
Abstract
Background and aims
Obesity is associated with an increased incidence of and mortality from colorectal cancer (CRC). Screening colonoscopy seems particularly important for individuals with obesity. The aim of this study is to analyse the characteristics of screening colonoscopy in individuals with obesity.
Methods
We performed a cross-sectional analysis of records of 75,278 patients from a national colonoscopy screening programme in Poland. The database contained demographic data, colonoscopy results, self-reported data on weight and height, a standardized screenees’ experience questionnaire and colorectal findings.
Results
Adenoma detection rate and advanced neoplasia detection rate increased significantly in groups of increasing body mass index (BMI). In subjects with morbid obesity, odds ratios for proximal adenoma and proximal advanced neoplasia were 1.69 (95% confidence interval (CI) 1.28–2.21) and 1.66 (95% CI 1.01–2.72), respectively, despite the fact that with BMI increasing over 30 the preparation for colonoscopy was worse. Moreover, caecal intubation increased with increasing BMI. Tolerance of colonoscopy was better and preparation for colonoscopy was less inconvenient in individuals with obesity.
Conclusions
Obesity and morbid obesity are associated with increased detection of colorectal precursor lesions and better performance of screening colonoscopy. Participation in screening colonoscopy should be emphasized among individuals with obesity, taking into account the burden of CRC in this population.
Key summary
Summarize the established knowledge on this subject:
Obesity is associated with an increased incidence of and mortality from colorectal cancer. Screening colonoscopy reduces the incidence and mortality of colorectal cancer. Screening colonoscopy seems particularly important for individuals with obesity. What are the significant and/or new findings of this study?
Obesity and morbid obesity are associated:
○ With increased detection of colorectal precursor lesions; ○ With better tolerance of colonoscopy.
Introduction
Obesity is associated with an increased incidence of and mortality from colorectal cancer (CRC). 1 Excessive body weight is also associated with increased technical difficulty and higher risk of adverse effects of colorectal surgery, worse chemoradiotherapy or adjuvant chemotherapy response, and worse cancer-specific and overall survival after CRC diagnosis. 2 Screening colonoscopy, which is known to reduce the incidence of and mortality from CRC, therefore seems particularly important for individuals with obesity. 3 However, despite this, it was demonstrated that CRC screening participation rates in individuals with obesity were inferior compared to healthy weight individuals. 4 The underlying cause of the inferior participation is unknown. Large population-based studies investigating colonoscopy performance in individuals with obesity are missing. These studies could help us to understand the underlying cause of the inferior participation and inform the targeted interventions with the data on screening colonoscopy performance in this particular population.
The aim of this study is to analyse the characteristics and quality indicators of screening colonoscopy in individuals with obesity.
Study design
We performed a cross-sectional analysis of national CRC screening programme database records of 40–66-year-old subjects who entered the national colonoscopy screening programme for the detection of colorectal cancer in Poland, between January 2007 and December 2008. The database contained demographic data, colonoscopy results, self-reported data on weight and height, a standardized screenees’ experience questionnaire and colorectal findings from all screening centres throughout Poland. Screenees with missing data on weight and height, or an incomplete report on the colorectal findings, were excluded. The research proposal was reviewed by the Bioethical Committee at the Maria Sklodowska-Curie Memorial Cancer Centre and Institute of Oncology on 3 October 2014, and was judged to be exempt from oversight, as data was deidentified and could not be linked to specific subject. The study protocol conforms to the 1975 Declaration of Helsinki, as reflected by abovementioned exemption by the Bioethical Committee. Written informed consent was obtained from all participants entering the national CRC screening programme.
Study procedures and definitions
Patients between the ages of 50 and 66 years (40 and 66 years in cases of a positive family history of cancer of any type) were advised by their family doctors or general practitioners to participate in the screening. Exclusion criteria were clinical suspicion of colorectal cancer; characteristics that met the criteria for Lynch syndrome, familial adenomatous polyposis or inflammatory bowel disease; and colonoscopy within the preceding 10 years, or past medical history of CRC. 1 Before colonoscopy, all the participants were asked to fill in an epidemiological questionnaire including data on self-reported weight and height. Screening colonoscopy procedures were described in detail elsewhere. 1 The use of sedation was at the discretion of the participating endoscopists. In a standardized colonoscopy report, caecal intubation was noted (no photo documentation was obligatory). Bowel preparation was scored according to the Aronchick scale. 5 In addition, screenees’ tolerance of colonoscopy was assessed by an endoscopist using a four-point verbal rating scale (very good, good, fair or bad). 6 A standardized screenee experience questionnaire was filled in by participants immediately after the examination (for unsedated colonoscopies) or just before discharge (for sedated colonoscopies). Two items from the questionnaire were used for the purpose of the study: inconvenience of the preparation for the examination (scored: no, slightly, yes or very) and tolerance of the examination (scored: very good, good, fair or bad). For the purpose of this study, the responses on patient experience were dichotomized (two positive and two negative responses pooled together, respectively).
Body mass index (BMI) was calculated using weight (kg)/(height (m))2 and stratified according to the World Health Organization classification. 7 Underweight was considered as BMI < 18.5 kg/m2, normal weight 18.5–24.99 kg/m2, overweight 25.00–29.99 kg/m2, obesity class I 30.00–34.99 kg/m2, obesity class II 35.00–39.99 kg/m2 and obesity class III 40.00 kg/m2. Class I and II obesity were pooled together, while class III obesity was analysed separately as a representation of morbid obesity.
Statistical methods
Descriptive statistics were prepared with the use of contingency tables. For each assessment, the BMI groups were compared with the use of a nonparametric test for trend. Multivariate logistic regression models were used to investigate the associations between clinical variables and colonoscopy features. Sex, age group, interaction term between sex and age group, and family history of CRC were tested for inclusion using forward stepwise regression at the 0.1 significance level. An interaction term was added in models for advanced neoplasia and distal advanced neoplasia to improve fit of the model. The Hosmer–Lemeshow test was used to check the goodness-of-fit of the models. A two-sided p-value < 0.05 was considered to denote statistical significance. The statistical analysis was performed using Stata Statistical Software, v. 13.1 (Stata Corporation, College Station, Texas, USA).
Definitions
Colorectal findings were categorized on the basis of the most advanced lesion identified at screening (including additional required colonoscopies to remove all polyps, when indicated). 8 Proximal lesions were defined as lesions localized proximally to the splenic flexure of the colon. Advanced neoplasia was defined as adenocarcinoma or advanced adenoma. Advanced adenoma was defined as adenoma ≥ 10 mm, with villous components (tubulovillous or villous) or with high-grade dysplasia. Adenoma detection rate (ADR) was defined as the proportion of screening colonoscopies that detect at least one adenoma. 9 Similarly, advanced neoplasia detection rate (ANDR) was defined as the proportion of screening colonoscopies that detect at least one advanced neoplasia. Serrated lesions were not classified at the time of the study period.
Results
Of the 82,957 participants who met the eligibility criteria and entered the national screening programme for CRC between January 2007 and December 2008, 7679 (9.25%) were excluded due to incomplete most advanced lesion categorization, incomplete screenee experience questionnaire, or missing data on weight and height. Baseline characteristics of the studied group are presented in Supplemental Table 7 (available online in supplemental material).
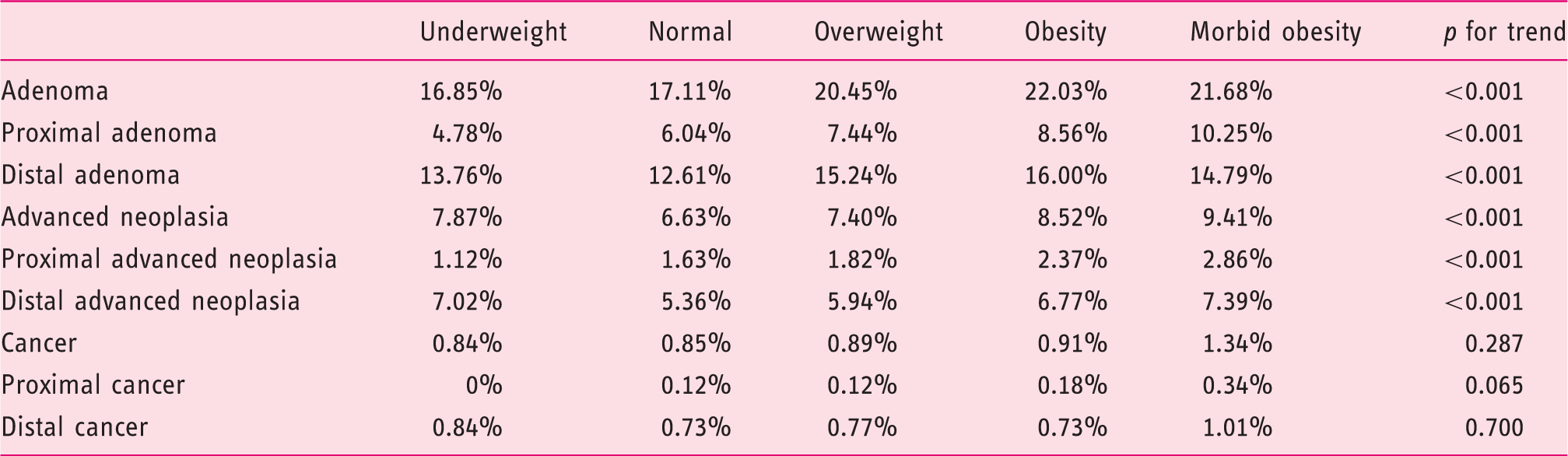
Detection rates of adenoma, advanced neoplasia and cancer in body mass index groups.
Adenoma, distal and proximal adenoma detection in a logistic regression model involving body mass index, age, sex and family history of colorectal cancer of the screenees.
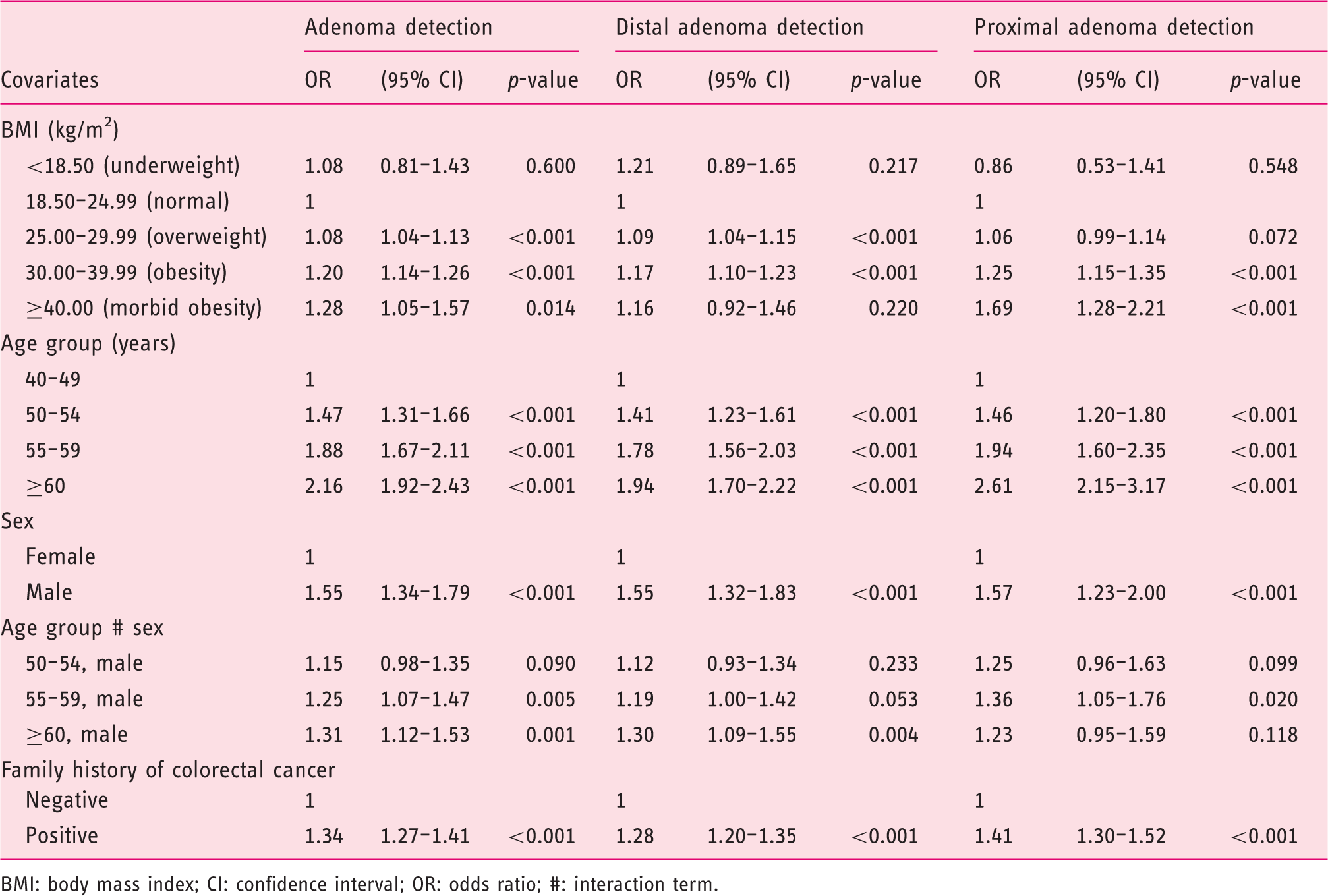
BMI: body mass index; CI: confidence interval; OR: odds ratio; #: interaction term.
Advanced neoplasia, distal and proximal advanced neoplasia detection in a logistic regression model involving body mass index, age, sex and family history of colorectal cancer of the screenees. Interaction term was added in models for advanced neoplasia and distal advanced neoplasia to improve fit of the model.
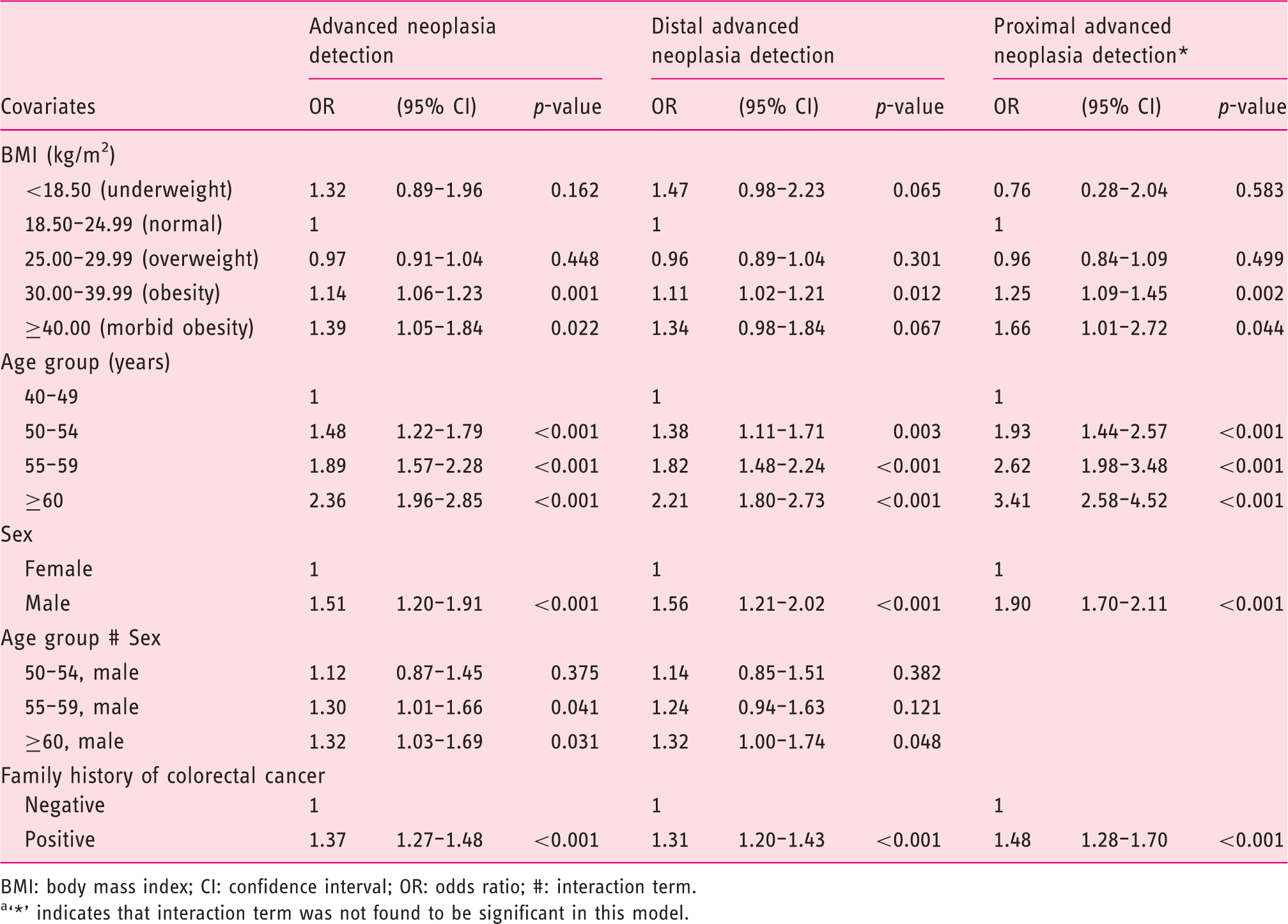
BMI: body mass index; CI: confidence interval; OR: odds ratio; #: interaction term.
‘*’ indicates that interaction term was not found to be significant in this model.
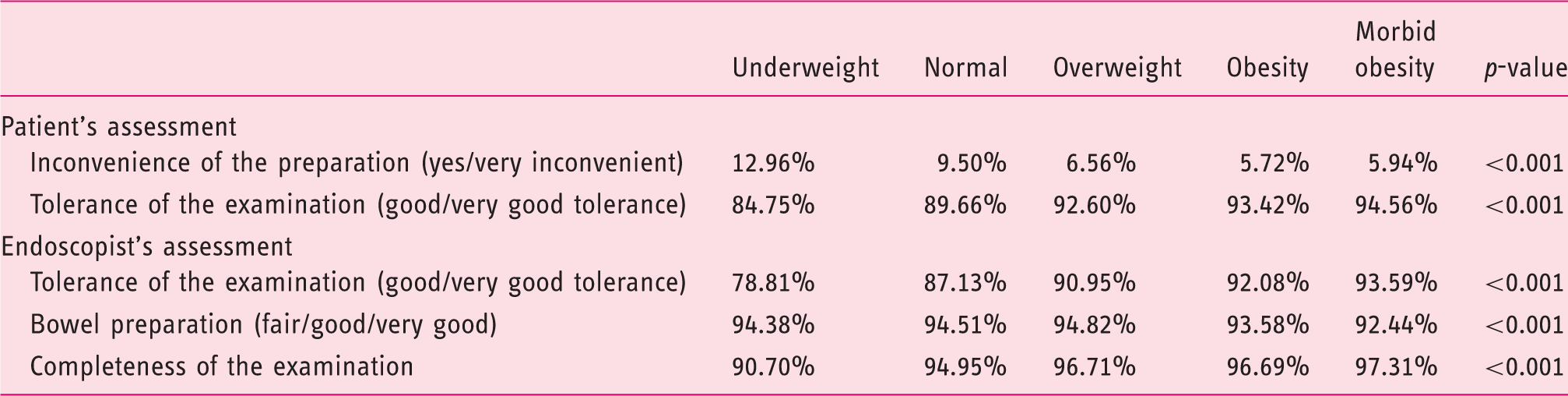
Summary of results of screenees’ questionnaire and endoscopists’ assessment.
Inconvenience of preparation for colonoscopy and tolerance of the examination (patient scored) in a logistic regression model involving body mass index, age and sex of the screenees. Odds ratios of not experiencing inconvenience during preparation for colonoscopy are given.
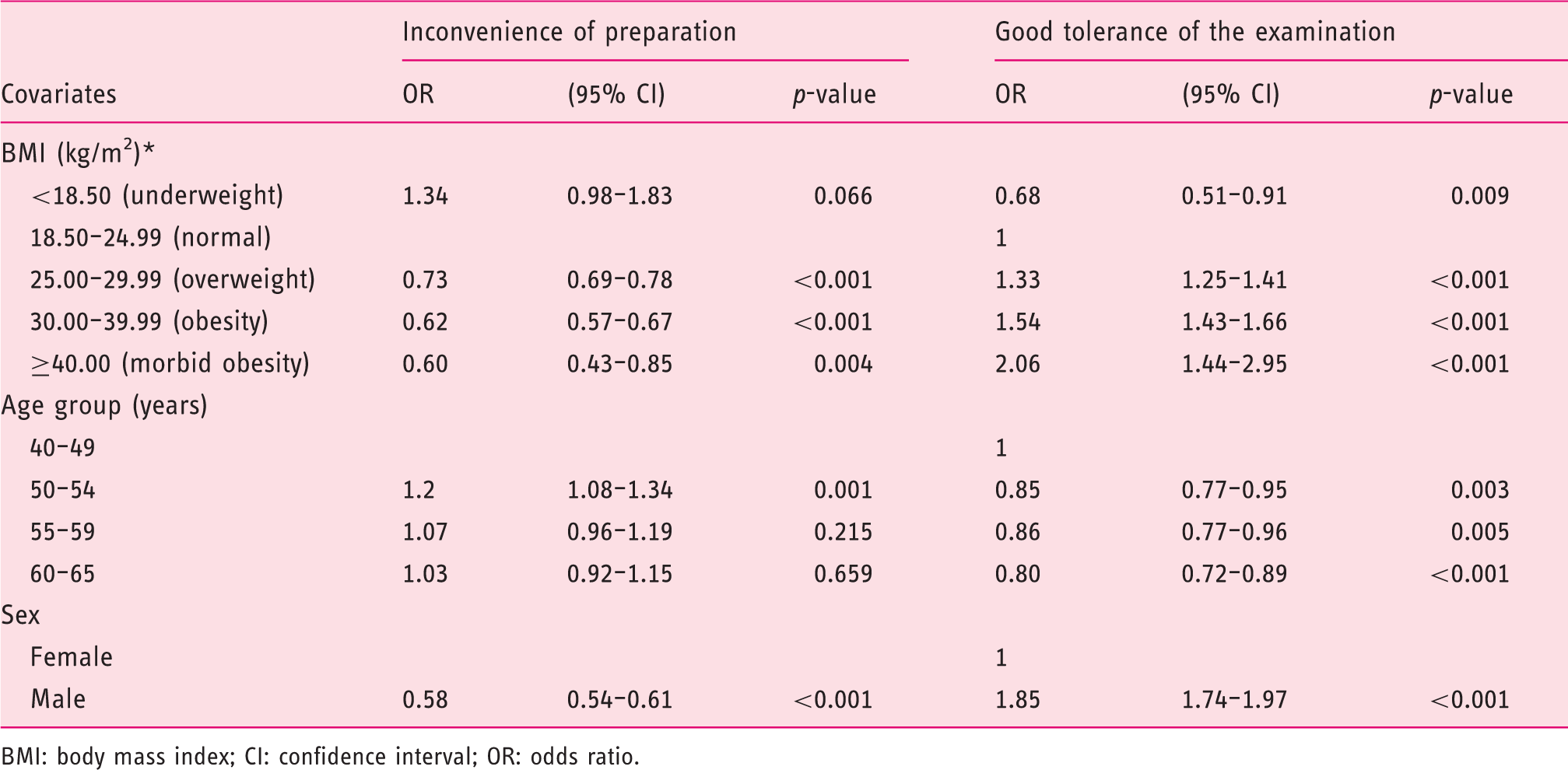
BMI: body mass index; CI: confidence interval; OR: odds ratio.
Tolerance of the examination (endoscopist scored), bowel preparation and completeness of the examination in a logistic regression model involving body mass index, age and sex of the screenees.
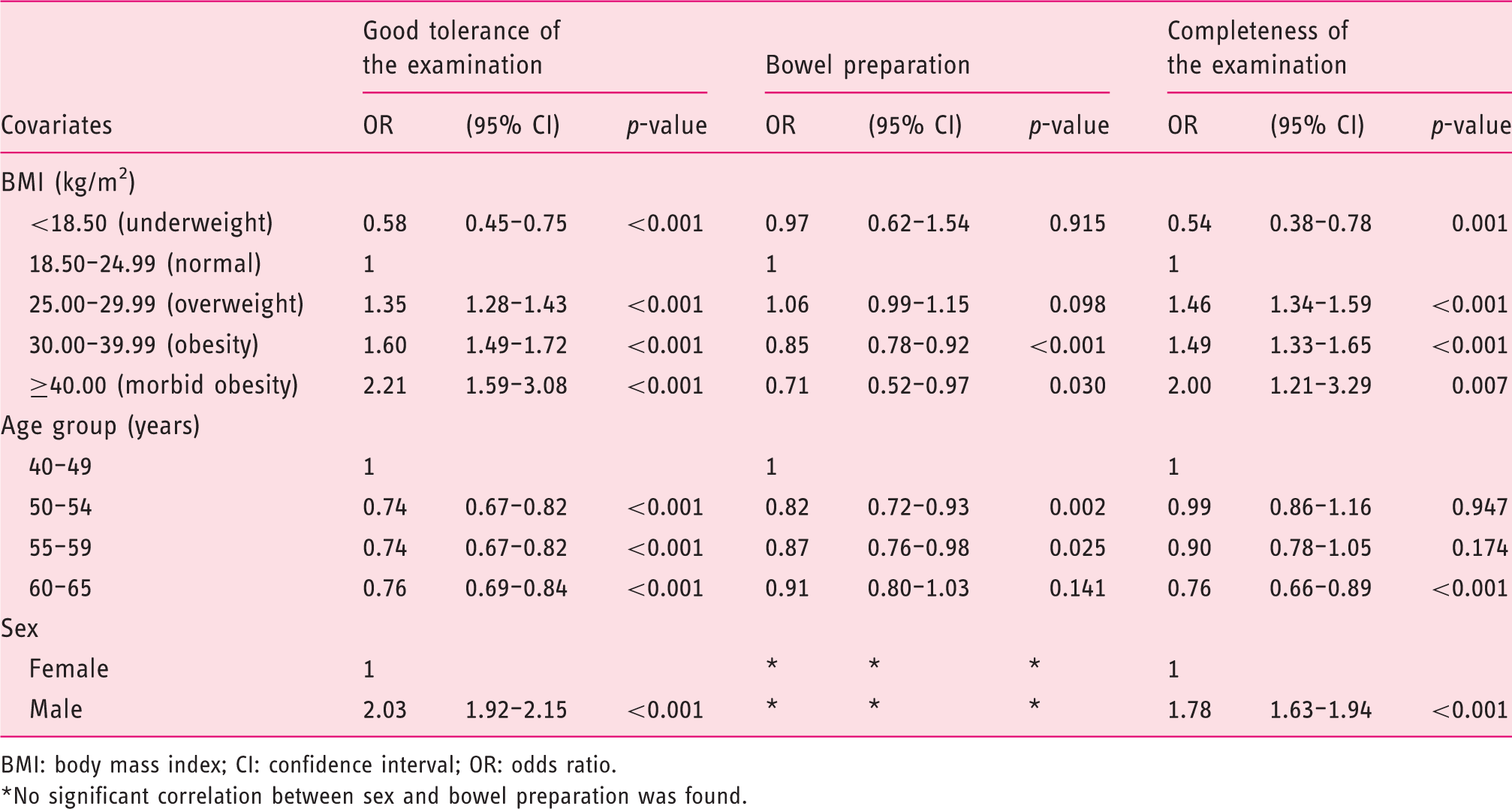
BMI: body mass index; CI: confidence interval; OR: odds ratio.
No significant correlation between sex and bowel preparation was found.
Discussion
The study provides a uniquely broad evaluation of characteristics of screening colonoscopies in a large population including individuals with obesity and morbid obesity. In this study, we described higher ADR, ANDR and CIR (caecal intubation rate) in individuals with obesity and morbid obesity undergoing screening colonoscopy. Detection rates observed for any, proximal and distal locations increased in subjects with excessive bodyweight. Subjects with obesity and morbid obesity reported better tolerance of the examination and less inconvenient preparation. Endoscopists’ reports confirmed better tolerance of the examination despite inferior bowel preparation. The associations with increasing BMI follow a dose-dependent relationship. A meta-analysis of 23 studies revealed that the overweight and obesity populations demonstrate an increased risk of colorectal adenoma prevalence of 24%. The positive association between BMI and adenoma prevalence also followed a dose-response relationship. 10 In another meta-analysis, Ben et al. have shown that for each 5-unit higher BMI, the risk of colorectal adenoma increases by about 20%. 11 In a recent systematic review and meta-analysis by Wong et al., risk of adenoma was described both in individuals with overweight and individuals with obesity with summary ORs of 1.44 and 1.42, respectively. 12 In our study, we additionally analysed a group of subjects with BMI > 40 kg/m2. This has never been analysed in such a large population, as in most previous studies BMI has been dichotomized using a BMI cut-off value of 25 with further subgroups not being considered. 13 Due to the unique subgroup analysis, we were able to conclude that detection rates increased with BMI in subjects with morbid obesity reaching ORs as high as 1.69 (95% CI 1.28–2.21; p < 0.001) and 1.66 (95% CI 1.01–2.72; p = 0.044) for proximal adenoma and proximal advanced neoplasia, respectively. These ORs translate to an increase of absolute detection rates of distal adenoma from 12.61 to 14.69%, while those of distal advanced neoplasia increased from 5.69 to 7.39% (both p-values < 0.001). The meta-analysis by Wong et al. involves almost 170,000 subjects of different ethnicity from 17 studies. We present results of over 75,000 white Caucasian subjects in a single study, being (to our knowledge) the most populated original study on BMI in screening colonoscopies so far. In our study, male sex was associated with higher risk of adenoma and advanced neoplasia, which is opposite to the findings of the meta-analysis by Wong et al. Our results are in accordance with a recently published small Canadian study, which reported that male sex associated with increased risk of adenoma and advanced adenoma. 14 In other studies, BMI appears to be consistently associated with an increased risk of colon or rectal cancer in men, but less so in women. 15 This gender difference might be explained by sex differences in the prevalence and age of onset of metabolic syndrome, or a protective effect of oestrogen attributable to the induction of apoptosis and inhibition of cell proliferation. 16 In our logistic regression model, increased BMI, increased age of screenees, male sex and positive family history of CRC were risk factors for the detection adenoma or an advanced neoplasia. For example, a cumulative risk of detecting an advanced neoplasia in a male with morbid obesity aged 60 or over with a positive family history of CRC is 10-fold higher than in a female without obesity aged under 50 with a negative family history of CRC. This disparity regarding the magnitude of the risk of subjects eligible for screening warrants a more active engagement of individuals with excessive body weight into the CRC screening programmes. It has been suggested that BMI should be considered an independent risk factor for advanced colorectal neoplasia and that people with high BMI should be recommended to undergo colonoscopy screening earlier than scheduled. 17 Considering an increasing incidence of CRC in individuals under 50 years old, further studies are warranted to assess the impact of excessive body weight in this age group. A recent meta-analysis study has shown that having obesity confers an approximately 1.334-fold increased risk of developing colorectal cancer relative to being normal weight. 18 Colorectal screening scores involving BMI for the prediction of adenoma and advanced neoplasia have recently been proposed for screening purposes. 19 On the other hand, the benefit of screening colonoscopy in individuals with obesity may be relatively lower due to obesity-related comorbidities (i.e. diabetes, cardiovascular and respiratory) of significant mortality rates. 20
Analyses stratified by the anatomical site suggest that higher BMI levels cause an equal increasing risk for both colon cancer and rectal cancer. 18 Meta-analyses have suggested that BMI may be more strongly associated with colon vs. rectal adenoma and cancer incidence.21,22 Similarly, a pooled analysis of seven prospective studies found an association with recurrent adenomas in the proximal colon, but not the distal colon or rectum. 23 In our study, ORs in increasing BMI groups were also higher for proximal than for distal locations of the lesions. Although the incidence of cancer in our study was not significantly different in the groups of increasing BMI, a remarkable trend (p = 0.065) was observed for cancers in proximal locations. The incidence of CRC in the group with normal BMI was 0.12% and increased with higher BMI to 0.34% in the morbidly obese group. Therefore, the effect of obesity on colorectal findings seems more pronounced in proximal locations. Recently, some reports have shown that the distribution of adenomas shifts to the proximal colon, and that increased BMI is associated with increased incidence of proximal colon cancer but not distal colon cancer. 24
In our study, the quality of bowel preparation was inferior in subjects with obesity and morbid obesity. Sharara et al. reviewed the quality of bowel preparation of patients with obesity in several clinical trials in which no association was found, while in a review of several retrospective and non-interventional studies, negative association was found. 25 It was suggested that patients with BMIs of 30 kg/m2 or greater should be considered for a more intensive preparation regimen. 26 Despite inferior bowel preparation in our study, caecal intubation was more frequently achieved in overweight and different degrees of obesity subjects than in subjects without obesity (ORs 1.46–2.00). This translates into an increase of caecal intubation of 2.36% in the group with morbid obesity. The tolerability of the examination itself, as assessed by the screenees and the endoscopist, increased with increasing BMI. These results, to some extent, stand in contrast with the belief that colonoscopy in patients with obesity represents a challenging issue for endoscopists, with much research focussing on the special features of colonoscopy in this population. 22
In our study, male sex was an independent predictor of less inconvenience of the bowel preparation and better tolerability of the examination, as scored by the patient and endoscopist. No relationship to the quality of bowel preparation was noted. Male sex was also a predictor of completeness of the examination with an OR 1.78 (95% CI 1.63–1.94; p < 0.001). Saunders et al. showed that women have a longer colon, predisposing to a loop formation. 27 Compared with men, women have more gluteal and femoral fat, and less visceral fat, providing less support for the colon. 28 Women also have a deeper and rounder pelvis. This results in larger intrapelvic volume and allows more sigmoid looping during colonoscopy. In addition, women have less abdominal wall musculature, which may act as resistance to loop formation. 29
Screening colonoscopy is not a high priority for primary care physicians, patients or both. The fact that patients with obesity, who constitute a high-risk population, receive colorectal cancer screening less often than others is a troubling finding. 30 Physicians may delay performing colorectal cancer screening or referral of patients with obesity for colorectal cancer screening due to competing demands of other comorbid conditions. From the patient’s point of view, people with obesity may avoid getting colorectal cancer screening more than other persons because of embarrassment, concerns about modesty, or fear of pain, or even to avoid being weighed or receiving a lecture about obesity. 31 Underrepresentation of individuals with overweight and individuals with obesity, suggested by several other authors, was not observed in our study. 32 The 2009 annual report of the Central Statistical Office of Poland was used to compare the BMI distribution in the studied cohort and the age-matched general population of Poland (22.51 vs. 22.40% of those with obesity and 45.75 vs. 43.04% of those with overweight in population aged 40–69). 33 The BMI distribution in the study was grossly similar to that of the general population of Poland.
Our study has some limitations. It is a retrospective analysis of a prospectively gathered data set. The BMI calculations were based on declared body weight and height, which may underestimate the actual BMI distribution. The questionnaire used to assess the inconvenience of preparation and tolerance of the examination is not a validated colonoscopy assessment tool; however, it has been routinely used in the programme since 2000. Similar questions, used in a telephone survey, were used in a study by Sarkar et al. 34 In our study, the questionnaire was completed directly after the examination and was filled out by the patient. Therefore, screenees could have refrained from expressing negative opinions. In a study by Denters et al., it was reported that perception worsens further in a follow-up interview after 6 weeks compared with baseline after colonoscopy. 35 Serrated lesions were not classified in this study, as it was not a standard classification during the study period. Another limitation is the fact that data on complications of colonoscopy were not recorded in the database used.
In conclusion, subjects with obesity and morbid obesity, especially males, have higher ADRs and ANDRs during screening colonoscopy. Despite inferior bowel preparation, the completion rates, tolerance of preparation and examination itself are better in subjects with obesity and morbid obesity. The magnitude of the risk disparity between subjects eligible for screening might suggest a need for more active engagement of individuals with excessive body weight in entering screening programmes. Tailoring screening recommendations for overweight and obese individuals does not seem yet justified; however, it might be worth consideration in the future. Therefore, public health efforts should be made at population level to encourage individuals with excessive body weight to participate in CRC screening.
Supplemental Material
Supplementary Material - Supplemental material for Association of obesity with colonic findings in screening colonoscopy in a large population-based study
Supplemental material, Supplementary Material for Association of obesity with colonic findings in screening colonoscopy in a large population-based study by Jarek Kobiela, Paulina Wieszczy, Jarosław Reguła and Michał F Kamiński in United European Gastroenterology Journal
Footnotes
Acknowledgements
Author contributions: JK designed and carried out the study, wrote the manuscript and approved the final version; PW designed the study, analysed the data and approved the final version; JR designed the study, critically revised the manuscript and approved the final version; and MFK designed the study, critically revised the manuscript and approved the final version.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was supported by a grant from the Foundation of Polish Science (TEAM/2012-9/5) financed by European Union structural funds: the Innovative Economy Operational Programme 2007–2013.
Ethics approval
The research proposal was reviewed by the Bioethical Committee at the Maria Sklodowska-Curie Memorial Cancer Centre and Institute of Oncology on 3 October 2014, and was judged to be exempt from oversight, as data was deidentified and could not be linked to specific subject. The study protocol conforms to the 1975 Declaration of Helsinki, as reflected by abovementioned exemption by the Bioethical Committee.
Informed consent
Written informed consent was obtained from all participants entering the national CRC screening programme.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.