
Abstract
Background
The prevalence of gastrointestinal involvement in systemic sclerosis is higher than 75%. The estimated prevalence of fecal incontinence varies from 22% to 77%, but suffers from recruitment bias and patient reluctance. Our goal was to evaluate the prevalence of fecal incontinence in systemic sclerosis, and to identify associated risk factors.
Methods
Patients were recruited in the referral systemic sclerosis network of the Lyon University Hospitals, using self-administered questionnaires including constipation, fecal incontinence and Bristol Stool scales, quality of life, anxiety and depression. The cohort was compared with the historical ORALIA cohort that established the prevalence of fecal incontinence in the general population of the Rhône-Alpes region (France).
Results
Seventy-seven patients were included (mean age: 60 years, range: 32–84), and 86% were female. These were compared to 153 ORALIA individuals matched for age and sex. Fecal incontinence was present in 38% of patients and 6% of the general population. A longer duration of systemic sclerosis was the only characteristic associated with fecal incontinence. Abnormal stool consistency was more frequent in patients with fecal incontinence.
Conclusion
Fecal incontinence and abnormal stool consistency are common in systemic sclerosis and should be systematically addressed.
Introduction
Gastrointestinal involvement is extremely frequent in systemic sclerosis (SSc), with an overall prevalence estimated to be between 75% and 99%.1,2 The most frequent complaints are related to esophageal motor disorders (gastro-esophageal reflux disease, dysphagia), constipation, dyschesia, diarrhea, and fecal incontinence. 3 The prevalence of fecal incontinence (FI) has been estimated to be between 22% and 77%.1,4–8 These estimations may suffer from recruitment bias (patients seen at gastroenterology clinics for example), and patients’ reluctance to talk about this embarrassing symptom. The pathophysiology of FI in SSc is thought to be mainly related to alteration of the connective tissue and atrophy of the internal anal sphincter.9–11 However, other causes of FI, such as associated constipation or diarrhea, may also be involved in SSc.2,3
The objective of the present study was thus to investigate the prevalence of FI in a cohort of SSc individuals followed by the SSc regional referral network of the Lyon teaching hospitals (Hospices Civils de Lyon) located in the Rhône-Alpes region of eastern France, and to identify factors associated with FI symptoms. We also compared the prevalence of FI and characteristics of the SSc patients with a historical cohort (ORALIA) that evaluated FI prevalence in the general population of the Rhône-Alpes region. 12
Materials and methods
Participants
Between December 2012 and December 2015, a self-administered questionnaire was given to all patients with SSc seen through the referral SSc network of the Hospices Civils de Lyon. There were no exclusion criteria. All patients signed an informed consent.
Data collection
Firstly, all patients completed four self-administered questionnaires: the KESS constipation scale, the Jorge and Wexner FI score, the Gastro-Intestinal Quality of Life Index (GIQLI), and the Hospital Anxiety and Depression scale (HAD), and one stool calendar for 14 days with the Bristol Stool Scale item.13–17 The demographic characteristics were extracted from clinical files of responding patients.
Secondly, this SSc cohort was compared with the historical cohort ORALIA that included 706 individuals among the general population in order to estimate the prevalence of FI in 2004 in the Rhône-Alpes region. 12 Participants were matched by sex and age (by 10-year periods) with the following ratio: one SSc patient:two controls. Because of this sex and age stratification, this 1:2 design was decided in order to include the same number of controls relative to SSc patients (larger numbers of controls would have skewed the age and sex matching).
Data analysis
The population was described in terms of demographic data, duration of SSc, presence of limited or diffuse SSc type, esophageal involvement, pulmonary arterial hypertension, interstitial lung disease, previous gynecological surgery, and number of vaginal deliveries. FI was defined by a Jorge and Wexner score ≥ 5/20.
Specific questions focusing on previous FI symptoms and medical management were evaluated. The following questions were used: “Did you already suffer from fecal incontinence?”, “If yes, did you already talk about this problem with a medical doctor?”, “If yes, were further investigations and/or medical and biofeedback treatments prescribed?” For the stool calendar data, the number of defecations and fecal leaks per week were analyzed. Stool consistency was analyzed based on the Bristol Stool Scale and categorized into two groups: (liquid/mushy (Bristol 5 to 7) or with an important variability (Bristol 1 or 2 to 6 or 7)) or (hard/normal (Bristol 1 to 4)). For the SSc and general population (ORALIA) comparison, the following criteria were available for both populations: gender (matched), age (matched), body mass index (BMI), previous gynecologic surgery, number of vaginal deliveries, Jorge and Wexner FI score.
Statistical analysis
Data were expressed as mean or median (range or interquartile range, IQR). Comparisons between groups were performed using Chi-square, Fisher’s exact test, and one-way analysis of variance when appropriate. A p value < 0.05 was considered as significant.
Results
Characteristics of the 77 patients with systemic sclerosis. Data are expressed as median (IQR) unless otherwise is mentioned.
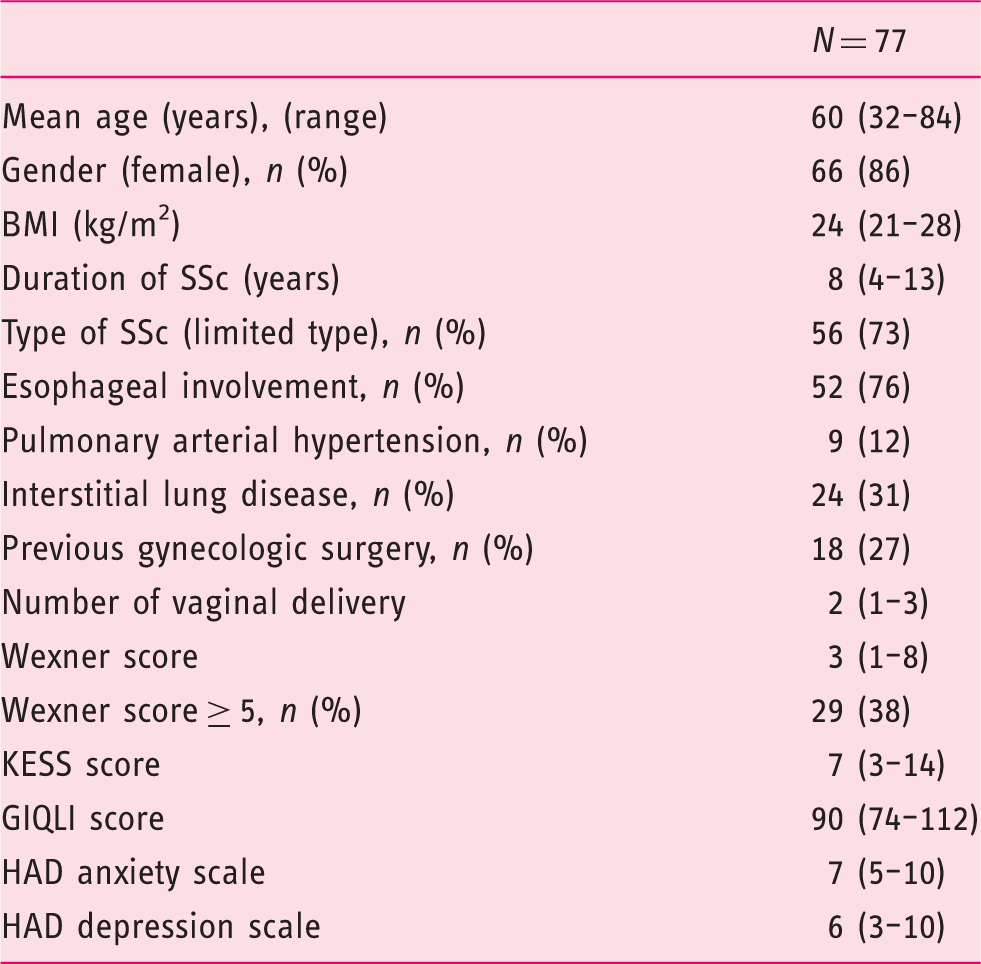
IQR: interquartile range; BMI: body mass index; SSc: systemic sclerosis; GIQLI: Gastro-Intestinal Quality of Life Index; HAD: Hospital Anxiety and Depression.
Scleroderma patients with and without FI
Comparison between patients with or without FI.
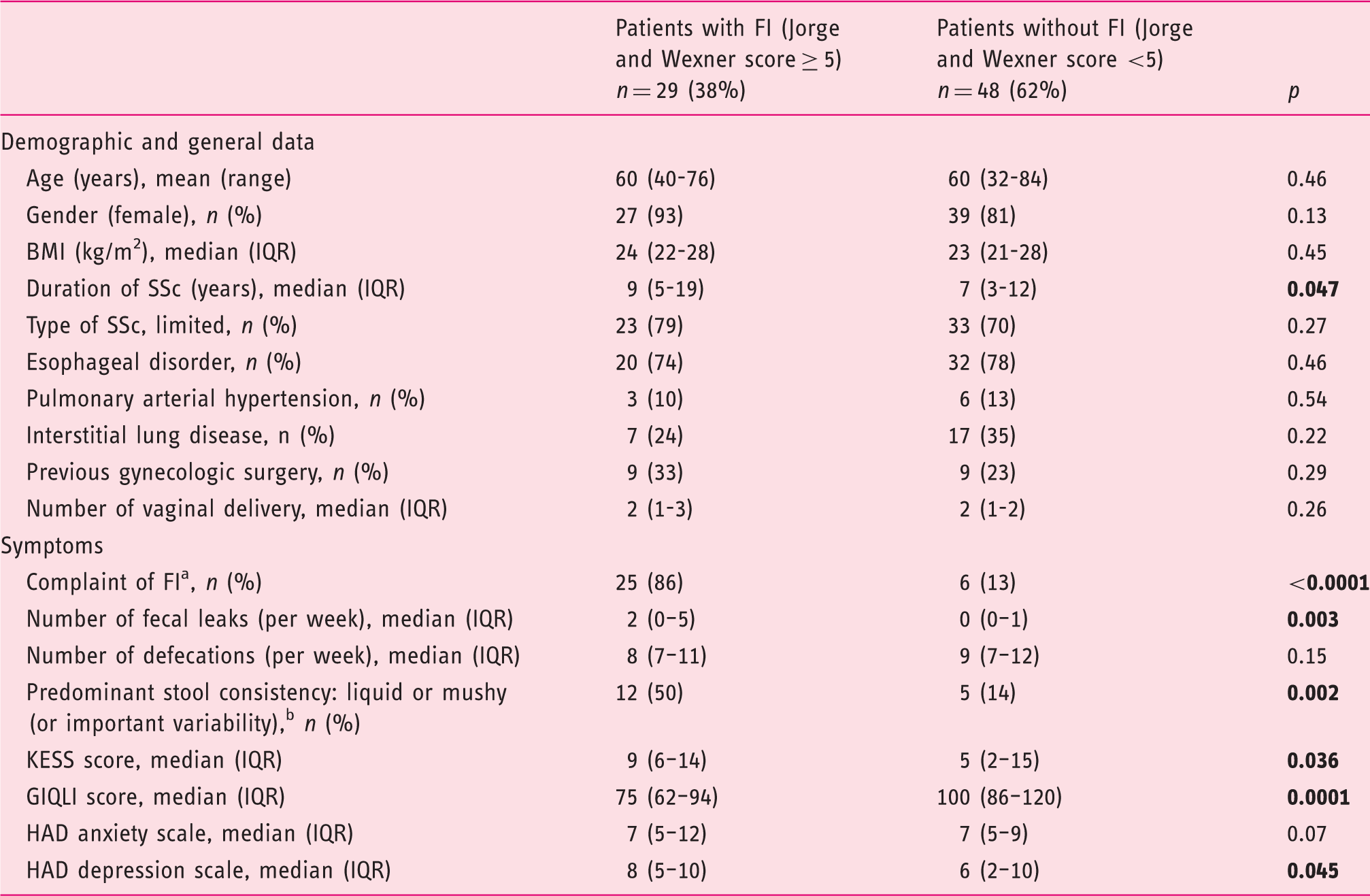
BMI: body mass index; IQR: interquartile range; SSc: systemic sclerosis; FI: fecal incontinence; GIQLI: Gastro-Intestinal Quality of Life Index; HAD: Hospital Anxiety and Depression Boldface values stand for p less than 0.05. aCorresponds to the answer to the question: “Did you already suffer from fecal incontinence disorder?” bStool consistency frequently hard with separate lumps and frequently mushy or liquid.
Among the 31 patients (40%) who reported past or present FI symptoms, 23 (74%) had already reported this problem to their physician, 10 (32%) had undergone functional anorectal testing, and six (20%) had undergone medical and/or biofeedback therapy.
Prevalence of FI in SSc compared to the regional general population (ORALIA cohort)
Comparison between systemic sclerosis and general population (matched on age and gender).
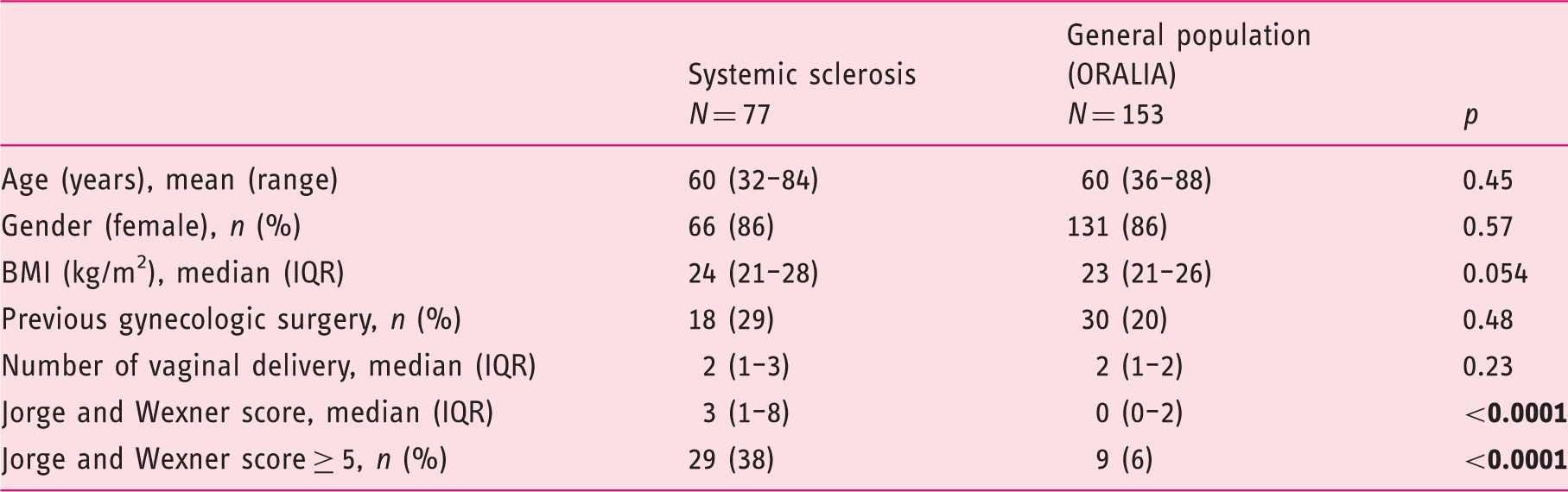
BMI: body mass index; IQR: interquartile range. Boldface values stand for p less than 0.05
Discussion
This study confirms the high prevalence of FI in an SSc population, estimated to be 38%, vs 6% in the general population of the Rhône-Alpes region of France, matched for age and sex. The only risk factor related to SSc characteristics predictive of FI was duration of disease. According to the stools calendar, abnormal stool consistency, especially liquid/mushy stools, was significantly more frequently encountered in patients with FI than in those without.
The epidemiology of FI in SSc has been evaluated in several studies, with variable results.1,4–8 We recruited patients within the SSc referral network of our institution, whether they were referred for gastrointestinal involvement or for other reasons. Our results are similar to those of Martin et al. that found a prevalence of FI of 25%. 8 Higher FI prevalence (77% in a recent study by Luciano et al.) may be due to recruitment bias linked to a gastrointestinal single-center study 7 .
Compared to the historical cohort ORALIA, and among individuals matched with SSc for age and sex, the prevalence of FI in SSc appears to be more than six-fold that found in the general population. We chose this historical cohort for several reasons: First, the ORALIA cohort was sampled in the Rhône-Alpes region of France, where most of the SSc patients were recruited; second, the same methodology and self-administered questionnaires were used in both cohorts; and finally, it is important to note that these two groups were equivalent also for other known risk factors of FI such as past gynecologic surgery, vaginal deliveries, and BMI. This cohort identifying the prevalence of FI in the general population of the Rhône-Alpes region thus constituted an excellent control group to evaluate the FI risk related to SSc. In the attempt to identify risk factors for the high prevalence of FI in SSc, we, as others, did not find factors related to a specific type of SSc.1,7 The present study found a longer SSc disease duration in the group of patients with FI. This factor has also been found in other studies that looked for this variable.7,8 Another parameter more frequently found in the group of SSc with FI was the high prevalence of abnormal stool consistency, including more liquid or mushy stools, or bowel habits with important variability (hard stools alternating with liquid stools). The association between liquid stools and FI in SSc has previously been suggested. 18 This may be related to intestinal bacterial overgrowth, a frequent situation in SSc with digestive involvement, 3 but this was not systematically investigated in the present cohort. Constipation is also frequent in SSc, and overflow FI may be present in patients with important variability of their bowel movements. The data suggest that constipation may be more frequent in SSc with FI, evidenced by the significantly higher values of the KESS score in the group of patients with FI compared to those without. The negative impact of FI on quality of life is also clear in this SSc cohort, with a significantly lower GIQLI score, and higher HAD anxiety and depression scores. This has already been demonstrated in large cohorts of FI and confirms the need to identify this debilitating symptom and to find therapeutic solutions.6,19 Indeed, despite numerous medical consultations in a referral SSc network, a quarter of our SSc patients who already complained of FI, never talked about this symptom with a medical doctor, and two-thirds did not undergo any supplementary examination. This observation should modify the management of SSc to include a systematic evaluation of FI, at least with the use of standardized self-administered questionnaires, and referral to a specialized gastroenterological consultation whenever this problem is detected.
There are some limits to this study. The number of SSc patients agreeing to participate to the study represents only a portion of the total number of SSc patients followed in the network: A recruitment bias may have potentially increased the observed prevalence of FI. In order to better understand the pathophysiological mechanisms implied in the development of FI in SSc patients, anorectal manometry (ARM) and endoanal ultrasound (EUS) results would have been of interest. Data were not in sufficient numbers (only 16 ARMs and one EUS were performed in the group of SSc patients) and we thus decided not to report them. This can be explained by the recruitment in non-digestive expert centers, and by the observational nature of the study.
In conclusion, the present study confirms the high prevalence of FI in SSc irrespective of type, especially after a long duration of the disease. FI symptoms are frequently associated with altered bowel habits and constipation, probably indicating the overall impact of SSc on the digestive tract. SSc patients appear reluctant to talk about this embarrassing symptom with physicians, and even when they do so, may not find an adequate response. A more systematic approach of this symptom negatively affecting quality of life should be recommended.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This work was supported by a research grant from the French Association of Patients Suffering from SSc (Association des Sclérodermiques de France, ASF).