
Abstract
Background
Although proton pump inhibitors are the mainstay of gastroesophageal reflux disease treatment, up to 30% of patients have a poor symptomatic response. Ambulatory pH impedance monitoring is the gold standard to assess whether this is due to persistent acid reflux. We aimed to characterize clinical predictors of persistent esophageal acid reflux on proton pump inhibitors including gastric pH measured during endoscopy.
Methods
We prospectively recruited patients with gastroesophageal reflux disease and/or Barrett esophagus on proton pump inhibitors. All patients completed a symptom questionnaire and underwent gastroscopy with gastric pH analysis, immediately followed by ambulatory 24-hour pH impedance. We used a modified cutoff of 1.3% for pathological esophageal acid exposure time. A multiple linear regression model was used to analyze the correlation between acid exposure time and predictive variables.
Results
We recruited 122 patients, of whom 92 (75.4%) were included in the final analysis (44 male (47.8%), median age 53 years (interquartile range (IQR): 43–66)). Forty-four patients (47.8%) had persistent acid reflux with a median total acid exposure time of 2.2% (IQR: 1.2–5.0), compared with 0.1% (IQR: 0.0–0.2) in patients without persistent reflux (n = 48; p < .001). There was no difference in age, sex, body mass index, proton pump inhibitor regimen, diagnosis of hiatus hernia or Barrett esophagus, and severity of symptoms between patients with normal and abnormal acid exposure time. Median gastric pH was significantly lower in patients with persistent acid reflux (5.8 vs 6.6, p = .032) and it correlated with the total acid exposure time (p = .045; R2 = 12.0%). With a pH cutoff of 5.05, single-point endoscopic gastric pH analysis had an area under the receiver operating characteristic curve of 63.0% (95% confidence interval: 51.3–74.7) for prediction of persistent acid reflux.
Conclusions
Symptoms and clinical characteristics are not useful to predict persistent acid reflux in patients on proton pump inhibitors. One-point gastric pH correlates with 24-hour esophageal acid exposure time and could guide clinicians to assess treatment response; however, its utility needs validation in larger studies.
Key summary
Up to one-third of patients with gastroesophageal reflux disease treated with proton pump inhibitors (PPIs) have poor symptomatic control, which could be due to persistent acid reflux or organ hypersensitivity to nonacid reflux. It is unclear whether clinical parameters at the time of the diagnostic endoscopy can guide in the diagnostic pathway. An ambulatory pH-impedance monitoring test is useful to distinguish between persistent acid reflux and esophageal hypersensitivity. Conventional clinical characteristics, including severity of symptoms, are not useful to predict persistent acid reflux in patients on PPIs. One-point gastric pH measured during endoscopy by EndoFaster correlates with total esophageal acid exposure time in a 24-hour pH-impedance test, with an area under the receiver operating characteristic curve of 63% for pathological esophageal acid exposure. Gastric pH measured with EndoFaster, in association with clinical assessment, can inform about suboptimal pharmacological response to PPIs and help triage patients for a pH-impedance test.
Introduction
Gastroesophageal reflux disease (GERD) develops when the reflux of stomach contents into the esophagus causes troublesome symptoms, esophageal mucosal injury, or both. 1 It is postulated that typical GERD symptoms, including heartburn and/or regurgitation, affect nearly 30% of the general population in the Western world. 2 The diagnosis of GERD is made in the presence of characteristic esophageal symptoms and can be corroborated by diagnostic tests demonstrating typical esophageal mucosal injury (endoscopy) or reflux of stomach contents (ambulatory pH-impedance monitoring). 3 Proton-pump inhibitors (PPIs) are the most commonly used drugs in GERD medical treatment. 4 These agents selectively inhibit the hydrogen/potassium adenosinetriphosphatase in gastric parietal cells, suppressing acid production. 4 However, in up to 30% of patients there is lack of or incomplete clinical response. 5 The mechanisms behind this are not fully understood, although esophageal hypersensitivity to weakly acidic or nonacidic reflux could be a potential cause. Esophageal pH monitoring is commonly performed during therapy in PPI-refractory GERD patients to assess persistent acid reflux and differentiate persistent GERD from functional disorders. This test, however, requires placement of a transnasal catheter for a 24-hour period and two additional hospital visits, which makes it inconvenient and often uncomfortable for the patients. It is unclear whether standard clinical and endoscopic findings, with the exception of the presence of esophagitis, can be reliable predictors of persistent esophageal acid exposure in patients on PPI therapy. Because PPIs suppress acid production in the stomach, real-time measurement of gastric pH could provide an objective measure of pharmacological response in patients on PPIs undergoing endoscopy.
EndoFaster (Niso BioMed, Italy) is a commercially available endoscopic adjunct device that is connected between the endoscope and the suction system within the endoscopy unit. It tests the gastric juice suctioned during a standard endoscopy, providing a real-time measure of the pH. The analysis of gastric pH has been used to aid in the diagnosis of gastric premalignant conditions, including atrophy, intestinal metaplasia and endocrine cell hyperplasia, which typically correlate with hypochloridia. 6 These conditions were found to be significantly correlated with the level of pH (r = 0.67; p < .01). 6 In patients on continued PPI therapy at the time of endoscopy, the gastric pH is expected to shift toward neutrality in case of good pharmacological response. Hence, we hypothesized that real-time EndoFaster measurement of gastric pH during gastroscopy, alone or in combination with other clinical parameters, could be useful to identify patients with incomplete pharmacological response to PPIs based on esophageal acid exposure time (AET) by the gold standard, ambulatory pH-impedance monitoring.
Methods
Study design
This was a prospective, single-center, cohort study conducted at the Addenbrooke’s Hospital (Cambridge, UK) between 2015 and 2018. This study proposal was approved by the ethical committee at the local institution (LREC01/149). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee. All patients provided written informed consent to participate in the study.
Patients
We prospectively recruited patients on PPI treatment referred for evaluation of GERD symptoms and/or surveillance of Barrett esophagus (BE) in the outpatient gastroenterology clinic. We included adult patients with or without symptoms on a stable PPI regimen for at least four weeks. Patients not compliant with the PPI treatment and those who missed the last scheduled dose of PPI prior to the endoscopy were excluded. Each patient completed a reflux disease questionnaire (RDQ) and underwent gastroscopy with gastric pH analysis and an ambulatory 24-hour pH-impedance monitoring test.
PPI regimens
For the purpose of the study, a PPI scoring system was established to group each patient into a group with a comparable PPI daily dose. The doses were established accordingly to the National Institute for Health and Care Excellence guidelines and the British National Formulary.
7
These groups included the following:
Group 1 (low dose): lansoprazole 15 mg/omeprazole 10 or 20 mg/pantoprazole 20 mg/esomeprazole 20 mg Group 2 (double dose): lansoprazole 30 mg/omeprazole 40 mg/pantoprazole 40 mg/esomeprazole 40 mg Group 3 (high dose): lansoprazole 60 mg/omeprazole 80 mg/pantoprazole 80 mg/esomeprazole 80 mg
RDQ
The RDQ is a self-administered, validated, 12-item diagnostic questionnaire used to evaluate the frequency and severity of the most common GERD symptoms. Each symptom, including heartburn, chest pain, regurgitation, acid taste and epigastric burning or pain, that has occurred over the last seven days was evaluated separately for its frequency and intensity by a six-point modified Likert scale. 8 For the purpose of the analysis, the median overall severity and frequency of the symptoms between 0 and 2 were defined as “no/minimal symptoms,” 3 to 4 as “moderate symptoms” and 5 to 6 as “severe symptoms.”
Endoscopy with EndoFaster analysis
Each patient underwent an upper gastrointestinal (GI) endoscopy with a high-definition endoscope (Olympus HQ260F) under conscious sedation (intravenous combination of midazolam and fentanyl) or local anesthetic (Xylocaine spray). Patient preparation was standardized with uniform fasting instructions that allow them to drink only a small amount of water not later than four hours before the endoscopic examination. Patients included in the study were examined at a similar time during the morning endoscopy session. During endoscopy, the presence of a hiatus hernia was assessed and the size was measured as the distance between the diaphragmatic pinch and the location of the gastroesophageal junction (GEJ), corresponding to the top of the gastric folds. Reflux esophagitis was graded according to the Los Angeles classification (LA grades A–D) 9 and BE, if present, was measured according to the Prague classification, as the circumferential and maximum extent of squamocolumnar junction (neo-Z-line) from the GEJ. 10 During inspection of the stomach, gastric juice was suctioned for the EndoFaster analysis (minimum 2.5 ml) to evaluate the gastric pH. In case of device malfunction leading to an inability to achieve a real-time measure of the pH (e.g. in the presence of food debris), a sample of the gastric juice was collected and stored for a short time. The pH was then measured at bedside either with the EndoFaster or a benchtop pH meter immediately after the endoscopic procedure. Patients with no gastric juice were excluded.
Twenty-four–hour pH impedance
Immediately after the endoscopy, an intraesophageal pH-impedance catheter (ZAN-BG-44, ComforTEC/pH, Sandhill) was placed transnasally. This catheter has two pH sensors. The esophageal pH sensor was placed 6 cm above the level of the endoscopically measured GEJ, whereas the distal pH sensor located 15 cm below the esophageal sensor allowed measurement of the gastric pH. To help position the esophageal pH sensor, we considered the difference in the level of the GEJ (+5 cm) between the transnasal and oral route, based on a previous randomized crossover study in which patients received both transnasal and conventional endoscopy. 11 Patients were given written and verbal instructions on body position recording, oral intake and symptom event marking during the 24-hour monitoring time via a Zephr Recorder (Sandhill). The timing of the symptoms was recorded by event markers. Sleuth Zephr software was used for analysis of the pH-impedance tracer by two physicians with experience in upper GI physiology (MdP and AH). Impedance was used to differentiate between anterograde and retrograde esophageal content movement and to identify true reflux events. Reflux events were distinguished in acidic and nonacidic with a pH cutoff of 4. The symptom index (SI) and symptom association probability (SAP) were evaluated. An SI greater than 50% and SAP greater than 95% (if there are more than three events) were considered positive. Because we postulated that the conventional cutoff of 4% could lead to underestimation of the residual acid reflux on PPI therapy, we used a modified validated cutoff for an on-PPI study of 1.3% for total 24-hour pathological AET in the esophagus (upright and supine), 1.5% in the upright position and 0.5% in the supine position. 12
Statistics
Quantitative variables were described as means and medians and SDs and interquartile ranges (IQRs), where appropriate. Categorical variables were presented as counts and percentages of the cohort. The two-sample Welch t test and Wilcoxon rank sum test were used to compare continuous variables, and the chi-square test was used to compare categorical data, where appropriate. The correlation between single-point gastric pH and 24-hour gastric AET was assessed using the Spearman method. Multiple linear regression models adjusted for clinical factors including age, sex, body mass index (BMI), PPI classifier, the presence of BE and hiatus hernia were used to analyze the association between single-point gastric pH and the 24-hour esophageal AETs. Receiver operating characteristic (ROC) curves and Fagan nomograms were used to present the accuracy of EndoFaster gastric pH measurement in predicting persistent acid reflux on PPIs. For all analyses, a p value of less than .05 was considered statistically significant. All analyses were performed using R Statistics version 3.4.3 (R Foundation for Statistical Computing, Vienna, Austria). Because this was a feasibility study, a formal power calculation was not possible.
Results
Patient characteristics
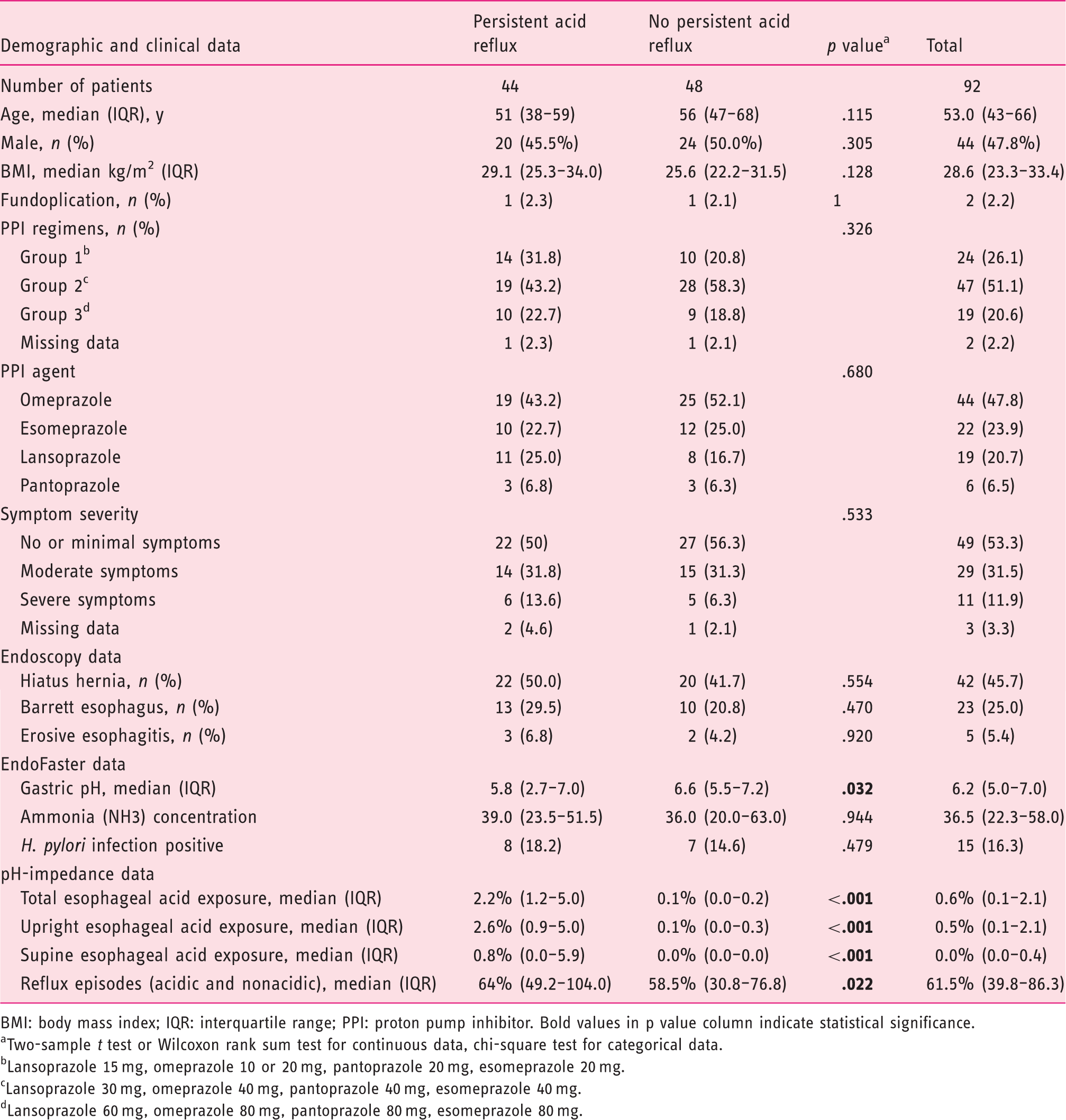
Of the 122 recruited patients, 30 were excluded because of no compliance with the PPI schedule (n = 7), EndoFaster technical failure or insufficient gastric juice for EndoFaster analysis (n = 17), intolerance to the pH-impedance catheter or pH-impedance technical failure (n = 6). The remaining 92 patients were included in the study; the study flowchart is presented in Figure 1. There were 44 men (47.8%) and 48 women (52.2%) with a median age of 53 years (IQR: 43–66) and a median BMI of 28.1 (IQR: 23.3–33.4). Forty-four patients (47.8%) had features of persistent acid reflux on 24-hour pH monitoring, and 48 patients (52.2%) had 24-hour esophageal AETs within normal limits. Patient characteristics are presented in Table 1. The median AETs (total, in upright and supine position) in patients with persistent acid reflux were 2.2% (IQR: 1.2–5.0), 2.6% (IQR: 0.9–5.0) and 0.8% (IQR: 0.0–5.9), respectively, and in patients without persistent acid reflux AETs were 0.1% (IQR: 0.0–0.2), 0.1% (IQR: 0.0–0.3) and 0.0% (IQR: 0.0–0.0), respectively (p < .001 for all comparisons). The median number of reflux episodes were 64 (IQR: 49.2–104.0) and 58.5 (IQR: 30.8–76.8), respectively, between both groups (p = .022). There were no differences in clinical characteristics between patients with and without persistent acid reflux, including age, sex, BMI, PPI regimen, the presence of a hiatus hernia and BE. Based on the results of 24-hour pH-impedance monitoring and clinical presentation, patients were further subdivided into four groups (Figure 1): (a) functional heartburn (moderate or severe symptoms in the presence of negative SI/SAP and normal AET, (b) esophageal hypersensitivity (moderate to severe symptoms, positive SI or SAP and normal AET), (c) GERD in remission (no or minimal symptoms and normal AET) and (d) persistent acid reflux (any symptom score and abnormal AET).
Study flowchart. *Three questionnaires missing. Patients’ characteristics. BMI: body mass index; IQR: interquartile range; PPI: proton pump inhibitor. Bold values in p value column indicate statistical significance. Two-sample t test or Wilcoxon rank sum test for continuous data, chi-square test for categorical data. Lansoprazole 15 mg, omeprazole 10 or 20 mg, pantoprazole 20 mg, esomeprazole 20 mg. Lansoprazole 30 mg, omeprazole 40 mg, pantoprazole 40 mg, esomeprazole 40 mg. dLansoprazole 60 mg, omeprazole 80 mg, pantoprazole 80 mg, esomeprazole 80 mg.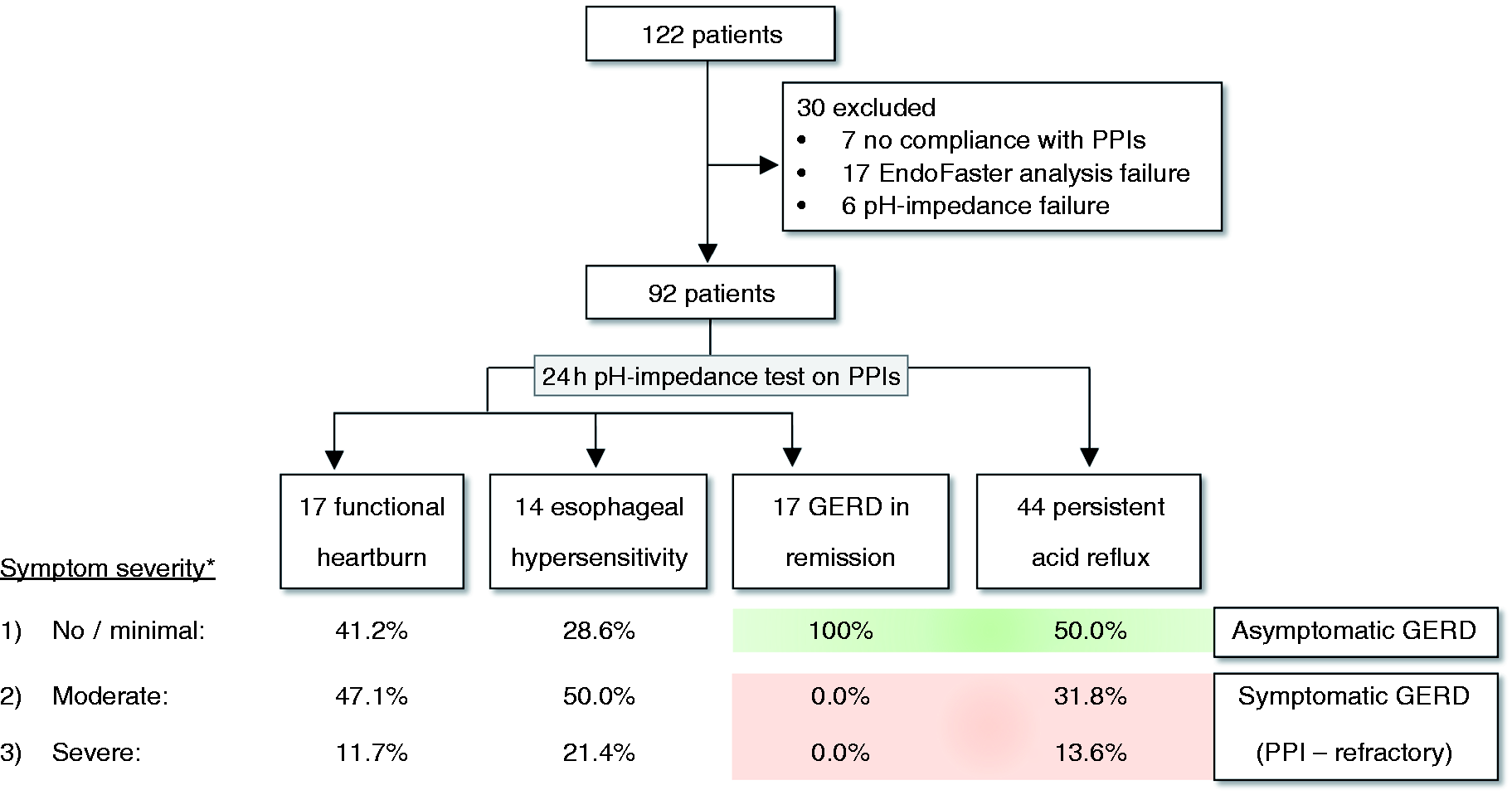
Symptoms
The overall median severity of symptoms in all patients with normal and abnormal AETs was 2.2 (IQR: 1.6–3.3) and 2.6 (IQR: 1.5–3.5), respectively (p = .526). Three patients had missing questionnaire scores. None of the six symptoms included in the RDQ questionnaire was predictive for persistent acid reflux in a multivariable logistic regression model (p = .797). The symptom scores for each group are presented in Supplementary Table 1. Also, we did not find a significant difference in the median symptom score among patients with esophageal hypersensitivity, functional heartburn and GERD with persistent acid reflux (Figure 2(a)). Patients with BE had a significantly lower median severity of symptoms compared with patients without BE (1.0 (IQR: 1.0–1.8) vs 2.5 (IQR: 1.0–4.0), p = .011), despite no difference in PPI regimens (p = .883) (Figure 2(b)). There was a trend for patients with higher symptom burden to have lower gastric pH, but this difference did not reach statistical significance. Namely, patients with no or minimal symptoms (n = 49), moderate symptoms (n = 29) and severe symptoms (n = 11) had a median gastric pH of 6.8 (IQR: 5.1–7.2), 6.1 (IQR: 4.5–7.0) and 5.6 (IQR: 5.3–6.8), respectively.
(a) Median severity of symptoms in esophageal hypersensitivity (EH), functional heartburn (FH) and gastroesophageal reflux disease with normal (GERD in remission) and abnormal (persistent acid reflux) esophageal acid exposure times. (b) Median severity of symptoms in patients with and without Barrett esophagus (BE).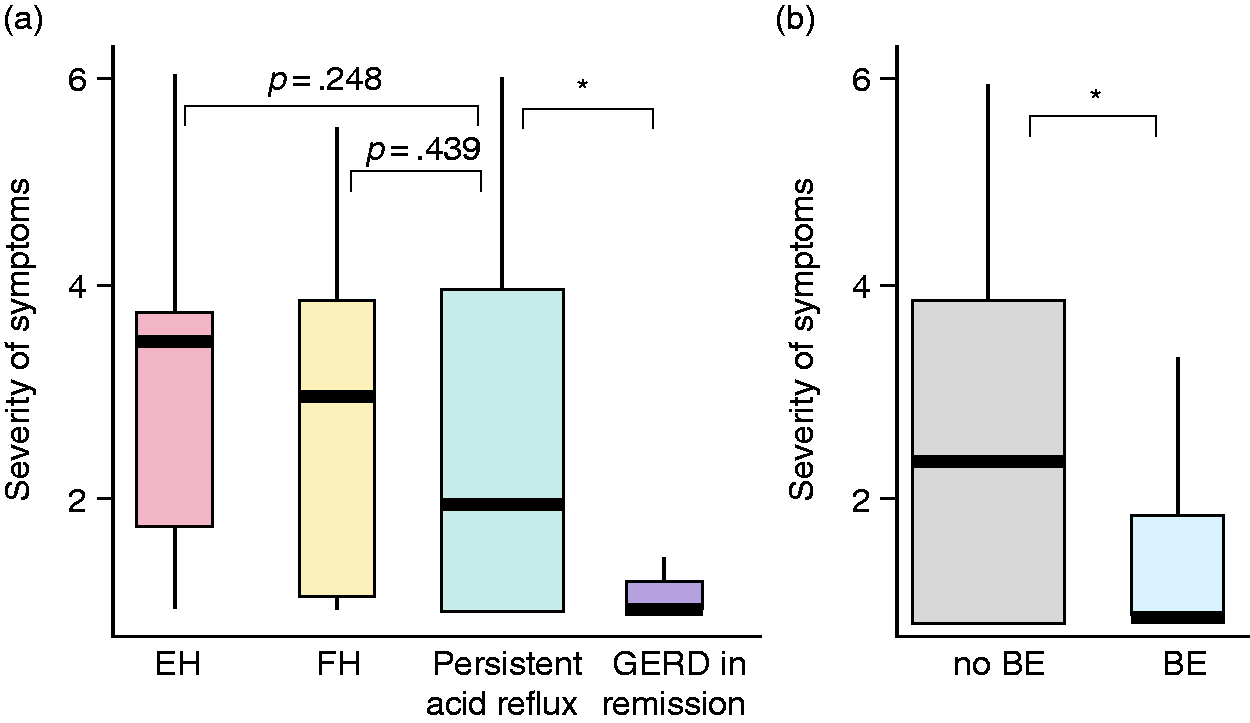
EndoFaster gastric pH and 24-hour pH impedance
First, using the Spearman method, we analyzed the correlation between one-point gastric pH measured by EndoFaster and the gastric acid exposure time (% of time pH < 4) measured by the gastric sensor during 24-hour pH-impedance monitoring. There was a statistically significant negative relationship between EndoFaster gastric pH and 24-hour gastric AET (r = −0.29, p = .004) (Figure 3).
Correlation between EndoFaster gastric pH and 24-hour gastric acidity measured by pH impedance, using the Spearman method.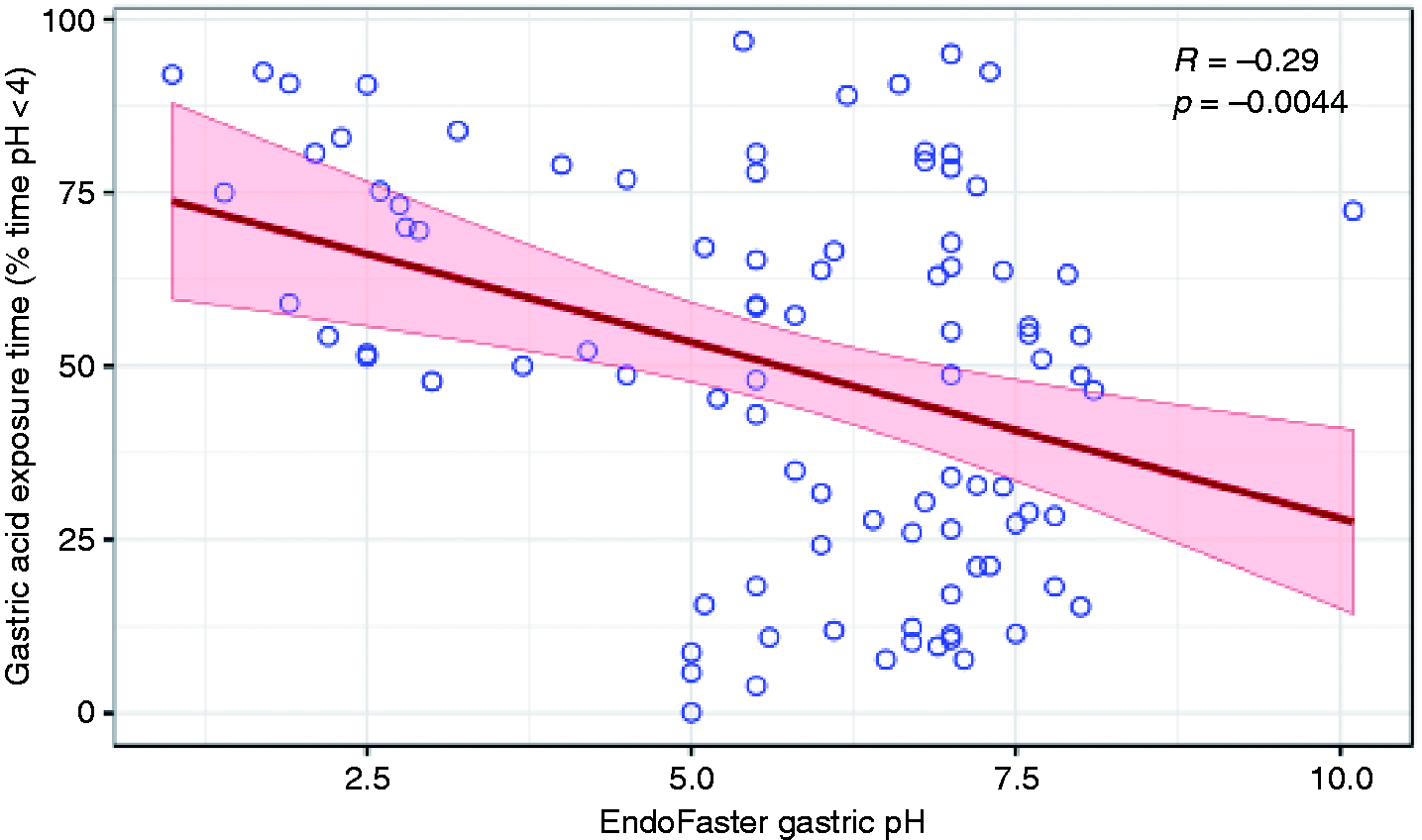
Second, we analyzed the relationship of single-point gastric pH and 24-hour total esophageal AET. We found a statistically significant difference (p = .032) between median values of gastric pH measured with EndoFaster between patients with pathological and normal AETs, which were 5.8 (IQR: 2.7–7.0) and 6.6 (IQR: 5.5–7.2), respectively (Figure 4). We therefore created a multivariable linear regression model adjusted for age, sex, BMI, PPI classifier, the presence of BE and hiatus hernia to predict AET. We found that EndoFaster gastric pH (beta = −0.9, p = .045), PPI classifier (beta = 2.5, p = .037) and presence of BE (beta = 5.6, p = .011) were significant predictors. The overall model fit, however, was only modest (adjusted R2 = 11.0%) (Supplementary Table 2).
EndoFaster gastric pH levels in patients with and without persistent acid reflux. *Statistically significant difference (p < .05).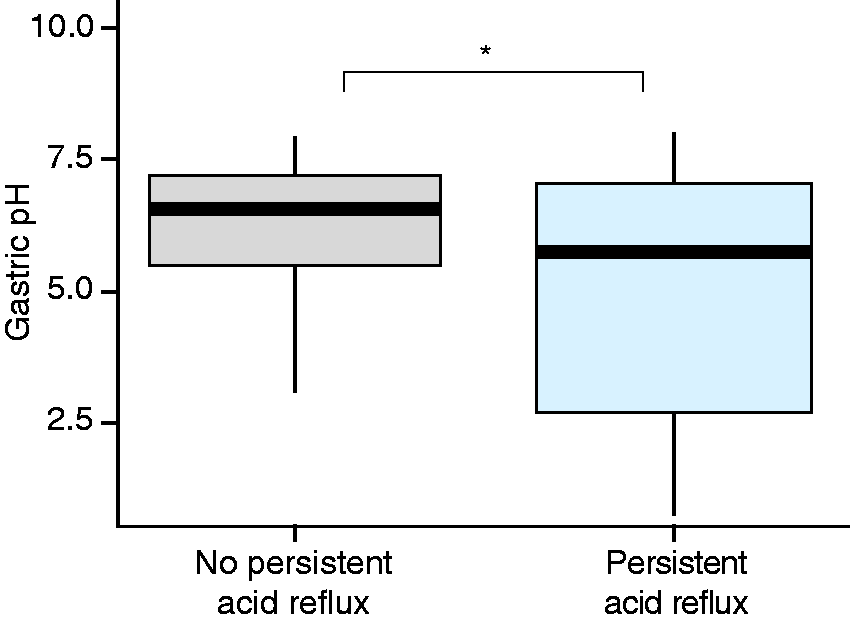
When we used EndoFaster gastric pH as a single predictor of persistent acid reflux (“normal AET” vs “abnormal AET”) using the ROC curves analysis, we found that the best threshold of gastric pH to diagnose persistent acid reflux was pH 5.05, with a sensitivity, specificity, positive predictive value and negative predictive value of 43.2%, 87.5%, 76.0%, and 62.7%, respectively. The area under the ROC curve was 63.0% (95% confidence interval: 51.3–74.7%) as shown in Figure 5(a). The positive likelihood ratio was 3.46 and the negative likelihood ratio was 0.65, yielding a post-test possibility of persistent acid reflux of 76.1% for a positive test (EndoFaster gastric pH < 5.05) and a 37.5% possibility of persistent acid reflux after a negative test (EndoFaster gastric pH ≥ 5.05), as demonstrated in the Fagan nomogram in Figure 5(b).
Accuracy of single-point gastric pH in predicting persistent acid reflux. (a) Area under the receiver operating characteristic curve. (b) Fagan nomograms. NLR: negative likelihood ratio; PLR: positive likelihood ratio.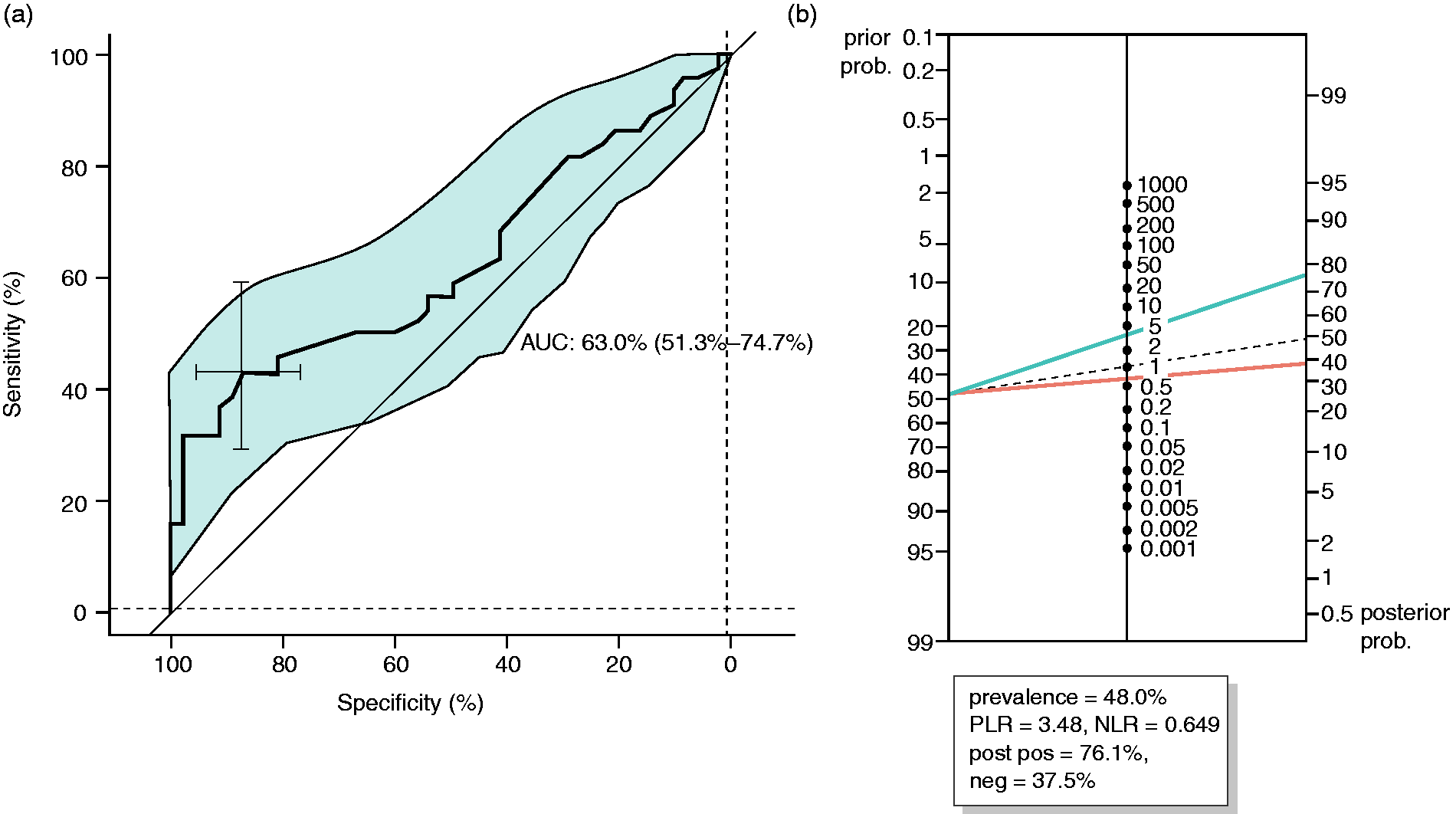
Sensitivity analysis using conventional cutoff for pathological acid exposure
Using the standard cutoff of 4% for pathological esophageal AET, 16 patients had an abnormal AET (17.4%) and 76 had a normal AET (82.6%). Like in the modified cutoff parameter, there was no difference in clinical characteristics between patients with and without persistent acid reflux, including age, sex, BMI, presence of BE and hiatus hernia. The abnormal AET group, however, had been taking significantly lower doses of PPIs than patients with normal AETs, with a median PPI classifier score of 2.0 (IQR: 1.0–2.0) and 3.0 (IQR: 2.0–3.0), respectively (p = .003). When the 24-hour AET was predicted in a multivariable regression model, the EndoFaster gastric pH parameter was not useful as a predictor of persistent acid reflux in the conventional cutoff cohort (p = .102).
Discussion
In this prospective, single-center study we have shown that clinical parameters, including severity and frequency of symptoms, are not useful in predicting persistent acid reflux in patients taking PPIs. Gastric pH measurement by EndoFaster during routine endoscopy is a good estimate of 24-hour gastric acidity and has a modest correlation with 24-hour total esophageal AET.
Patients with GERD who have partial or no response to PPI treatment represent a particularly difficult category because the lack of response to PPI is a negative predictor of success of antireflux surgery, which, based on randomized trials, has a similar rate of symptomatic remission to PPIs.13,14 The definition and mechanisms behind PPI-refractory GERD are not fully understood. It is debatable whether a lack of response to treatment should be defined by the presence of residual symptoms or rather by the evidence of persistent reflux in physiology studies. Previous studies have shown symptoms and persistent acid reflux do not correlate well, with up to one-third of patients on 40 mg esomeprazole daily treatment having evidence of persistent acid reflux.15,16 In our study the overall proportion of patients with abnormal AET was 47.8%. This high proportion is most likely because we used a less-stringent but validated cutoff value of 1.3%, which is an adjusted value for a study on PPIs. In fact, in patients on PPI esophageal AET between 1.3% and 4% could cause residual symptoms and indicate that dose adjustment should be recommended. 17 Previous studies performed in asymptomatic patients with BE during PPI therapy showed that more than two-thirds of the participants had evidence of persistent acid reflux on 24-hour pH-impedance testing. 18 In our study, we have shown that the presence of BE is significantly correlated with persistent acid reflux despite having a significantly lower degree of symptoms compared with patients without this condition. This could relate to the fact that Barrett metaplasia is an adaptive mechanism in individuals with acid reflux to reduce the burden of symptoms.
A proportion of patients who do not fully respond to PPIs have either esophageal hypersensitivity or functional heartburn. These patients have a lower threshold for nociception in response to physiological reflux episodes or other triggering stimuli. The gold standard for diagnosing these pathological entities is ambulatory 24-hour pH impedance monitoring. However, the pH-impedance test might have limited availability in clinical practice and requires two additional visits to the hospital, with related increased indirect costs. In addition, some patients do not tolerate a transnasal catheter. The clinical utility of our findings could be speculated as follows. Using the best cutoff pH value of 5.05, single-point gastric acidity can predict persistent acid reflux with a sensitivity of 43.2% and a specificity of 87.5%. Despite the low sensitivity, the high specificity indicates that patients with a gastric pH higher than 5.05 are unlikely to have persistent acid reflux. Low gastric pH at the time of endoscopy in patients on PPI therapy with persistent symptoms may indicate a suboptimal pharmacological response, suggesting that increasing the dose of medication should be attempted, rather than referring the patient for further testing (24-hour pH impedance) in the first instance.
Our study has limitations. This was a single-center study with a relatively small sample size (n = 92). Given the lack of previous data on the accuracy of real-time gastric pH measurement in predicting esophageal AET, a formal sample size was not possible. We did not use a predefined, uniform regimen of PPI treatment, which may confound the comparative analyses. We have, however, established a dedicated PPI scoring system to group each patient into a category with a comparable PPI daily dose. All regression analyses in this study were adjusted for the PPI regimen. Moreover, we did not perform pH-impedance assessment off PPIs in patients included in our study nor did we perform baseline high-resolution manometry. In standard clinical practice this is useful to locate the lower esophageal sphincter; therefore, we cannot technically exclude slight misplacement of the esophageal pH sensor in some patients. In our study protocol, the pH impedance was designed to be tested immediately after the endoscopy and it would have been impractical to perform manometry in the endoscopy room. Hence, we used careful endoscopic measurement of the GEJ landmarks and we accounted for the difference in the oral and transnasal routes to minimize the risk of pH sensor misplacement. In addition, in our main analysis we used a modified cutoff of 1.3% total AET for assessment of residual esophageal acid exposure, which could result in an overestimation of the rate of persistent acid reflux. Moreover, this cutoff for patients on various types of PPIs can be seen as a confounding factor. Nevertheless, we also performed a sensitivity analysis with a standard cutoff value of total AET of 4%; however, the small numbers of patients with abnormal AET using this cutoff may limit the interpretation of the results.
In conclusion, real-time gastric pH analysis with EndoFaster in patients on PPI treatment may provide information on persistent gastric acidity and have a role in the future to guide patient management, particularly when pH impedance is not available or tolerated. However, larger studies are required to confirm the findings of this study and provide more guidance on the best diagnostic cutoff. Until then, the ambulatory 24-hour pH-impedance monitoring remains the gold standard to guide management of GERD and differentiate among the spectrum of GERD presentations, including esophageal hypersensitivity and functional heartburn.
Supplemental Material
UEG880362 Supplemental Material - Supplemental material for Endoscopic measurement of gastric pH is associated with persistent acid reflux in patients treated with proton pump inhibitors for gastroesophageal reflux disease
Supplemental material, UEG880362 Supplemental Material for Endoscopic measurement of gastric pH is associated with persistent acid reflux in patients treated with proton pump inhibitors for gastroesophageal reflux disease by Wladyslaw Januszewicz, James Hartley, William Waldock, Geoffrey Roberts, Bincy Alias, Anthony Hobson, Lorenz Wernisch and Massimiliano di Pietro in United European Gastroenterology Journal
Footnotes
Acknowledgments
MDP is the guarantor of this article. Authors’ contributions include the following: study concept and design (MDP and LW), data collection (MDP, WJ, AH, GR, BA, JH and WW), statistical analysis (LW and WJ), data analysis and interpretation (LW, MDP, JH and WJ), drafting of the manuscript (WJ and MDP), critical revision of the manuscript (WJ, JH, WW, BA, AH, LW and MDP). All authors approved the final version of the article, including the authorship list.
Declaration of conflicting interest
None declared.
Ethics approval
This study proposal was approved by the ethical committee at the local institution September 26, 2014 (LREC01/149). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
Funding
The EndoFaster and the ambulatory pH-impedance monitoring equipment were funded by an Addenbrooke’s Charitable Trust grant. This study received infrastructure support from the Experimental Cancer Medicine Centre and from the Cambridge Cancer Centre. WJ was funded by a Cancer Research UK Multidisciplinary Project Award.
Informed consent
All patients provided written informed consent to participate in this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.