
Abstract
Ineffective esophageal motility (IEM) is the most frequently encountered esophageal motility disorder. Patients may present with a variety of symptoms, such as dysphagia, heartburn, odynophagia, and regurgitation. Over the past years, the landscape of esophageal motility testing has been revolutionized; however, our current treatment options for IEM still remain limited. Previous studies have suggested that buspirone, a serotonin receptor agonist, enhances esophageal peristalsis and lower esophageal sphincter (LES) function. Recent work provides the first evidence that buspirone may influence LES resting pressure in patients with systemic sclerosis. Future research should evaluate whether the beneficial effects of buspirone also apply to the broad clinical entity of esophageal dysphagia patients with IEM.
Keywords
Ineffective esophageal motility (IEM), also known as esophageal hypocontractility, is a manometric pattern characterized by ineffective swallows with poor bolus transit in the distal esophagus. In previous versions of the Chicago Classification of esophageal motility disorders, IEM has been characterized by breaks in the 20 or 30 mmHg isobaric contour.1,2 With the introduction of version 3.0 of the Chicago Classification, 3 ineffective swallows are defined on Clouse plots using the distal contractile integral (DCI) of less than 100 mmHg/s/cm (failed contraction) or less than 450 mmHg/s/cm (weak contraction), with more than 50% ineffective swallows constituting IEM. It is the most frequently encountered esophageal motor disorder in large clinical series. 4 IEM is observed in 20%–58% of patients who underwent esophageal manometry for various indications.5–7 IEM is highly prevalent in gastroesophageal reflux disease (GERD),7–9 and is often encountered in systemic conditions with esophageal involvement, such as scleroderma, or related connective tissue disorders, diabetes mellitus, and hypothyroidism. In our own experience, IEM (weak, absent, or frequent failed peristalsis) was found in 51% of 131 patients with symptoms of esophageal dysphagia referred for high-resolution manometry (unpublished observations). Patients may present with symptoms of dysphagia, heartburn, odynophagia, and regurgitation.
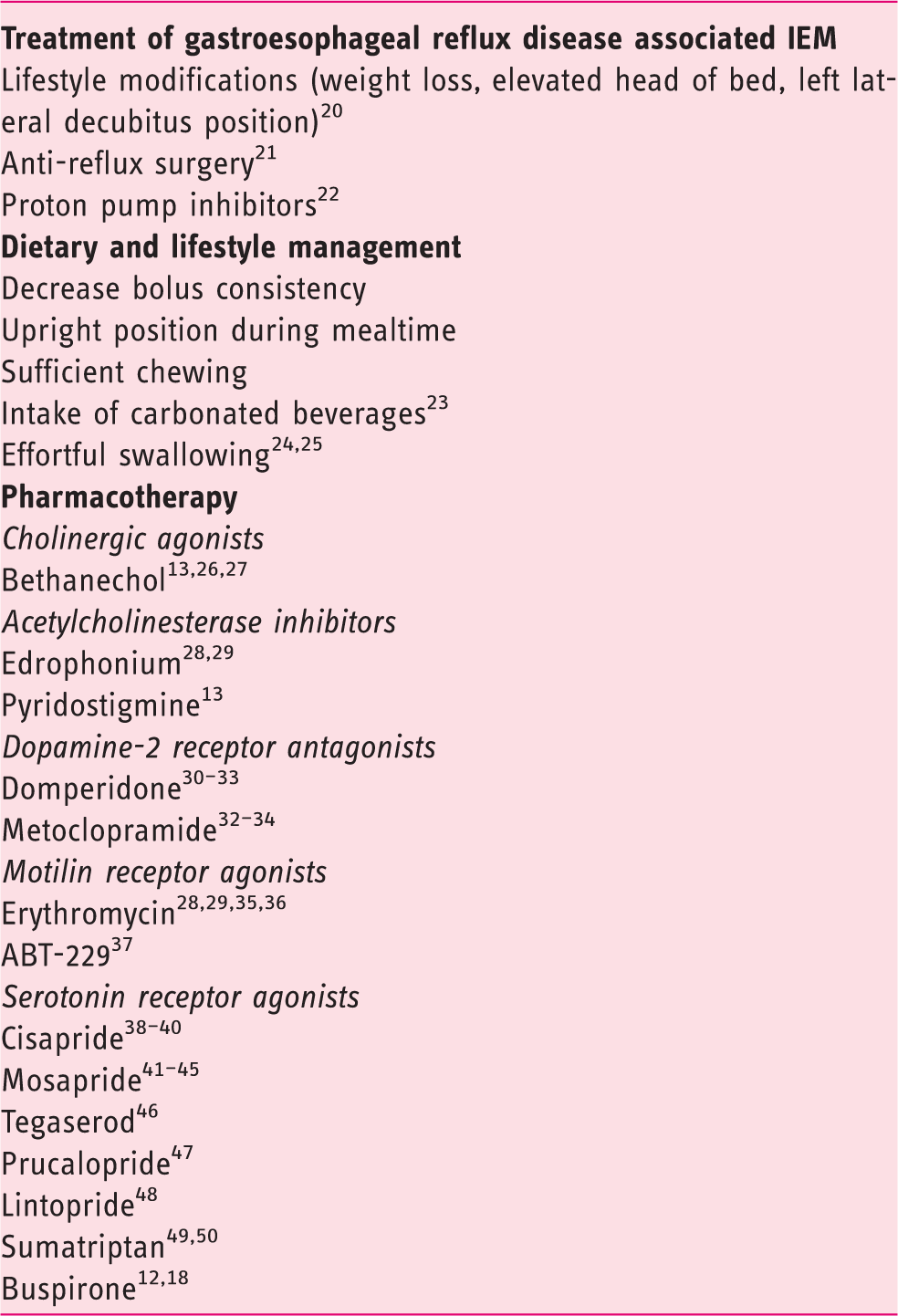
Overview of current treatment possibilities for ineffective esophageal motility (IEM)
Recently, two studies assessed the effect of buspirone, a serotonin receptor agonist, on esophageal motor function in healthy controls. Blonski and colleagues 13 studied the effect of oral administration of 20 mg of buspirone in ten healthy volunteers, and found significant increases in distal esophageal amplitude and residual lower esophageal sphincter (LES) pressure. Di Stefano and coworkers 12 have demonstrated significant increase in amplitude and duration of distal esophageal pressure waves, in addition to increased residual pressure and decreased duration of LES relaxation, after an oral dose of 20 mg of buspirone in 20 healthy volunteers. These results motivated additional studies on the clinical application of buspirone in patients with IEM. In this issue of the United European Gastroenterology Journal, Karamanolis and colleagues report the results of their open-label pilot study on the effect of buspirone on esophageal motility in patients with systemic sclerosis (SSc). 14 To our knowledge, this is the first study reporting the effect of buspirone in a patient cohort. The authors enrolled a consecutive series of 30 SSc patients with symptoms of esophageal involvement in a non-randomized fashion. Twenty patients underwent high-resolution manometry before and after administration of 10 mg buspirone. Ten patients received 10 mg of domperidone, a peripheral dopamine antagonist, a commonly used prokinetic agent in the clinical management of patients with SSc. Changes in amplitude, duration, and velocity of distal esophageal body contractions, lower esophageal sphincter (LES) resting pressure, and LES residual pressure, were assessed unblinded to the study medication. The authors reported a significant increase in LES resting pressure (p = 0.0002), and a non-significant trend (p = 0.09) toward increased amplitude of esophageal body contractions after acute administration of buspirone, but not of domperidone. The authors concluded that “the beneficial acute effect of buspirone on impaired LES function associated with SSc suggests a role of 5-HT1A receptor-mediated interactions in these patients”. 14
The study by Karamanolis and colleagues 14 provides the first evidence that buspirone may exert a beneficial effect on LES resting pressure in SSc patients with esophageal involvement. 14 The study found only a trend towards increased amplitude of esophageal body contractions, unlike the previous healthy volunteer studies. This may relate to the lower oral buspirone dose administered in this study (10 mg vs 20 mg in the healthy volunteers study). It is also important to consider that the pathophysiology of gastrointestinal dysmotility in scleroderma is multifactorial, with three stages described in the development of esophageal involvement: neuropathy, myopathy, and fibrosis. 10 While pharmacological therapy may help to overcome neuropathic and to some extent myopathic dysfunction, it is unlikely to alter fibrosis, whose presence may down-grade the efficacy of buspirone.
The Karamanolis study 14 is the first one to assess the effect of buspirone on esophageal function in SSc, paving the way to investigate the possible beneficial effect of buspirone in other systemic diseases with esophageal involvement, such as idiopathic IEM, diabetes mellitus, and hypothyroidism. Future randomized placebo-controlled trials of prolonged administration are needed to further establish the potential therapeutic effect of buspirone in these patients. The anxiolytic properties of buspirone may provide additional benefit in patients with psychosocial comorbidity, as suggested in some functional esophageal disorders. 15 This strongly motivates further evaluation of the use of buspirone in patients with esophageal hypersensitivity.
Buspirone is an anxiolytic drug available for oral administration with well-established safety, initially developed for clinical use in the treatment of depression and generalized anxiety disorder (GAD). 16 The most common side effects observed in placebo-controlled clinical trials include dizziness, nausea, headache, nervousness, light-headedness, and agitation. The underlying mechanism of action is not clear-cut; however, it is suggested that its main neuropharmacological effects are mediated via serotonin 5-HT1A receptors. Buspirone is a partial agonist for these receptors, as well as being an antagonist for dopamine D2 autoreceptors, with some evidence of a weak affinity to 5-HT2 receptors. 16 In the enteric nervous system, 5-HT1A receptors activation decreases the release of acetylcholine from excitatory motor neurons, 17 and, in agreement with this pathway, buspirone has been shown to relax the proximal stomach and slow down gastric emptying. 18 On the other hand, in the central nervous system of the guinea pig, buspirone was reported to stimulate the release of acetylcholine in the hippocampus, and behavioral changes through activation of 5-HT1A receptors. 19 The effects on esophageal motility are reminiscent of cholinergic activation, but none of the available human studies allow elucidation of the site of action of buspirone when stimulating esophageal motility.
While promising, the clinical application of buspirone should probably await additional studies. Future research should evaluate whether the beneficial effects of buspirone reported in this issue of the United European Gastroenterology Journal 14 also apply to the broad clinical entity of esophageal dysphagia patients with IEM, as this would be a welcome, attractive treatment for the most frequently encountered esophageal motility disorder, which currently holds very limited treatment options.
Footnotes
Conflict of interests
None of the authors have any financial, professional or personal conflicts to disclose that are relevant to this manuscript.