
Abstract
Background
Esophageal involvement in systemic sclerosis (SSc) carries significant morbidity and is empirically managed with domperidone, albeit with questionable efficacy. The oral 5-HT1A receptor agonist buspirone may enhance esophageal peristalsis and lower esophageal sphincter (LES) function in healthy volunteers.
Aim
We aimed to test the hypothesis that buspirone may exert a beneficial acute effect on esophageal motor dysfunction in symptomatic patients with SSc.
Methods
Twenty consecutive patients with SSc reporting esophageal symptoms underwent high-resolution manometry before and 30 minutes after administration of buspirone (10 mg). Ten other patients received domperidone (10 mg) and served as control group. Changes in LES resting and residual pressure, amplitude, duration, and velocity of distal esophageal body contractions were examined.
Results
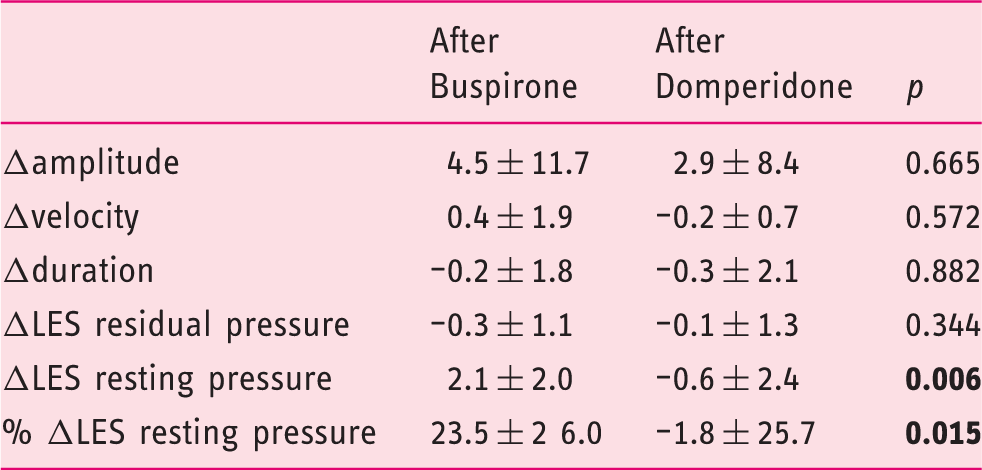
Esophageal hypomotility and hypotensive LES was found in 63% and 67% of patients, respectively. Demographic and clinical characteristics, including baseline manometric parameters, were comparable between groups. Resting pressure of LES increased after buspirone from 9.42 ± 2.6 to 11.53 ± 3.4 mmHg (p = 0.0002 by paired t-test), but not after domperidone; a trend for increase of amplitude of contractions was also observed after buspirone (p = 0.09). Comparison of the individual changes revealed that buspirone was superior to domperidone in enhancing LES pressure ( + 2.11 ± 2.0 versus –0.45 ± 2.3 mmHg, p = 0.006). No significant effects of either drug were noted on other examined parameters of esophageal function.
Conclusion
The beneficial acute effect of buspirone on impaired LES function associated with SSc suggests a role of 5-HT1A receptor-mediated interactions in these patients. Prospective studies to examine whether buspirone is of long-term therapeutic value for SSc-associated esophageal disease are warranted.
Introduction
Involvement of the gastrointestinal system in patients with systemic sclerosis (SSc) is second in frequency only to the skin. Εsophagus is the most commonly affected organ, occurring in up to 90% of patients with SSc.1–3 Clinically it is characterized by symptoms of gastroesophageal reflux disease (GERD) and of esophageal motor dysfunction. Typical symptoms of heartburn and dysphagia are reported by 80% of patients.4,5 However, symptoms do not always correlate with the extent of esophageal involvement as assessed by manometry, whereas some patients do not report any symptoms despite the presence of esophageal disease. 6
Manometry is the gold standard method for the assessment and detection of esophageal dysmotility in early stages of esophageal involvement in patients with SSc. The main manometric findings include the presence of ineffective or absent distal esophageal peristalsis and decreased lower esophageal sphincter (LES) pressure.5,7 The new technology of esophageal high-resolution manometry (HRM) is more sensitive to assess esophageal motility using multiple closely spaced pressure sensors, allowing a better assessment of LES and of the whole esophagus. 8
Currently, there are two main medical therapeutic options for SSc patients with esophageal involvement: (i) antisecretory agents, such as proton pump inhibitors (PPIs), which are effective for treating GERD, and (ii) prokinetic agents, including metoclopramide, cisapride, erythromycin, octreotide and domperidone, aiming to improve the SSc-associated esophageal dysmotility and GERD symptoms.9–12 It has been reported that metoclopramide and erythromycin may increase LES pressure in SSc patients, while cisapride has been shown to increase LES pressure and amplitude of distal esophageal body peristalsis. 9 However, use of these agents is restricted due to safety profile issues and administration route problems. Domperidone, a peripheral dopamine antagonist, is currently the most common prokinetic agent used in clinical practice in patients with SSc, although data on its effect on esophageal motility are conflicting.10,11
Recent data suggest that buspirone, an orally available 5-HT1A receptor agonist, enhances esophageal peristalsis and LES function in healthy subjects.13,14 Given the paucity of drugs that are able to enhance esophageal motor function in SSc, 15 we conducted an open-label, pilot study in 20 symptomatic SSc patients aiming to test the hypothesis that buspirone could exert a beneficial acute effect on esophageal motor dysfunction and LES pressure. We also studied the effects of domperidone in 10 additional symptomatic SSc patients.
Materials and methods
Study population
Thirty consecutive, consented patients (aged 52.3 ± 10.4 years, 26 women) who fulfilled classification criteria for SSc 16 and were able to perform HRM participated in this open-label, non-randomized study. Seven additional SSc patients did not consent to participating, while three did not complete the study. The only inclusion criterion was the presence of symptoms associated with esophageal involvement, such as heartburn, regurgitation, dysphagia and chest pain. Before esophageal manometry studies all patients filled out a symptom questionnaire used to characterize the severity of their symptoms. Severity of dysphagia, heartburn, regurgitation and chest pain was measured on a 10-point Likert scale ranging from 1 (absent) to 10 (very severe). Demographic data and characteristics of the disease were collected from the clinical charts. The study protocol was approved by the ethics committee of our hospital. Informed consent was obtained from all participating patients.
High-resolution manometry
All patients were fasted and studied in the supine position. None of the patients was on any prokinetics and PPIs were discontinued 48 h prior to the study. Esophageal manometry was performed with a water-perfused assembly with 22 pressure sensors (Solar GI HRM, MMS, Enschede, The Netherlands). The HRM catheter was passed trans-nasally and positioned to record from the hypopharynx to the stomach. The catheter was fixed in place by taping it to the nose. The manometric examination included a 30-s period to assess basal sphincter pressure and 10 swallows of 5 ml water. Double swallows were discarded and these were repeated.
All patients underwent a HRM study at rest. The study was repeated 30 min after an oral single-dose administration of 10 mg buspirone or 10 mg domperidone. We used buspirone 10 mg, as this is the current tablet formulation that is being reimbursed in our country. We recorded (i) amplitude, duration and velocity of contractions at the distal part (defined as the mean amplitude at 3 and 8 cm proximal to the LES upper border) of the esophagus and (ii) resting and residual LES pressure. The LES pressures were referenced to intragastric pressure and we reported the mean resting pressure values. All HRM tracings were interpreted by the same investigator, who was not blinded to the study medications. Esophageal hypomotility was considered when amplitude of distal contractions was ≤30 mmHg. Hypotensive LES was considered when LES resting pressure was ≤10 mmHg. For the Chicago classification isobaric contour<20 mmHg was considered as the cut-off for esophageal hypomotility. 17
Statistical methods
A Shapiro–Wilk’s test was used to examine the distribution of each variable. As all data analyzed were approximately normally distributed for both buspirone and domperidone group, paired-samples t-test was used to compare changes from baseline values following buspirone or domperidone administration while independent-samples t-test was used to investigate differences between the groups. Pearson correlation coefficient test was used to study possible correlations between symptoms and esophageal motility parameters. Values were expressed as mean ± SD. A p-value <0.05 was considered significant.
Results
Demographic characteristics, disease characteristics, symptoms, and manometric findings in 30 patients with SSc
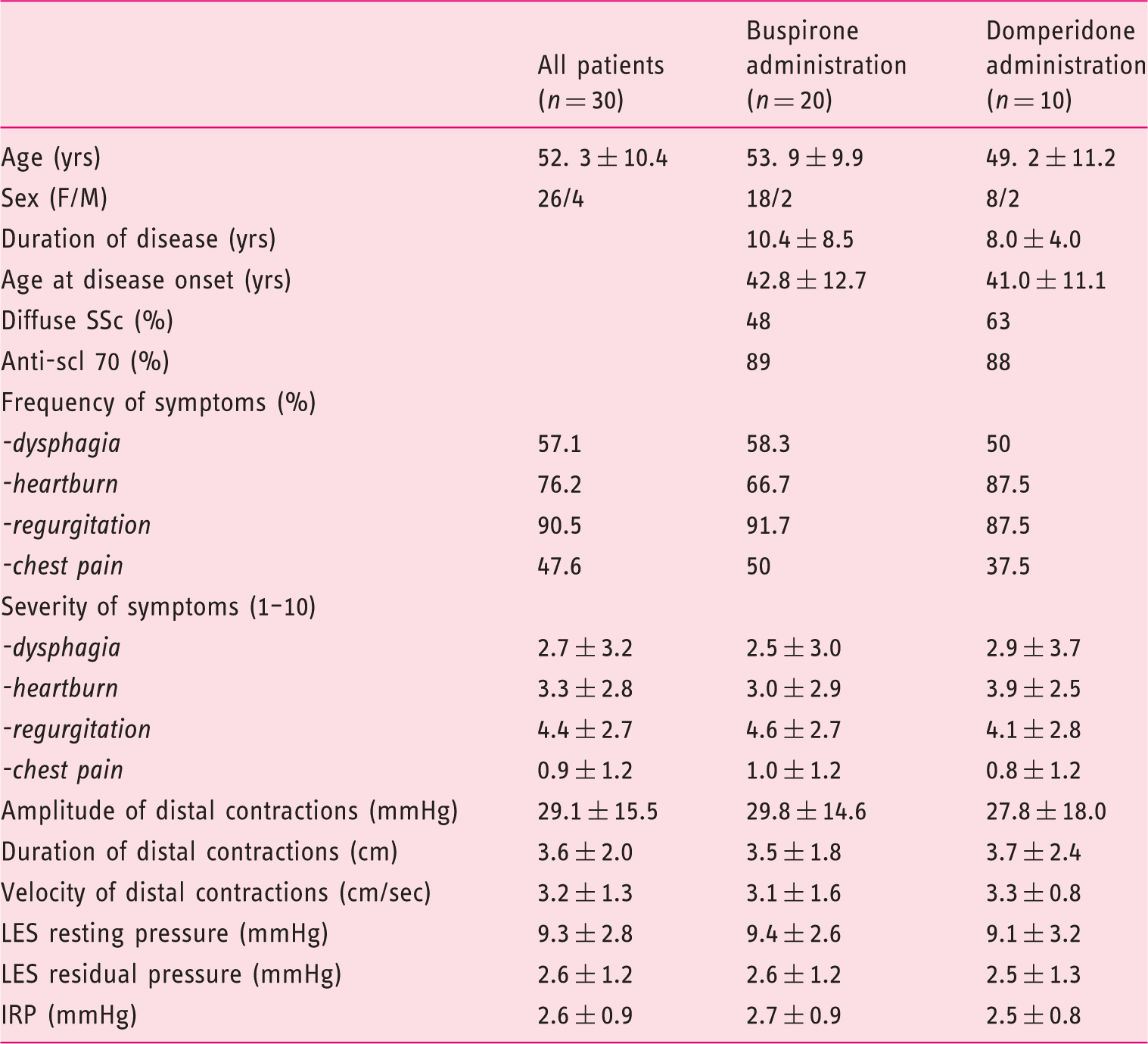
Regurgitation was reported by almost all patients (90.5%), while dysphagia was reported by 57.1% of patients (Table 1). Regurgitation was also the most bothersome symptom reported, followed by heartburn. No significant correlations between the severity of any of the reported subjective symptoms and the manometric findings were observed (data not shown).
Acute effects of buspirone
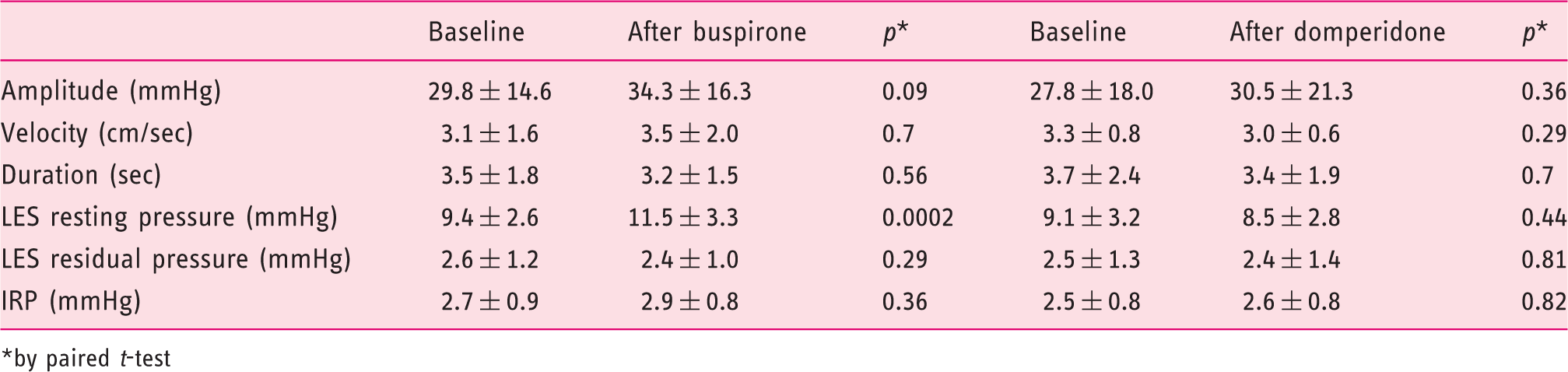
Following buspirone administration the LES resting pressure increased from 9.4 ± 2.6 to 11.5 ± 3.3, (p = 0.0002). Increases ranged from 1 to 5 mmHg (from 11.1% to 71.4%, accordingly) and were observed in 16 of 20 (80%) patients (Figure 1). Residual LES pressure did not change significantly (Table 2). However, buspirone administration failed to increase the duration and velocity of esophageal body contractions compared with baseline values, but a trend for increase of amplitude of contractions was observed (p = 0.09) (Table 2). Buspirone was well tolerated by all patients.
Change of LES pressure in each individual after administration of buspirone. Manometric parameters at baseline and after administration of buspirone and domperidone by paired t-test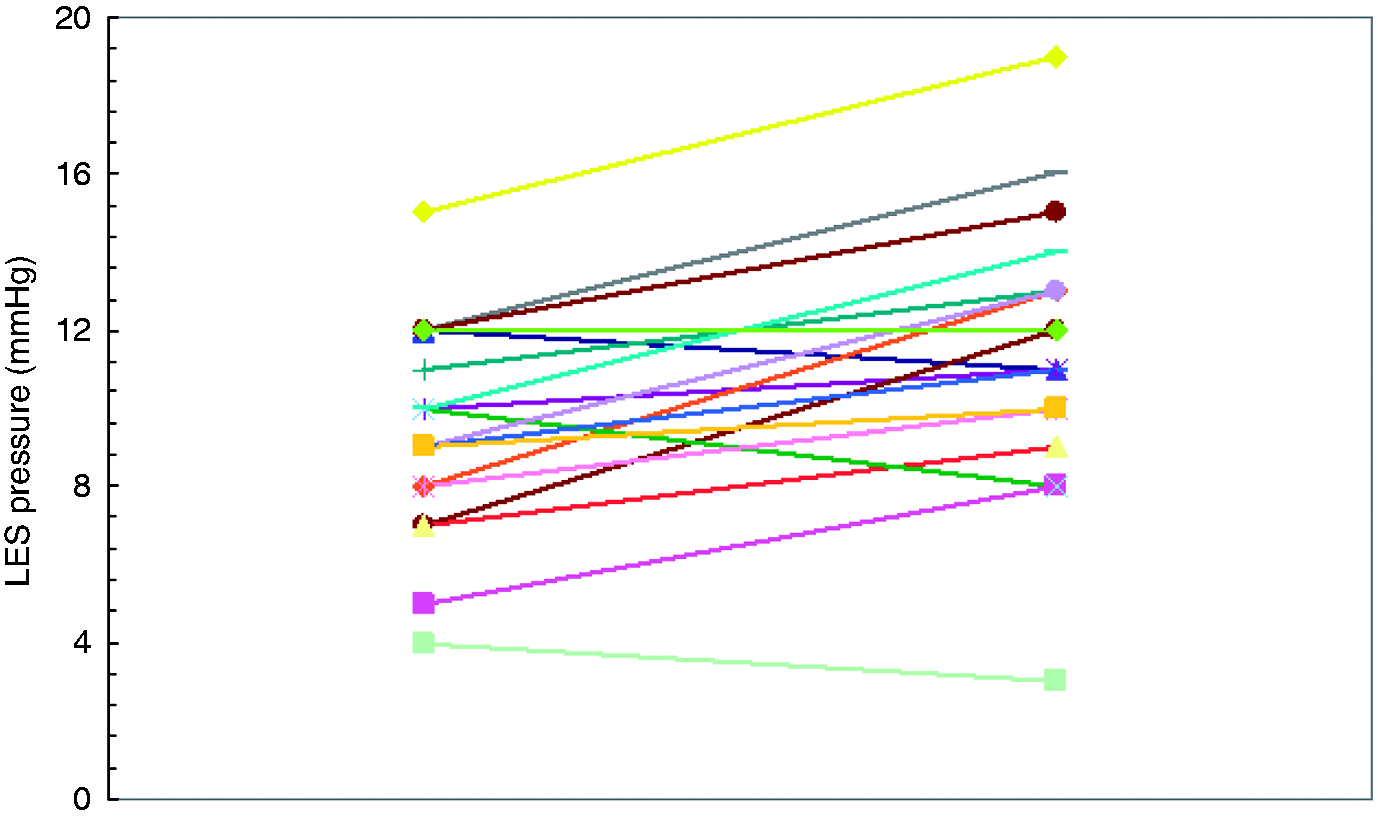
Acute effects of domperidone
Domperidone had no effect on the amplitude, duration and velocity of esophageal body contractions compared with baseline. In addition, it had no effect on LES resting and residual pressure (Table 2).
Comparison of changes observed after acute administration of buspirone versus domperidone
Discussion
The data of the present open-label, pilot study have shown that the 5-HT1A receptor agonist, buspirone, given orally in a single dose, significantly increases the LES resting pressure by 11.1% to 71.4% over the baseline values in 80% of the patients with SSc. On the contrary, domperidone failed to produce any significant effect on established esophageal motility dysfunction. It seems, therefore, that the reported effectiveness of domperidone stems from the acceleration of gastric emptying rather than from its effect on esophageal motor function.10,11,18
We used the new technique of HRM, allowing a better evaluation of esophageal motility and a more detailed investigation of the effect of drugs on esophageal motor function.8,19 Our data show that esophageal body abnormalities are present in 63% of SSc patients, and reduced LES resting pressure in 67% of them. These findings are in agreement with published studies showing esophageal dysmotility and reduced LES pressure in 67–83% and 39–83% of SSc patients, respectively.9,20,21
Esophageal peristalsis and LES function are under control of the autonomic and enteric nervous systems. Serotonin (5-hydroxytryptamine, 5-HT) is considered one of the putative neurotransmitters involved in esophageal motor function, and indeed a recent study showed that the mouse esophagus was endowed with rich serotonin-positive intrinsic innervations. 22 Several studies have evaluated the effects of 5-HT4 agonists on esophageal peristalsis and LES function in non-SSc patients, showing different results.23–27 However, use of these agents is restricted due to cardiac safety profile issues. Another serotonin receptor agonist, namely the 5-HT1A receptor agonist sumatriptan, may enhance esophageal peristalsis after subcutaneous administration in healthy subjects. 28 The effect of 5-HT1A receptor agonists was recently confirmed with the use of orally administered buspirone. Two studies in healthy volunteers showed that acute administration of buspirone had a strong stimulatory effect on esophageal peristalsis and LES function, suggesting a putative therapeutic role of buspirone in patients with ineffective esophageal motility.13,14
Since buspirone significantly enhances the LES resting pressure in SSc patients it is tempting to speculate a role for serotonin in the pathophysiology of esophageal dysfunction in patients with SSc. Pathophysiology of gastrointestinal dysmotility in scleroderma is multifactorial; decreased muscle function, increased wall stiffness, and motilin/VIP are all involved in the development of gastrointestinal symptoms.29–31 Thus, absence of stimulatory effect of buspirone administration on esophageal peristalsis in SSc patients in comparison with the strong stimulatory effect on healthy subjects could be justified by the fact that factors such as involvement of esophageal muscle might have a key role in disease progress. Serotonin exerts its effects through different receptors. The stimulatory effect of buspirone on esophageal motility suggests a putative role of 5-HT1A receptor-mediated interactions in these patients. Whether these effects are clinically relevant in terms of symptomatic improvement should be further evaluated. Theoretically, the strong stimulatory effect of buspirone on LES resting pressure could decrease the risk of regurgitation and reflux in patients with SSc, ameliorating symptoms related to esophageal involvement.
A methodological weakness of the present study is that it is not a randomized, placebo-controlled investigation. However, the buspirone and domperidone effects on LES resting pressure are compared with baseline measurements of the same patient. Another limitation of our study is that we cannot estimate whether the significant increase of LES resting pressure following buspirone administration is clinically relevant. Furthermore, we studied a challenging group of SSc patients having several medical disabilities due to the chronic nature of their disease, and it was difficult to recruit volunteers to our study.
In conclusion, our study using HRM confirmed that esophageal dysmotility may occur in up to two-thirds of SSc patients. Regurgitation is the most common symptom reported, but there is no correlation between severity of symptoms and manometric findings. We have also shown that acute administration of buspirone, but not of domperidone, increases the LES resting pressure of patients with SSc. Prospective studies are needed to investigate whether buspirone exerts a long-term beneficial effect in SSc-associated esophageal symptoms.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.