
Abstract
Background
Endoscopic therapy, including by radiofrequency ablation (RFA) or endoscopic mucosal resection (EMR), is first line treatment for Barrett’s esophagus (BE) with high-grade dysplasia (HGD) or intramucosal cancer (IMC) and may be appropriate for some patients with low-grade dysplasia (LGD).
Objective
The purpose of this study was to investigate the molecular effects of endotherapy.
Methods
mRNA expression of 16 genes significantly associated with different BE stages was measured in paired pre-treatment BE tissues and post-treatment neo-squamous biopsies from 36 patients treated by RFA (19 patients, 3 IMC, 4 HGD, 12 LGD) or EMR (17 patients, 4 IMC, 13 HGD). EMR was performed prior to RFA in eight patients. Normal squamous esophageal tissues were from 20 control individuals.
Results
Endoscopic therapy resulted in significant change towards the normal squamous expression profile for all genes. The neo-squamous expression profile was significantly different to the normal control profile for 11 of 16 genes.
Conclusion
Endotherapy results in marked changes in mRNA expression, with replacement of the disordered BE dysplasia or IMC profile with a more “normal” profile. The neo-squamous mucosa was significantly different to the normal control squamous mucosa for most genes. The significance of this finding is uncertain but it may support continued endoscopic surveillance after successful endotherapy.
Keywords
Introduction
Barrett’s esophagus (BE) is a premalignant condition in which the normal squamous lining of the lower esophagus is replaced by an intestinal metaplastic (IM) columnar epithelium in response to prolonged severe gastro-esophageal reflux. BE is the major risk factor for esophageal adenocarcinoma (EAC), a cancer with a high case fatality ratio and a rapidly rising incidence. 1 The progression from normal esophagus to BE and adenocarcinoma is thought to involve a complex, multistep process, from IM to low-grade dysplasia (LGD), high-grade dysplasia (HGD), early intramucosal cancer (IMC), to invasive EAC.
Intervention is recommended for patients with HGD or IMC, based on the estimated 7–19% yearly risk of EAC developing in patients with HGD. 1 Endoscopic therapy has replaced esophagectomy as the preferred first-line treatment for most patients with HGD/IMC, as it avoids the morbidity and mortality associated with esophagectomy, preserves the esophagus, and has equivalent survival outcomes.2,3 Guidelines1,4,5 have recommended endoscopic mucosal resection (EMR) for visible lesions and radiofrequency ablation (RFA) of flat mucosae, including after EMR. Complete Barrett’s excision (CBE) endoscopic resection is an alternative for shorter Barrett’s segments. 2 More recently, endoscopic therapy has been recommended for patients with persistent and confirmed (by two expert gastrointestinal pathologists, in two or more endoscopies) multifocal LGD.6,7
Eradication of cancer, dysplasia, and all BE is reported in up to 94% of patients treated with RFA or EMR,3,8–10 The risk of EAC development is also significantly reduced. 11 The rate of progression to EAC was one per 181 patient-years (0.55%/patient-years) in a multicenter US study, at three years after RFA or RFA and EMR combined treatment for dysplastic BE. 8 In another study, the cancer-related mortality rate was 0.2% in EMR treated patients with IMC after five years. 3
Although RFA and EMR have proven to be safe and effective in at least the medium term,9,12,13 there are reports of recurrence. 13 The durability over decades, which is relevant for this disease, and underlying molecular effect, remains unknown. It has previously been shown that the altered mRNA expression of certain genes is associated with different stages of the Barrett’s to adenocarcinoma sequence. 14 By comparing gene expression in the tissue biopsies of dysplastic Barrett’s or IMC mucosa before endoscopic therapy and in the normal-appearing neo-squamous mucosa post-treatment, we evaluated the molecular effect of endoscopic treatment.
Methods
Patients
Patients in the treatment group undergoing RFA, EMR, or combination of RFA plus EMR for the treatment of histopathologically confirmed BE with dysplasia or IMC were invited to participate in this prospective multi-center study. The treatment selected was at the discretion of the endoscopist. BE length was recorded using the Prague classification. Post-treatment biopsies were taken from the macroscopically normal appearing neo-squamous mucosa from the same area as the pre-treatment BE, as measured by distance from the incisors.
A control group consisted of individuals with the typical reflux symptoms of heartburn or regurgitation but without a history of current or past macroscopic reflux esophagitis (RE) or BE (non RE/BE). Inclusion criteria for both groups were age ≥18 years and ability to give informed consent. Approval for the study was obtained from the Human Research Ethics Committee at each center and participants provided written informed consent.
Endoscopic treatment
Radiofrequency ablation
After removal of visible lesions where present by EMR, the abnormal mucosa was ablated by RFA using either a circumferential balloon catheter or a flat plate device (BARRx Medical/Covidien, Inc., Sunnyvale California, USA). The radiofrequency energy was delivered to the Barrett’s mucosa (12 J/cm2, 40 W/cm2) twice in sequence. The device was removed and cleaned between applications, and the ablated epithelium was cleaned by irrigation or scrapped off with the edge of the device.
Endoscopic mucosal resection
The irregular mucosa was resected using the Duette multiband mucosectomy system (Cook Medical, Bloomington, Indiana, USA). The mucosa is lifted by aspiration, ligated to form a pseudopolyp, and resected by electrocautery, as described previously. 10 Both RFA and EMR were performed in single or multiple sessions, depending on the extent of BE.
Tissue specimens
From review of the histopathological reports of routine hematoxylin and eosin-stained (H&E) tissue sections, archival formalin-fixed, paraffin-embedded (FFPE) esophageal tissue samples were obtained from the study centers. The worst histopathological grade of BE/IMC was selected for the pre-treatment dysplastic BE or IMC study tissues. The post-treatment samples were matched neo-squamous mucosa collected from the same area as the previous BE mucosa.
RNA isolation
Two 7 µm unstained sections cut from each FFPE sample block were used for RNA extraction. At least 55 ng total RNA was isolated by a column-based purification method using the Ambion RecoverAll Total Nucleic Acid Isolation kit for FFPE, Cat # AM1975 (Life Technologies, Carlsbad, California, USA) or the QIAGEN RNeasy FFPE kit, Cat # 744404 (Qiagen, Valencia, California, USA), according to the manufacturer’s protocol. RNA purity and concentration was measured using a NanoPhotometer (Implen, Westlake Village, California, USA).
mRNA quantification by multiplex tandem polymerase chain reaction (MT-PCR)
Sixteen genes significantly differentially expressed at the mRNA level in BE and EAC compared to normal squamous esophagus were selected from previous studies.14,15 Full details of the MT-PCR methods were reported previously. 14 In brief, mRNA expression levels of the genes of interest and the internal reference gene, NONO (“non-POU domain containing, octamer-binding”; NM_007363), were measured in duplicate with pre- and post-treatment tissues assessed simultaneously. MT-PCR was performed using a real-time quantitative PCR system (Rotor-Gene RG6000, Qiagen, Valencia, California, USA). Primers for study genes and NONO were designed using Primer 3 software; the size of the “inner” amplicon was restricted to 70–90 bp and the “outer” amplicon to <150 bp. All primer pairs spanned an intron-exon boundary and the products were evaluated on a Bioanalyser DNA separation chip for the correct size (Agilent, Santa Clara, California, USA).
MT-PCR was performed in two steps. In the first step the RNA was converted into cDNA and amplified using multiplexed gene specific primers (“outer” primers). In the second step the product from step one was used as a template for PCRs in a 72-well disc containing lyophilized single-gene primers (“inner” primers) in each well. “Outer” primer mix was prepared by adding to one single tube 1 µl of each primer (forward and reverse) of all genes to 53 µl RNAse free diethylpyrocarbonate (DEPC) water to a total 125 µl, and they were lyophilized in 0.2 ml tubes. “Inner” primer mixes were prepared in different tubes (for each gene) by adding 4 μl of each primer (forward and reverse) into 424 μl of DEPC water.
Statistical analysis
The mRNA relative expression values were measured as the ratio of the absolute expression values of each target gene to the expression of the reference gene NONO, set to a fixed level (10,000). Gene expression values were not normally distributed, and therefore are summarized as medians with the 25th–75th interquartile range (IQR).
To identify genes differentially expressed post-treatment compared to pre-treatment values, unpaired (all subjects) and paired (subset of subjects with pre- and post-treatment samples) analyses were performed using the Wilcoxon rank-sum and signed rank test respectively. The Wilcoxon rank-sum test was also used to compare gene expression in normal squamous control versus post-treatment neo-squamous. Fold change was calculated to describe the magnitude of the change in gene expression levels pre- and post-treatment. All data analyses were performed using the SAS software (version 9.3).
Results
Patients, pathology and treatment data
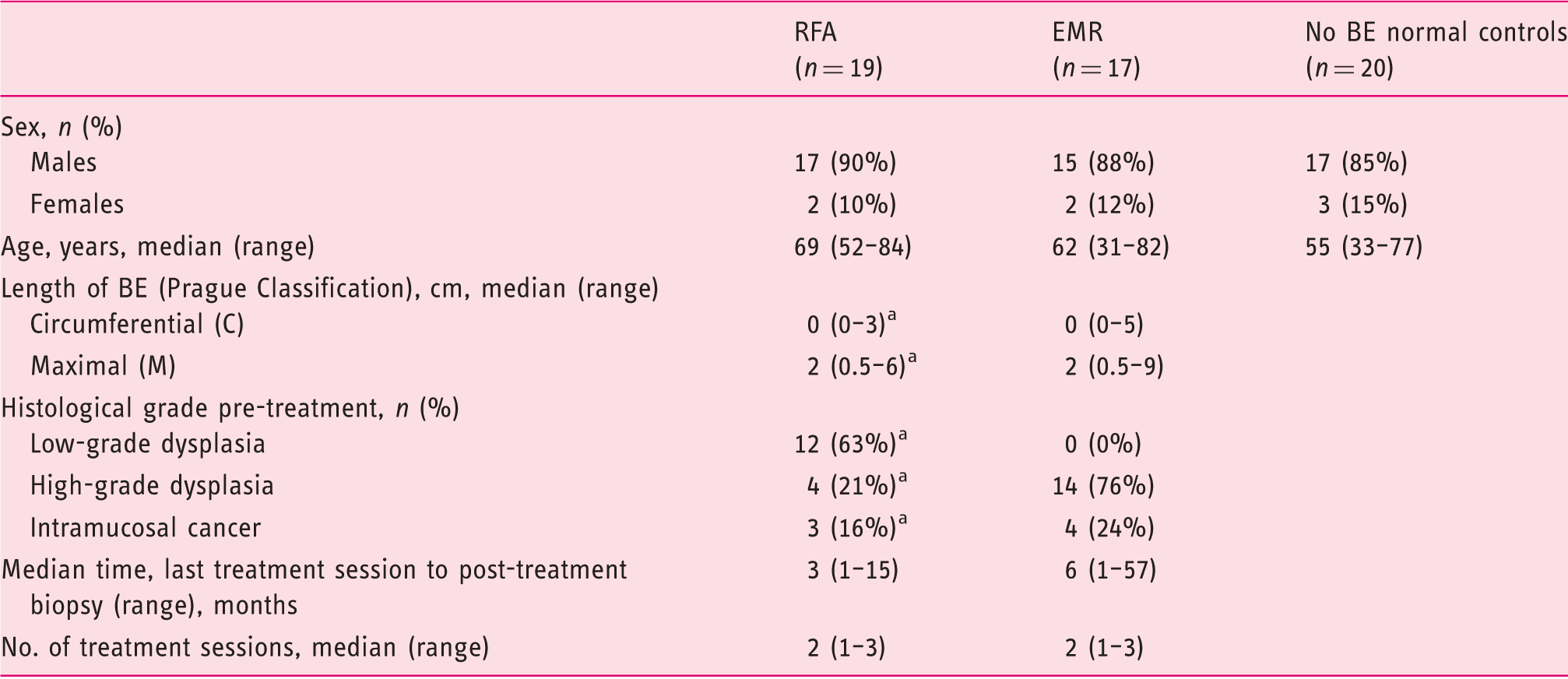
BE: Barrett's esophagus; EMR: endoscopic mucosal resection; RFA: radiofrequency ablation.
Pre-RFA, post-EMR wherever applicable.
Maximal BE length was 6 cm pre-RFA and 9 cm pre-EMR, with a median of 2 cm for both treatment groups, and RFA or EMR was performed in up to three sessions at 2–3 month intervals. The median interval between the last treatment session and the post-treatment neo-squamous biopsy was three months for RFA and six months for EMR.
At the time of neo-squamous biopsy for this study, 17 of 19 (89%) RFA treated patients and 14 of 17 (82%) EMR patients had complete eradication of dysplasia; with complete eradication of IM in 6/19 (32%) RFA and 10/17 (59%) EMR patients. Subsequent to the post-treatment study biopsy, dysplasia was eradicated in all patients apart from one EMR patient who chose not to have further treatment because of advanced age, and IM has been eradicated in 58% and 88% of RFA and EMR patients, respectively. There was no sub-squamous BE in any of the neo-squamous or normal squamous tissues.
Twenty individuals were enrolled in the control group. Normal esophagus biopsies were obtained from the distal esophagus in 11 individuals and from the proximal (∼25 cm from incisors) esophagus in nine individuals.
Difference in gene expression, pre- versus post-endoscopic treatment
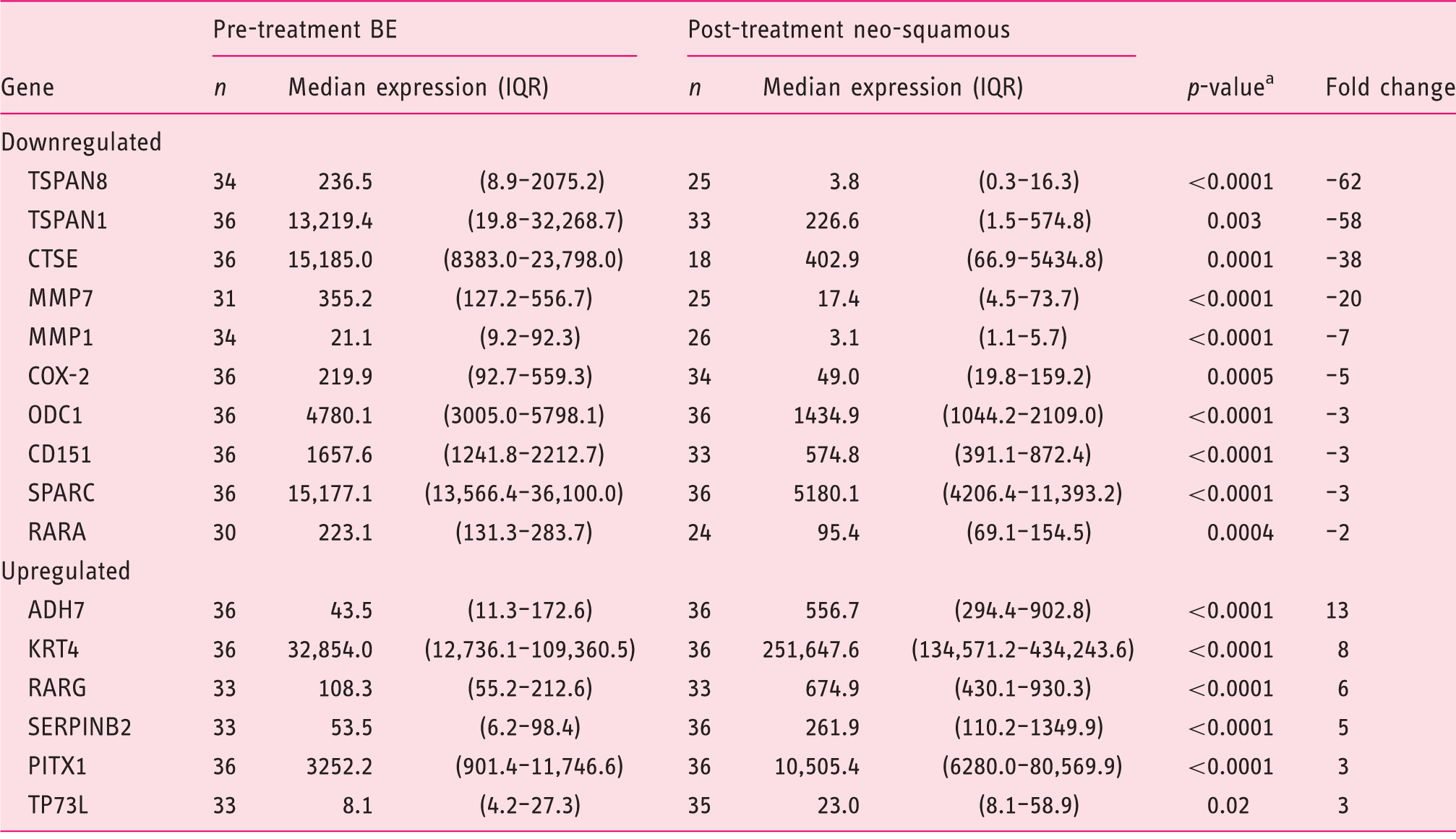
IQR: interquartile range, aWilcoxon test.
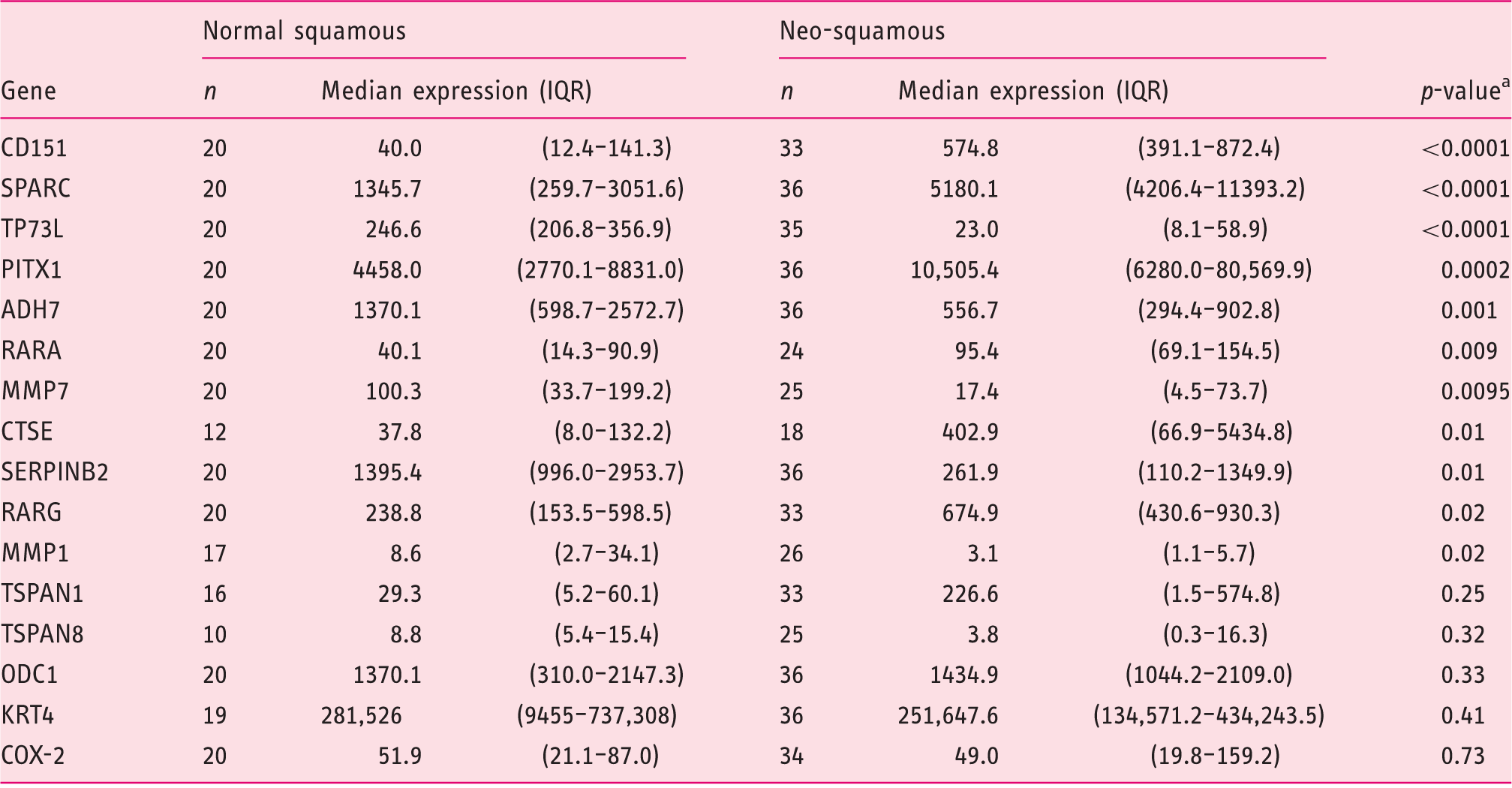
Table 3 shows the relative gene expression levels in the neo-squamous epithelium compared to true normal squamous tissue from the 20 control individuals with gastro-esophageal reflux disease symptoms, but no RE/BE. The neo-squamous mucosa was significantly different to true normal squamous mucosa for 11/16 (69%) genes. This difference was most marked for CD151, SPARC and TP73L (p < 0.0001, shown graphically in Figure 1). Figure 1 also shows data for three genes with no significant difference between neo-squamous esophagus and true normal esophagus.
Endoscopic therapy resulted in significant changes in relative mRNA expression levels pre- and post-treatment for Barrett’s esophagus (BE) with dysplasia or intramucosal cancer, compared to true normal squamous mucosa from control individuals with reflux symptoms but no BE. (a) Neo-squamous mucosa is significantly different to normal (p < 0.0001). (b) Neo-squamous mucosa difference is not significant (ns) compared to normal. Box plots show median (heavily longitudinal bar) and interquartile range (box). Difference in gene expression: normal squamous versus neo-squamous IQR: interquartile range, aWilcoxon test.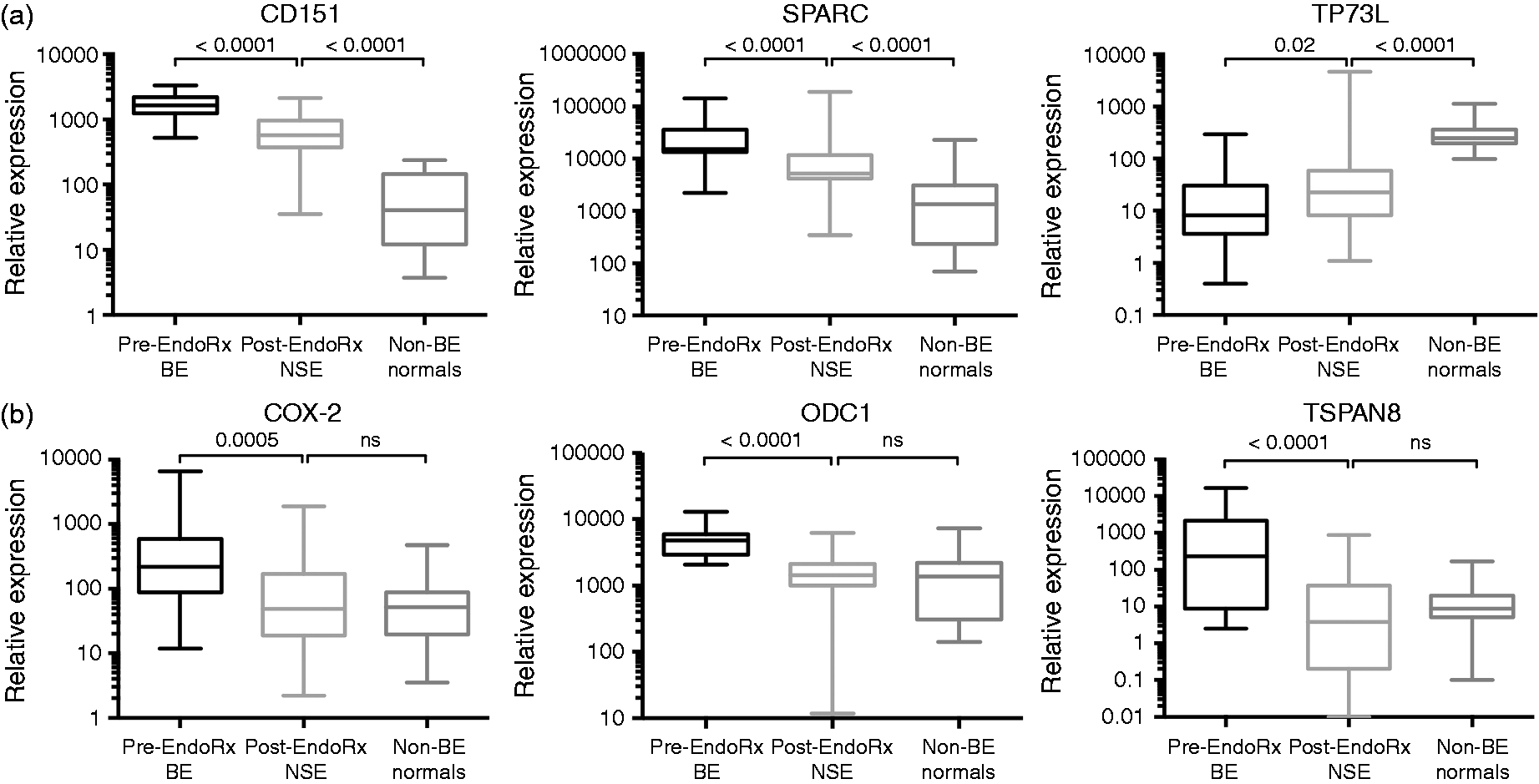
Comparing neo-squamous biopsies taken less than three months post-treatment versus more than three months post-treatment, there was no significant difference found except that SPARC mRNA expression was significantly lower in the greater than three months follow-up tissue cohort (p = 0.0159; data no shown)
Discussion
This study shows that there are marked changes in the relative mRNA expression levels of selected genes after RFA or EMR for the treatment of dysplastic BE or IMC. These changes are, as expected, towards a more “normal” squamous esophagus profile from non-BE patients. The mRNA expression in the neo-squamous mucosa post-treatment is not the same as found in the normal squamous mucosa, however, despite the neo-squamous mucosa being histopathologically indistinguishable from normal squamous epithelia.
Our findings indicate molecular as well as macro- and microscopic reversal of BE by endoscopic therapy. The expression of genes which have previously shown to be increased in a stepwise fashion from normal squamous esophagus to BE to EAC are significantly down-regulated by endotherapy, whereas those genes underexpressed in BE and EAC compared to normal mucosa are increased in expression after endotherapy. Although our study is the first to report mRNA expression changes, previous studies using different laboratory approaches have been reported. 16 Pouw et al. found no abnormal immunohistochemical (IHC) expression for Ki-67 and p53, and no numerical chromosomal abnormalities in the neo-squamous epithelia of 22 patients successfully treated with RFA for HGD or IMC. 17 Most of the patients (73%) in that study were treated with EMR before RFA for visible lesions, and salvage EMR was used on 18% of the patients after five RFA sessions to achieve complete eradication of BE. Krishnan et al., using IHC and Western blot methods, showed similar β-catenin expression in the neo-squamous and normal squamous mucosa at 12 months after successful RFA. 18 Other studies have shown persistent genetic abnormalities in remnant BE after photodynamic therapy (PDT) or argon plasma coagulation (APC).19–21
Comparing the gene expression profile of the neo-squamous mucosa with the normal squamous mucosa from individuals with typical reflux symptoms but no history of RE or BE, we found a significant difference for most genes. The relevance of this finding is unclear; we discuss three possible interpretations here. One interpretation is that this reflects ongoing wound healing, although only a minority of our selected genes (such as COX-2, matrix metallopeptidases 1 and 7) is clearly involved in wound healing. There was also no important change in the findings when we compared early post-treatment results (<3 months after endotherapy) with later post-treatment results (>3 months), suggesting that wound healing does not explain our results.
A second interpretation is that the differences in gene expression between the neosquamous and the normal squamous mucosa reflects a degree of molecular abnormality that is found even in the squamous mucosa in patients with BE. Brabender et al., for example, found a widespread carcinogenic field effect, measured in RNA quantification as in our study, in the normal squamous esophageal epithelia in patients with either BE or Barrett’s adenocarcinoma. 22 In this respect the ideal design for our study would have included normal pre-treatment squamous esophagus tissues from the patients with BE, but we lacked the biopsy samples to do this.
A third interpretation is that patients with dysplastic BE/IMC retain some risk of disease persistence or recurrence, even after successful endoscopic therapy. This further suggests that ongoing surveillance after successful endotherapy is warranted, especially in younger patients. In keeping with this, Lewis et al. found raised cell proliferation (Ki-67) and COX-2 protein expression by IHC in buried subsquamous glands after APC. They interpreted this finding as making it unclear whether the risk of cancer is adequately reduced by ablation, with potential implications for patient follow up. 23 Similarly, Dijckmeester et al. found significantly higher expression of the microRNA-143 in neo-squamous after APC compared to normal squamous from control subjects, although expression of CK-8, CK-14, and microRNA-205 was similar. 24
Clinical studies also suggest the need for ongoing surveillance and optimal reflux control after endoscopic therapy. Disease recurrence has been reported after complete eradication of Barrett’s at variable rates. In a Netherlands cohort study, IM was present in 10% of patients treated with RFA after EMR for visible nodules at five years after treatment. 25 Others report worse outcomes, including 33% BE recurrence rates at two-year follow-up after EMR and RFA, 12 5% recurrence of IM per year after RFA, 26 and 14.5% recurrence of neoplasia (HGD or EAC) after approximately two years for EMR. 3 Cancer can recur even five or more years after successful endotherapy. 3 There are several clinical factors associated with worse response to endotherapy, including ongoing acid reflux exposure (which is usual in BE patients treated by PPIs), longer Barrett’s segment, and a longer history of dysplastic BE.27–29
Genetic biomarkers could play a role in predicting response to endoscopic treatment. 16 A lower response to endoscopic treatment has been reported in patients with multiple chromosomal gains (gain of two or more locus-specific probes to MYC, p16, HER-2/neu and ZNF217, evaluated by fluorescence in situ hybridization (FISH)) in the dysplastic Barrett’s epithelium. 30 After PDT, p16 allelic loss, also detected by FISH, was found to predict loss of dysplasia. 31
Our study was prospective, used biopsies evaluated by H&E (rather than an adjacent biopsy with unknown pathology), and by simultaneously running pre- and post- treatment biopsies we limited the possibility of a “batch effect”. Despite these methodological advantages, we acknowledge some limitations. Some neo-squamous biopsies were obtained pre-complete BE eradication. Consequently, it is possible (but unknown) if the remnant BE may effect the gene expression of the neo-squamous mucosa. Our normal squamous samples also include biopsies at various levels above the gastroesophageal junction, which has been reported to influence gene expression, 32 although there was no significant difference in expression in distal compared to proximal esophagus biopsies in our study (data not shown). We did not compare the mRNA expression changes after EMR compared to RFA because of the small number of patients in each group and the difference in severity of Barrett’s disease: most of the patients undergoing EMR had IMC or HGD whereas patients undergoing RFA had mostly LGD (after EMR treatment of IMC or HGD in some cases).
Our study found that the abnormal gene expression present at baseline in patients with dysplastic Barrett’s or IMC is altered after endotherapy towards a normal esophagus expression profile. This alteration was highly significant for all genes, indicating that the neo-squamous mucosa harbors a very greatly reduced malignant risk compared to untreated Barrett’s disease. This is consistent with the normal histopathological appearance of the neo-squamous mucosa and the reassuring results of clinical studies regarding the long-term cancer risk after endoscopic therapy. The neo-squamous mucosa was significantly different to the normal control squamous mucosa for most genes but the significance of this finding is uncertain. One interpretation is that it suggests that attention should be given to careful inspection of the neo-squamous mucosa as well as, of course, any persistent BE areas after endotherapy. This could include taking random biopsies from a normal appearing neo-squamous mucosa; although the benefit of this is disputed it can rarely uncover buried (sub-squamous) BE or even adenocarcinoma.17,33–35 Altogether, we interpret our results as providing some support for long-term endoscopic surveillance after endoscopic treatment of BE/IMC, even if the BE has been completely eradicated, we acknowledge that more extensive studies with longer follow-up periods are needed to more thoroughly evaluate the neo-squamous mucosa.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Australian National Health and Medical Research Council (project grant 100837) and the Cancer Council New South Wales (SRP 08-04).