
Abstract
Background
The significance of a family history of esophageal adenocarcinoma in the progression to esophageal adenocarcinoma in patients with Barrett’s esophagus has not been thoroughly evaluated. The purpose of this study is to evaluate the presence of esophageal adenocarcinoma in a first-degree relative in patients with Barrett’s esophagus.
Methods
A retrospective cohort study was conducted of patients with Barrett’s esophagus at a tertiary care center undergoing radiofrequency ablation. Family history, demographics, and pathology and endoscopy reports were assessed in all patients.
Findings
Three hundred and one patients with Barrett’s esophagus were assessed. Nineteen patients who had a diagnosis of esophageal adenocarcinoma on index endoscopy were excluded. Nineteen (6.7%) patients had a first-degree relative with esophageal adenocarcinoma. Four (21.1%) of these patients progressed to esophageal adenocarcinoma. Of patients without first-degree relative with esophageal adenocarcinoma 22/263 (8.7%) progressed to esophageal adenocarcinoma. In a logistic regression model adjusted for sex and the number of radiofrequency ablation treatments, we found that family history of esophageal adenocarcinoma was a significant independent predictor of progression to esophageal adenocarcinoma (odds ratio = 5.55, 95% confidence interval: 1.47–20.0).
Conclusion
Our study indicates that Barrett’s esophagus patients with a first-degree family member with esophageal adenocarcinoma are at 5.5-fold higher risk for disease progression to esophageal adenocarcinoma. Family history of esophageal adenocarcinoma in Barrett’s esophagus patients should be considered in patient surveillance and radiofrequency ablation treatment, beyond recommended guidelines.
Key summary
The incidence of esophageal adenocarcinoma (EAC) is on the rise. The literature was limited but some studies suggested a familial inheritance pattern of both Barrett’s esophagus (BE) and EAC. This study indicates that BE patients with a first-degree family member with EAC are at 5.5-fold higher risk for disease progression to EAC. Barrett’s esophagus patients with a positive family history (FH) of EAC developed EAC at a much younger age compared to those BE patients that denied having a FH of EAC.
Introduction
Barrett’s esophagus (BE) is a metaplastic change from the normal stratified squamous epithelium of the esophagus to simple columnar epithelium with goblet cells, similar to that found in the small intestine. This process is known as intestinal metaplasia (IM). BE, the only known precursor lesion to esophageal adenocarcinoma (EAC), has an estimated prevalence between 0.5–2.0% and its incidence continues to rise. 1 As a result, the incidence of EAC continues to rise. 2
A number of factors increase the risk for both BE and its progression to EAC. These include male sex, advanced age, Caucasian race, obesity, tobacco use, and long-segment BE. 3 The relationship between family history (FH) and risk for BE and progression to EAC is less well described. Although rare, both familial BE and familial EAC have been reported. Generally, this is defined as two or more first degree family members diagnosed with BE, EAC, or gastroesophageal (GE) junction adenocarcinoma. Chak et al. estimated the prevalence of familial BE and EAC to be about 7%.4,5 A few studies have compared the characteristics of familial and sporadic BE and EAC. For both BE and EAC, no differences were observed for gender, ethnicity, and tobacco or alcohol use. The findings related to body mass index (BMI) have varied, with one study reporting no difference and another reporting a lower BMI with familial BE and EAC. 6 Both familial BE and EAC occur at a younger age. Compared to sporadic EAC, patients in the familial group are diagnosed 5–10 years earlier.6,7 We were interested in the effect of FH on the risk of EAC in those with BE. The primary aim of our study was to determine whether having a first-degree relative (FDR) with EAC increases the risk for developing EAC in patients with known BE, and secondarily to compare the characteristics of BE patients that progressed to EAC with a FH of EAC versus those who did not have a FH of EAC.
Methods
Approval was obtained from the Ethical and Institutional Review Board at Thomas Jefferson University Hospital (TJUH) on 18 March 2016. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. This was a retrospective medical record review and included 301 patients with dysplastic BE that underwent radio frequency ablation (RFA) at TJUH between March 2006–March 2016. Informed consent of subjects was waivered given the non-existent to minimal risk to subjects and the retrospective design of the study. The following data was obtained from the electronic and paper medical record: age, gender, race, age at diagnosis of BE, age at diagnosis of EAC, FH of EAC, endoscopy results, pathology results, and length of follow up a TJUH. FH was obtained based on reporting in the medical record. All pathology specimens with dysplasia or indefinite for dysplasia were reviewed by a second expert gastrointestinal pathologist. All RFA treatments were performed by four expert gastroenterologists using the HALO ablation system.
We used SPSS statistical software, version 24 for analysis. We calculated descriptive statistics for each data point, including sample size, mean, and standard deviation. When evaluating the patients with EAC and the impact of a positive FH, we assessed continuous variables using a nonparametric Mann-Whitney U test. Categorical variables were assessed using a Fisher’s exact test. We compared the cohort of patients with EAC and a positive FH of EAC to the cohort without a FH.
Results
A total of 301 patients underwent RFA for BE between March 2006–March 2016. Two hundred and forty-nine (82.7%) patients were male. All patients underwent at least one RFA session. Two hundred and seventy-nine (92.7%) patients were Caucasian. The mean age at diagnosis of BE was 62.1 years. The mean BE segment length was 3.5 cm, with segment lengths ranging from less than 1 cm to 18 cm. Following review of the original pathology, 88 (29.2%) patients had nondysplastic BE (NDBE); 79 (26.3%) had low grade dysplasia (LGD); 94 (31.2%) had high grade dysplasia (HGD); 21 (7.0%) were indefinite for dysplasia (IFD); and 19 (6.3%) had EAC (Figure 1). One hundred and sixty-two (69.5%) pathology specimens were originally collected outside TJUH. Specimens that did not originate from a tertiary medical center with expert gastro-intestinal pathology were reviewed at TJUH.
Original pathology on index endoscopy of all patients. EAC: esophageal adenocarcinoma; IFD: indefinite for dysplasia; NDBE: nondysplastic Barrett’s esophagus; LGD: low grade dysplasia. HGD: high grade dysplasia.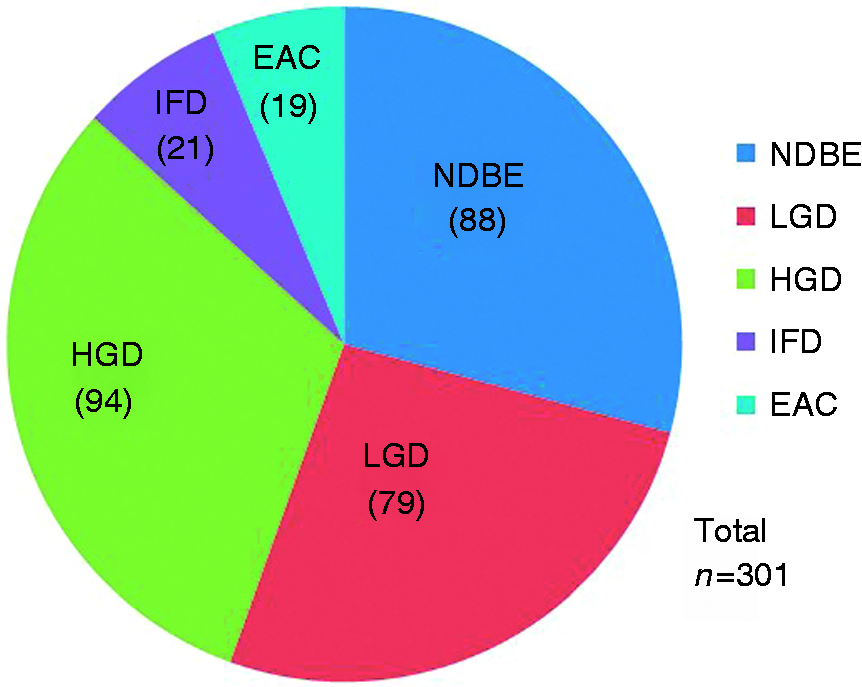
We compared the post-RFA outcomes of patients with a history of EAC with patients who did not have EAC. Patients who were lost to follow-up or still undergoing RFA were excluded from this analysis. There was no statistically significant difference in the number of RFA sessions (3.5 vs 3.3, p = 0.266). Patients with EAC were less likely to achieve complete remission of intestinal metaplasia (CR-IM) (70.5% vs 95.2%, p < 0.001) and complete remission of dysplasia (CR-D) (81.8% vs 100%, p < 0.001).
A total of 282 patients were included in our study group. The average follow-up at our institution was 36.3 months. Twenty-six (9.2%) patients progressed to EAC from an original diagnosis of BE at index endoscopy - six had NDBE, five had LGD, 13 had HGD, and two had IFD (Figure 2).
Original pathology on index endoscopy of patients diagnosed with esophageal adenocarcinoma (EAC). IFD: indefinite for dysplasia; NDBE: nondysplastic Barrett’s esophagus; LGD: low grade dysplasia. HGD: high grade dysplasia.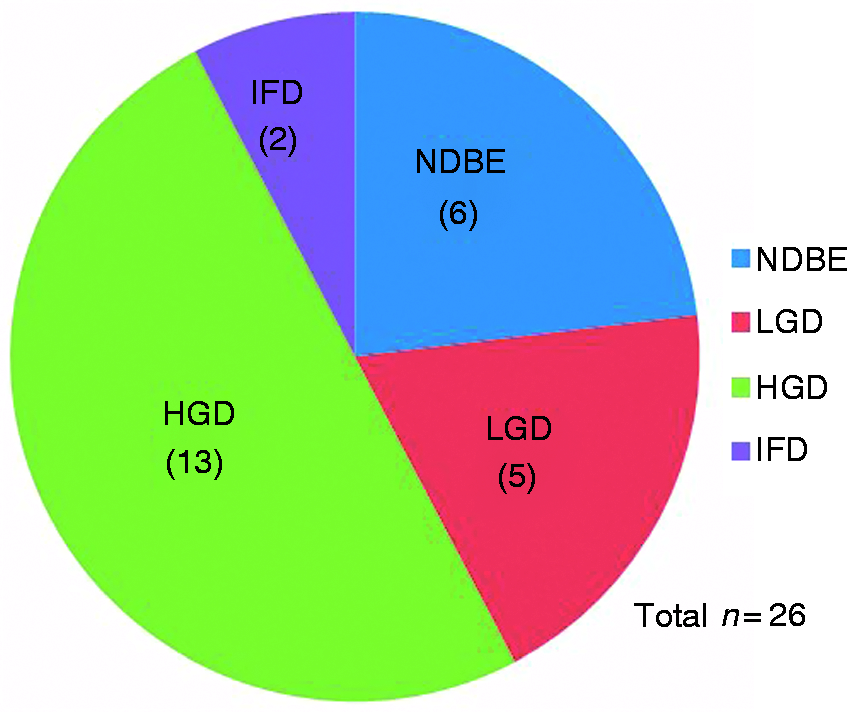
Nineteen (6.7%) patients in the cohort reported at least one first-degree family member with EAC, while 263 (93.3%) patients reported no known FH of esophageal cancer. Of the 19 BE patients that had a FDR with EAC, four (21.1%) progressed to EAC during the study period. The pathology of these patients on index endoscopy diagnostic of BE were one NDBE, one LGD, and two HGD. Of the 263 BE patients without a FH of EAC, 22 (8.4%) progressed to EAC during the study period. The pathology of these patients on index endoscopy diagnostic of BE were five NDBE, four LGD, 11 HGD, and two IFD. A FH of EAC was significantly associated with the risk of BE progression to EAC (FH = 21.1% vs no FH 8.4%; odds ratio (OR) = 5.55, 95% confidence interval (CI) (1.47–20.0), p = 0.012)
Comparison of esophageal adenocarcinoma (EAC) patients with a family history (FH) positive for EAC with those who had a negative FH.
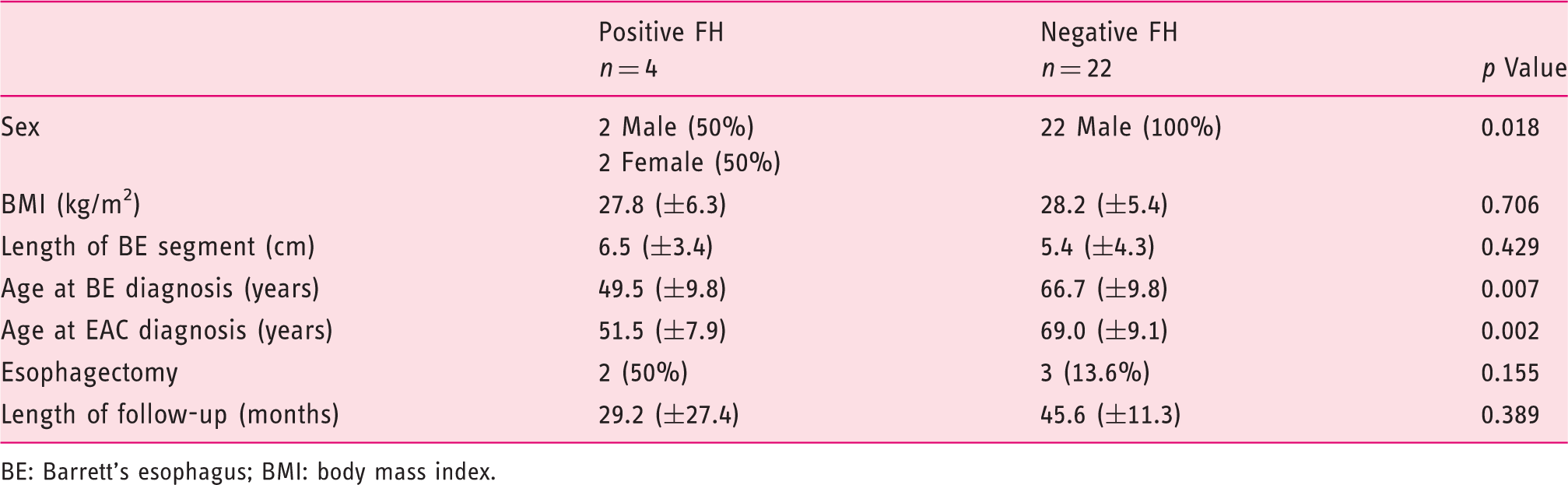
BE: Barrett’s esophagus; BMI: body mass index.
We also evaluated whether exclusion of the 19 patients referred for dysplastic BE and found to have EAC at the time of presentation to our institution might have affected these findings. None of these 19 patients had a FDR with EAC. Inclusion of these 19 patients did not change the findings of earlier diagnosis of both BE and EAC in those with a FH vs those without a FH (BE: 49.5 ± 9.8 years vs 66.8 ± 8.8 years, p = 0.003; EAC: 51.5 ± 7.9 years vs 67.9 ± 8.4 years, p = 0.001).
We compared the post-RFA outcomes of patients with EAC with patients who did not have EAC. Patients who were lost to follow-up or still undergoing RFA were excluded from this analysis. There was no statistically significant difference in the number of RFA sessions (3.5 vs 3.3, p = 0.266). Patients with EAC were less likely to achieve CR-IM (70.5% vs 95.2%, p < 0.001) and CR-D (81.8% vs 100%, p < 0.001).
Discussion
BE is a known risk factor for EAC. The incidence of EAC has risen dramatically over the past several decades, especially in the Western hemisphere. 7 Hur et al. reported that, despite the continued rise in incidence, the rate of rise of early stage EAC has decreased. Furthermore, since the 1990s the survival with localized EAC has improved. 8 The reason for this is unclear but has been speculated to be related to both endoscopic screening of high-risk individuals resulting in the detection of earlier stage cancers as well as Barrett’s ablation in those at high risk for progression to EAC. Nonetheless, the incidence of late stage EAC continues to rise. 9
Our study demonstrates that a FH of EAC in a FDR increases the risk for EAC in patients with BE. This finding is supported by additional small studies of familial clustering of BE and EAC.7,10,11 Furthermore, our study also found that EAC in the setting of BE occurs at an earlier age in those with a FH of EAC. Our study focused on patients referred for dysplastic BE who developed EAC during the course of follow-up at our institution, and we excluded those found to have EAC at the time or referral. However, a separate analysis including these excluded patients did not affect our findings.
Many cancers are known to have a familial predisposition. Hereditary factors appear to play a role in both the development of BE and EAC. 12 Endoscopic screening in relatives of BE and EAC patients may lead to an increase in the number of diagnoses of both BE and EAC. 13 However, most cases of BE and EAC are sporadic and related to somatic gene mutations as well as environmental factors, especially long-standing gastroesophageal reflux. Ash et al. reported no difference in endoscopic findings when patients with familial BE were compared to those with sporadic BE. 6 As previously noted, Chak et al. reported that approximately 7% of patients with both BE and EAC had a positive FH for BE or EAC.4,5 However, this estimate included a combination of gastroesophageal junction (GEJ) and esophageal body cancers. Some experts believe the inclusion of GEJ cancers may falsely inflate the prevalence of familial EAC, as some of these cancers may arise from gastric mucosa and not necessarily from underlying BE. 14 A possible autosomal dominant inheritance with incomplete penetrance has been suggested.7,11
Our study has some limitations. First, we employed a retrospective design. FH was based on patient reporting, as documented in the electronic medical record. This could lead to errors in either reporting or documentation. Next, our sample size is small and thus our study may be underpowered. Additionally, all patients in our study were treated at a single tertiary care medical center and our results may not be generalizable. Furthermore, we cannot exclude the possibility of differences in the performance of surveillance endoscopy in those with a FH of EAC, contributing to an increased diagnosis of EAC in these patients. However, the occurrence of EAC approximately 17 years earlier in BE patients with a FH is not likely to be explained by screening differences alone. With respect to the earlier diagnosis of BE in those with a FH of EAC, it is possible that earlier endoscopic screening was performed in this group precisely as a result of an EAC FH.
BE patients with a FDR with EAC are over five times more likely to progress to EAC. These cancers occur more than a decade earlier as compared to BE patients without a FDR with EAC. If confirmed using larger, multicenter, prospective studies, a FH of EAC in a FDR should be considered an additional risk factor (along with long BE segment, obesity, and tobacco use) for progression of BE to EAC. Our findings may impact screening and surveillance recommendations. For instance, a FH of EAC may lower the threshold to institute endoscopic screening for BE in those with risk factors such as longstanding acid reflux. Further, given the earlier onset of both BE and EAC in those with a FH of EAC, endoscopic screening should be considered at a younger age and perhaps in both men and women. FH of EAC may also be a consideration in determining surveillance interval as well as utilization of emerging intra-procedure adjunct diagnostic and predictive techniques that assist with risk stratification. Finally, FH of EAC may be a consideration when weighing ablative therapy in those with BE. Larger, prospective studies are needed to determine optimal screening recommendations, surveillance intervals and potentially treatment options in BE patients who report a FH of EAC.
Declaration of conflicting interests
All authors report no conflicts of interest to disclose in regards to this article.
Ethics approval
The need for ethic approval for this study was exempted as it was retrospective and did not directly involve human subjects or animals.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Informed consent is not applicable for this study as it was retrospective and did not directly involve human subjects.