
Abstract
Background
Due to few randomized trials, there is uncertainty about the long-time effect of endoscopic screening on colorectal cancer (CRC) incidence and mortality.
Aim
To evaluate the long-term effect of endoscopic screening on CRC incidence and mortality, we performed a population-based randomized controlled trial in Norway.
Materials and methods
In 1983, 799 Norwegian men and women, age 50–59 years were drawn from the population registry and randomly assigned to flexible sigmoidoscopy screening (400 individuals), or no screening (399 individuals). Colonoscopy surveillance was offered after two and six years for all polyp-bearers in the screening group. In 1996, both groups were offered colonoscopy. Only individuals with advanced adenomas at colonoscopy in 1996 were recommended surveillance. All individuals were followed through Norwegian registries until 2008. Hazard ratios (HR) for CRC incidence, and CRC and overall mortality rates were calculated.
Results
During 26 years of follow up (17,327 person-years), 26 colorectal cancers were observed: seven in the screening group and 19 in the control group (HR in screening group 0.40, 95% CI 0.17–0.95, p = 0.04). Eight individuals died of colorectal cancer; one in the screening group and seven in the control group (HR 0.16, 95% CI 0.02–1.28, p = 0.08).
Conclusions
This first randomized trial on the long-term effect of endoscopic screening shows reduced CRC incidence and mortality if screening is combined with rigorous surveillance for individuals with polyps. Colonoscopy screening without such surveillance may not be effective.
Introduction
Colorectal cancer (CRC) is one of the leading causes of cancer-related death in the Western world. Most cases of CRC develop from colorectal adenomas through the adenoma–carcinoma sequence of molecular and morphological changes. 1 Removing adenomas by colonoscopy has been suggested to reduce CRC incidence and mortality.2,3 However, results from randomized trials evaluating the effect of colonoscopy screening on CRC incidence and mortality are lacking.
In 1996, the 13-year follow-up results from the Telemark Polyp Study, the first randomized trial of endoscopic screening for colorectal cancer, indicated an 80% reduction of CRC incidence due to screening. 4 More recently, three large randomized trials on flexible sigmoidoscopy screening have shown a risk reduction of 18–23% in CRC incidence and 22–31% in CRC mortality5–7. Another large-scale flexible sigmoidoscopy screening study did not, however, show any protective effect after 7 years of follow up. 8 The long-term effect on CRC incidence and mortality of endoscopic screening, is therefore still uncertain.
The present paper reports the 26-year follow-up results from the Telemark Polyp Study.
Materials and methods
Population and interventions
In 1983, 799 men and women (1:1 ratio) aged 50–59 years living in Telemark County, Norway were randomly drawn from the Norwegian population registry. Of these, 400 (born in the months of January, February, and March) were invited to a flexible sigmoidoscopy screening examination (screening group), and 399 (with no preference to month of birth), were allocated to the control group (Figure 1).
9
The control group was not offered any screening intervention. Individuals in the screening group with polyps of any kind detected at screening were scheduled for full colonoscopy with polypectomy (Figure 1).
Flowchart of the study from 1 March 1993 to 31 December 2008.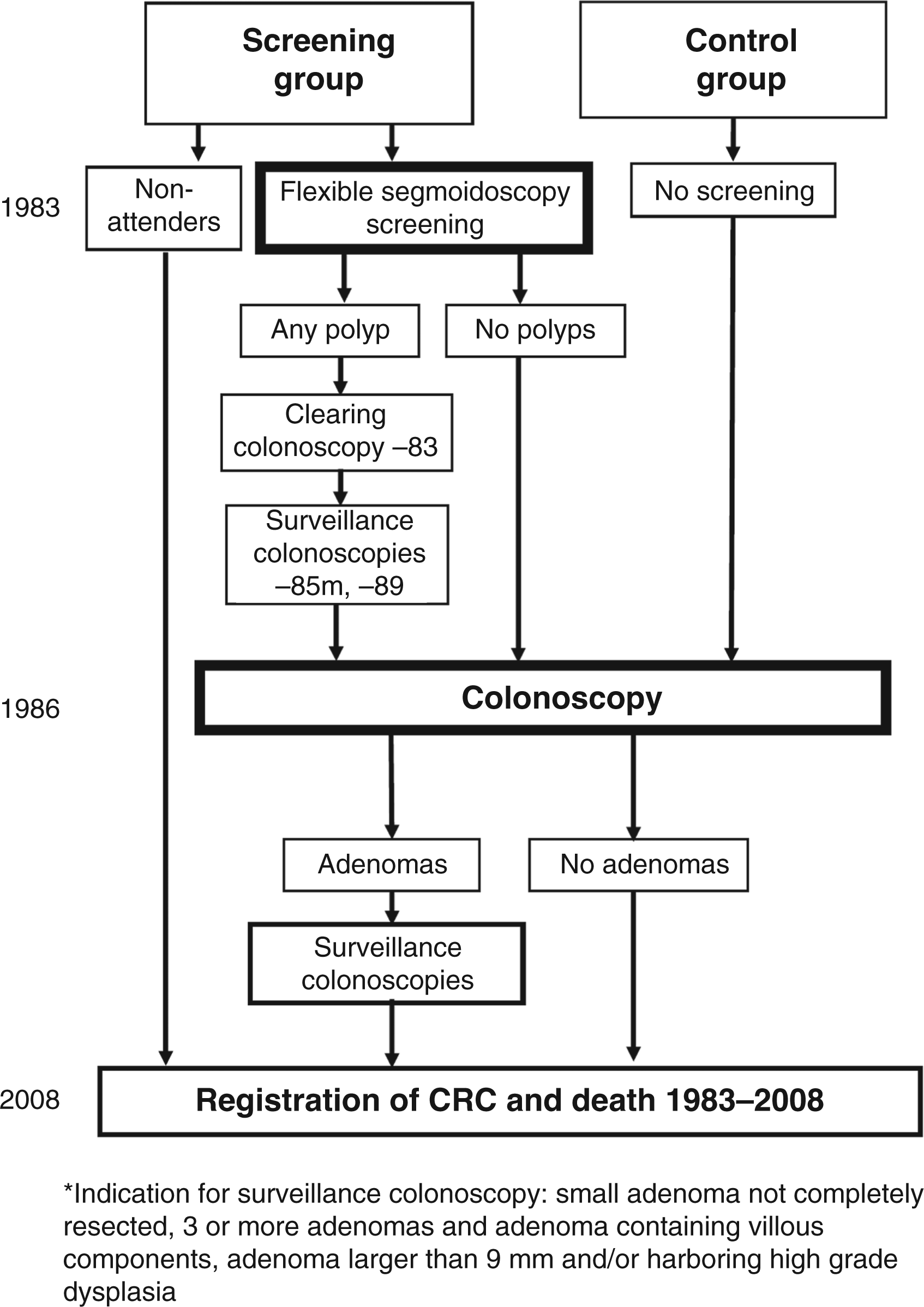
In 1996, colonoscopy was offered to all survivors from the screening and control groups (692 individuals) (Figure 1). The 58 survivors of the 76 non-attendees of the 1983 screening were not invited as this group had declined the invitation to participate in 1983, and the Regional Ethics Committee did not approve further contact being made. In the present paper, however, these non-attendees are included in the screening group for statistical analyses.
Post-screening surveillance
The time period from 1983 to 1995 was defined as time period I, and the time period from 1996 to 2008 was defined as time period II. Surveillance after screening was different in time period I compared with time period II. All individuals in the screening group who had polyps at screening in 1983 were offered colonoscopy surveillance both in 1985 and 1989. In time period II, colonoscopy surveillance was scheduled according to the Norwegian guidelines for polyp surveillance. 10 This implied surveillance only for individuals with advanced findings; after 5 years for individuals with three or more adenomas, first-degree relative with CRC, and endometrial cancer or adenomas not completely removed at screening; and after 10 years for individuals with adenomas larger than 9 mm, villous components, or high-grade dysplasia provided good bowel cleansing and complete resection. All endoscopic examinations in the study period between 1983 and 2008 were performed at Telemark Hospital by experienced endoscopists.
Endpoint acquisition
All individuals in the screening and control groups were followed until death, emigration, or the end of follow up (31 December 2008). By linkage of the data to the Cancer Registry of Norway, the Cause of Death Registry, and Statistics Norway, we obtained information on colorectal cancer incidence, date, and cause of death. The Cancer Registry of Norway registers all cancers in Norway and is close to 100% complete.11,12 Patients are identified in the Registry by their individually unique national registration number.
Statistical analysis
Comparisons between the groups were performed with intention-to-treat analyses, including all individuals randomized. Pearson chi-squared test was used to compare participation rates, findings at screening, and death rates between the groups. CRC-specific survival and overall survival were illustrated by Kaplan–Meier plots and cumulative hazard ratios (HRs) for CRC incidence were illustrated by Nelson-Aalen estimates. For calculation of colorectal cancer mortality rates, censoring occurred at date of death from causes other than colorectal cancer or at the end of follow up, whichever came first. For calculation of colorectal cancer incidence rates, censoring occurred at date of death, emigration, or the end of follow up, and for calculations of mortality rates, censoring occurred at emigration or the end of follow up.
Individuals with CRC before study entry (1 March 1983) were excluded from the analyses (none in the screening group and three in the control group). HRs with 95% confidence intervals (CI) were calculated using Cox proportional hazard models. We used likelihood ratio statistics to compare groups. The proportional hazards assumption was tested by both graphical methods and Schoenfeld residuals. Mortality and incidence rates were calculated by the standardized incidence method.
All test statistics were two tailed, p-values <0.05 were considered statistically significant. Calculations were performed with the statistical packages SPSS version 15.0 (SPSS, Chicago, IL, USA) and Stata 10.0 (StataCorp, TX, USA).
Ethical review
All screened participants provided written informed consent. The study was approved by the regional ethics committee and performed in accordance with the Helsinki Declaration.
Results
Age, attendance rates, and findings of adenomas and high-risk adenomas at screen in 1983 and 1996
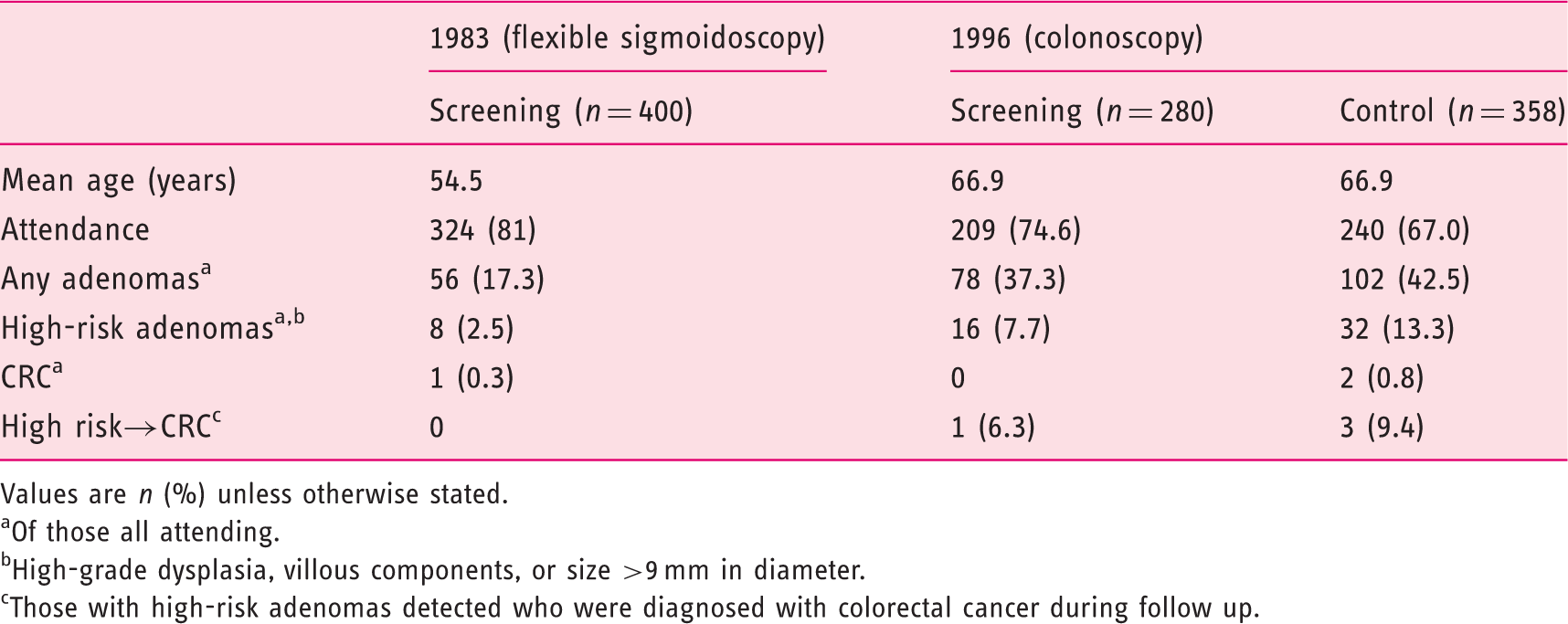
Values are n (%) unless otherwise stated.
Of those all attending.
High-grade dysplasia, villous components, or size >9 mm in diameter.
Those with high-risk adenomas detected who were diagnosed with colorectal cancer during follow up.
Colorectal cancer incidence
After a follow-up period of 26 years, with a total of 17,327 person-years, 26 patients were diagnosed with CRC; seven (1.8%) in the screening group and 19 (4.8%) in the control group. In the screening group, three out of the cancers occurred in individuals who had attended screening in 1983 and four in individuals who had not attended the screening (non-compliers).
The cumulative CRC incidence was reduced by 60% in the screening group compared to the control group (HR 0.40, 95% CI 0.17–0.95, p = 0.04; Table 2, Figure 2a). The incidence reduction was comparable in time period I and time period II (HR for period I 0.30, 95% CI 0.06–1.44, p = 0.13; HR for period II 0.43, 95% CI 0.15–1.22, p = 0.11). An 80% reduction in colorectal cancer incidence for the whole trial period was observed for those attending in 1983 compared with the control group (HR 0.20, 95% CI 0.06–0.69, p = 0.01). Table 3 shows CRC incidence rates in the screening and control groups. There was no difference in the localization of the CRCs in the colon.
(a) Cumulative incidence of colorectal cancer from 1983–2008 for the screening and control groups. (b) Yearly cumulative colorectal cancer incidence rate (per 100,000 person-years) from 1983–2008 in the different study groups. In 1996, marked by a vertical line, both the initial screening and the initial control group were offered colonoscopy. Incidence and mortality of colorectal cancer and all-cause mortality in the screening group from 1983–2008 Intention-to-treat analyses including all individuals as randomized. Control group was used as the reference. Colorectal cancer, colorectal cancer deaths, deaths from all-causes, person-years, and incidence and mortality rates per 100,000 person-years for the two study groups IR, incidence rate per 100,000 person-years; MR, mortality rate per 100,000 person-years.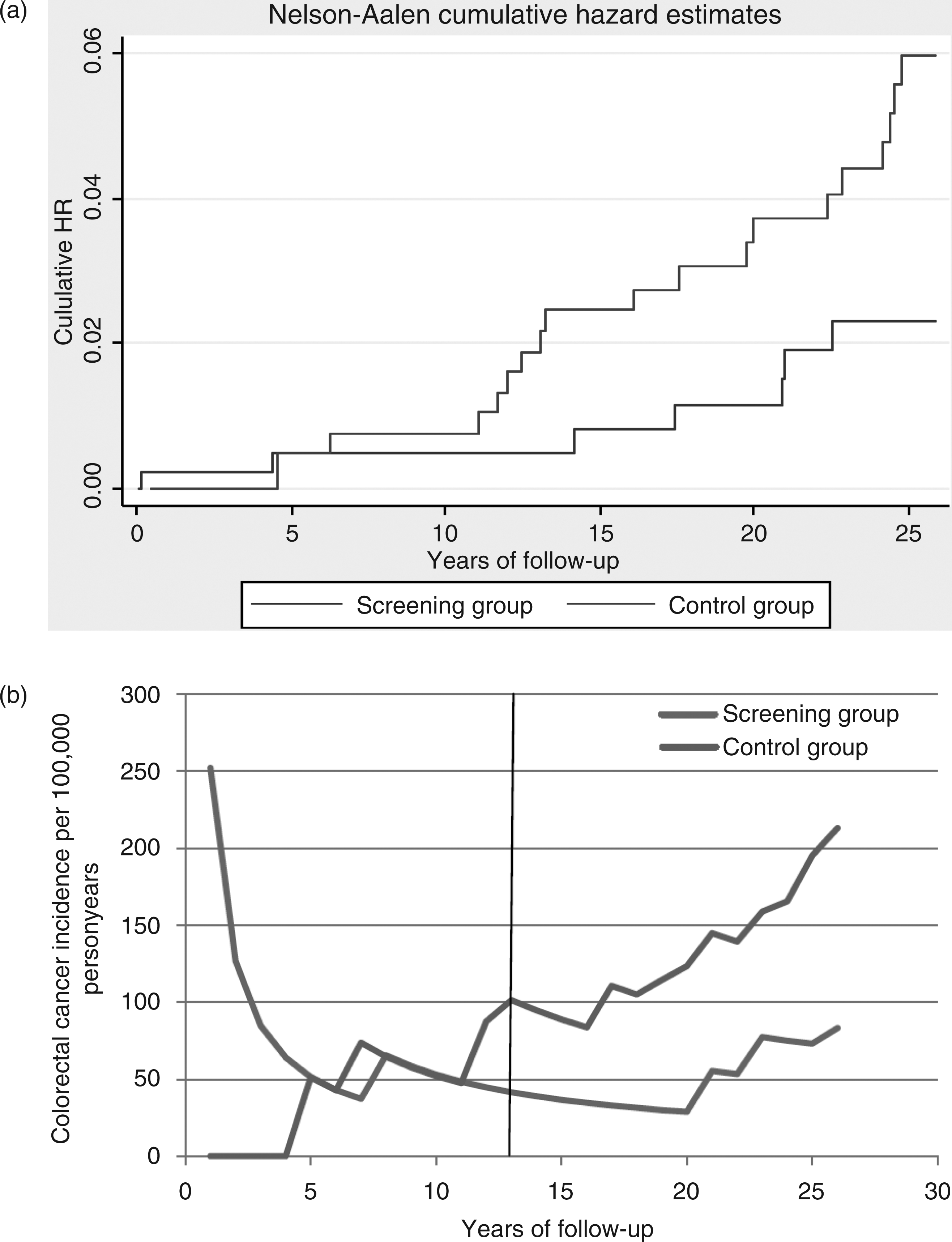
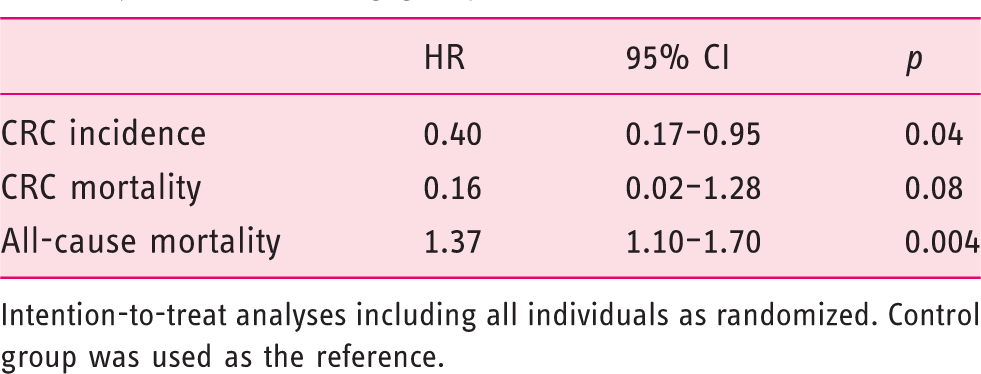
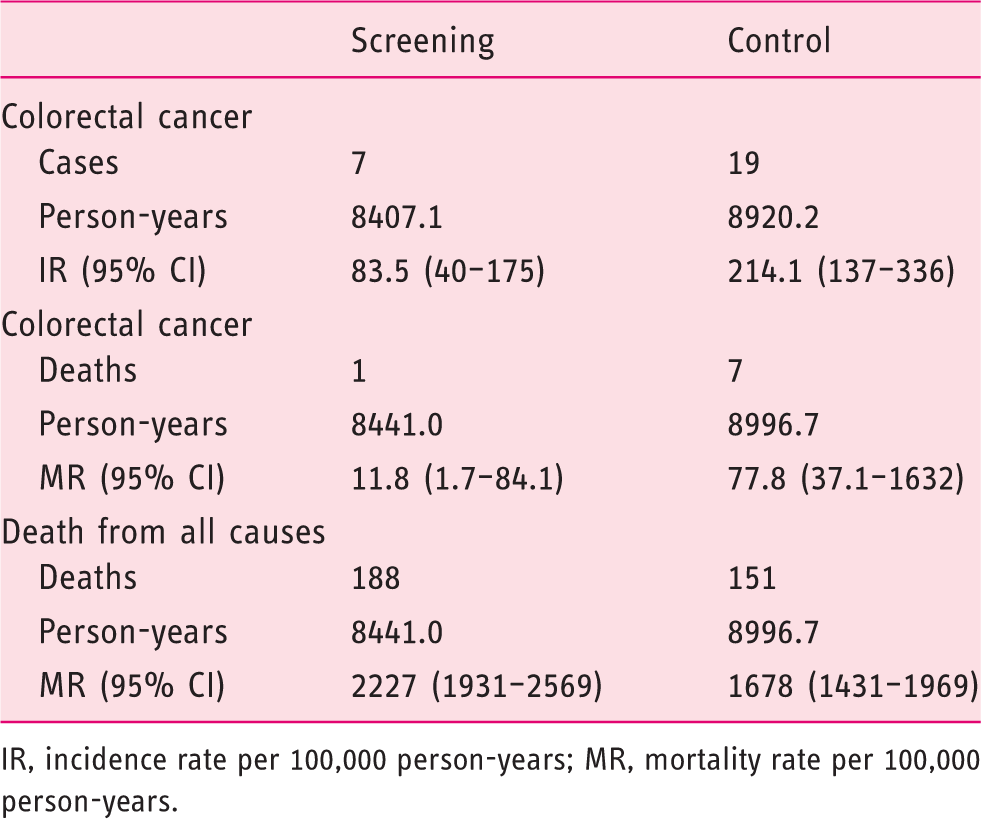
Figure 2b displays yearly cumulative incidence rates of CRC. After an initial peak of CRC incidence in the screening group due to cancers diagnosed at screening, there is a sustained reduction of CRC incidence throughout the trial period. In comparison, CRC incidence is increasing in the control group during the course of the trial, regardless of the colonoscopy in 1996.
Colorectal cancer mortality
Altogether, eight individuals died of colorectal cancer; one in the screening group (0.25%) and seven in the control group (1.8%). The hazard of death from CRC was reduced by 85% in the screening group compared to the control group (HR 0.16, 95% CI 0.02–1.28, p = 0.08). Table 3 shows the corresponding CRC mortality rates in the screening and control groups.
All-cause mortality
After 26 years of follow up, 188 (47%) individuals had died in the screening group, compared with 151 (38%) in the control group (HR 1.37, 95% CI 1.10–1.70, p = 0.004). This difference was only apparent during time period I from 1983 to 1995 (HR 1.68, 95% CI 1.12–1.52, p = 0.04), but not during time period II from 1996 to 2008 (HR 1.10, 95% CI 0.85–1.42, p = 0.46). No differences were found in the distribution of cause of death in the different study groups.
Discussion
This is the first report from a randomized trial addressing long-term effectiveness of endoscopic screening on CRC incidence, mortality, and all-cause mortality. Due to its design with different endoscopic screening approaches during different time periods, this study could provide new insight into the optimal intensity of surveillance after initial screening.
The main finding of this study is that endoscopic screening by flexible sigmoidoscopy at age 50–59 years, combined with rigorous colonoscopic surveillance has a large, long-lasting effect on CRC incidence, with a 60% risk reduction after 26 years of follow up. The CRC incidence reduction in the screening group was similar in time period I (intensive surveillance) and in period II (modest surveillance) – in spite of the control group being subjected to endoscopy screening at the start of period II. We also found a profound reduction in CRC mortality in the screening group, but due to the few events this difference was not statistically significant. All-cause mortality was, however, higher in the screening group compared to the control group, an unexpected finding which is a signal for caution and further study. However, this effect was apparent only in the first period of the study.
The present trial was originally designed as a flexible sigmoidoscopy feasibility trial in the early 1980s, before the concept of endoscopic screening gained widespread interest. Although the comparison of CRC incidence and death between the screening and control groups has been a primary interest of the study right from the start, it was not sufficiently powered to detect clinically meaningful differences with a high degree of statistical certainty. Due to the relatively low number of CRC deaths in the trial, the difference between the screening and control group did not reach statistical significance.
The initial screening was followed by a very comprehensive colonoscopy surveillance program, which included frequent colonoscopies of all individuals with polyps of any kind at the screening exam. At that time, it was generally believed that endoscopy had to be repeated frequently to prevent future development of cancer. Later, starting in the mid-1990s, guidelines were changed towards longer surveillance intervals. 15 In accordance with these guidelines, individuals in the second phase of trial did not get the same rigorous surveillance after polypectomy. The reduction in CRC incidence persisted for the screening group throughout the study period, with an increasing incidence in the latest years (Figure 2).
We were not able to disentangle the effect of age at screening and the different surveillance protocols in the present study. However, there should not be any large differences between the expected effects of endoscopic screening for age groups around 60 years. 16
One factor that could have reduced an effect of the colonoscopy in 1996 is the increased utilization of endoscopic procedures in the health service. We found, however, no significant difference in the proportion of individuals that had had non-screening endoscopies in time period II compared to period I.5,12 Therefore, screening contamination is not likely.
The incidence of adenomas and high-risk adenomas increase with age and the detection rates of adenomas and high-risk adenomas in this study are comparable to other studies. 17
In light of our results, it seems that individuals with adenomas might have to be followed rigorously with frequent colonoscopies to provide long-term protection from colorectal cancer. In this setting, endoscopic screening seems highly effective. We do not know, however, whether this effect of endoscopic screening and surveillance might differ in different age groups.
A limitation of this study is a slightly unbalanced randomization; the initial screening group and the initial control group had different patterns of months of birth. Due to a hypothesis of high compliance if screening invitations are timed in proximity to the individuals’ birthdays, 18 all individuals in the screening group were born in the months of January to March, while the individuals in the control group were born throughout all months of the year. We analysed the mortality rate based on the month of birth, and found that individuals born in the first quartile of the year had slightly higher all-cause mortality rates compared to those born in the three last quartiles of the year (data not shown). Further, it has been suggested that screening may lead to unfavourable lifestyle changes for attendees.19,20 One hypothesis that could explain some of the mortality difference between the groups is that screening may undermine incentives to reduce the risk of lifestyle-related morbidity and mortality, as demonstrated in the recent Norwegian Colorectal Cancer Prevention trial using flexible sigmoidoscopy. After three years of follow up, the screening group gained more weight, ended smoking less frequently, and had poorer improvement in exercise habits and less improvement in servings of fruit, berries, and vegetables per day compared with controls. 19
The observed excess mortality is largely confined to the first period of the trial (before 1996) when addressing people at a younger age. Although plausible, there is no documentation that younger people are more susceptible to unwanted lifestyle effects of screening. Due to the design of the study, it was not possible to compare baseline characteristics between the screening and control groups. They were, however, randomized from a socioeconomic heterogeneous area of Norway so we do not expect large differences between the groups.
In conclusion, endoscopic screening is effective in reducing CRC incidence and mortality for a long time after screening, but the findings might indicate that individuals should be followed rigorously with colonoscopy surveillance.
Clinical trial identifier
NCT01014039.
Footnotes
Acknowledgements
We are grateful for Dr David Ransohoff’s comments to the manuscript.
Funding
This work was supported by the Norwegian Cancer Society (grant number E 96008/007). MK received research grants from the Norwegian Research Council (grant number 205243).
Conflict of interest
MB has received research support from Olympus, Fujinon, Ferring, CCS, and Falk Pharma. The other authors have nothing to report.