
Abstract
Background
Esophageal squamous cell carcinomas (ESCCs) are often accompanied by head and neck second primary tumors (HNSPTs). The prognosis of patients with an additional HNSPT is worse compared with patients with only ESCC. Therefore, early detection of HNSPTs may improve the overall outcome of patients with ESCC.
The purpose of this study was to investigate the yield of endoscopic screening for HNSPTs in patients with primary ESCC.
Methods
We conducted a systematic literature search of all available databases. Studies were included if ESCC patients were endoscopically screened for HNSPT. The primary outcome was the pooled prevalence of HNSPTs.
Results
Twelve studies, all performed in Japan, were included in this systematic review with a total of 6483 patients. The pooled prevalence of HNSPTs was 6.7% (95% confidence interval: 4.9–8.4). The overall heterogeneity was high across the studies (I2 = 89.0%, p < 0.001). Most HNSPTs were low stage (85.3%) and located in the hypopharynx (60.3%). The proportion of synchronous (48.2%) and metachronous (51.8%) HNSPTs was comparable.
Conclusion
Based on our results, HNSPT screening could be considered in patients with primary ESCC. All studies were performed in Japan; it is therefore not clear whether this consideration applies to the Western world.
Key summary
The prognosis of patients with esophageal squamous cell carcinoma (ESCC) and an additional head and neck second primary tumor (HNSPT) is worse than patients with only ESCC. Early detection of HNSPT may improve patient outcome. The pooled prevalence of HNSPT in patients with ESCC is 6.7%. Most HNSPTs are low stage (85.3%) and located in the hypopharynx (60.3%). HNSPT screening could be considered in patients with primary ESCC. Western screening studies are needed, since all studies have been performed in Japan.
Introduction
Both esophageal and head and neck (HN) cancer are common malignancies worldwide.1,2 Esophageal squamous cell carcinoma (ESCC) is the most common histologic type in the esophagus. 3 Patients with ESCC frequently develop second primary tumors (SPTs) in the upper aerodigestive tract, most often in the HN region, but also in the esophagus and lungs.4,5 The presence of SPTs can be explained by the “field cancerization” theory: Premalignant epithelial changes can occur because of chronic local exposure to common carcinogens, such as alcohol and tobacco, which contributes to the development of syn- and metachronous SPTs. 6 An important risk factor in Western countries for the development both of ESCC and SPTs is alcohol.7,8
Head and neck second primary tumors (HNSPTs) in patients with primary ESCC are reported to be up to 7% in retrospective studies.4,5 The prognosis and survival of patients with esophageal cancer (EC) is poor because most ECs are diagnosed in advanced stages, when definitive cure is most often not achievable. 9 The long-term prognosis is even worse in patients with an additional HNSPT compared with ESCC alone (five-year survival rate of 9.2% vs 21.0%). 10 This poor prognosis makes early detection of HNSPTs vitally important, especially for ESCC patients with low-stage tumors that could be treated endoscopically, since they have a considerably higher five-year survival rate. 11
Different endoscopic techniques for HN cancer screening have been studied. Although Lugol chromoendoscopy is often used in the esophagus to detect dysplastic mucosal lesions, it is known to cause side effects in the HN region such as chest pain and aspiration. 12 Narrow-band imaging (NBI) seems to be the best technique for the detection of HNSPTs in patients with primary ESCC. 13 The HNSPT detection rate is significantly higher using NBI (sensitivity 100%, specificity 97.5%) compared with only white-light endoscopy (WL). 13 The sensitivity of fluorodeoxyglucose–positron-emission tomography/computed tomography (CT) for the detection of HNSPTs is 61.5%; more HNSPTs have been detected by endoscopy. 14
The European Society for Medical Oncology Clinical Practice Guidelines for EC recommends endoscopic screening of the HN region and trachea-bronchoscopy to detect SPTs in the upper aerodigestive tract in all ESCC patients with chronic tobacco and alcohol consumption. 15 However, no Western screening studies have been published to date. The Japanese EC guidelines recommend appropriate diagnostic measures of other organs (HN, stomach, large intestine) after treatment of ESCC because of the risk of developing SPTs. 16 However, no specific screening recommendations (i.e. diagnostic method and time of screening) are mentioned. 16
We have performed a systematic review and meta-analysis of studies that investigated the use of endoscopic screening for the detection of HNSPTs in patients with primary ESCC. Our primary objective was to investigate the yield of endoscopic screening for HNSPTs in patients with primary ESCC. Our secondary objectives were to investigate whether there is evidence to justify endoscopic HN screening in primary ESCC patients in the Western world, and to investigate whether screening should be performed synchronously or metachronously.
Materials and methods
Literature search and selection criteria
A systematic literature search was performed in collaboration with the medical library of the Erasmus University Rotterdam, the Netherlands, in February 2019, with no limit on publication date. The search was performed in PubMed, Embase, Medline, Cochrane Central, Google Scholar and Web of Science databases. The full electronic search strategy for the Embase database is provided in Supplementary Appendix 1. The search was limited to English studies performed on humans. After removing duplicate citations, the remaining articles were reviewed based on title and abstract by two independent reviewers (S.E.M.V. and O.B.). Subsequently, the full text of the remaining articles was screened by the same authors and discrepancies were discussed mutually. If there was no agreement, a third party was involved (A.D.K.). Studies were included if patients with primary ESCC were endoscopically screened for HNSPTs. Studies were excluded if patients with primary head and neck squamous cell carcinoma (HNSCC) were screened for esophageal SPTs, since we investigated the yield of HNSPT screening in patients with primary ESCC. Moreover, these studies are already included in a systematic review about screening for esophageal SPT in patients with primary HNSCC. 17 Studies without full text, case reports, reviews, and studies in which only imaging techniques were used to detect HNSPTs were excluded. References of the retrieved studies were manually screened to locate additional studies.
Study quality
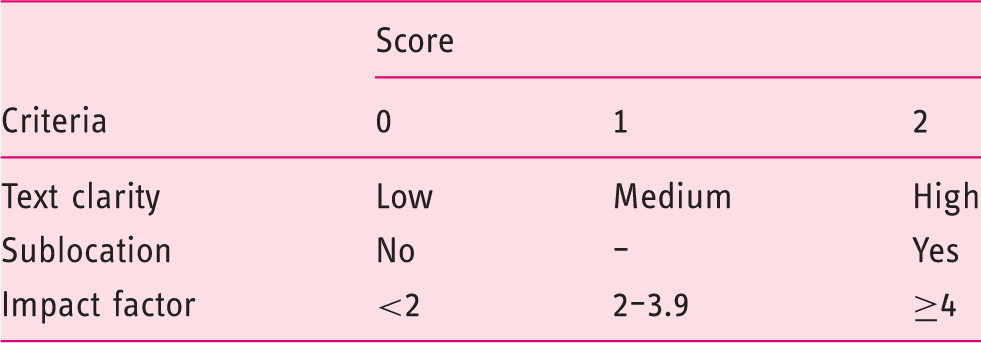
Relevance criteria.
Data extraction and outcome parameters
Data from included studies were summarized as a Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist and flowchart. 19 The primary outcome was the prevalence of diagnosed HNSPTs. An HNSPT was defined as a lesion in the HN region classified as carcinoma in situ or carcinoma. With NBI, these lesions can be described as well-demarcated brownish areas without magnification, irregular microvascular patterns, and increased intraepithelial papillary capillary loops. 20 Secondary outcomes were recorded when possible: (1) HNSPT prevalence per sublocation (upper, middle and lower esophagus) and per tumor stage (0 to IV according to the Vienna classification of gastrointestinal epithelial neoplasia) of the primary ESCC, (2) synchronously (≤6 months after diagnosis of primary ESCC) or metachronously (>6 months after diagnosis of primary ESCC) diagnosed HNSPTs and (3) tumor stage and sublocation of HNSPTs. 21 Other characteristics of the studies were also recorded: first author, publication year, study design, size and country of the study population.
Statistical analysis
For each study, the HNSPT prevalence was calculated (total number of HNSPTs divided by the total population that was screened). The standard error (SE) was calculated from the prevalence using the following formula:
Results
Study selection and quality assessment
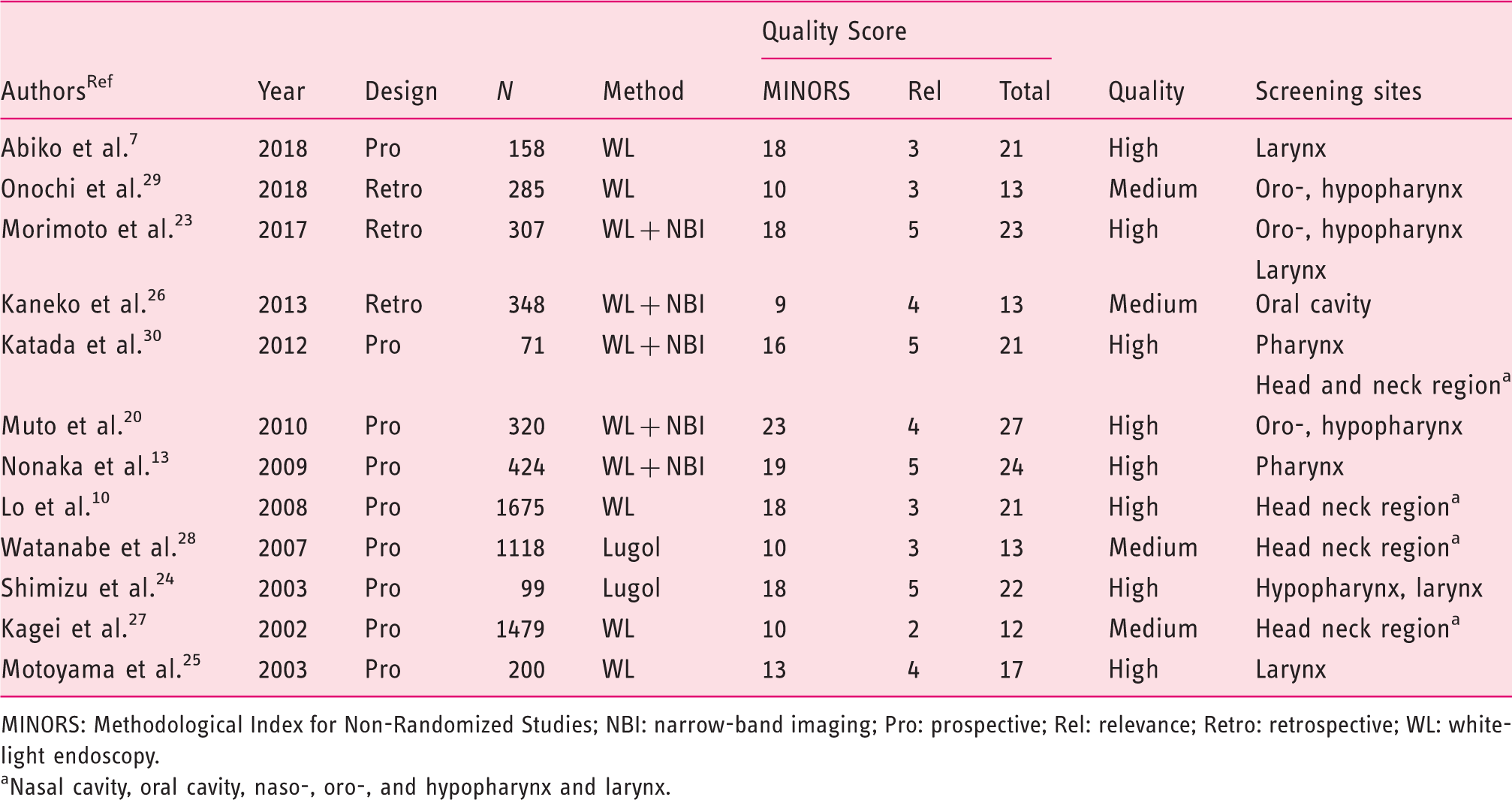
The study selection process and eligibility assessment are outlined in Figure 1. The literature search identified 4537 citations. After screening, 148 articles were examined by full-text review for their eligibility by two reviewers (S.E.M.V. and O.B.). Discrepancies were discussed mutually without any final disagreements. One additional study was included after screening the references. Twelve studies were included in our systematic review.7,10,13,20,23–30 Exclusion reasons are shown in Figure 1. All 12 included studies qualified as medium or high (Table 2). The relevance criteria score ranged between 0 and 5 points (maximum possible score is 6). The MINORS criteria score ranged from 9 to 23 points (maximum possible score of 24).
Study selection process. Study characteristics and quality score of all 12 studies. MINORS: Methodological Index for Non-Randomized Studies; NBI: narrow-band imaging; Pro: prospective; Rel: relevance; Retro: retrospective; WL: white-light endoscopy. Nasal cavity, oral cavity, naso-, oro-, and hypopharynx and larynx.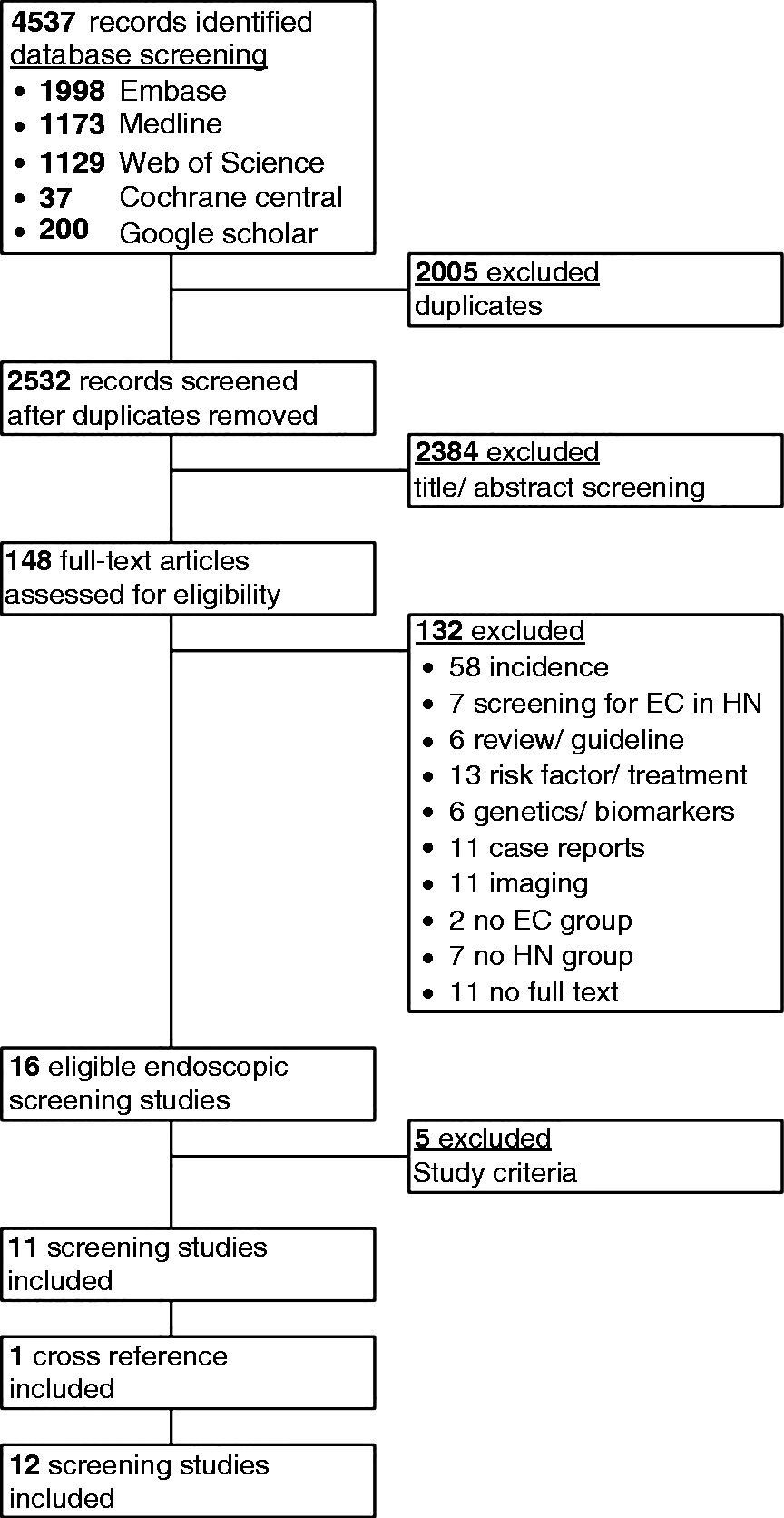
Study characteristics
The study characteristics are reported in Table 2. All studies were performed in Japan and published between 2002 and 2018. Nine of the 12 studies (75%) collected their data prospectively7,10,13,20,24,25,27,28,30 and three (25%) retrospectively.23,26,29 The total number of included patients was 6483 (median, 313; range, 71–1674). In two studies Lugol iodine was used for screening of the HN region.24,28 In five other studies both WL and NBI were used for screening.13,20,23,26,30 In the remaining five studies, only WL was used for screening.7,10,25,27,29 In only four studies, the entire HN region was screened.10,20,27,28,30 Screening was limited to the pharynx and larynx, sublocations known to be at an increased risk, in most other studies. Eleven of the 12 studies screened only patients with ESCC.7,10,13,20,23–26,28–30 One study screened patients with both ESCC (93%) and esophageal adenocarcinoma (7%). 27 In total, 98% of the esophageal tumors were squamous cell carcinomas and 2% adenocarcinomas. Screening was performed by an otolaryngologist or head and neck surgeon in 5/12 included studies.7,24,25,27,28 Screening was performed by a gastroenterologist in 2/12 studies.20,29 In these two studies, only the oropharynx and hypopharynx were screened. In 5/12 included studies, however, it was not clearly reported who performed the screening endoscopy of the head and neck region (otolaryngologist or gastroenterologist).10,13,23,26,30
Pooled SPT prevalence
The prevalence of HNSPTs in patients with ESCC is shown for each study in Figure 2. In total, 353/6483 patients were diagnosed with HNSPT. Meta-analysis with a random-effect model was used to calculate the pooled prevalence since the I2 was 89.0%. The pooled prevalence for HNSPTs of the 12 included studies was 6.7% (95% CI: 4.9–8.4%) (Figure 2).
Forest plot of prevalence of head and neck second primary tumors in patients with esophageal squamous cell carcinoma.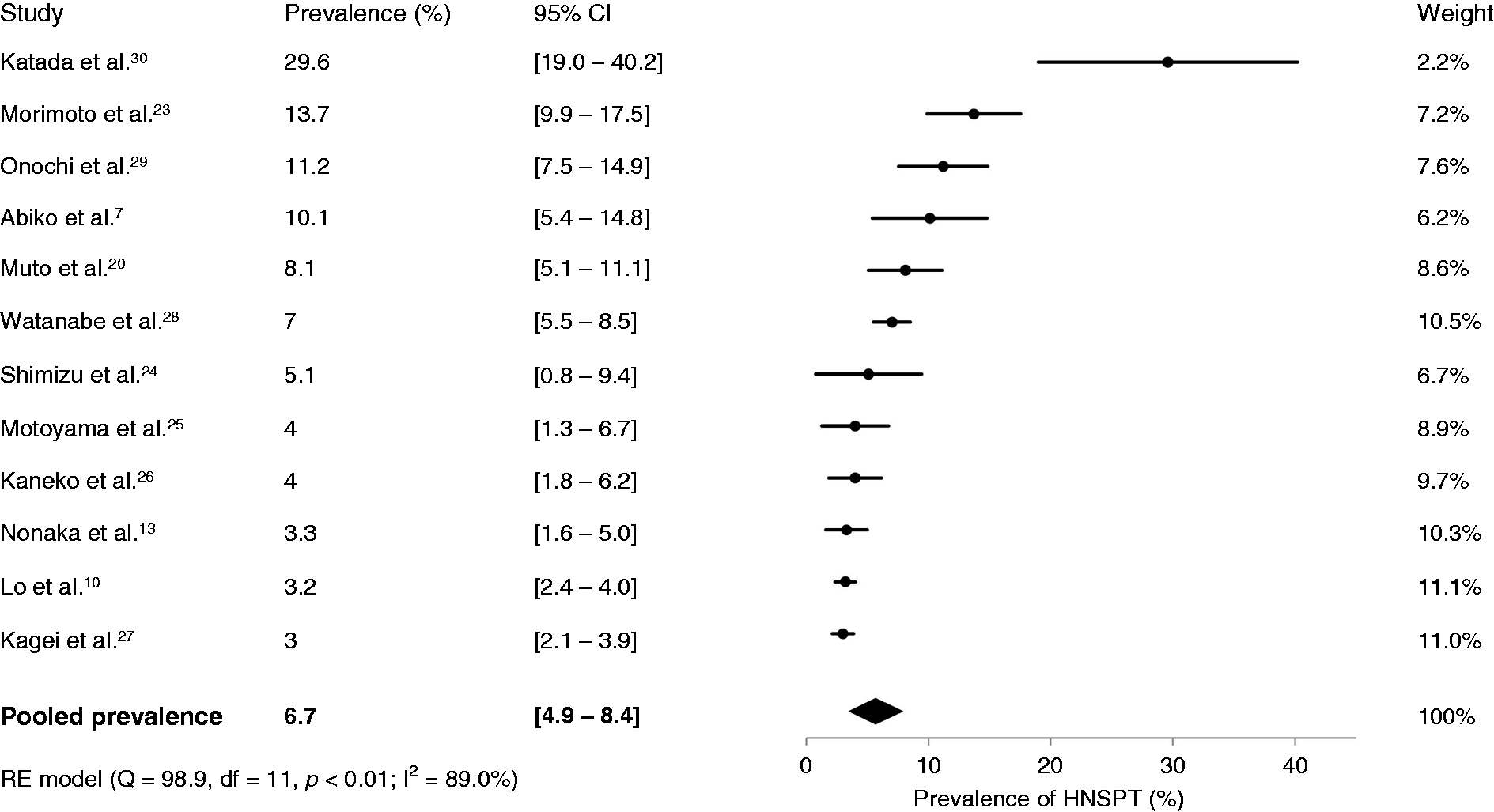
Sublocation of HNSPT and tumor stage
The sublocation of the HNSPTs was reported in eight of the 12 studies, for a total of 288 SPTs.10,13,23–26,28,30 In one study the sublocation was reported together for primary HN tumors and HNSPTs. Therefore, we excluded the study for this subanalysis. 10 A total of 234 HNSPTs remained. The combined data showed that 60% (141/234) of all HNSPTs were located in the hypopharynx, 18% (41/234) in the oropharynx, 11% (26/234) in the oral cavity, 9% (22/234) in the larynx and 2% (4/234) in other sublocations. In total, 405 HNSPTs were detected in 353 patients. Tumor stage of HNSPTs was reported in eight of the 12 studies.13,20,23,24,26–28,30 Morimoto et al. reported tumor characteristics of metachronous HNSPTs only. 23 Combined data showed that tumor stage was available for 62% of the HNSPTs (251/405). Overall, HNSPTs were classified as low stage (stage 0, I and II) in 85% (214/251) and high stage (stage III and IV) in 15% (37/251).
Time to diagnosis
Percentages of synchronous and metachronous HNSPT.
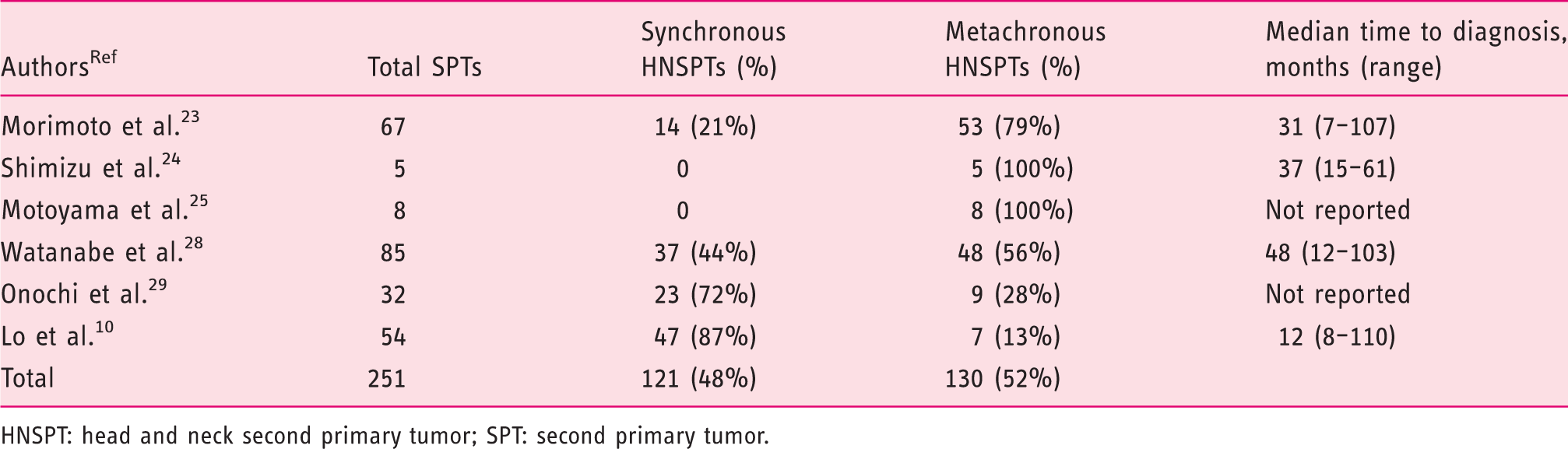
HNSPT: head and neck second primary tumor; SPT: second primary tumor.
Two studies performed only HN screening synchronously,26,27 and two only metachronously.7,13 The HNSPT prevalence in the study by Nonaka and colleagues 13 was 3.3% (14/424) with a median detection period of 27.6 months (range, 7.1–143.5) in patients screened with NBI and 101.0 months (range, 11.0–134.5) in patients screened with WL.
Primary ESCC tumor characteristics
Only four studies reported the sublocation of the index esophageal tumor.10,24,25,27 One study included only patients who underwent esophagectomy for thoracic ESCC. 25 The prevalence of HNSPTs in this study was 4.0%. The average percentages of index upper, middle and lower ESCC of the other three studies were 17.0%, 57.7% and 25.3% respectively.10,24,27 However, they did not report the prevalence of HNSPT per ESCC sublocation. The tumor stage of the primary ESCC was reported in nine studies (75%).7,10,20,23–25,27,29,30 On average, most esophageal lesions were stage 1 (29.0%) and stage 3 (29.8%). Other tumor stages were 0 (high-grade dysplasia) (7.3%), 2 (20.2%) and stage 4 (13.6%). The HNSPT prevalence per tumor stage of the primary ESCC was reported in three studies, for which only superficial ESCCs (stage 0 and I) were screened.7,29,30
Discussion
To our knowledge, this is the first systematic review on endoscopic screening for HNSPTs in patients with primary ESCC. Worldwide, the incidence of HN cancer is more than 550,000 cases annually. 2 We found an HNSPT (pooled) prevalence of 6.7%. Most HNSPTs were located in the hypopharynx (60.3%) and classified as low stage (85.3%). The proportion of synchronous and metachronous HNSPTs was comparable. Although the worldwide incidence cannot be compared directly with the pooled prevalence from this meta-analysis, the concept of endoscopic screening in patients with ESCC shows promise. An increase in early detection of HNSPTs could potentially improve the overall survival of ESCC patients.
Screening in Western countries will possibly show a different HNSPT prevalence because the etiology partly differs among these continents, and ESCC and HNSCC have a higher prevalence in Asia.3,31 The etiology of ESCC in Asia is, besides smoking and alcohol intake, clearly linked to a lowered fruit and vegetable intake. 32 The overall incidence of HN cancer in Japan was increasing, whereas the incidence in the United States was decreasing.31,33 Since the included studies were performed in Japan, it is unlikely that these results can be applied to the contemporary Western population.
Nonscreening Asian studies have reported HNSPT prevalence up to 7% in patients with primary ESCC.4,5 This is lower than the prevalence of the included studies (3.0%–29.6%). This might indicate that active screening of ESCC patients increases the number of detected HNSPTs. 23 Early diagnosis and treatment of both tumors can increase survival rate.23,34
Eighty-five percent of the HNSPTs were classified as low stage, which is higher than in the general HN cancer population. 35 Morimoto et al. reported a higher percentage of low-stage HNSPTs in patients with primary ESCC who were actively screened, and 83% of these HNSPTs could be treated with endoscopic resection. 23 Furthermore, survival was better in ESCC patients with HNSPTs who were actively screened. 23 ESCC patients could benefit from HN screening because this could result in an increased detection of superficial HN cancer, which can be treated with curative intent.
There is a lack of standardization in HN examination protocols among the included studies because different screening techniques are used (WL, NBI and Lugol). Studies that compared NBI with WL described a significantly higher detection rate of HNSPTs and a higher sensitivity and accuracy when using NBI.13,20,23,26 It would therefore be useful to always perform HN screening with WL and NBI. Lugol chromoendoscopy is not recommended in the HN region because this has to be performed under general anesthesia because of possible side effects. 28
The average percentage of synchronous and metachronous HNSPTs of all studies together is comparable. This could indicate that HN screening in patients with ESCC should be performed during work-up and follow-up. The median detection time of metachronous HNSPTs ranged from 12 to 101 months.10,13,23,24,28 However, the optimal moment for screening during follow-up has yet to be defined.
Our systematic review showed that 78% of the HNSPTs were located in the pharynx, which suggests that the pharynx has the highest risk of developing SPTs. Moreover, patients with pharyngeal cancer also showed the highest prevalence of esophageal SPTs. 17 The pharynx is the head and neck region that should definitely be screened in patients with primary ESCC. Although 10 of the 12 included studies performed screening of the pharynx, only four studies screened the whole HN region. We are aware of the fact that, of these four studies, only two studies reported the HNSPT sublocation.28,30 It was not possible to state whether there was a correlation between ESCC tumor stage and the occurrence of HNSPTs since this information was reported in only three studies.7,29,30 In these studies, only superficial ESCCs (stage 0 and I) were screened, which could underestimate the true HNSPT prevalence per ESCC tumor stage.
Some potential limitations about the methodology of the included studies need to be discussed: 1) Different screening techniques (i.e. WL, NBI, Lugol chromoendoscopy) were used. The combination of WL and NBI has the highest HNSPT detection rate; potential HNSPTs could be missed when using only WL; 2) one study performed screening with endoscopy and CT scan. 27 It was not clearly described which proportion of HNSPTs were detected by endoscopic screening. The proportion of HNSPTs detected by endoscopic screening could be lower than reported; 3) a different definition of metachronous and synchronous was used in three studies, whereby the comparison of the different studies was more difficult and the proportion of metachronous SPTs could be higher than reported;7,27,28 4) only four studies screened the whole HN region. Therefore, we could not easily determine which HN sublocation was at increased risk of developing HNSPTs; and 5) because this meta-analysis contained both prospective and retrospective data, a significant bias may be present.
In conclusion, the pooled prevalence of HNSPTs in patients with primary ESCC is 6.7%. Most HNSPTs were classified as low stage. Patients with low-stage HN tumors can be treated curatively with an excellent prognosis. Screening for HNSPTs could therefore be useful in ESCC patients. More screening studies are needed to investigate which type of ESCC (i.e. tumor stage and sublocation) increases the risk of HNSPTs and to report on risk factors associated with HNSPTs. More important, it is necessary to perform Western screening studies to assess the HNSPT prevalence since it is unclear whether the results of Asian studies can be extrapolated to the Western population. Head and neck examination protocols should be standardized in Japan; screening should be performed during work-up and follow-up with WL in combination with NBI. The pharynx is the head and neck region that should always be screened.
Supplemental Material
Supplemental material for Screening for head and neck second primary tumors in patients with esophageal squamous cell cancer: A systematic review and meta-analysis
Supplemental Material for Screening for head and neck second primary tumors in patients with esophageal squamous cell cancer: A systematic review and meta-analysis by SEM van de Ven, O Bugter, JA Hardillo, MJ Bruno, RJ Baatenburg de Jong and AD Koch in United European Gastroenterology Journal
Footnotes
Acknowledgment
The authors thank W.M. Bramer of the Erasmus MC medical library for developing the search strategy.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
No ethical approval was required, since this is a systematic review.
Informed consent
Informed consent was not required for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.