
Abstract
Objective
The thermal destruction of non-dysplastic Barrett’s esophagus (BE) and its replacement by squamous epithelium is an attractive, but unproven strategy to avoid further development of dysplasia or cancer.
The goal of this study was to estimate the persistence of restoration of squamous epithelium and the risk of cancer in BE that was eradicated using argon plasma coagulation (APC) in the absence of high-grade dysplasia, 16 years after its application.
Design
We followed 32 patients with BE who underwent eradication of metaplastic epithelium using APC, up to 16 years later.
Results
At the end of the initial treatment, 25 of 32 patients (78%) had complete endoscopic eradication, there was partial squamous re-epithelialization in four patients (13%) and it was absent in three patients (9%). We observed buried metaplastic glands under new squamous epithelium in 6 of the 25 patients who had complete endoscopic eradication. At follow-up, sustained complete endoscopic eradication was observed in 16 of 32 patients (50%), partial eradication in 11 of 32 patients (35%); there were two patients (6%) lost to follow-up and three patients (9%) developed esophageal adenocarcinoma. Two of the latest cases arose from the buried glands under neosquamous epithelium after complete eradication and one arose from a small remaining Barrett’s segment.
Conclusions
We observed long-term re-epithelialization in the majority of patients who had previously had complete eradication of Barrett’s esophagus. This did not provide protection against cancer development, as the incidence of cancers arising from buried glands or from residual Barrett’s esophagus was similar to that observed in patients undergoing no specific treatment.
Keywords
Introduction
Barrett’s esophagus (BE) is defined as a condition in which the stratified squamous epithelium of the distal esophagus is replaced by metaplastic columnar epithelium containing goblet cells. 1 The presence of intestinal metaplasia is an accepted histological marker for BE, because development of dysplasia or cancer is usually associated with intestinal metaplasia. 2
Adenocarcinoma in the setting of BE develops according to a well-known histological sequence, from non-dysplastic Barrett’s to low-grade dysplasia, followed by high-grade dysplasia (HGD) and cancer. 3 The annual incidence of adenocarcinoma in non-dysplastic BE is reported in old series to be 0.5–0.8%, but more recent data suggest that it is as low as 0.12%. 4 This increases to 10% per patient-year when HGD is present, and 40–50% of patients with HGD in BE present with adenocarcinoma within 5 years. 5 HGD BE is associated with a cancer risk that may justify invasive treatment, while non-dysplastic and low-grade dysplasia (LGD) BE are much less severe conditions, and their risk for cancer progression is much lower; however, the significance of LGD is not completely clear and may be largely underestimated, with a higher risk in the cases of confirmed diagnosis.6,7
The destruction of non-dysplastic intestinal metaplasia and its replacement by squamous epithelium is an attractive potential strategy for making a direct impact on the risk of tumor development. Over the past 15 years many ablative modalities have been developed, with various outcomes. 8 All of these methods ablate tissue without the benefit of histological specimen retrieval.9–13 Their aim is to destroy the metaplastic/dysplastic epithelium, which will then be replaced, in non-acid environments, by squamous epithelium. 14 The interest in ablation techniques was revived by the development of radiofrequency ablation (RFA) devices. This is supported by strong clinical data on the short- and mid-term efficacy of RFA in treating HGD or LGD, potentially in conjunction with mucosal resection in the cases where visible lesions are present. The use of RFA or other ablative techniques in non-dysplastic BE with the hope of preventing dysplasia and/or cancer development; however, is unproven and should not be recommended routinely.
If an ablation procedure does not destroy all the metaplastic epithelium, then the partially-ablated mucosa may heal with an overlying layer of neosquamous epithelium that buries metaplastic glands in the lamina propria, where they become hidden from the endoscopist’s view. This ‘buried metaplasia’ may have malignant potential and adenocarcinoma can arise from buried metaplasia. The frequency with which endoscopic ablation results in buried metaplasia is not well-defined. It is not clear whether neoplasms develop from non-neoplastic glands that were buried by ablation, neoplastic glands that were already subsquamous before ablation, or were buried by the ablation procedure 15 ; however, it is of major importance to gather information on the long-term outcome of these patients, because ablation of non-dysplastic BE might be indicated, if it is associated with a dramatic decrease in cancer incidence and avoids the need for surveillance.
The present study evaluated long-term outcomes in a cohort of patients who were included in a prospective study of non-dysplastic BE ablation using argon plasma coagulation (APC) between March 1996 and January 1997, who were followed prospectively during 16 years or who we relocated after the 16-year follow-up period.
Methods
Patients
We enrolled patients with Barrett’s esophagus at least 3 cm in length, with biopsy-proven intestinal metaplasia, between March 1996 and January 1997. Exclusion criteria were as follows: Previous history of gastro-esophageal surgery, BE with HGD or cancer, uncontrolled significant comorbidities, use of non-steroidal anti-inflammatory drugs and age <18 years. The study was approved by our local ethics committee and all patients signed informed consent before treatment.
Endoscopic treatment
Diagnostic upper endoscopy defined the extent and circumferential character of BE and presence of hiatal hernia. Four-quadrant biopsies were obtained every 2 cm and reviewed by two experienced pathologists. Such biopsies were performed during the baseline endoscopy, after completion of endotherapy and during our follow-up. The size of BE ranged from 3–11 cm (median 4.5 cm). Five patients had LGD.
APC (60 watts, forced coagulation, ERBE ICC 200, Germany) was applied at 4-week intervals until there was no endoscopic evidence of Barrett’s esophagus and a decision to stop APC was made. APC was applied by maintaining the probe at a short distance from the mucosa and creating lines of coagulation while pulling the scope backwards. All patients received proton pump inhibitor (PPI) 40 mg daily during their period of endotherapy. All patients underwent surveillance endoscopy, with biopsies taken at 3, 6, and 12 months after their APC treatment; and also yearly or every 3 years during follow-up, depending on the presence or absence of dysplasia. Results were histologically confirmed as follows:
Complete eradication: No finding of residual metaplastic columnar epithelium within the neosquamous epithelium; Partial eradication: Finding residual metaplastic columnar islands, tongues or segments above the proximal extent of gastric folds; or Absence of eradication: In cases of treatment failure.
Statistical methods
We used statistical methods of: frequency analysis of qualitative variables for the determination of absolute frequencies, relative frequencies in percents and cumulative relative frequencies; analysis of variance for calculation of averages; standard deviation, standard error and determining the 95% confidence interval (CI) of the average; correlation analysis methods to evaluate the unknown outcome values containing random errors; calculation of Spearman’s linear correlation coefficient; regression analysis methods for mathematical modeling of data, by use of linear regression; and search parameters evaluation.
Results
Initial endoscopic ablation was administered to 32 patients with Barrett’s esophagus (26 men, 6 women; mean age 64 years, range 46–76 years) who were then followed for 16 years (n = 22), until death (n = 8), or until lost to follow-up (n = 2). The initial mean length of Barrett’s segment for the cohort was 4.5 cm (range, 3–11 cm). The segment was circumferential in 22/32 patients (69%). Intestinal metaplasia without dysplasia was observed in 27/32 patients (84%) and with LGD in 5/32 patients (16%). Our patients underwent 1–5 APC applications within a period of 1–5 months and received PPI 40 mg daily during the period of endotherapy. PPI therapy was maintained for 12 months after endotherapy and then given thereafter, according to symptoms.
Immediate results (1 month after the last APC application), as presented in Figure 1, showed complete endoscopic eradication in 25 of 32 patients (78%), partial squamous re-epithelialization in four patients (13%) and absence of eradication in three patients (9%). The presence of residual buried metaplastic glands under the new squamous epithelium was observed in six patients (19%) who had complete eradication. Complete eradication was significantly more frequent in short and non-circumferential Barrett’s segments.
16
Immediate results 1 month after the last argon plasma coagulation application (%).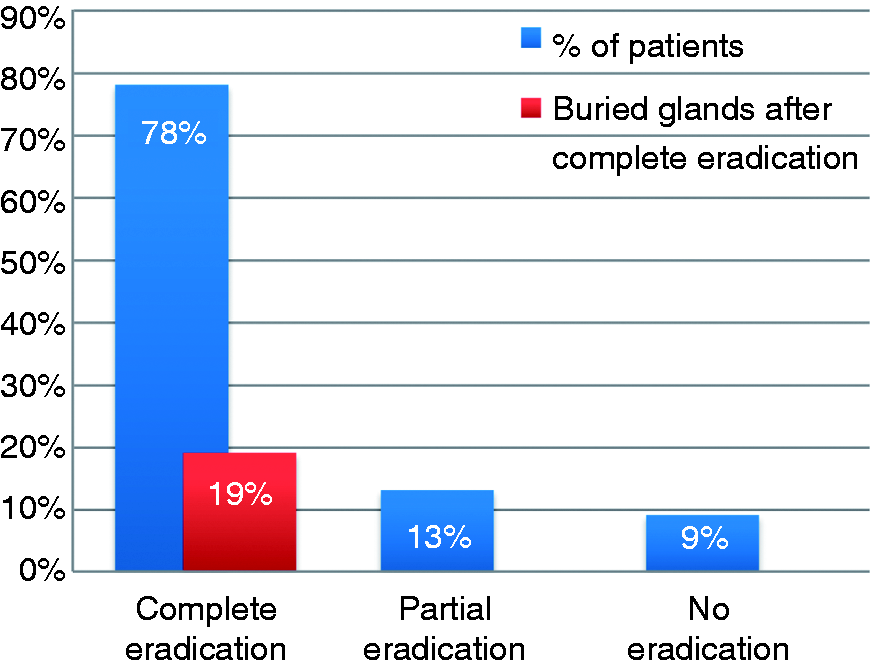
Complications after the APC procedure included strictures in two patients (6%) and bleeding in one patient (3%). Esophageal strictures were successfully treated with 2–3 balloon dilatations and bleeding was rapidly stopped endoscopically.
We observed, 16 years after the end of initial treatment or at the last endoscopy before death, sustained complete endoscopic eradication in 16 of 32 patients (50%), as is shown in Figure 2. The presence of residual buried metaplastic glands under the new squamous epithelium was observed in three of these patients (9%). Partial eradication was observed in 11 of 32 patients (35%), due to persistence of intestinal metaplasia without dysplasia. Two patients (6%) were lost to follow-up and three patients (9%) developed esophageal adenocarcinoma.
Long-term outcomes 16 years after the last argon plasma coagulation application (%).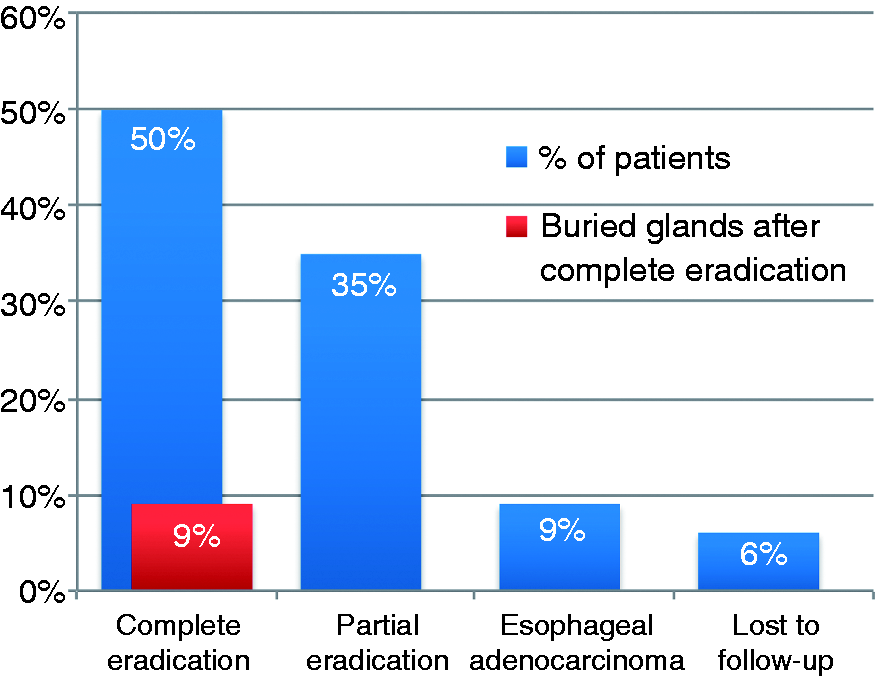
During the long-term follow-up eight patients died, but none of these deaths were due to esophageal adenocarcinoma. Two patients were also lost to follow-up, one of them due to the development of Alzheimer’s disease.
A total of 376 patient-years (pt-yrs) of follow-up were available in this study. Amongst the patients who initially had complete endoscopic eradication, the incidence of cancer appearing underneath the mucosa was 0.53% per pt-yr (2 cancers per 376 pt-yrs), and for those with partial eradication, 1.1% per pt-yr (1 cancer per 94 pt-yrs). When considering only the patients without dysplasia (n = 27) who were followed for a total of 323 pt-yrs of follow-up, the incidence of adenocarcinoma was 0.61% per pt-yr; and for those with initial LGD who were followed for a total of 75 pt-yrs of follow-up, the incidence of adenocarcinoma was 1.3% per pt-yr (Figure 3).
Incidence of esophageal adenocarcinoma after APC ablation of non-dysplastic and LGD BE.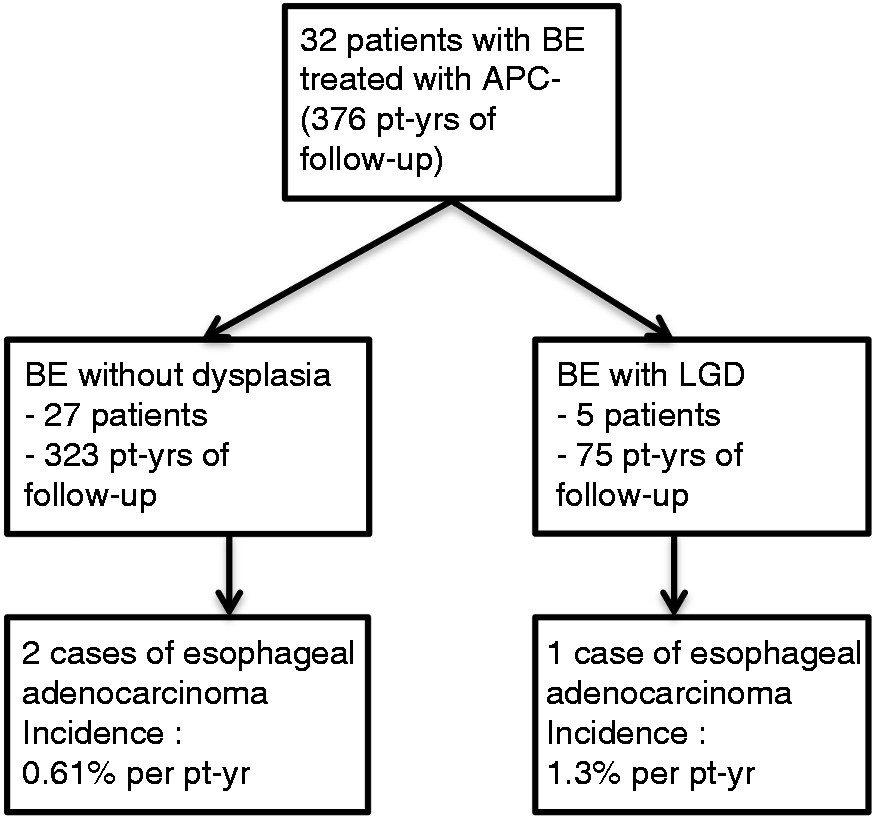
Of the patients who developed adenocarcinoma, the first patient developed intramucosal esophageal adenocarcinoma 18 months after the complete eradication of an initially non-dysplastic 8-cm long circumferential Barrett’s segment. Histologically, some remaining buried metaplastic glands were observed under the new squamous epithelium, 1 month after the last APC application. 17 Diagnosis of a buried subsquamous adenocarcinoma (TisN0M0) was confirmed 18 months after APC and endoscopic mucosal resection was performed, with complete resection of the neoplastic lesion. The patient was followed, with absence of relapse, and died from another disease 6 years later.
The second patient developed esophageal adenocarcinoma 12 years after complete eradication of a 6-cm long circumferential Barrett’s segment with LGD. During long-term follow-up, recurrence of a 2-cm Barrett’s segment without dysplasia and an adenocarcinoma was observed that arose from the re-epithelialized area, 3 cm above the residual Barrett’s segment. Endoscopic mucosal resection was performed and histology showed a well-differentiated esophageal adenocarcinoma with submucosal infiltration. Given the age of the patient was 89 years, no surgery was recommended.
The third patient developed intramucosal esophageal adenocarcinoma 13 years after incomplete endoscopic eradication of an initially non-dysplastic 6-cm long circumferential Barrett’s segment. A relapse of a semi-circumferential 2-cm Barrett’s segment was found 6 months after the last APC session and then a tumor developed on this segment, 13 years later. Endoscopic mucosal resection was performed with complete resection of the neoplastic lesion (TisN0M0). Endoscopic and histological follow-up showed an absence of relapse 1 and 2 years after the endoscopic resection. We show summarized results in Figure 4.
Endoscopic treatment of BE with APC: Immediate and long-term outcomes.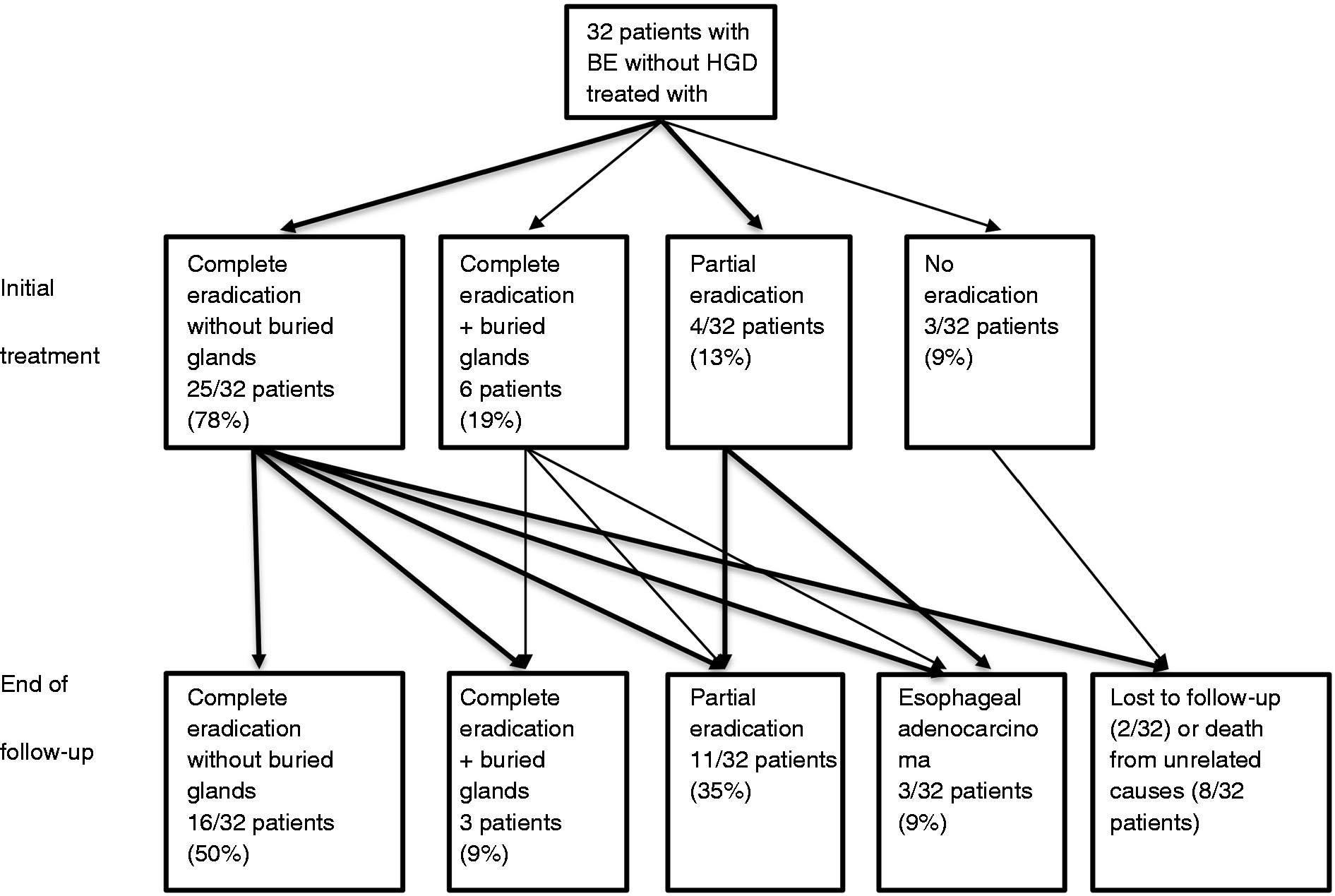
Discussion
The present study demonstrates that BE without dysplasia or with LGD can be completely eradicated using APC in 78% of patients and that squamous re-epithelialization is maintained at very long-term follow-up, in almost two-thirds of the subjects. This study also shows that those patients undergoing ablation for non-dysplastic or LGD BE will develop cancer at a rate which is at least similar to that reported in the usual follow-up of patients with similar Barrett’s who did not undergo ablation. Two out of the three tumors which occurred in patients after APC of BE took place underneath the neosquamous epithelium, whereas buried glands were previously identified in only one case, by systematic 4-quadrant biopsies after ablation.
Ablation is proposed as a means of decreasing or abolishing the risk of cancer; therefore, there is a need for surveillance. The present findings, where the incidence of cancer in patients who underwent ablation was similar to that reported in patients who had no ablative treatment and received regular surveillance, bring this into question. Furthermore, the fact that two tumors arose underneath the neosquamous epithelium argues that ablation may make surveillance more difficult and may favor diagnosis of a ‘visible lesion’ at a later stage.
The disappointing results obtained in this study may be related, in part, to the fact that we reported on the use of a type of ablation used in the last century. Indeed, APC equipment available in the 1990s allowed the application only of forced coagulation; and the other settings with the new APC-2, such as ‘PRECISE’ APC or ‘PULSED’ APC, allowing to apply a more homogeneous, superficial ‘spray-like’ coagulation were not available then. The dose of PPI used during ablation was also low, when compared with the one used in more recent publications, but this was the one recommended in most series of BE ablation.14,18
The APC performed as we did it is obviously no longer the preferred method of ablation. This does not mean that APC should be abandoned, because it has been recently shown to be useful when associated with focal resection of HGD, 19 and a revival of the technique might take place in the future, when combined with simultaneous submucosal injection 20 ; however, at the time of our study, the 19% rate of buried glands that we initially observed in patients with complete endoscopic eradication compared favorably with other techniques, like photodynamic therapy (PDT), which had reported frequencies of buried metaplasia up to 51%.15,21 Radiofrequency ablation is now considered the current gold standard for ablation, with a lowest reported frequency of buried metaplasia of 0.9%, as described in 18 studies (6 without dysplasia, and 12 with LGD or HGD), including 1004 patients after RFA of BE with follow-up intervals that ranged from 8 weeks to 5 years.15,22 Buried metaplasia is, however, clearly not the only issue, and two of the three cancers that we observed in our follow-up study occurred in patients in whom buried glands under the neosquamous epithelium were not initially observed.
The risk of cancer associated with buried metaplasia is unclear, and different hypotheses have been proposed to explain why that risk might be greater or less than that of the native surface metaplastic epithelium. One proposal is that genetic abnormalities acquired during carcinogenesis might convey survival advantages that render neoplastic Barrett’s cells more resistant than non-neoplastic cells to ablative therapies.23,24 If this is true, then ablative therapies might be better suited to destroy normal cells than neoplastic ones and ablation might be predisposed to bury neoplastic cells that have a high risk of malignancy. Other investigators believe that sub-squamous buried glands may regress or remain clinically unimportant, due to protection by the neosquamous epithelium from the carcinogenic effects of refluxed acid and bile. Buried glands have also been noted to have fewer deoxyribonucleic acid (DNA) content abnormalities, suggesting that they may have a lower neoplastic potential.23,25
In contrast, several reports describe the development of subsquamous adenocarcinoma from buried glands after treatment of advanced BE with either APC or PDT.23,26 There are 37 cases with subsquamous neoplasia described in the literature: 31 cases after PDT, 3 cases after APC and 3 cases after apparently successful RFA.26–28 It is probable that all ablation techniques are not at an equivalent risk of being associated with buried glands, and even for APC, recent reports suggest that results might be improved by careful application, especially after ablation of a visible malignant lesion or by combining APC and submucosal injection.19,29
In the long 16-year follow-up of our study, we observed two cases of adenocarcinoma arising underneath the neosquamous epithelium after complete eradication and one case arising from relapsed Barrett’s segment after incomplete eradication. Our observation showed that endoscopic inspection of the mucosa is not sufficient for defining complete eradication, and in our case, only targeted biopsies proved the presence of intramucosal adenocarcinoma that had developed under the neosquamous layer. This suggests that surveillance programs and targeted biopsies from the previous Barrett’s area are recommended, even after reversal therapy, because the lesion may be covered by neosquamous epithelium.
Of the three cancers we observed in this study, only one had LGD diagnosed before therapy and two had no dysplasia detected, despite random biopsies performed every 2 cm in every patient, before inclusion. The possibility of a lesion not being detected at the time of treatment has already been discussed when we reported our first case of ‘buried’ cancer, 17 and we believe that we did everything possible to avoid it with the endoscopic imaging available then and our protocol of systemic biopsies; however, the missed diagnosis is even more improbable for the two other cancers that were diagnosed 12 and 13 years after treatment.
Even in 2014, the recommendations for careful examination using our ‘best scopes’ remain paramount when any thermal ablation is foreseen. If HGD or early cancer are suspected, endoscopic mucosal resection has to be performed and completed before any ablation. 19 In the case of LGD, histological confirmation by an experienced pathologist or using diagnostic endoscopic mucosal resection (EMR) should be performed, before deciding treatment.6,19
Eight patients died during follow-up, none related to esophageal adenocarcinoma. The three patients with cancers underwent local curative therapy and the one with advanced cancer is 89 years old, not a candidate for surgery, and is still alive. This stresses again the fact that BE should not be considered a life-threatening condition when appropriate follow-up is available.
A limitation of our study is the relatively modest size of the study population, collected from a single referral center, which limits the application of our results to the general population; however, it is counterbalanced by the remarkable long-term follow-up of these patients, which highlights the possible development of cancer from subsquamous buried glands.
Our results showed that ablating the specialized Barrett’s epithelium with APC could lead to complete eradication, but the low sustained success rate and the fact that intramucosal adenocarcinoma can originate from metaplastic glands buried by ablation, brings into question the final objective of this ablative treatment, which is cancer prevention. The risk of developing cancer in our study population was similar to that reported in surveillance studies of non-dysplastic Barrett’s patients, who had no ablative treatment and underwent regular surveillance. Endoscopic ablation should not be recommended as a routine treatment for non-dysplastic Barrett’s esophagus, because it not only may not prevent cancer development, but also might render its diagnosis more difficult by burying metaplastic glands with malignant potential.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there are no conflicts of interest.