
Abstract
Background
Immigration-related new diseases pose a growing challenge for healthcare services in receptor countries. Following Latin American migration, Chagas disease has inevitably appeared in Europe.
Aim
To determine the prevalence and characteristics of oesophageal motility disorders in immigrants infected with Trypanosoma cruzi, using high resolution oesophageal manometry (HREM).
Methods
In all newly-diagnosed cases with chronic Chagas infection referring upper digestive symptoms, a protocolized clinical evaluation and complementary tests including barium oesophagogram and HREM were carried out. As control group, 14 healthy subjects from the same endemic areas were studied with HREM.
Results
We included 61 patients (46 female, 15 male; age range 26–63 years). Only seven patients (11%) had a minor alteration on barium oesophagogram. By contrast, 23 (37%) patients showed an alteration in oesophageal manometry, mainly minor motility disorders (34%). Only one healthy control (7%) had a minor motility disorder at HREM (p = 0.029 vs. patients).
Conclusions
Oesophageal motor disorders in infected immigrants with Chagas disease are common, and mainly characterized by a minor motility disorder that is not detected by barium oesophagogram. Hence, as well as barium oesophagogram examination, HREM should be considered, to assess oesophageal damage in this specific group of patients.
Keywords
Introduction
Immigration is an increasing phenomenon that poses a new and growing challenge for healthcare services in receptor countries due to the introduction of new diseases among other effects. Chagas disease is a zoonosis caused by the parasite Trypanosoma cruzi, a flagellated protozoa mainly transmitted to humans by blood-sucking triatomine-vector insects such as Triatoma infestans and others. Historically, the geographical distribution of Chagas disease was confined to that of its vector, namely Central and South America. Following the influx of immigration by Latin Americans to Europe, however, the disease has inevitably appeared in European Union nations; up to 3,000,000 Latin American immigrants have arrived in Spain since year 2000, and it has been estimated that 58,000 to 68,000 of these individuals are infected by T. cruzi.
The natural history of the disease consists in a usually self-limited acute phase followed by a long asymptomatic period of latency. After decades of undetected infection, over 30% of individuals develop clinical symptoms reflecting tissue damage. The heart is the organ mainly affected by the disease, followed by the digestive tract (mainly the oesophagus, colon or both). It has been reported that about 7–10% of infected individuals have involvement of the digestive tract. 1 The frequency of digestive disease varies according to the predominance of specific subspecies of T. cruzi. T. cruzi IIb and V in the Southern Cone of South America are particularly found in digestive tissues. 2
Classically, barium oesophagogram has been considered as the first line diagnostic test to study the oesophageal involvement of Chagas disease.3,4 However, oesophageal manometry has developed as an important tool in the diagnostic work-up of the disorder, with a spectrum of patients ranging from asymptomatic minor motility disorders to severe achalasia-like megaesophagus.5–8 Recently, the development of high resolution oesophageal manometry (HREM) has effected an important advance in the diagnosis and understanding of oesophageal motility disorders, leading to a new classification of oesophageal motility disorders.9,10
Considering these advantages, we hypothesized that HREM could improve detection of oesophageal motor disorders in infected immigrants with Chagas disease, especially in the period of quiescence of the disease, and designed a prospective controlled study to evaluate HREM in all infected immigrants who reported oesophageal symptoms.
Methods
Subjects
All consecutive adult patients newly diagnosed with Chagas infection at the International Healthcare Unit Metropolitana Nord of Barcelona were contacted. This International Healthcare Unit is a referral unit that belongs to the Institut Català de la Salut, the main public health provider in Catalonia and, therefore, all healthcare provided is free of charge for the patients. The majority of patients were referred by family practitioners as foreseen in the protocol of the Chagas screening programme for populations at risk at primary care level in Catalonia.
Patients with a diagnostic test positive for Chagas infection and upper digestive symptoms were consecutively included. Children under 18 years, pregnant women, patients with oesophageal disease, or other disease that could affect oesophageal motility, and patients with conditions that contraindicated HREM were excluded.
There is no clinical or serological marker to determine the duration of the infection. Most of our patients were probably infected by T. cruzi in childhood. These patients lived in adobe houses where the vector transmitting infection is originated. So, the duration of the infection could range between 15 and more than 40 years.
A group of 14 healthy subjects originary from endemic areas of South America (seven female, seven male, age range 21–68 years) and without abdominal symptoms or Chagas infection were included in the study as controls.
The study protocol was approved by the Ethics Committee of the University Hospital Germans Trias i Pujol, and all participants gave their written informed consent.
Diagnosis and general evaluation of Chagas disease
Individuals were considered to have ‘Chagas infection’ when two commercialized ELISA-based serological tests (against crude and recombinant T. cruzi antigens) were positive. In the case of discrepant results, a third IFI (indirect immunofluorescence) based test was performed. In all these newly-diagnosed patients a full clinical evaluation was performed, including a 12-lead electrocardiogram (ECG) with a 30-second DII strip and a two-dimensional Doppler echocardiogram. Presence of Chagas cardiac involvement was defined on the identification of any abnormality either at ECG or echocardiogram. 11 Every patient referring upper digestive symptoms was studied following a protocol that included blood analysis (eosinophil count, calcium, proteins, thyroid-stimulating hormone (TSH) and antinuclear antibodies (ANA)), 13C-urea breath test, parasites in stools, barium oesophagogram and HREM. Parasite or Helicobacter pylori infections were treated prior to the completion of oesophagogram and HREM.
Questionnaires
Each participant filled in one questionnaire with the following variables: age, sex, country of origin and self-reported family history of Chagas infection (yes/no).
Upper digestive symptoms were evaluated using a questionnaire that included the following symptoms: dysphagia, chest pain, heartburn and regurgitation. The frequency of each specific customary symptom was registered using a 0–5 score scale, 0 being ‘never’, 1 ‘yearly’, 2 ‘monthly’, 3 ‘weekly’, 4 ‘daily’ and 5 ‘at every meal’.
Other, non-digestive-related, symptoms (recurrent respiratory infections and weight loss), ECG alterations, echocardiographic abnormalities, presence of H. pylori or parasites in stools were also registered.
Radiological study
Barium oesophagogram was performed as follows: 200 ml of barium contrast was administered orally to the patient in erect position and right anterior oblique projections were taken. The contrast was administered until a column of sufficient height was obtained to ensure passage of contrast to the stomach, allowing visualization of the shape, diameter, wall contours and kinetic activity of the oesophagus. X-ray plots were taken at the time of administration of barium and 60 s later.
High resolution oesophageal manometry
HREM was performed in all the participants using a solid-state HREM assembly with 36 circumferential sensors spaced at 1-cm intervals (Sierra Scientific Instruments, Los Angeles, CA, USA). On the day of the study, participants were intubated after a 6-h fast. The manometric probe was introduced transnasally, and positioned to record from the hypopharynx to the stomach with at least three intragastric sensors. The catheter was fixed in place by taping it to the nose, and the participant was asked to lie in supine position for recording to start. The protocol started with a 30-s period of basal recording without swallowing to assess basal pressures, followed by 10 5-ml water swallows at 30-s intervals.
Experimental design
Each patient participated in only one study. All patients referred to the International Care Unit were evaluated by the same physician, and when inclusion criteria were fulfilled, one radiologic examination and one HREM were performed in each patient.
Data analysis
Demographic data, concomitant conditions and symptoms frequency were sampled for further analysis.
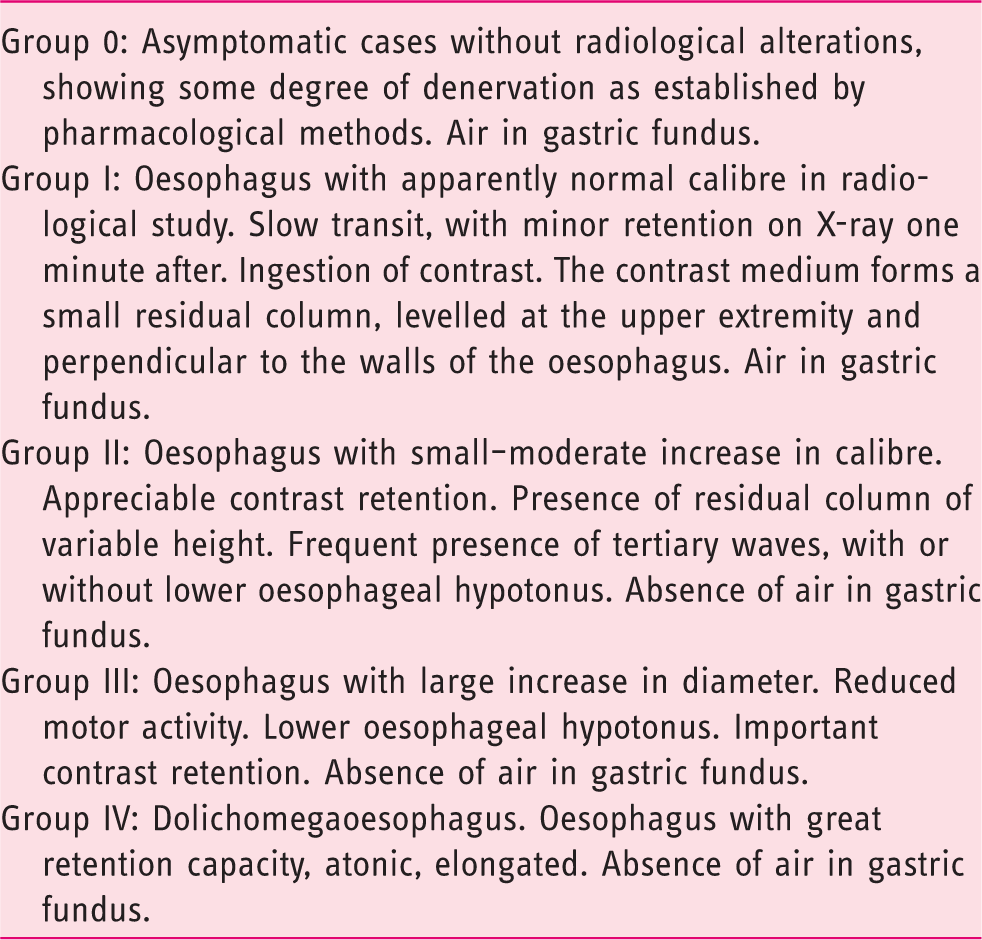
Radiological classification of alterations in Chagas disease. 4
Manometric data was analysed using the Mano-View analysis software (Sierra Scientific Instruments Inc., Los Angeles, CA, USA) following the parameters described in the Chicago consensus, and a final diagnosis was established for each patient according to the Chicago 3.0 Classification. 10
All demographic data was sampled by the same investigator (SR), evaluation of barium X-ray plots was performed by the same radiologist (MIG-D) and HREM traces were evaluated by the same gastroenterologist (JS). Neither the radiologist nor the gastroenterologist was aware of the results of the other tests performed.
Statistical analysis
The relative frequency of each registered variable was analysed using SPSS statistical software version 20 (Chicago, IL, USA). According to the results obtained, contingency tables were constructed and the prevalence of oesophageal motility disorders in patients and healthy controls were compared by χ2 testing. Further, radiological abnormalities, cardiological involvement, concomitant infections and oesophageal symptoms in patients with and without oesophageal motility disorders were compared, and when differences were observed in the bivariate analysis, stepwise multiple logistic regression analysis was performed. Statistical significance was considered as a p value of 0.05.
Results
Baseline characteristics of patients.
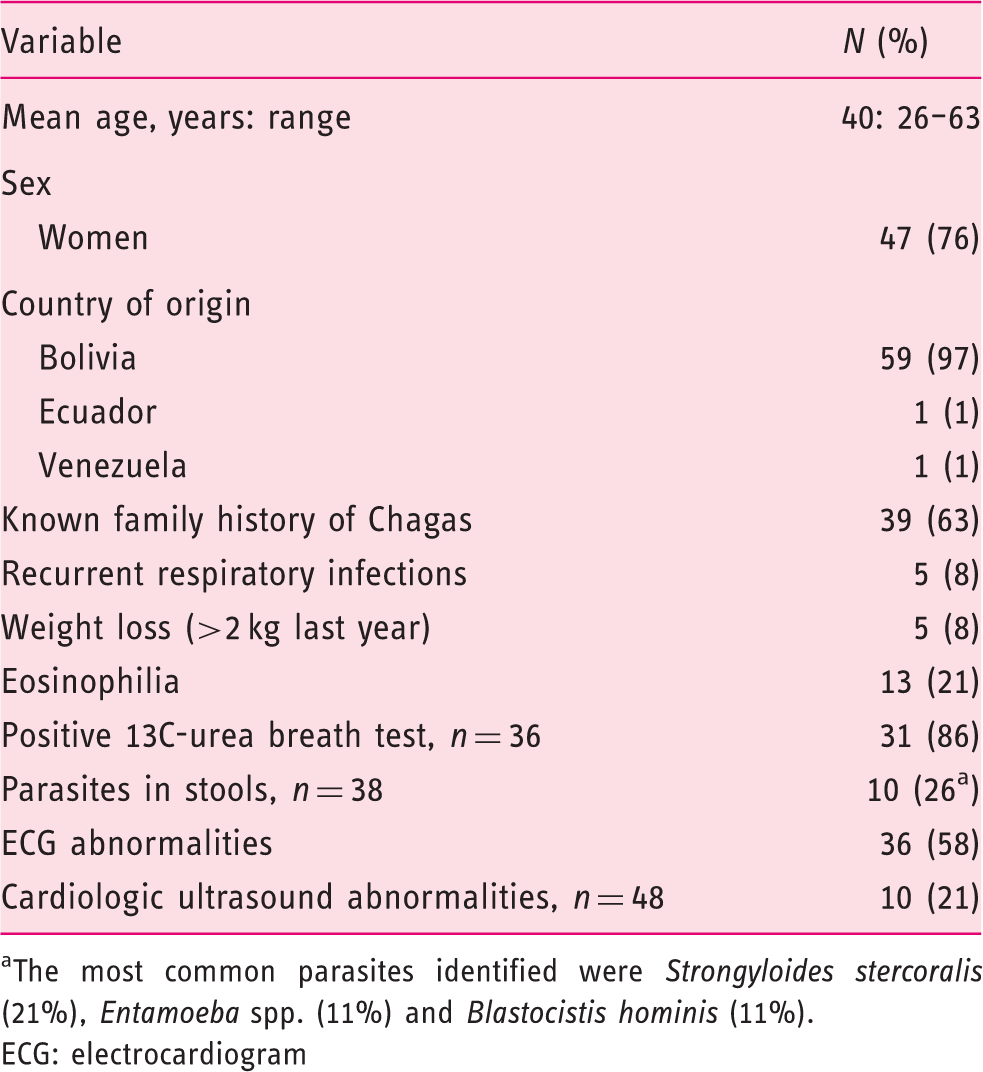
The most common parasites identified were Strongyloides stercoralis (21%), Entamoeba spp. (11%) and Blastocistis hominis (11%).
ECG: electrocardiogram
H. pylori infection and parasites in stools were frequent findings (Table 2). All these infections were treated, and normalization of 13C-urea breath test and parasites in stools were checked before inclusion in the study. Recurrent respiratory infections and weight loss were uncommon (Table 2).
ECG abnormalities were also common (Table 2). The most frequent electrocardiographic changes were block right bundle branch (50%) and sinus bradycardia (38%). Six patients had advanced Chagas cardiomyopathy (four had low ejection fraction, below 50%, and two had a pacemaker implanted).
Barium oesophagogram
According to the Rezende criteria
4
(Table 1), the majority of patients had a normal radiologic examination (grade 0), only seven patients (11%) had an abnormal examination (Figure 1), and in all cases minor radiological abnormalities (grade 1 in six patients and grade 2 in one patient). Five of these patients had also a minor motility disorder at HREM, whereas the remaining two patients had a normal HREM according to Chicago 3.0 criteria, and all but one had cardiologic involvement. Note: when bivariate and multivariate analysis was performed, altered cardiologic ultrasound examination was the only finding significantly associated with an altered barium oesophagogram (odds ratio (OR) 32 (1–737); p = 0.030).
High resolution oesophageal manometry detected a greater number of motility abnormalities than barium oesophagogram in patients infected with Chagas disease. Oesophageal motility disorders were uncommon in healthy controls from the same origin. However, the great majority of alterations in infected patients were minor motility disorders, and no patient had an achalasia-like motor alteration.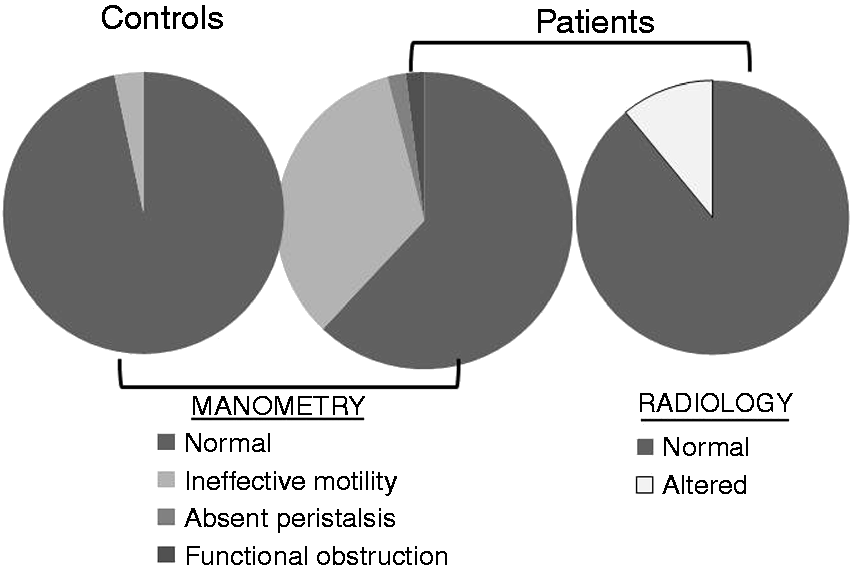
HREM
Correlation between oesophageal alterations at HREM, and alterations in barium oesophagogram, cardiologic studies, and daily oesophageal symptoms (n (% of patients)).
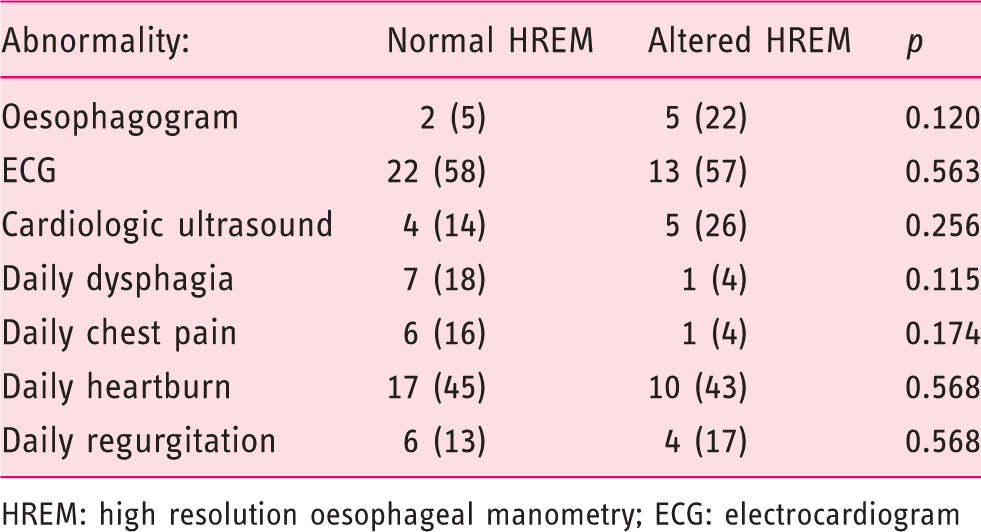
HREM: high resolution oesophageal manometry; ECG: electrocardiogram
Heartburn was the predominant symptom in both patients with altered oesophageal motility and patients with normal HREM (Figure 2), whereas other symptoms, such as regurgitation, dysphagia and chest pain, were uncommon (Figure 2). When only daily oesophageal symptoms (score 4 or greater) were analysed, no association between any single abdominal symptom and altered oesophageal motility was present (Table 3). Likewise, there was no association between altered oesophageal motility and other factors as antecedent of H. pylori infection, eosinophilia, stool parasites or respiratory infections (data not shown).
Symptoms referred by patients with Chagas disease. Note that referral of heartburn and regurgitation was similar in patients with normal motility and patients with altered manometry.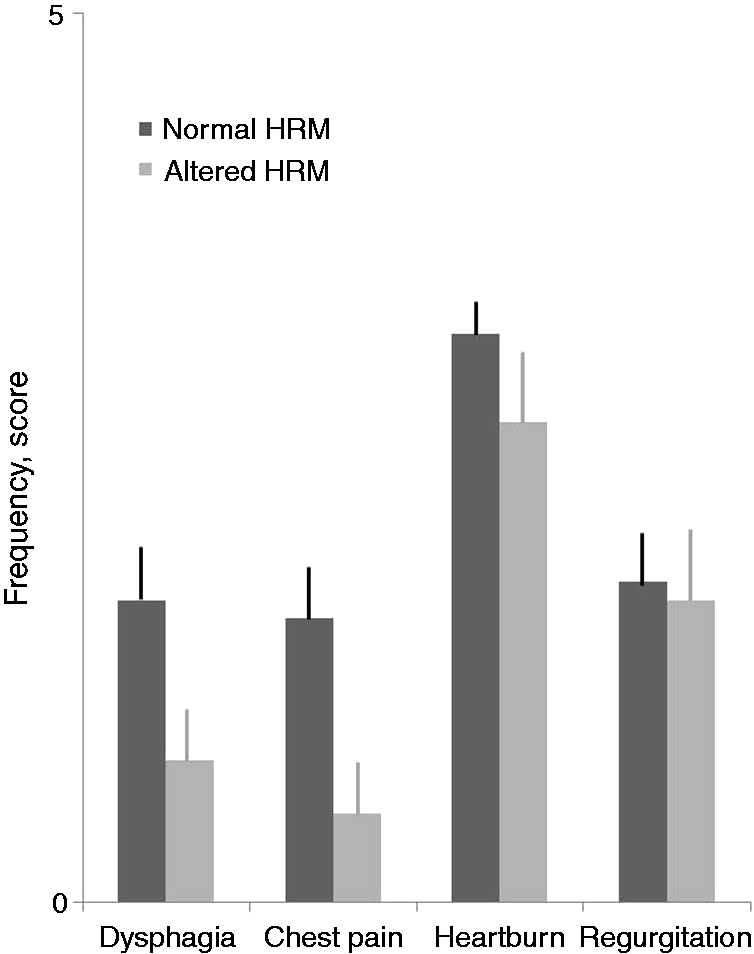
Patients with Chagas disease showed a tendency towards lower lower oesophageal sphincter (LES) pressures (17 ± 1 mmHg) than healthy controls (23 ± 2 mmHg; p = 0.056). Hence, 49% of patients with Chagas infection but only 27% of healthy controls had a LES pressure bellow 15 mmHg (p = 0.099). Moreover, when low LES pressure (below 15 mmHg) and ineffective oesophageal motility were considered together, 69% of patients with Chagas infection but only 29% of healthy controls showed an abnormality in the HREM (p = 0.007).
Discussion
The present study, using HREM to assess oesophageal motility, demonstrates that oesophageal motor disorders in infected immigrants with Chagas disease in a non-endemic area are common, and are mainly characterized by minor disorder of peristalsis, distinct from the typical achalasia-like Chagasic oesophageal involvement, and that this disorder is undetected using conventional radiographic studies.
To our knowledge, this is the first study published in a population of immigrants studied in a non-endemic area using HREM. The vast majority of data published on Chagas disease has been obtained from countries where the disease is endemic, using radiologic studies in patients with severe digestive symptoms.12,13 The clinical characteristics of the patient population in the present study are different. Our patients, like most immigrants from endemic areas in Europe, are young and, in general, healthy subjects, with the Chagasic infection in the quiescence phase. Consequently, the typical achalasic megaoesophagus with aperistalsis that has been described in Chagas disease using radiological examinations4,14,15 is a rare finding in these specific patients. By contrast, using such a sensitive tool as HREM, an oesophageal motility disorder was found in a significantly greater proportion of patients with Chagas disease than in healthy controls from the same endemic areas. The type of motility disorder predominant in these patients is an ineffective oesophageal motility. Aperistalsis was present in only one patient, and functional EGJ obstruction in another patient. Additionally, patients with Chagas infection had a tendency towards lower LES pressures than healthy controls. These findings are similar to what has been reported in infected subjects with incidentally discovered Chagas disease in their country of origin using HREM, 16 mainly hypocontractile peristalsis, which could reflect the oesophageal involvement of an early stage of the disease. Similar findings have also been reported in infected immigrants studied in the same European area using conventional manometry. In these studies, the typical achalasia-like motility disorder was uncommon, and a decreased LES pressure and ineffective oesophageal peristalsis were the most common findings. However, if both ineffective motility and low LES-pressure are considered, the number of patients with manometric abnormalities in these studies was smaller (3–55%) than in our study (69%), reflecting the greater accuracy of HREM in the detection of oesophageal motility disorders.17,18
The vast majority of infected immigrants in our area are originally from Bolivia, and are infected by specific subtypes of Trypanosoma, subtype TcI and TcV.19–21 Subtype TcI is associated with severe cardiologic disease, and subtype TcV produces mixed cardiologic and digestive alterations. In our study no patient had a severe oesophageal disorder, but six patients had a severe Chagas cardiopathy. Three of these patients had ineffective oesophageal motility at HREM, and the remaining patients had an isolated hypotensive LES. These results suggest that using a more sensitive tool such as HREM, mixed cardiologic and digestive involvement may be found to be more frequent than previously reported.1,12,22 However, these results could have been different if other populations of immigrants infected with other Trypanosoma subtypes had been evaluated.
The types of motor alterations observed in our patient population are similar to the abnormalities observed in patients with gastrooesophageal reflux, and among the different symptoms evaluated, heartburn was the most frequently referred symptom. Regrettably, a pH-measurement was not obtained from our patients, and studies of asymptomatic patients with Chagas disease could not be performed due to logistic problems related to their difficult working conditions. However, this motor alteration was not observed when a cohort of non-symptomatic healthy subjects of the same origin were studied, and the prevalence and frequency of typical reflux symptoms (heartburn and regurgitation) were similar whether or not ineffective motility was present at HREM. Previous studies evaluating the association between Chagas disease and gastrooesophageal reflux could not demonstrate a clear association between them, even though Troncon et al. found that patients with Chagas disease have a tendency to develop reflux.23,24 Hence, even though neither heartburn nor regurgitation was associated with ineffective oesophageal motility, we cannot exclude the possibility that an association between reflux and T. cruzi infection exists. To note, dysphagia and chest pain were more frequently referred by patients with normal manometry. However, both symptoms had a low frequency, and when only daily symptoms were compared, we found no differences between groups, so the clinical relevance of these differences seems doubtful.
In our study, as in other studies published in similar patient populations using conventional manometry,17,18 hypotensive LES tended to be more common in patients with Chagas disease than in healthy controls, but the relevance of hypotensive LES in the development of a more severe motility disorder in patients with Chagas disease is unknown, and future studies are needed to determine the specific relevance of isolated hypotensive LES.
The relevance of our findings in the clinical setting will depend on the association between the manometric abnormalities detected by HREM during the phase of latency of the disease, and the development of severe oesophageal damage in the future. This point is important because in the chronic phase of Chagas disease treatment has low efficacy, there is no clinical marker of early start of the disease that helps the clinician to determine which patients should be treated, and there is growing consensus considering treatment with benznidazole as the most appropriate in the early stages of the disease. Therefore, an early identification by HREM of tissue damage could lead to an early treatment and perhaps prevent the development of severe tissue damage and thereby improve the bad prognosis of the disease. Some authors have suggested that HREM could represent the most affordable way to notice early Chagas tissue damage since such an accurate assessment of harm in the oesophageal nervous plexus may be easier and surer than similar cardiologic studies. 12 In this respect, the advantages of HREM compared with oesophageal transit seem to be clear, taking into account that oesophageal transit is able to determine only advanced stages of the disease, when the nerve damage has produced irreversible structural damage beyond pharmacologic treatment.
To date there are no identified markers of progression of Chagas disease, and the degree of response to treatment cannot be assessed in the short term because serologic determinations take years to decrease antibody titles. 25 The findings of the present study open the possibility to perform new studies comparing HREM prior to and after a course of the World Health Organization-recommended two months’ treatment with benznidazole 26 and, therefore, to determine whether this methodology could help identify responders to treatment.
In conclusion, the present study shows that oesophageal motility disorders are common among immigrant patients infected with Chagas disease. Most of these alterations are minor peristaltic disorders detected when a sensitive tool such as HREM is used and otherwise mainly undetected during barium radiograph studies. Hence, in addition to barium oesophagogram examination, HREM should be considered to assess oesophageal damage in this specific group of patients.
Footnotes
Acknowledgments
The authors thank Conxa Julià and Pilar Bayo for technical support, and Irma Casas for help with statistical analysis.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Spanish Ministry of Health, Instituto de Salud Carlos III (grant numbers PI10/02135 and PI14/01703).