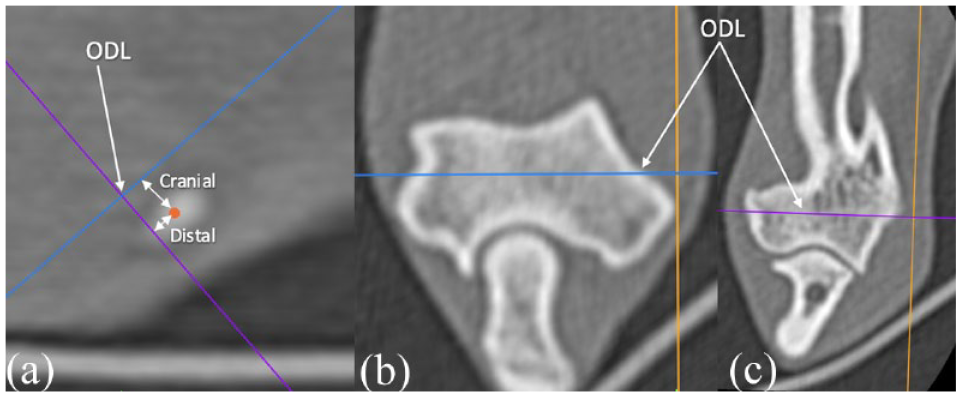
CT multiplanar reconstruction images showing (a) sagittal, (b) transverse and (c) frontal plane images depicting how the medial entry/exit point was determined. The medial epicondyle (orange dot) was identified in the sagittal plane and the cranial and distal measurements to the optimal drill line (ODL) were measured. This was then repeated for the lateral epicondyle to determine the lateral entry/exit point.
To correct for the variation in size between individual elbows, the ME and LE entry point values were normalised. To normalise the cranial and distal measurements of the ME and LE entry points, they were individually divided by the respective humeral condylar diameter (HCD) for that elbow. The means of the cranial and distal ME entry points and LE entry points were calculated to provide guidelines for optimum screw entry/exit points.
The guidelines for the ODL were applied to each elbow to evaluate whether safe insertion of a transcondylar screw would be achieved. The MPR images were oriented as previously described. The ME and LE entry points were individually measured from their respective epicondyles and a mark was placed at this point. The MPR reference lines were oriented so that they would intersect both of these ME and LE entry points in the frontal and transverse planes. This line was called the calculated drill line (CDL).
Safe corridor determination
To define a safe corridor for screw placement, tolerance angles were calculated from the CDL in the frontal and transverse planes (Figure 4). A tolerance angle was defined as the angle between the medial or lateral entry point, the exit point (opposite aspect of the HC) and the first boundary point encountered. For a feline transcondylar screw, it was assumed the smallest screw placed would be 2.0 mm or 2.4 mm. A distance of 1.5 mm from the cranial, caudal, proximal and distal boundaries of the HC in the transverse and frontal planes was used as the boundary margin. This value (1.5 mm) was chosen as the CDL is the location of the centre of the screw and a 2.4 mm screw has a radius of 1.2 mm. The boundary points in the frontal and transverse plane are shown in Figure 4 and are the same as described in the study by Barnes et al. 11 The angle between the CDL and a line drawn cranially from the ME entry point to where this line touched the first boundary point was calculated, and was termed the medial cranial tolerance angle. This was repeated caudally, to define the medial caudal tolerance angle. The medial craniocaudal tolerance angle was calculated by adding the cranial and caudal values. The cranial and caudal lateral tolerance angles were calculated. This was repeated on the frontal plane images to calculate the medial proximal, medial distal, lateral proximal and lateral distal tolerance angles. The medial and lateral proximo-distal tolerance angles were calculated.

Frontal and transverse plane multiplanar reconstruction images showing (a) the medial craniocaudal tolerance angle in the transverse plane and (b) the medial proximo-distal tolerance angle in the frontal plane image. The yellow lines mark the boundary points of the humeral condyle, each 1.5 mm. The black line represents the calculated drill line. The medial cranial tolerance angle (1), medial caudal tolerance angle (2), medial proximal tolerance angle and medial distal tolerance angle (4) are indicated. M = medial; L = lateral
Data analysis
Descriptive statistics were used to describe median HCD and the normalised ME and LE entry points. To compare the tolerance angles of the elbows, paired t-tests were performed using a computer-based statistical software (Microsoft Excel 2021). Significance was set at P ⩽0.05.
Results
CTs of 20 elbows from 12 cats were included in this study. Breeds included domestic shorthair (n = 6), Maine Coon (n = 2), domestic longhair (n = 1), British Shorthair (n = 1), Exotic Shorthair (n = 1) and Chartreux (n = 1). Median age was 6.5 years (range 1.0–15.0). Six cats were male neutered and six were female neutered. Median weight was 4.8 kg (range 2.0–7.1). Seven cats were sedated and five cats had general anaesthesia to acquire the CT.
Four cats had a bilateral elbow CT scan performed owing to unilateral orthopaedic disease of the forelimb, including elbow osteoarthritis (OA), distal ulnar lesion, metacarpal lesion and a forelimb digit lesion. In the remaining cats, elbows were included in a CT scan of the thorax for non-orthopaedic disease for reasons such as screening for metastasis (n = 3), respiratory and gastrointestinal investigations (n = 4), and following a road traffic accident (n = 1).
Elbow measurements
Median HCD was 6.0 mm (range 5.1–6.9). The median epicondylar width was 18.0 mm (range 17.1–20.9). The mean normalised ME entry point in a cranial direction was 0.38 × HCD; in a distal direction it was 0.16 × HCD. Mean normalised LE entry point was 0.30 × HCD in a cranial direction and 0.16 × HCD in a distal direction. Based on these normalised medial and lateral epicondylar entry points, guidelines were created for the optimal location of the drill entry and exit points. The medial entry/exit point was 0.38 × HCD cranial and 0.16 × HCD distal to the ME. The lateral entry/exit point was 0.3 × HCD cranial and 0.16 × HCD distal to the LE. These guidelines were used to plot the ODL on the elbows when calculating for tolerance angles. No ODL crossed the boundary points of the HC in the transverse or frontal planes when applied to all elbows. The cranial and caudal tolerance angles measured from the medial and lateral entry points in the transverse plane and the proximal and distal tolerance angles in the frontal plane are shown in Table 1.
Medial and lateral tolerance angles in the frontal and transverse planes defining the safe corridor for transcondylar screw placement

Discussion
Tolerance angles were statistically significantly (P <0.05) larger in both frontal (34.5% larger) and transverse (21.1% larger) planes when drilled from a lateral to medial direction compared with drilling from a medial to lateral direction. This is in contrast to the canine elbow, where the tolerance angles were significantly larger when drilled in a lateral to medial direction in the frontal plane but not in the transverse plane. 11 The authors of that study attributed the significant difference in drilling from lateral to medial to the different geometry of the medial and lateral aspects of the HC. In the dog, the geometry of the lateral part of the HC is similar in size to the humeral isthmus, with the medial aspect of the condyle being much larger, allowing more tolerance for changes in angulation when drilling from lateral to medial. The difference in tolerance angles in the transverse plane in this study could be due to the cat having more similarly sized humeral medial and lateral aspects of the condyle compared with the dog. 3
In the clinical setting, the medial and lateral epicondylar landmarks could be obscured by development of OA. The prevalence of OA in cats aged ⩾6 years is 61%. 12 Eight cats in this study were aged >6 years and five were aged >10 years; the guidelines resulted in safe virtual insertion of a transcondylar screw in all elbows. However, these cases were selected based on having no elbow pathology and may not represent the general cat population. Furthermore, medial humeral epicondylitis has been reported in 10% of cats in one cadaveric study. 13 It could be proposed that insertion of a transcondylar screw using the guidelines proposed in this study in cats with OA or medial humeral epicondylitis may pose a challenge or may not be possible.
Our results show that tolerance angles were significantly larger when drilled from a lateral to medial direction. In dogs, when treating humeral intracondylar fissures, it is recommended that a transcondylar screw that is 30–50% of the HC diameter is placed. 14 The mean HCD in this study was 6 mm. Therefore, a 2.0 mm or 2.4 mm screw would be the most appropriate for placement as a transcondylar screw in this group of cats. With the boundary points in the frontal and transverse planes being 1.5 mm, 0.3 mm more than half the diameter of a 2.4 mm screw, our results show that a 2.4 mm screw can, in a virtual setting, be safely inserted across the feline HC. A 2.7 mm screw has been placed in previously reported cases. 1 The guidelines developed in this study would also result in safe insertion of this screw across the HC. However, a larger screw would result in a smaller tolerance angle and greater risk of complications such as intra-articular placement.
The direction of drilling for a transcondylar screw will depend on the fracture configuration and surgeon preference. For the treatment of humeral intracondylar fissures in dogs, beginning the transcondylar screw insertion from both lateral and medial have been reported, with lateral-to-medial drilling being the most commonly reported.15,16 Both insertion directions have been associated with high complication rates: 59.4% with lateral-to-medial drilling 15 and 57% with medial-to-lateral drilling. 16 However, the true complication rate for transcondylar screw placement in cats is unknown.
The previous study defining the safe corridor for insertion of a canine transcondylar screw also showed that the HCD diameter measured from a mediolateral radiograph correlated well with the HCD measured from a sagittal CT image. 11 It was our initial aim to determine whether this would be the case for the feline elbow; however, only one of the cases had an appropriate mediolateral radiograph and so this was not possible. This is a limitation of this paper, as in the clinical setting, although dependent on the fracture complexity, a clinician is more likely to base surgical planning on preoperative radiographs than a CT scan.
In a clinical setting, aiming devices and fluoroscopic guidance can be used to improve the accuracy of screw placement. Recently, computer-aided design (CAD) software has been used in an attempt to improve accuracy in planning and executing surgical procedures.17,18 The use of three-dimensionally printed patient-specific drill guides for placement of a canine transcondylar screw were recently reported. 18 It resulted in accurate and consistent placement of a transcondylar screw. CAD software and the use of patient-specific drill guides, along with these guidelines, may aid clinicians in placement of a feline transcondylar screw. However, these steps add cost and time to the procedure and potentially delay surgery, whereas the methodology described in this study is readily adoptable.
One of the major limitations of this study was the small sample size. A limited number of cats specifically had elbow CT scans and a limited number of these did not have elbow pathology, or had been incidentally included in a thoracic study. Therefore, inherently, there was also some variation in the CT scanning protocol slice thickness and positioning. Owing to the scarcity of feline elbow CT scans at our institution, both elbows from a single cat were included in the study if they were both scanned and clinically normal. Ideally, we would have used a different animal for each elbow; however, the very small variation in geometry between different cats indicates that the geometry of the feline elbow is consistent and hence that this is a reasonable approach. The measurements of this study were recorded to one-tenth of a millimetre; however, there are inherent errors in measurements and intra- and interobserver variations are likely. However, in the context of surgery, the variations are likely to be insignificant compared with surgical error. Repeatability of the measurements obtained could also have been assessed. Additionally, the entry/exit points located on CT may not be repeatable in the clinical setting. Finally, one cat in the study had its CT scan performed on a 16-slice CT scanner whereas the remainder were taken using a 320-slice CT scanner. All cats were at least 1 year old and therefore these guidelines may not be appropriate for juvenile cats.
Conclusion
This study established guidelines for the safe insertion of a transcondylar screw across the feline HC, resulting in safe virtual placement of a transcondylar screw across the feline elbow based on multiplanar CT images. The medial entry or exit point should be located at a distance in millimetres of 0.38 × HCD cranially and 0.16 × HCD distally from the ME. The lateral entry or exit point should be located 0.3 × HCD cranially and 0.16 × HCD distally from the LE. Tolerance angles were significantly larger when drilling in a lateral to medial direction. Further studies are warranted to determine whether these guidelines are clinically useful and result in the safe insertion of a transcondylar screw in the clinical setting.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.